- Презентация суставов и позвоночника

Содержание
- 2. Классификация болезней суставов и позвоночника Воспалительные Ревматоидный артрит Анкилозирующий спондилит Реактивный артрит (болезнь Рейтера) Псориатический артрит
- 3. Rheumatoid Arthritis: Background Ревматоидный артрит (РА) – хроническое системное аутоиммунное заболевание синовиальных суставов неизвестной этиологии, характеризующееся
- 4. Ревматоидный артрит
- 5. РА: Эрозии суставов
- 6. Частота: примерно 3 случая на 10,000 населения (распространеность примерно 1%) Ассоциируется со значительной смертностью/заболеваемостью и нетрудоспособностью.
- 7. RA has a significant genetic component, and the so-called shared epitope of the HLA-DR4/DR1 cluster is
- 8. Артропатический псориаз Тяжелое инвалидизирующее заболевание
- 9. АНКИЛОЗИРУЮЩИЙ СПОНДИЛОАРТРИТ: распространенное воспалительное ревматическое заболевание
- 10. RA pathophysiology
- 11. Infliximab (Remicade) E.HSIA, K.Ruley, M.Rahman. APLAR Journal of Rheumatology, 2006; 8: 107-118 Chimeric IgG1 monoclonal antibody
- 12. TNFα Effects
- 13. The American College of Rheumatology (1987) developed the following criteria for the classification of RA. Morning
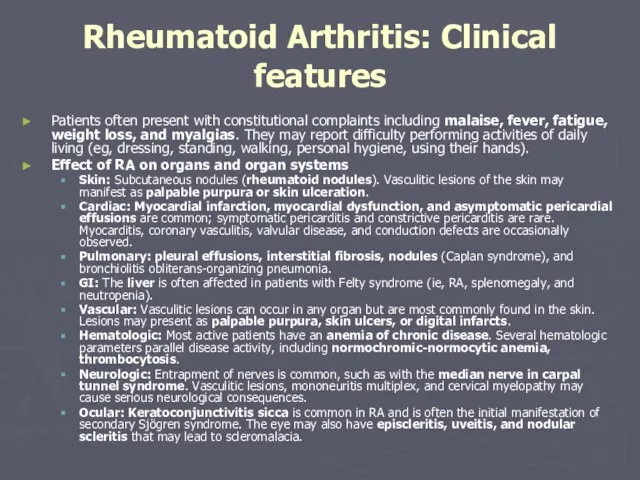
- 14. Patients often present with constitutional complaints including malaise, fever, fatigue, weight loss, and myalgias. They may
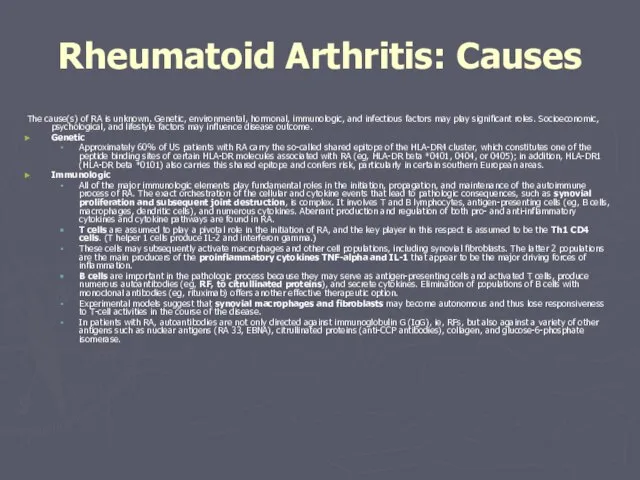
- 15. The cause(s) of RA is unknown. Genetic, environmental, hormonal, immunologic, and infectious factors may play significant
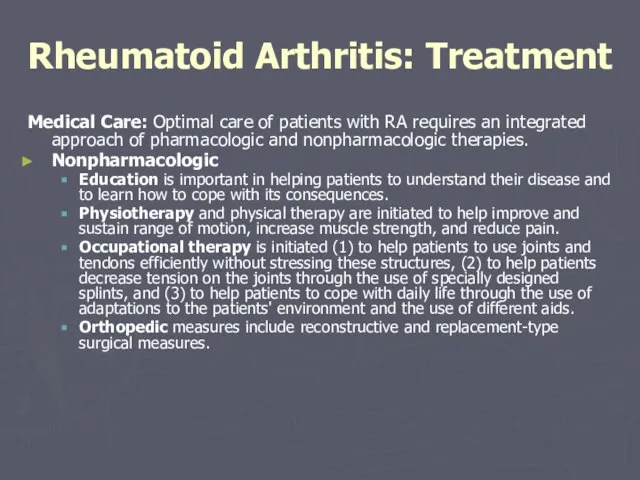
- 16. Medical Care: Optimal care of patients with RA requires an integrated approach of pharmacologic and nonpharmacologic
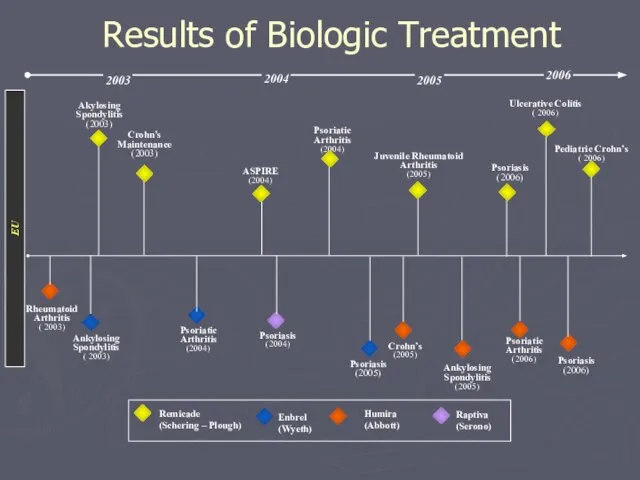
- 17. 2003 2006 Akylosing Spondylitis (2003) Psoriatic Arthritis (2004) Ulcerative Colitis ( 2006) Ankylosing Spondylitis ( 2003)
- 18. Pharmacologic The most important measure to successfully treat RA is the use of DMARDs. DMARDs can
- 19. Biologic agents: The recognition of TNF-alpha and IL-1 as central proinflammatory cytokines has led to the
- 20. Glucocorticoids: Glucocorticoids are potent anti-inflammatory drugs and are commonly used in patients with RA to bridge
- 21. Surgical Care: Cervical spine involvement usually affects C1-C2 and may potentially cause serious neurological consequences. Patients
- 22. Osteoarthritis Background: Osteoarthritis (OA) is the most common articular disease worldwide, affecting over 20 million individuals
- 23. Pathophysiology Traditionally, OA has been considered a disease of articular cartilage. The current concept holds that
- 24. Frequency In the US: OA affects over 20 million individuals. Radiologic definition indicates that more than
- 25. Age OA can be defined epidemiologically (ie, using radiographic criteria) or clinically (eg, radiographs plus clinical
- 26. The etiopathogenesis of OA Stage 1: Proteolytic breakdown of the cartilage matrix occurs. Chondrocyte metabolism is
- 27. Diagnosis Diagnosis usually can be made on clinical grounds. The history and physical examination findings are
- 28. Lab Studies/ Imaging Studies Lab Studies: No specific laboratory abnormalities are associated with OA. The acute-phase
- 29. Medical Care Medical Care (patient education, temperature modalities, weight loss, exercise, physical therapy, occupational therapy) Reduction
- 30. Pharmacologic therapy Begin treatment with acetaminophen for mild or moderate pain without apparent inflammation. If clinical
- 31. The goals of pharmacotherapy are to reduce morbidity and to prevent complications. Pay careful attention to
- 32. Surgical Care Closed-needle joint lavage Arthroscopy Osteotomy Arthroplasty
- 33. Reactive Arthritis and Reiter Syndrome
- 34. Reiter Syndrome •Complicates 1-2% of cases of NGU •Most common peripheral inflammatory arthritis in young men
- 35. Reiter Syndrome •Urethritis: initial manifestation in 80%; other features develop 1-5 weeks later •Arthritis: –Begins within
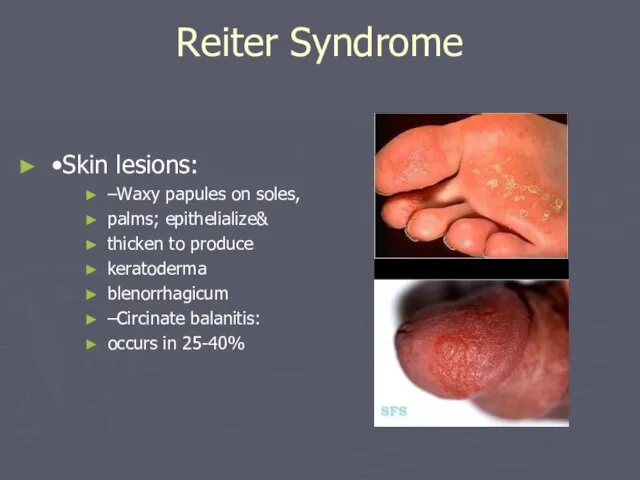
- 36. Reiter Syndrome •Skin lesions: –Waxy papules on soles, palms; epithelialize& thicken to produce keratoderma blenorrhagicum –Circinate
- 37. Reiter Syndrome •Initial episode usually lasts 2-6 months •>50% will relapse •Nearly half develop some degree
- 38. Management of Sex Partners •Chlamydia is isolated from 30-60% of female partners of men with GC
- 39. Asymptomatic STDs % Men Asymptomatic % Women Asymptomatic C.trachomatis 17-56 32-48 N. gonorrhoeae 2-10 33 T.vaginalis
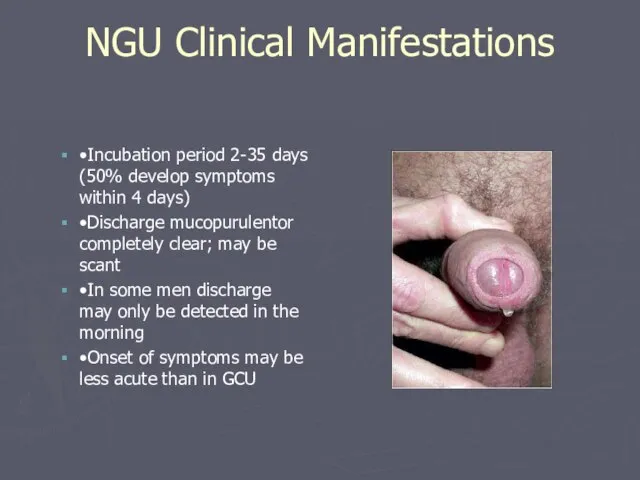
- 40. NGU Clinical Manifestations •Incubation period 2-35 days (50% develop symptoms within 4 days) •Discharge mucopurulentor completely
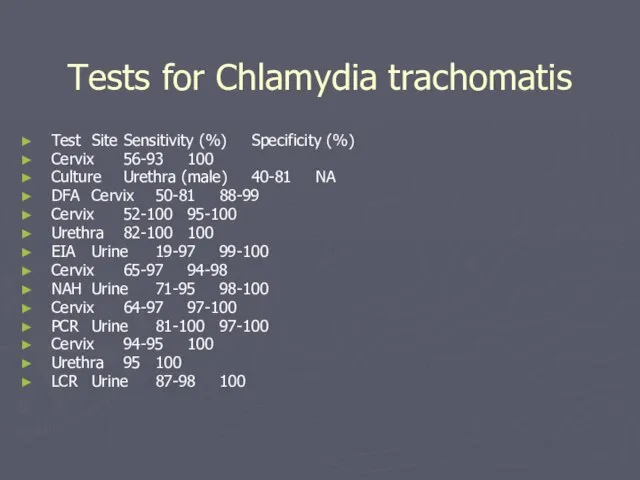
- 41. Tests for Chlamydia trachomatis Test Site Sensitivity (%) Specificity (%) Cervix 56-93 100 Culture Urethra (male)
- 42. Urethral Gram Stain: Non-gonococcal Urethral Gram Stain: Gonococcal
- 43. The syndrome has been associated with gastrointestinal infections with Shigella, Salmonella, and Campylobacter species and other
- 44. Mortality/Morbidity: Reactive arthritis typically follows a self-limited course, with resolution of symptoms by 3-12 months, even
- 45. History: Reactive arthritis usually develops 2-4 weeks after a genitourinary or gastrointestinal infection. The onset is
- 46. Physical: Joints, axial skeleton, entheses. Peripheral joint involvement is typically asymmetric and most frequently affects the
- 47. Medical Care Nonsteroidal anti-inflammatory drugs Corticosteroids Antibiotics (Doxycycline) Disease-modifying antirheumatic drugs (Sulfasalazine, methotrexate)
- 48. Ankylosing Spondylitis Frequency: In the US: The prevalence of ankylosing spondylitis is 0.1-0.2% overall but is
- 49. General symptoms Symptoms include those related to inflammatory back pain, peripheral enthesitis, arthropathy, and constitutional and
- 50. Extraarticular manifestations: Uveitis (also called iritis or iridocyclitis) Cardiovascular involvement (distortion of the aortic ring, resulting
- 51. HLA-B27 HLA-B27 positivity is present in 92% of white patients with ankylosing spondylitis and is present
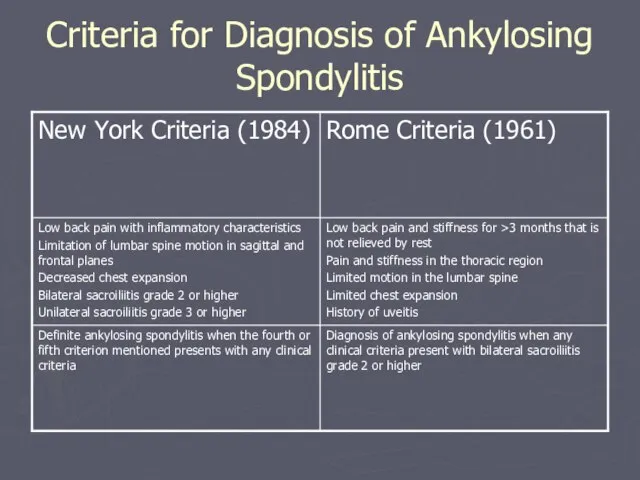
- 52. Criteria for Diagnosis of Ankylosing Spondylitis
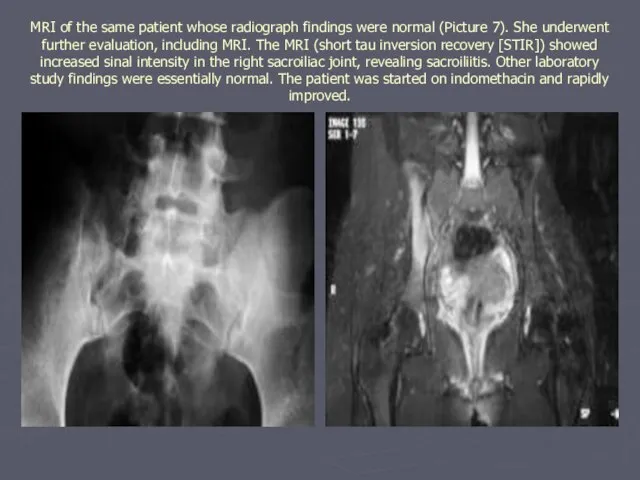
- 53. Imaging Studies Standard radiographs (sacroiliitis is usually bilateral, symmetric, and gradually progressive over years) Magnetic resonance
- 54. Medical Care Nonsteroidal anti-inflammatory drugs Sulfasalazine The TNF-a antagonists have been shown to be effective in
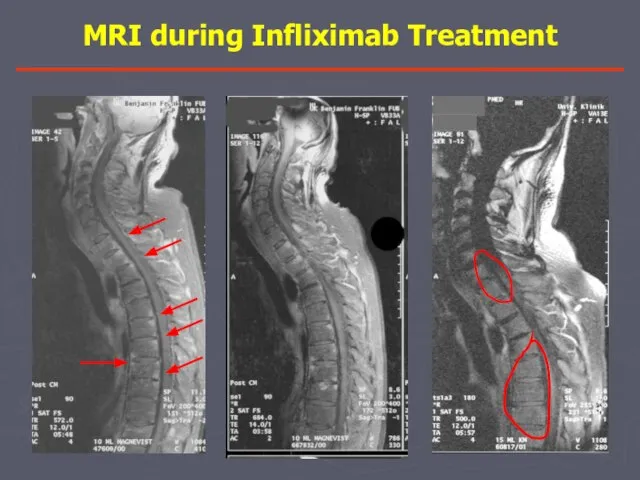
- 55. MRI during Infliximab Treatment 0 неделя 12 неделя
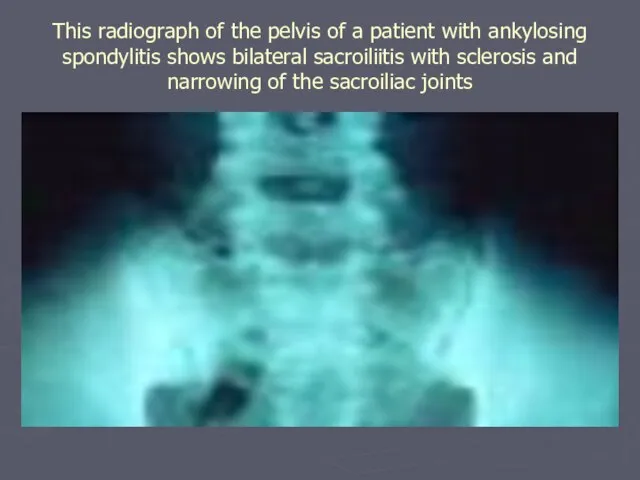
- 56. This radiograph of the pelvis of a patient with ankylosing spondylitis shows bilateral sacroiliitis with sclerosis
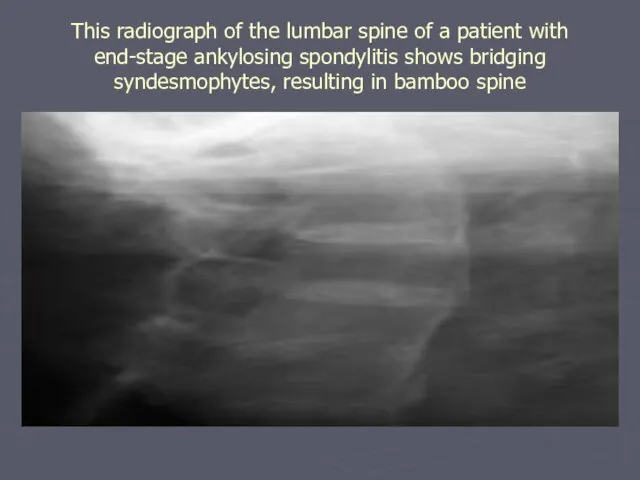
- 57. This radiograph of the lumbar spine of a patient with end-stage ankylosing spondylitis shows bridging syndesmophytes,
- 58. MRI of the same patient whose radiograph findings were normal (Picture 7). She underwent further evaluation,
- 59. Gout Gout is a common disorder of uric acid metabolism that can lead to recurrent episodes
- 60. Gout: Pathophysiology Gout is caused by excess stores of uric acid that accumulate in tissues, including
- 61. Gout: Pathophysiology Gout flares can be triggered by fluxes in uric acid levels or by microtrauma,
- 62. Gout: Frequency Gout is present in approximately 1% of the general population. Gout has a worldwide
- 63. Gout: History Acute monoarticular arthritis is the initial presentation of gout in 90% of patients. In
- 64. Tophi are collections of uric acid crystals in the soft tissues. They occur in more than
- 65. Patients with gout have a 1000-fold increased incidence of renal stones and therefore may have a
- 66. Causes: Gout can develop when excessive stores of uric acid are present. Uric acid is a
- 67. Individual attacks of gout often are triggered by acute fluxes in uric acid levels that may
- 68. Diagnosis Synovial fluid: When a patient presents with acute inflammatory monoarticular arthritis, aspiration of the involved
- 69. TREATMENT There are 3 stages in the management of gout: (1) treating the acute attack, (2)
- 70. Gout: Diet Diet modifications can only improve the serum uric acid levels by 1 mg/dL and
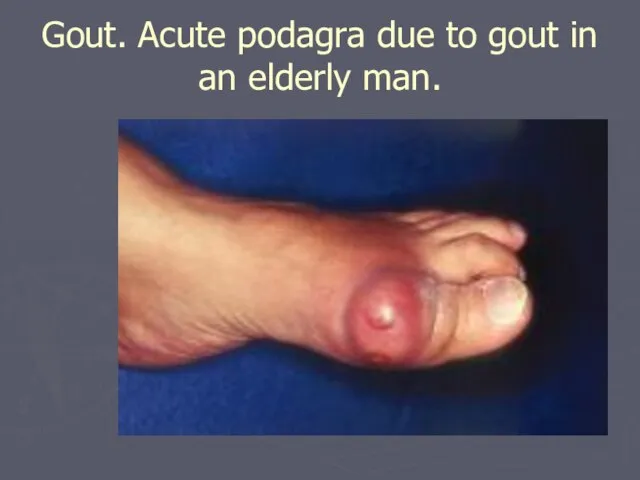
- 71. Gout. Acute podagra due to gout in an elderly man.
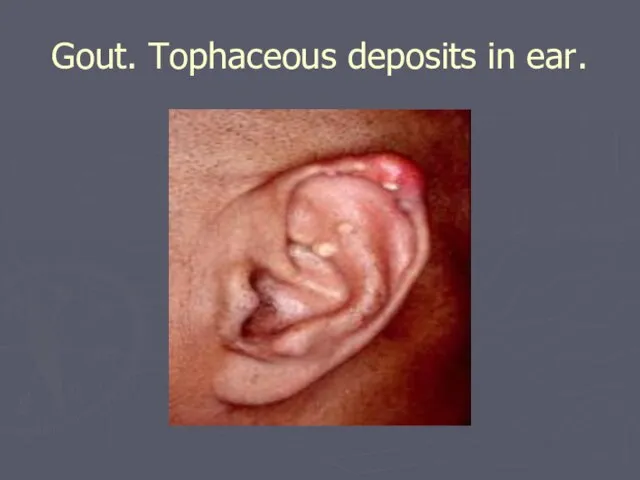
- 72. Gout. Tophaceous deposits in ear.
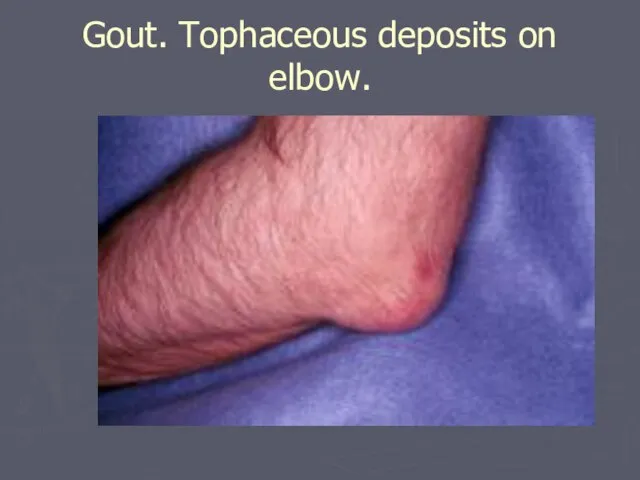
- 73. Gout. Tophaceous deposits on elbow.
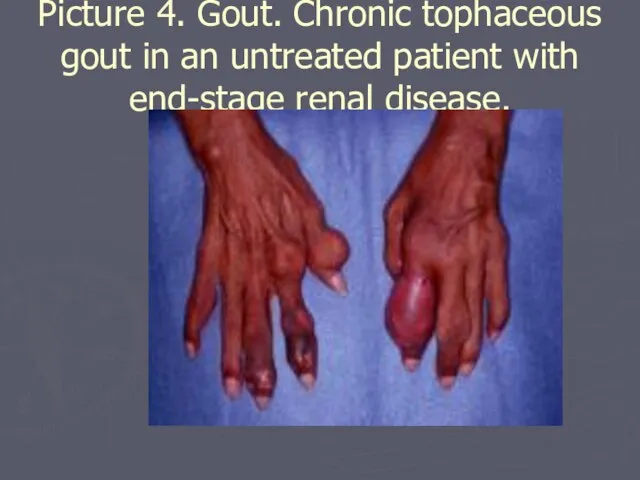
- 74. Picture 4. Gout. Chronic tophaceous gout in an untreated patient with end-stage renal disease.
- 75. Gout. Fluid obtained from a tophaceous deposit in a patient with gout.
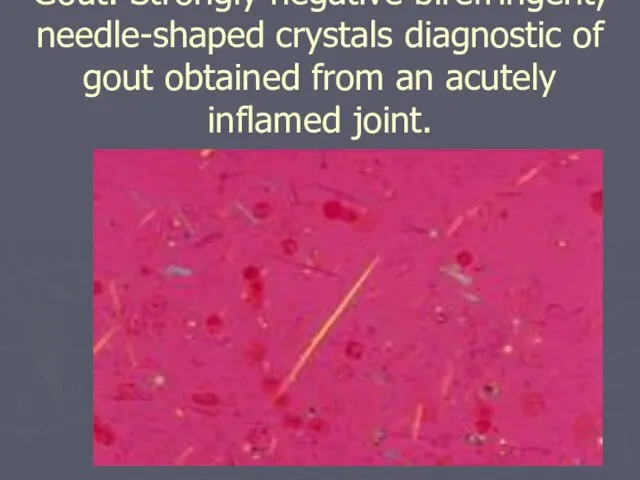
- 76. Gout. Strongly negative birefringent, needle-shaped crystals diagnostic of gout obtained from an acutely inflamed joint.
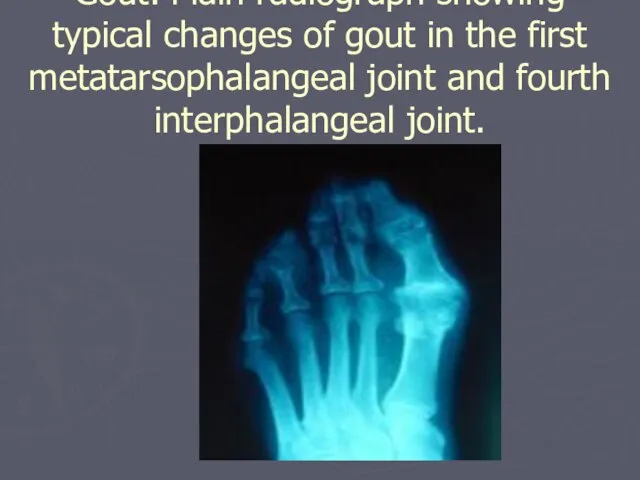
- 77. Gout. Plain radiograph showing typical changes of gout in the first metatarsophalangeal joint and fourth interphalangeal
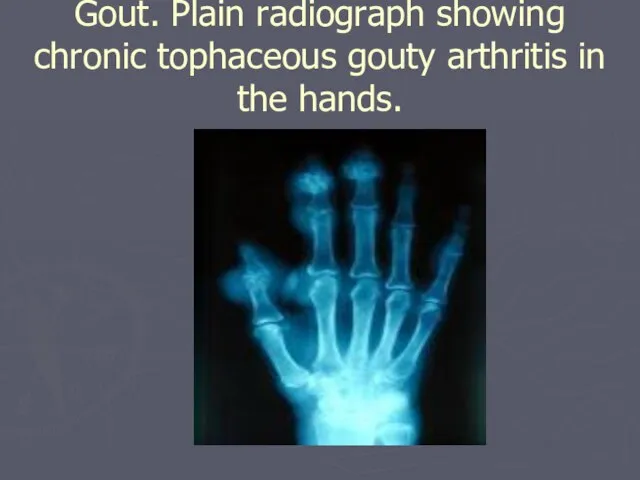
- 78. Gout. Plain radiograph showing chronic tophaceous gouty arthritis in the hands.
- 80. Скачать презентацию
Слайд 2Классификация болезней суставов и позвоночника
Воспалительные
Ревматоидный артрит
Анкилозирующий спондилит
Реактивный артрит (болезнь Рейтера)
Псориатический артрит
Дегенеративные
Остеоартроз
остеохондроз
Метаболические
Подагра
Пирофосфатная артропатия
Классификация болезней суставов и позвоночника
Воспалительные
Ревматоидный артрит
Анкилозирующий спондилит
Реактивный артрит (болезнь Рейтера)
Псориатический артрит
Дегенеративные
Остеоартроз
остеохондроз
Метаболические
Подагра
Пирофосфатная артропатия
Слайд 3Rheumatoid Arthritis: Background
Ревматоидный артрит (РА) – хроническое системное аутоиммунное заболевание синовиальных суставов
Rheumatoid Arthritis: Background
Ревматоидный артрит (РА) – хроническое системное аутоиммунное заболевание синовиальных суставов
Слайд 4Ревматоидный артрит
Ревматоидный артрит

Слайд 5РА: Эрозии суставов
РА: Эрозии суставов

Слайд 6Частота: примерно 3 случая на 10,000 населения (распространеность примерно 1%)
Ассоциируется со значительной
Частота: примерно 3 случая на 10,000 населения (распространеность примерно 1%)
Ассоциируется со значительной
Слайд 7RA has a significant genetic component, and the so-called shared epitope of
RA has a significant genetic component, and the so-called shared epitope of
Слайд 8Артропатический псориаз
Тяжелое инвалидизирующее заболевание
Артропатический псориаз
Тяжелое инвалидизирующее заболевание

Слайд 9АНКИЛОЗИРУЮЩИЙ СПОНДИЛОАРТРИТ:
распространенное воспалительное ревматическое заболевание
АНКИЛОЗИРУЮЩИЙ СПОНДИЛОАРТРИТ:
распространенное воспалительное ревматическое заболевание

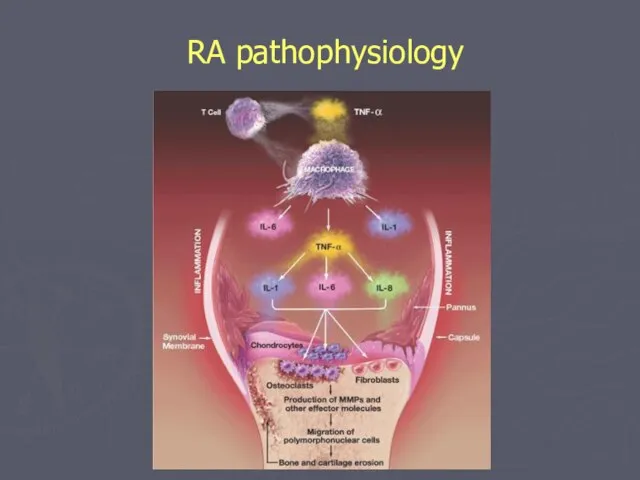
Слайд 10RA pathophysiology
RA pathophysiology
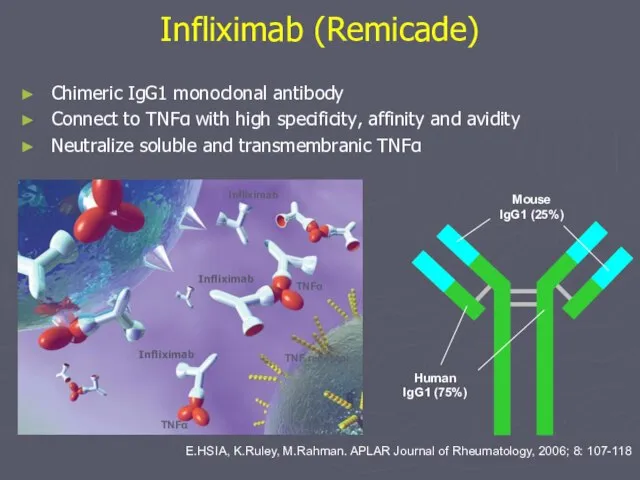
Слайд 11Infliximab (Remicade)
E.HSIA, K.Ruley, M.Rahman. APLAR Journal of Rheumatology, 2006; 8: 107-118
Chimeric IgG1
Infliximab (Remicade)
E.HSIA, K.Ruley, M.Rahman. APLAR Journal of Rheumatology, 2006; 8: 107-118
Chimeric IgG1
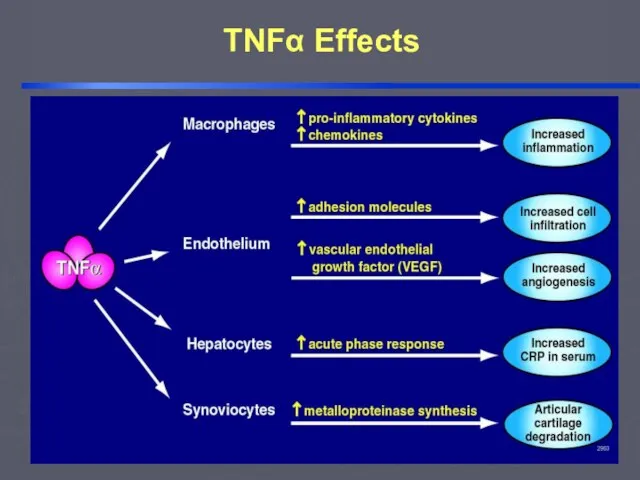
Слайд 12TNFα Effects
TNFα Effects
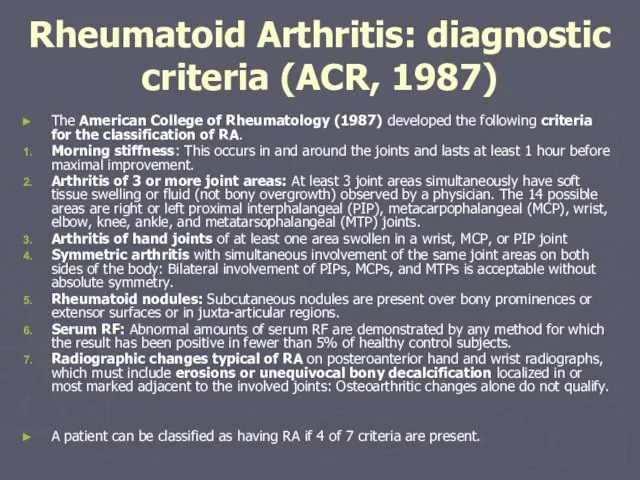
Слайд 13The American College of Rheumatology (1987) developed the following criteria for the
The American College of Rheumatology (1987) developed the following criteria for the
Слайд 14Patients often present with constitutional complaints including malaise, fever, fatigue, weight loss,
Patients often present with constitutional complaints including malaise, fever, fatigue, weight loss,
Слайд 15The cause(s) of RA is unknown. Genetic, environmental, hormonal, immunologic, and infectious
The cause(s) of RA is unknown. Genetic, environmental, hormonal, immunologic, and infectious
Слайд 16Medical Care: Optimal care of patients with RA requires an integrated approach
Medical Care: Optimal care of patients with RA requires an integrated approach
Слайд 172003
2006
Akylosing Spondylitis
(2003)
Psoriatic
Arthritis
(2004)
Ulcerative Colitis
( 2006)
Ankylosing
Spondylitis
( 2003)
2004
Crohn’s
(2005)
Humira
(Abbott)
Remicade
(Schering – Plough)
Psoriasis
(2006)
ASPIRE
(2004)
EU
Crohn’s Maintenance
2003
2006
Akylosing Spondylitis
(2003)
Psoriatic
Arthritis
(2004)
Ulcerative Colitis
( 2006)
Ankylosing
Spondylitis
( 2003)
2004
Crohn’s
(2005)
Humira
(Abbott)
Remicade
(Schering – Plough)
Psoriasis
(2006)
ASPIRE
(2004)
EU
Crohn’s Maintenance
Слайд 18Pharmacologic
The most important measure to successfully treat RA is the use of
Pharmacologic
The most important measure to successfully treat RA is the use of
Слайд 19Biologic agents:
The recognition of TNF-alpha and IL-1 as central proinflammatory cytokines
Biologic agents:
The recognition of TNF-alpha and IL-1 as central proinflammatory cytokines
Слайд 20Glucocorticoids:
Glucocorticoids are potent anti-inflammatory drugs and are commonly used in patients
Glucocorticoids:
Glucocorticoids are potent anti-inflammatory drugs and are commonly used in patients
Слайд 21Surgical Care:
Cervical spine involvement usually affects C1-C2 and may potentially cause
Cervical spine involvement usually affects C1-C2 and may potentially cause
Слайд 22Osteoarthritis
Background: Osteoarthritis (OA) is the most common articular disease worldwide, affecting over
Osteoarthritis
Background: Osteoarthritis (OA) is the most common articular disease worldwide, affecting over
Слайд 23Pathophysiology
Traditionally, OA has been considered a disease of articular cartilage. The current
Pathophysiology
Traditionally, OA has been considered a disease of articular cartilage. The current
Слайд 24Frequency
In the US: OA affects over 20 million individuals. Radiologic definition indicates
Frequency
In the US: OA affects over 20 million individuals. Radiologic definition indicates
Слайд 25Age
OA can be defined epidemiologically (ie, using radiographic criteria) or clinically (eg,
Age
OA can be defined epidemiologically (ie, using radiographic criteria) or clinically (eg,
Слайд 26The etiopathogenesis of OA
Stage 1: Proteolytic breakdown of the cartilage matrix occurs.
The etiopathogenesis of OA
Stage 1: Proteolytic breakdown of the cartilage matrix occurs.
Слайд 27Diagnosis
Diagnosis usually can be made on clinical grounds. The history and physical
Diagnosis
Diagnosis usually can be made on clinical grounds. The history and physical
Слайд 28Lab Studies/ Imaging Studies
Lab Studies:
No specific laboratory abnormalities are associated with
Lab Studies/ Imaging Studies
Lab Studies:
No specific laboratory abnormalities are associated with
Слайд 29Medical Care
Medical Care (patient education, temperature modalities, weight loss, exercise, physical therapy,
Medical Care
Medical Care (patient education, temperature modalities, weight loss, exercise, physical therapy,
Слайд 30Pharmacologic therapy
Begin treatment with acetaminophen for mild or moderate pain without apparent
Pharmacologic therapy
Begin treatment with acetaminophen for mild or moderate pain without apparent
Слайд 31The goals of pharmacotherapy are to reduce morbidity and to prevent complications.
The goals of pharmacotherapy are to reduce morbidity and to prevent complications.
Слайд 32Surgical Care
Closed-needle joint lavage
Arthroscopy
Osteotomy
Arthroplasty
Surgical Care
Closed-needle joint lavage
Arthroscopy
Osteotomy
Arthroplasty
Слайд 33Reactive Arthritis and Reiter Syndrome
Reactive Arthritis and Reiter Syndrome
Слайд 34Reiter Syndrome
•Complicates 1-2% of cases of NGU
•Most common peripheral inflammatory arthritis in
Reiter Syndrome
•Complicates 1-2% of cases of NGU
•Most common peripheral inflammatory arthritis in
Слайд 35Reiter Syndrome
•Urethritis: initial manifestation in 80%; other features develop 1-5 weeks later
•Arthritis:
–Begins
Reiter Syndrome
•Urethritis: initial manifestation in 80%; other features develop 1-5 weeks later
•Arthritis:
–Begins
Слайд 36Reiter Syndrome
•Skin lesions:
–Waxy papules on soles,
palms; epithelialize&
thicken to produce
keratoderma
blenorrhagicum
–Circinate
Reiter Syndrome
•Skin lesions:
–Waxy papules on soles,
palms; epithelialize&
thicken to produce
keratoderma
blenorrhagicum
–Circinate
Слайд 37Reiter Syndrome
•Initial episode usually lasts 2-6 months
•>50% will relapse
•Nearly half develop
Reiter Syndrome
•Initial episode usually lasts 2-6 months
•>50% will relapse
•Nearly half develop
Слайд 38Management of Sex Partners
•Chlamydia is isolated from 30-60% of female partners of
Management of Sex Partners
•Chlamydia is isolated from 30-60% of female partners of
Слайд 39Asymptomatic STDs
% Men Asymptomatic % Women Asymptomatic
C.trachomatis 17-56 32-48
N. gonorrhoeae 2-10 33
T.vaginalis 6-50 50
Asymptomatic STDs
% Men Asymptomatic % Women Asymptomatic
C.trachomatis 17-56 32-48
N.
% Men Asymptomatic % Women Asymptomatic
C.trachomatis 17-56 32-48
N. gonorrhoeae 2-10 33
T.vaginalis 6-50 50
Asymptomatic STDs
% Men Asymptomatic % Women Asymptomatic
C.trachomatis 17-56 32-48
N.
Слайд 40NGU Clinical Manifestations
•Incubation period 2-35 days (50% develop symptoms within 4 days)
•Discharge
NGU Clinical Manifestations
•Incubation period 2-35 days (50% develop symptoms within 4 days)
•Discharge
Слайд 41
Tests for Chlamydia trachomatis
Test Site Sensitivity (%) Specificity (%)
Cervix 56-93 100
Culture Urethra (male) 40-81 NA
DFA Cervix 50-81 88-99
Cervix 52-100 95-100
Urethra 82-100 100
EIA Urine 19-97 99-100
Cervix 65-97 94-98
NAH Urine 71-95 98-100
Cervix 64-97 97-100
PCR Urine 81-100 97-100
Cervix 94-95 100
Urethra 95 100
LCR Urine 87-98 100
Tests for Chlamydia trachomatis
Test Site Sensitivity (%) Specificity (%)
Cervix 56-93 100
Culture Urethra (male) 40-81 NA
DFA Cervix 50-81 88-99
Cervix 52-100 95-100
Urethra 82-100 100
EIA Urine 19-97 99-100
Cervix 65-97 94-98
NAH Urine 71-95 98-100
Cervix 64-97 97-100
PCR Urine 81-100 97-100
Cervix 94-95 100
Urethra 95 100
LCR Urine 87-98 100
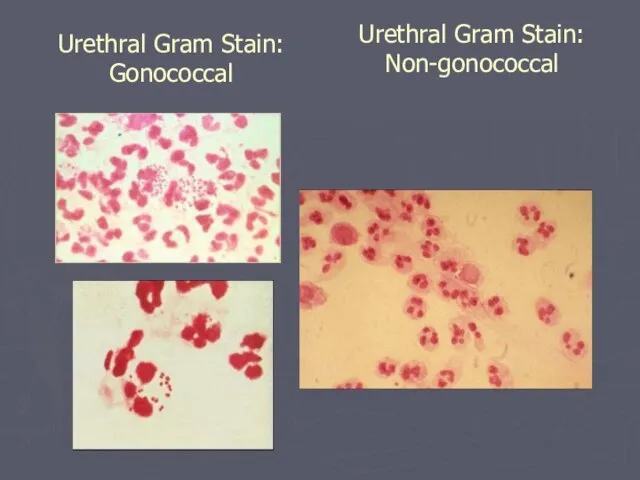
Слайд 42Urethral Gram Stain:
Non-gonococcal
Urethral Gram Stain:
Gonococcal
Urethral Gram Stain:
Non-gonococcal
Urethral Gram Stain:
Gonococcal
Слайд 43The syndrome has been associated with gastrointestinal infections with Shigella, Salmonella, and
The syndrome has been associated with gastrointestinal infections with Shigella, Salmonella, and
Слайд 44Mortality/Morbidity: Reactive arthritis typically follows a self-limited course, with resolution of symptoms
Mortality/Morbidity: Reactive arthritis typically follows a self-limited course, with resolution of symptoms
Слайд 45History: Reactive arthritis usually develops 2-4 weeks after a genitourinary or gastrointestinal
History: Reactive arthritis usually develops 2-4 weeks after a genitourinary or gastrointestinal
Слайд 46Physical:
Joints, axial skeleton, entheses. Peripheral joint involvement is typically asymmetric and
Physical:
Joints, axial skeleton, entheses. Peripheral joint involvement is typically asymmetric and
Слайд 47Medical Care
Nonsteroidal anti-inflammatory drugs
Corticosteroids
Antibiotics (Doxycycline)
Disease-modifying antirheumatic drugs (Sulfasalazine, methotrexate)
Medical Care
Nonsteroidal anti-inflammatory drugs
Corticosteroids
Antibiotics (Doxycycline)
Disease-modifying antirheumatic drugs (Sulfasalazine, methotrexate)
Слайд 48Ankylosing Spondylitis
Frequency: In the US: The prevalence of ankylosing spondylitis is 0.1-0.2%
Ankylosing Spondylitis
Frequency: In the US: The prevalence of ankylosing spondylitis is 0.1-0.2%
Слайд 49General symptoms
Symptoms include those related to inflammatory back pain, peripheral enthesitis, arthropathy,
General symptoms
Symptoms include those related to inflammatory back pain, peripheral enthesitis, arthropathy,
Слайд 50Extraarticular manifestations:
Uveitis (also called iritis or iridocyclitis)
Cardiovascular involvement (distortion of the aortic
Extraarticular manifestations:
Uveitis (also called iritis or iridocyclitis)
Cardiovascular involvement (distortion of the aortic
Слайд 51HLA-B27
HLA-B27 positivity is present in 92% of white patients with ankylosing
HLA-B27
HLA-B27 positivity is present in 92% of white patients with ankylosing
Слайд 52Criteria for Diagnosis of Ankylosing Spondylitis
Criteria for Diagnosis of Ankylosing Spondylitis
Слайд 53Imaging Studies
Standard radiographs (sacroiliitis is usually bilateral, symmetric, and gradually progressive over
Imaging Studies
Standard radiographs (sacroiliitis is usually bilateral, symmetric, and gradually progressive over
Слайд 54Medical Care
Nonsteroidal anti-inflammatory drugs
Sulfasalazine
The TNF-a antagonists have been shown to be effective
Medical Care
Nonsteroidal anti-inflammatory drugs
Sulfasalazine
The TNF-a antagonists have been shown to be effective
Слайд 55MRI during Infliximab Treatment
0 неделя
12 неделя
MRI during Infliximab Treatment
0 неделя
12 неделя
Слайд 56This radiograph of the pelvis of a patient with ankylosing spondylitis shows
This radiograph of the pelvis of a patient with ankylosing spondylitis shows
Слайд 57This radiograph of the lumbar spine of a patient with end-stage ankylosing
This radiograph of the lumbar spine of a patient with end-stage ankylosing
Слайд 58MRI of the same patient whose radiograph findings were normal (Picture 7).
MRI of the same patient whose radiograph findings were normal (Picture 7).
Слайд 59Gout
Gout is a common disorder of uric acid metabolism that can lead
Gout
Gout is a common disorder of uric acid metabolism that can lead
Слайд 60Gout: Pathophysiology
Gout is caused by excess stores of uric acid that
Gout: Pathophysiology
Gout is caused by excess stores of uric acid that
Слайд 61Gout: Pathophysiology
Gout flares can be triggered by fluxes in uric acid
Gout: Pathophysiology
Gout flares can be triggered by fluxes in uric acid
Слайд 62Gout: Frequency
Gout is present in approximately 1% of the general population.
Gout
Gout: Frequency
Gout is present in approximately 1% of the general population.
Gout
Слайд 63Gout: History
Acute monoarticular arthritis is the initial presentation of gout in 90%
Gout: History
Acute monoarticular arthritis is the initial presentation of gout in 90%
Слайд 64Tophi are collections of uric acid crystals in the soft tissues. They
Tophi are collections of uric acid crystals in the soft tissues. They
Слайд 65Patients with gout have a 1000-fold increased incidence of renal stones and
Patients with gout have a 1000-fold increased incidence of renal stones and
Слайд 66Causes: Gout can develop when excessive stores of uric acid are present.
Causes: Gout can develop when excessive stores of uric acid are present.
Слайд 67Individual attacks of gout often are triggered by acute fluxes in uric
Individual attacks of gout often are triggered by acute fluxes in uric
Слайд 68Diagnosis
Synovial fluid: When a patient presents with acute inflammatory monoarticular arthritis, aspiration
Diagnosis
Synovial fluid: When a patient presents with acute inflammatory monoarticular arthritis, aspiration
Слайд 69TREATMENT
There are 3 stages in the management of gout: (1) treating
TREATMENT
There are 3 stages in the management of gout: (1) treating
Слайд 70Gout: Diet
Diet modifications can only improve the serum uric acid levels by
Gout: Diet
Diet modifications can only improve the serum uric acid levels by
Слайд 71Gout. Acute podagra due to gout in an elderly man.
Gout. Acute podagra due to gout in an elderly man.
Слайд 72Gout. Tophaceous deposits in ear.
Gout. Tophaceous deposits in ear.
Слайд 73Gout. Tophaceous deposits on elbow.
Gout. Tophaceous deposits on elbow.
Слайд 74Picture 4. Gout. Chronic tophaceous gout in an untreated patient with end-stage
Picture 4. Gout. Chronic tophaceous gout in an untreated patient with end-stage
Слайд 75Gout. Fluid obtained from a tophaceous deposit in a patient with gout.
Gout. Fluid obtained from a tophaceous deposit in a patient with gout.
Слайд 76Gout. Strongly negative birefringent, needle-shaped crystals diagnostic of gout obtained from an
Gout. Strongly negative birefringent, needle-shaped crystals diagnostic of gout obtained from an
Слайд 77Gout. Plain radiograph showing typical changes of gout in the first metatarsophalangeal
Gout. Plain radiograph showing typical changes of gout in the first metatarsophalangeal
Слайд 78Gout. Plain radiograph showing chronic tophaceous gouty arthritis in the hands.
Gout. Plain radiograph showing chronic tophaceous gouty arthritis in the hands.
 Получите новых клиентов в 2 раза дешевле с помощью Антикризисного маркетинга! Создание продающих сайтов!
Получите новых клиентов в 2 раза дешевле с помощью Антикризисного маркетинга! Создание продающих сайтов! Детские поэты и писатели
Детские поэты и писатели  Правильное питание школьников
Правильное питание школьников Проектная деятельность в работе с обучающимися. Информационно- коммуникационные технологии в учебно-воспитательном процессе.
Проектная деятельность в работе с обучающимися. Информационно- коммуникационные технологии в учебно-воспитательном процессе. Благодарность или коррупция, есть ли золотая середина
Благодарность или коррупция, есть ли золотая середина Твоих садов ажурные ограды…
Твоих садов ажурные ограды… 1
1 Слайд оқу сауаттылық
Слайд оқу сауаттылық Пантеон - храм всех богов
Пантеон - храм всех богов ФГБОУ ВПО «НОВОСИБИРСКИЙ ГОСУДАРСТВЕННЫЙ ПЕДАГОГИЧЕСКИЙ УНИВЕРСИТЕТ»
ФГБОУ ВПО «НОВОСИБИРСКИЙ ГОСУДАРСТВЕННЫЙ ПЕДАГОГИЧЕСКИЙ УНИВЕРСИТЕТ» Этика деловых отношений. Коммуникативная сторона общения. ЛЕКЦИЯ 1
Этика деловых отношений. Коммуникативная сторона общения. ЛЕКЦИЯ 1 Исследование по улучшению доступности лекарств для лечения пациентов с бронхиальной астмой в рамках Программы Государственных Г
Исследование по улучшению доступности лекарств для лечения пациентов с бронхиальной астмой в рамках Программы Государственных Г Африка
Африка МОУ Тудовская основная общеобразовательная школа
МОУ Тудовская основная общеобразовательная школа Единая Служба Знакомств и Общения
Единая Служба Знакомств и Общения БРЯНСКИЙ ЗАВОДпо производству изделий из ПВХ
БРЯНСКИЙ ЗАВОДпо производству изделий из ПВХ Сангина
Сангина Урок по рассказу Ивана Бунина «Холодная осень»
Урок по рассказу Ивана Бунина «Холодная осень» Презентация на тему Религия Индии
Презентация на тему Религия Индии  Авторская воспитательная система Католикова
Авторская воспитательная система Католикова Пейзаж в живописи
Пейзаж в живописи Станки лазерной и плазменной обработки
Станки лазерной и плазменной обработки Алена Терещенко и Роман Белоснежный представляют кампанию по приглашению твое преображение каталоги №11-13
Алена Терещенко и Роман Белоснежный представляют кампанию по приглашению твое преображение каталоги №11-13 РЕЧЬ В ШКОЛЕ
РЕЧЬ В ШКОЛЕ ~의 수. Корейский язык
~의 수. Корейский язык Идеал красоты в искусстве
Идеал красоты в искусстве НОД и НОК Делимость чисел
НОД и НОК Делимость чисел «Школьная риторика»под редакцией Т.А. Ладыженской
«Школьная риторика»под редакцией Т.А. Ладыженской