- Wounds. wounds healing amp complications

Содержание
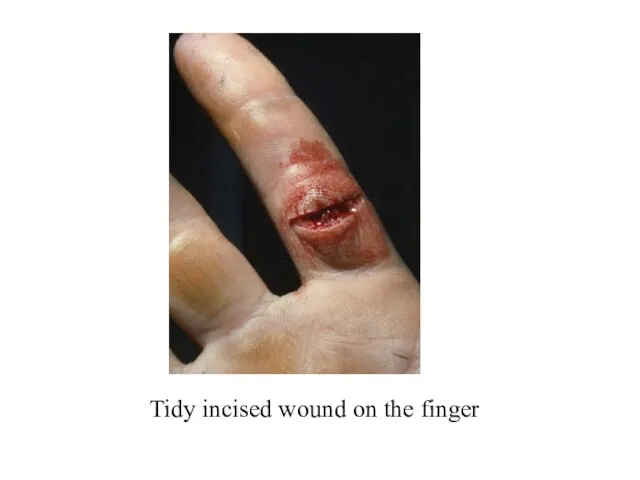
- 10. Tidy incised wound on the finger
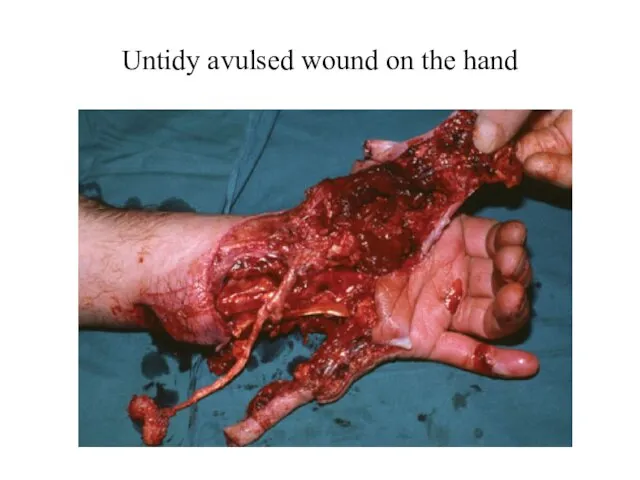
- 17. Untidy avulsed wound on the hand
- 18. Facial trauma – apparent tissue loss but none found after careful matching
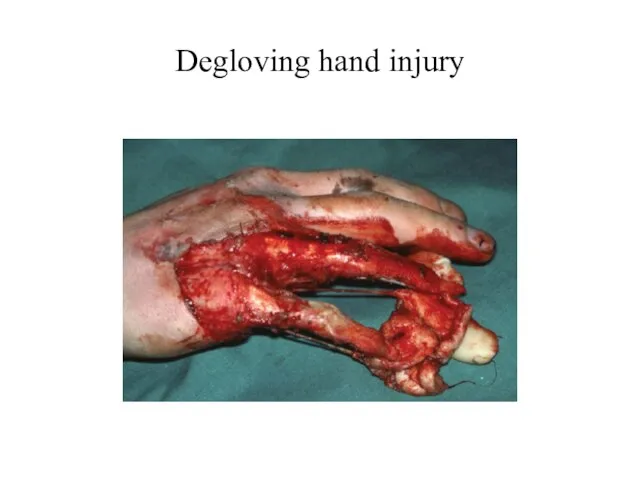
- 19. Degloving hand injury
- 20. Dog bite in a child
- 21. Degloving buttock injury
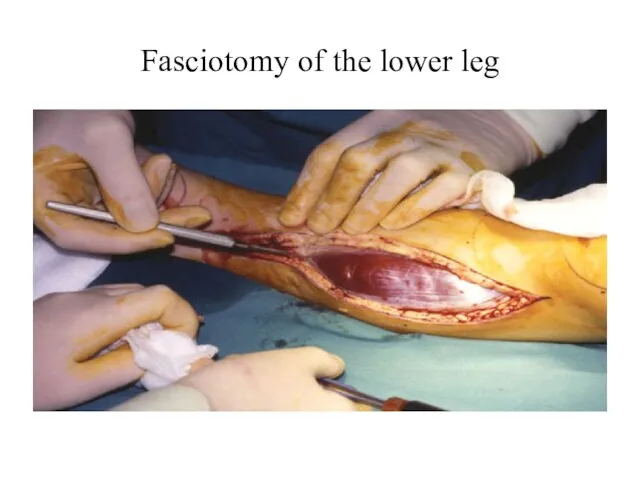
- 22. Fasciotomy of the lower leg
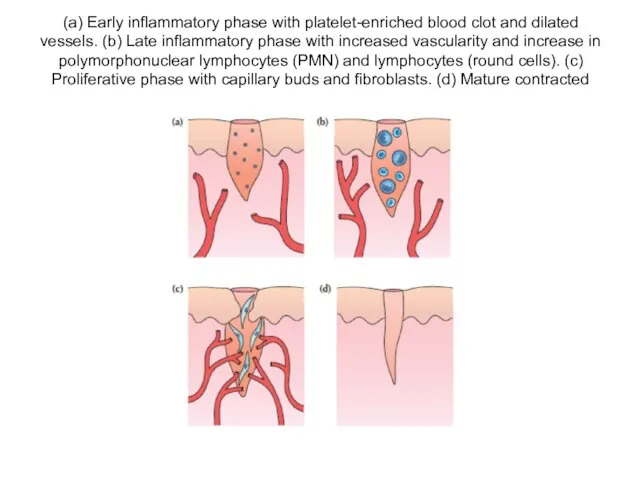
- 34. (a) Early inflammatory phase with platelet-enriched blood clot and dilated vessels. (b) Late inflammatory phase with
- 70. Multiple keloid scars
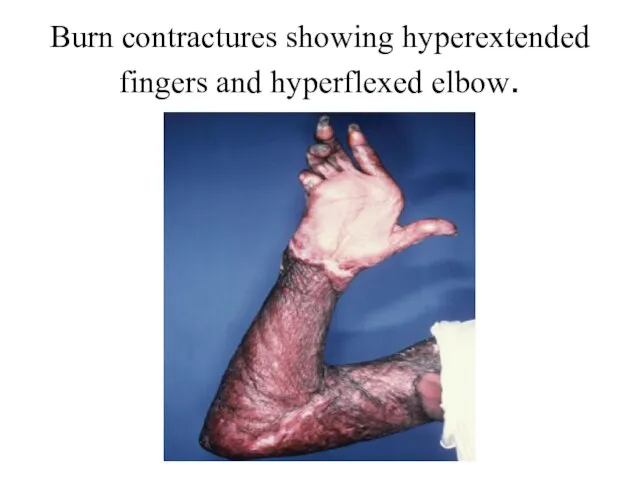
- 74. Burn contractures showing hyperextended fingers and hyperflexed elbow.
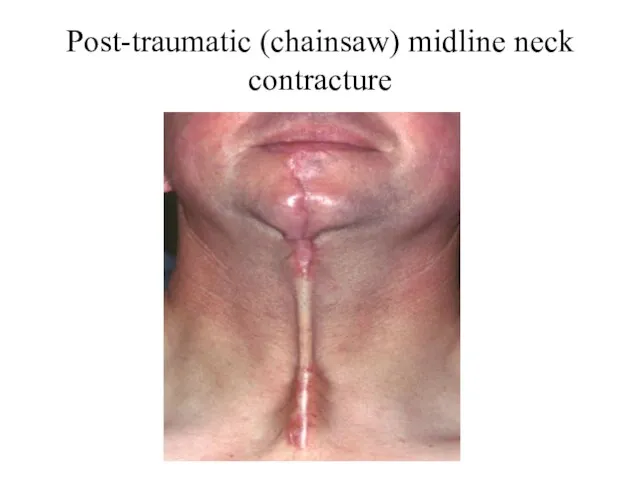
- 75. Post-traumatic (chainsaw) midline neck contracture
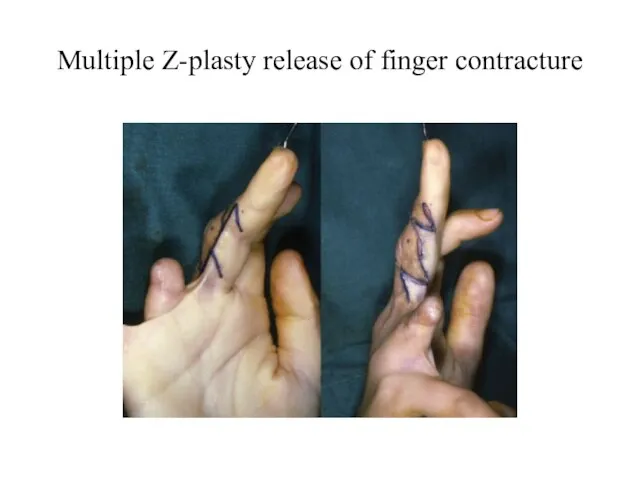
- 76. Multiple Z-plasty release of finger contracture
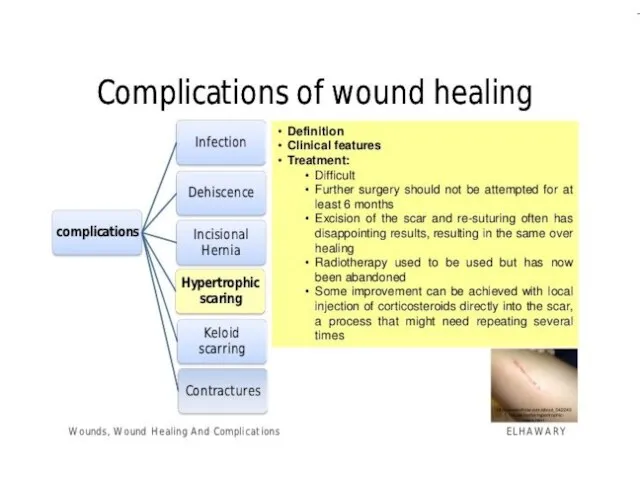
- 77. Treatment of hypertrophic and keloid scars Pressure – local moulds or elasticated garments Silicone gel sheeting
- 78. MANAGING THE ACUTE WOUND The surgeon must remember to examine the whole patient A bleeding wound
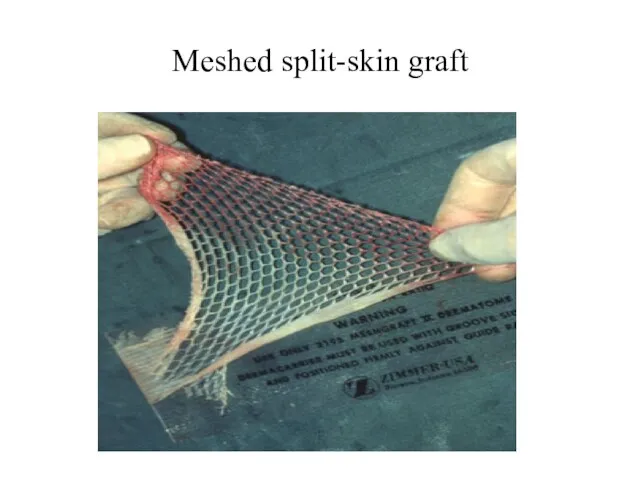
- 79. Meshed split-skin graft
- 80. Managing the acute wound Cleansing Exploration and diagnosis Debridement Repair of structures Replacement of lost tissues
- 81. CHRONIC WOUNDS 1.Leg ulcers Aetiology of leg ulcers Venous disease leading to local venous hypertension (e.g.
- 83. Скачать презентацию
Слайд 10
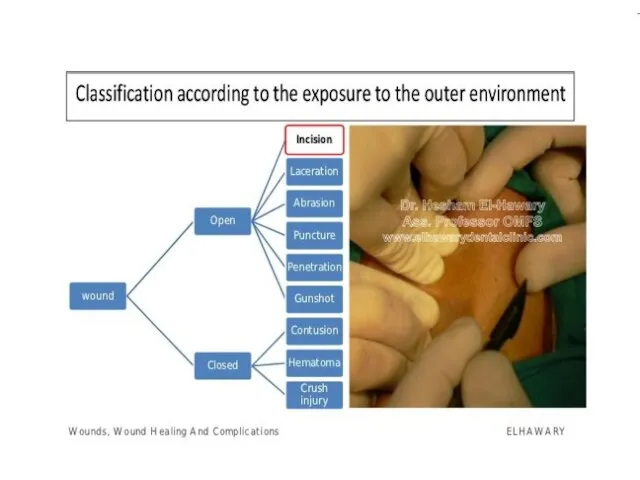
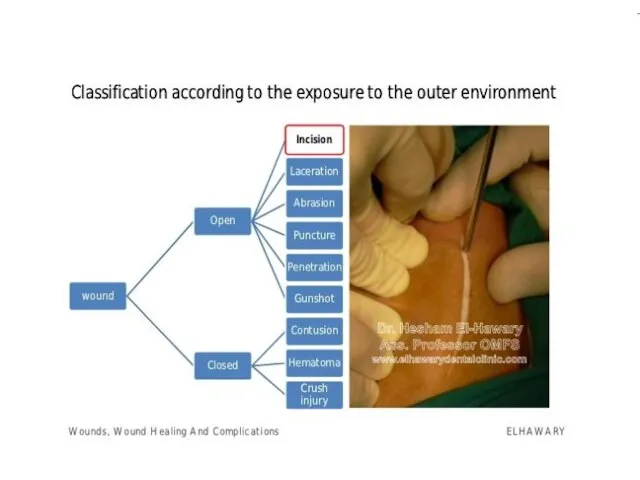
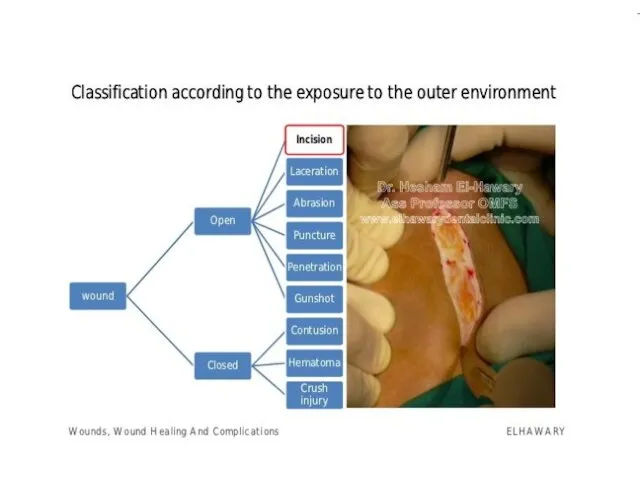
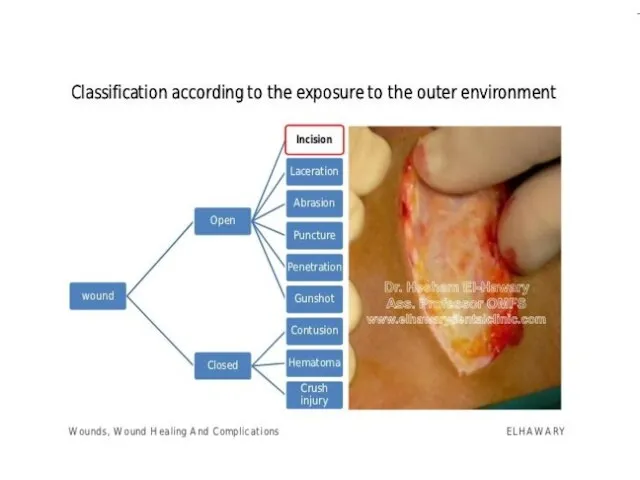
Tidy incised wound on the finger
Tidy incised wound on the finger
Слайд 17Untidy avulsed wound on the hand
Untidy avulsed wound on the hand
Слайд 18Facial trauma – apparent tissue loss but none found after careful matching
Facial trauma – apparent tissue loss but none found after careful matching

Слайд 19Degloving hand injury
Degloving hand injury
Слайд 20Dog bite in a child
Dog bite in a child

Слайд 21Degloving buttock injury
Degloving buttock injury

Слайд 22Fasciotomy of the lower leg
Fasciotomy of the lower leg
Слайд 34(a) Early inflammatory phase with platelet-enriched blood clot and dilated vessels. (b)
(a) Early inflammatory phase with platelet-enriched blood clot and dilated vessels. (b)




Слайд 70Multiple keloid scars
Multiple keloid scars


Слайд 74Burn contractures showing hyperextended fingers and hyperflexed elbow.
Burn contractures showing hyperextended fingers and hyperflexed elbow.
Слайд 75Post-traumatic (chainsaw) midline neck contracture
Post-traumatic (chainsaw) midline neck contracture
Слайд 76Multiple Z-plasty release of finger contracture
Multiple Z-plasty release of finger contracture
Слайд 77Treatment of hypertrophic and keloid scars
Pressure – local moulds or elasticated garments
Silicone
Treatment of hypertrophic and keloid scars
Pressure – local moulds or elasticated garments
Silicone
Слайд 78MANAGING THE ACUTE WOUND
The surgeon must remember to examine the whole patient
A
MANAGING THE ACUTE WOUND
The surgeon must remember to examine the whole patient
A
Слайд 79Meshed split-skin graft
Meshed split-skin graft
Слайд 80Managing the acute wound
Cleansing
Exploration and diagnosis
Debridement
Repair of structures
Replacement of lost tissues where
Managing the acute wound
Cleansing
Exploration and diagnosis
Debridement
Repair of structures
Replacement of lost tissues where
Слайд 81CHRONIC WOUNDS
1.Leg ulcers
Aetiology of leg ulcers
Venous disease leading to local venous hypertension
CHRONIC WOUNDS
1.Leg ulcers
Aetiology of leg ulcers
Venous disease leading to local venous hypertension
 Многофигурная композиция на свободную тему
Многофигурная композиция на свободную тему Белокуриха. Фотографии
Белокуриха. Фотографии Презентация проектаНетрадиционные способы изображения в изодеятельности
Презентация проектаНетрадиционные способы изображения в изодеятельности Имущественные отношения супругов:
Имущественные отношения супругов: Вучетич Евгений Викторович (1908-1974)
Вучетич Евгений Викторович (1908-1974) Подсолнух
Подсолнух Из рода странников небесных
Из рода странников небесных Копия_Лекция_2_Концепты_русской_культуры
Копия_Лекция_2_Концепты_русской_культуры Дисциплина: Товароведение и экспертиза товаров Тема: Металлохозяйственные товары
Дисциплина: Товароведение и экспертиза товаров Тема: Металлохозяйственные товары Агенти політичних відносин
Агенти політичних відносин Стекловолокно. Получение стекловолокна
Стекловолокно. Получение стекловолокна Как вести себя с первоклассником
Как вести себя с первоклассником Хакассий эпос и его влияние на формирование правовой культуры народа
Хакассий эпос и его влияние на формирование правовой культуры народа Реформы П. А. Столыпина
Реформы П. А. Столыпина Листая школьные страницы 2009-2010 учебного года
Листая школьные страницы 2009-2010 учебного года Презентация на тему Countryside of Britain (Сельская местность Британии)
Презентация на тему Countryside of Britain (Сельская местность Британии) Размножение и развитие птиц
Размножение и развитие птиц Презентация на тему Весна в мире насекомых
Презентация на тему Весна в мире насекомых Решение задач с помощью системы уравнений
Решение задач с помощью системы уравнений Проведение вечера встречи выпускников
Проведение вечера встречи выпускников Правописание приставок А 6 ГИА
Правописание приставок А 6 ГИА Процесс закупа на примере предприятия
Процесс закупа на примере предприятия Город Владимир
Город Владимир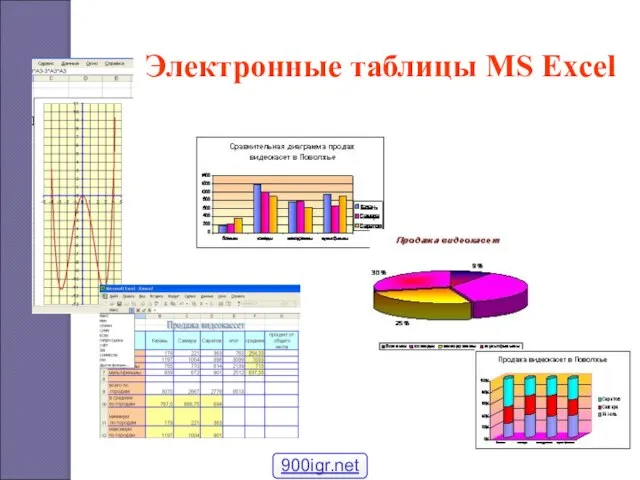 Таблицы Excel ознакомление
Таблицы Excel ознакомление Правильные многоугольники
Правильные многоугольники  Акция «Спешите делать добро детям!»
Акция «Спешите делать добро детям!» УМК Школа России
УМК Школа России Презентация на тему Площадь прямоугольника
Презентация на тему Площадь прямоугольника