- CHAIR OF PEDIATRICTS WITH MEDICAL GENETICS

Содержание
- 2. Anatomy- physiological features of hypophysis Hypophysis is located at the depression of Turkish saddle. At adults
- 3. STH – is the main stimulator of growth. It activates synthesis of ACTH, it assists the
- 4. Gigantism Growth pathology takes the 3rd place in the structure of children’s endocrinal morbidity. Gigantism –
- 5. Gigantism Diagnostics. -Enhancement of STH level (up to 400 ng/ml); -Increase of somatomedin content (N=0,31-1,4 UA/ml).
- 6. Gigantism Differential diagnostics. 2. Syndrome of Morfan – STH level is not increased, typical clinical manifestations,
- 7. Growth inhibition Dwarfism (nanism) – is heterogenic pathology, that accompanies plenty of endocrine, somatic and genetic
- 8. Classification Endocrine- independent variants of growth inhibition – synthesis of STH is not violated. Deficiency of
- 9. Endocrine- dependent variants of growth inhibition Etiology. -destructive changes in hypothalamus or hypophysis, that are caused
- 10. Endocrine- dependent variants of growth inhibition І. Total STH deficiency. 2 variants: Idiopathic: -growth inhibition is
- 11. Endocrine- dependent variants of growth inhibition І. Total STH deficiency. 2. Organic: -organic damage of hypothalamus-
- 12. Endocrine- dependent variants of growth inhibition ІІ. Isolated STH deficiency: -women’s height is less then 125
- 13. Endocrine- dependent variants of growth inhibition ІІ. Isolated STH deficiency. 3 variants: Partial deficiency of growth
- 14. Diagnostic criteria of growth inhibition -proportional growth inhibition, growth temps are not more then 4 sm
- 15. Treatment Nordithropin – in case of subcutaneus injection 0,07-0,1 МО/kg 6-7 times a week or 2-3
- 16. Obesity A complicated chronic violation of lipid exchange, that is accompanied with over fat accumulation (triglycerides)
- 17. Physiology of fat tissue Fat tissue (FT) – is an metabolic- active system, that is controlled
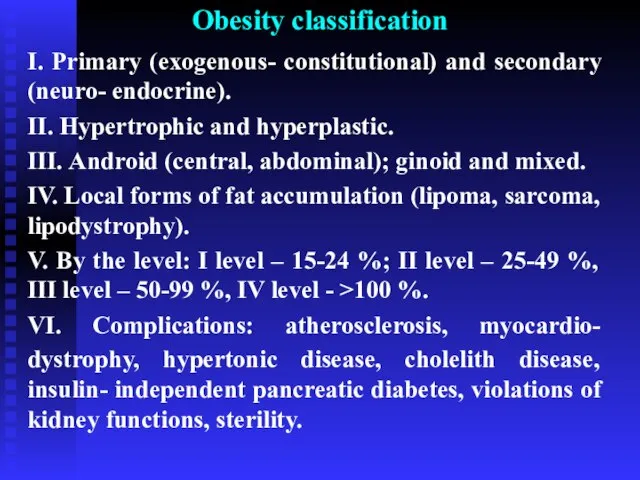
- 18. Obesity classification І. Primary (exogenous- constitutional) and secondary (neuro- endocrine). ІІ. Hypertrophic and hyperplastic. ІІІ. Android
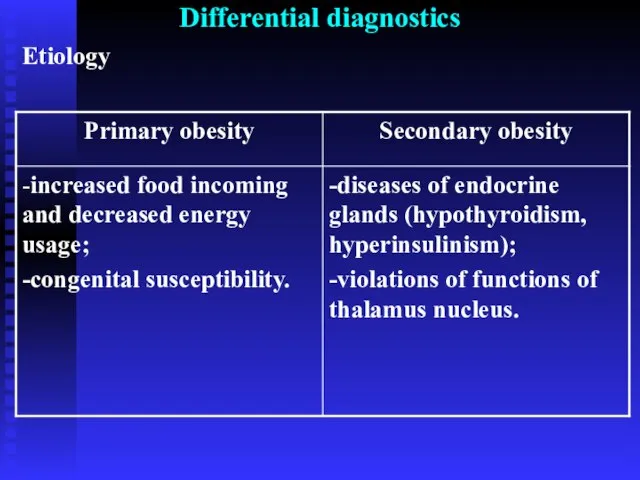
- 19. Differential diagnostics Etiology
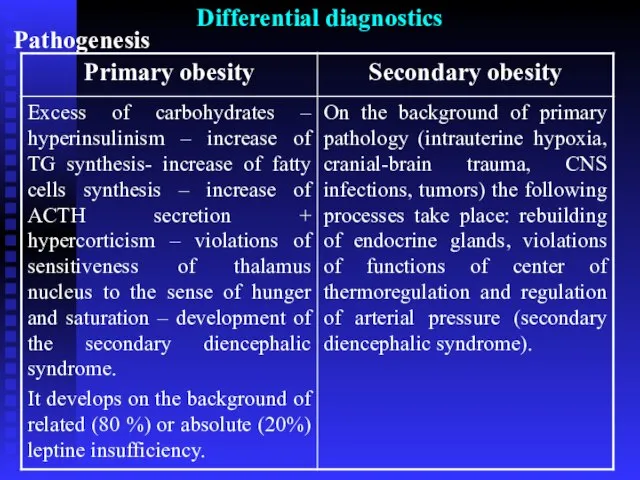
- 20. Differential diagnostics Pathogenesis
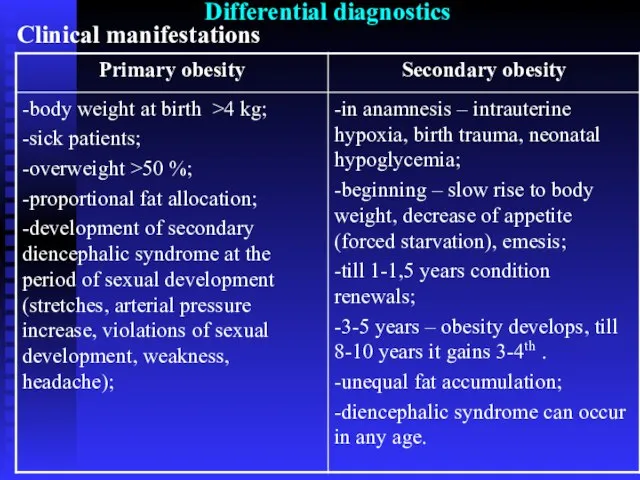
- 21. Differential diagnostics Clinical manifestations
- 22. Diagnostics -anamnesis; -clinical signs; -assess of state of carbohydrates exchange (glucose- tolerant test is necessary); -craniography;
- 23. Treatment Diet- therapy. In case of obesity of the І-ІІ levels calorie content is limited at
- 25. Скачать презентацию
Слайд 2Anatomy- physiological features of hypophysis
Hypophysis is located at the depression of Turkish
Anatomy- physiological features of hypophysis
Hypophysis is located at the depression of Turkish
Слайд 3 STH – is the main stimulator of growth. It activates synthesis of
STH – is the main stimulator of growth. It activates synthesis of
Слайд 4Gigantism
Growth pathology takes the 3rd place in the structure of children’s endocrinal
Gigantism
Growth pathology takes the 3rd place in the structure of children’s endocrinal
Слайд 5Gigantism
Diagnostics.
-Enhancement of STH level (up to 400 ng/ml);
-Increase of somatomedin content (N=0,31-1,4
Gigantism
Diagnostics.
-Enhancement of STH level (up to 400 ng/ml);
-Increase of somatomedin content (N=0,31-1,4
Слайд 6Gigantism
Differential diagnostics.
2. Syndrome of Morfan – STH level is not increased, typical
Gigantism
Differential diagnostics.
2. Syndrome of Morfan – STH level is not increased, typical
Слайд 7Growth inhibition
Dwarfism (nanism) – is heterogenic pathology, that accompanies plenty of endocrine,
Growth inhibition
Dwarfism (nanism) – is heterogenic pathology, that accompanies plenty of endocrine,
Слайд 8Classification
Endocrine- independent variants of growth inhibition – synthesis of STH is not
Classification
Endocrine- independent variants of growth inhibition – synthesis of STH is not
Слайд 9Endocrine- dependent variants of growth inhibition
Etiology.
-destructive changes in hypothalamus or hypophysis,
Endocrine- dependent variants of growth inhibition
Etiology.
-destructive changes in hypothalamus or hypophysis,
Слайд 10Endocrine- dependent variants of growth inhibition
І. Total STH deficiency. 2 variants:
Idiopathic:
-growth inhibition
Endocrine- dependent variants of growth inhibition
І. Total STH deficiency. 2 variants:
Idiopathic:
-growth inhibition
Слайд 11Endocrine- dependent variants of growth inhibition
І. Total STH deficiency.
2. Organic:
-organic damage of
Endocrine- dependent variants of growth inhibition
І. Total STH deficiency.
2. Organic:
-organic damage of
Слайд 12Endocrine- dependent variants of growth inhibition
ІІ. Isolated STH deficiency:
-women’s height is less
Endocrine- dependent variants of growth inhibition
ІІ. Isolated STH deficiency:
-women’s height is less
Слайд 13Endocrine- dependent variants of growth inhibition
ІІ. Isolated STH deficiency. 3 variants:
Partial deficiency
Endocrine- dependent variants of growth inhibition
ІІ. Isolated STH deficiency. 3 variants:
Partial deficiency
Слайд 14Diagnostic criteria of growth inhibition
-proportional growth inhibition, growth temps are not more
Diagnostic criteria of growth inhibition
-proportional growth inhibition, growth temps are not more
Слайд 15Treatment
Nordithropin – in case of subcutaneus injection 0,07-0,1 МО/kg 6-7 times
Treatment
Nordithropin – in case of subcutaneus injection 0,07-0,1 МО/kg 6-7 times
Слайд 16Obesity
A complicated chronic violation of lipid exchange, that is accompanied with
Obesity
A complicated chronic violation of lipid exchange, that is accompanied with
Слайд 17Physiology of fat tissue
Fat tissue (FT) – is an metabolic- active system,
Physiology of fat tissue
Fat tissue (FT) – is an metabolic- active system,
Слайд 18Obesity classification
І. Primary (exogenous- constitutional) and secondary (neuro- endocrine).
ІІ. Hypertrophic and hyperplastic.
ІІІ.
Obesity classification
І. Primary (exogenous- constitutional) and secondary (neuro- endocrine).
ІІ. Hypertrophic and hyperplastic.
ІІІ.
Слайд 19Differential diagnostics
Etiology
Differential diagnostics
Etiology
Слайд 20Differential diagnostics
Pathogenesis
Differential diagnostics
Pathogenesis
Слайд 21Differential diagnostics
Clinical manifestations
Differential diagnostics
Clinical manifestations
Слайд 22Diagnostics
-anamnesis;
-clinical signs;
-assess of state of carbohydrates exchange (glucose- tolerant test is necessary);
Diagnostics
-anamnesis;
-clinical signs;
-assess of state of carbohydrates exchange (glucose- tolerant test is necessary);
Слайд 23Treatment
Diet- therapy. In case of obesity of the І-ІІ levels calorie content
Treatment
Diet- therapy. In case of obesity of the І-ІІ levels calorie content
 Госэкзамены. Письменные контрольные работы
Госэкзамены. Письменные контрольные работы Серебряный век
Серебряный век Кирпичный стиль
Кирпичный стиль Порядок приведения к военной присяге (принесения обязательства)
Порядок приведения к военной присяге (принесения обязательства) Презентация на тему Рациональные уравнения
Презентация на тему Рациональные уравнения Презентация на тему Млечный Путь и другие галактики
Презентация на тему Млечный Путь и другие галактики  Маркетинг преку социјални медиуми
Маркетинг преку социјални медиуми Как превратить рекламу в продажи благодаря CRM
Как превратить рекламу в продажи благодаря CRM Экзаменационное задание по результатам Центра Оценки на позицию директор ОП
Экзаменационное задание по результатам Центра Оценки на позицию директор ОП Структура центрального аппарата акционерного общества КТЖ – Грузовые перевозки
Структура центрального аппарата акционерного общества КТЖ – Грузовые перевозки Презентация на тему Герб и флаг Республики Беларусь
Презентация на тему Герб и флаг Республики Беларусь Вино нового поколения
Вино нового поколения Кандидат_на_должность_председателя_Студенческого_Союза_ФПМИ
Кандидат_на_должность_председателя_Студенческого_Союза_ФПМИ Конференц-зал в Бизнес Центре «РФЦА»
Конференц-зал в Бизнес Центре «РФЦА» Презентация на тему ЛИДЕРЫ, ЭЛИТА и ТОЛПА в политической жизни
Презентация на тему ЛИДЕРЫ, ЭЛИТА и ТОЛПА в политической жизни  Административное право как отрасль права
Административное право как отрасль права Михаил Юрьевич Лермонтов «Бородино»
Михаил Юрьевич Лермонтов «Бородино» Отчет по производственной практике
Отчет по производственной практике Экскурсия в город Правил дорожного движения Подготовила старшая вожатая МОУ СОШ№2 Санкубаева Салтанат Ельтаевна
Экскурсия в город Правил дорожного движения Подготовила старшая вожатая МОУ СОШ№2 Санкубаева Салтанат Ельтаевна Антропогенез 9 класс
Антропогенез 9 класс Основы технологии оклейки стен обоями
Основы технологии оклейки стен обоями Indoor Media
Indoor Media Субкультуры
Субкультуры Проект
Проект Кровоснабжение организма человека.
Кровоснабжение организма человека. Жизнь и борьба за колючей проволокой.
Жизнь и борьба за колючей проволокой. Виктор Михайлович Васнецов
Виктор Михайлович Васнецов Детское экспериментирование как средство развития познавательной активности дошкольников
Детское экспериментирование как средство развития познавательной активности дошкольников