- Common Pediatrics Infectious Diseases

Содержание
- 2. Is a widespread rashIs a widespread rash, usually viralIs a widespread rash, usually viral, and usually
- 3. Exanthema Measles. Rubella. Scarlet fever Chicken pox. Erythema infectiosum. Roseola infantum.
- 4. Historically, exanthems in children have been numbered in the order they were identified: First disease -
- 5. Measles
- 6. Measles Measles, also known as rubeola, is a disease, is a disease caused by a virus,
- 7. Symptoms fever for at least three days, 40° Celsius. Three Cs—coughs—cough, coryzas—cough, coryza (runny nose) conjunctivitis
- 8. DIAGNOSIS A detailed history. vaccination history, contact history, and travel history. Clinical diagnosis of measles requires
- 10. Measles Measles
- 11. TREATMENT No specific therapy for measles . Adequate hydration and antipyretics. Avoid strong light :photophobia. IV
- 12. Complications Otitis media.the most common Interstitial pneumonia. giant cell pneumonia. Activate latent T.B. Myocarditis ,and mesentric
- 13. Prognosis Death due to bronchopneumonia or encephlitis,and subacute scelorosing panencephlitis. Mortality rate is 15%with 20% to
- 14. Prevention & vaccination MMR vaccine first dose 12 to 15 months of age. second dose at
- 15. Rubella German measles Three days measles
- 16. Rubella ( German Measles ) Rubella is also called as 3 day Measles or German Measles.
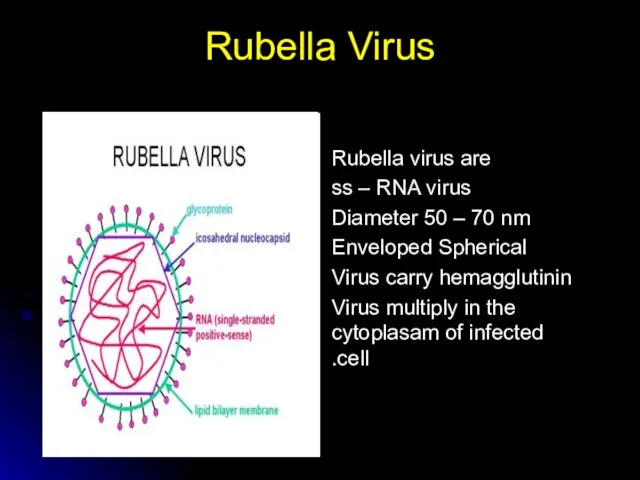
- 17. Rubella Virus Rubella virus are ss – RNA virus Diameter 50 – 70 nm Enveloped Spherical
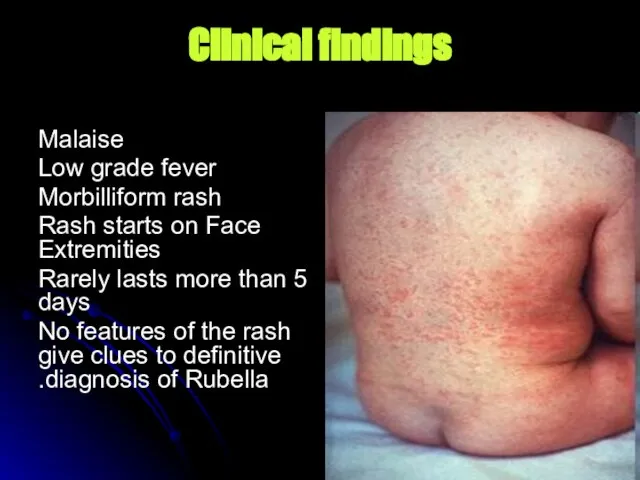
- 18. Clinical findings Malaise Low grade fever Morbilliform rash Rash starts on Face Extremities Rarely lasts more
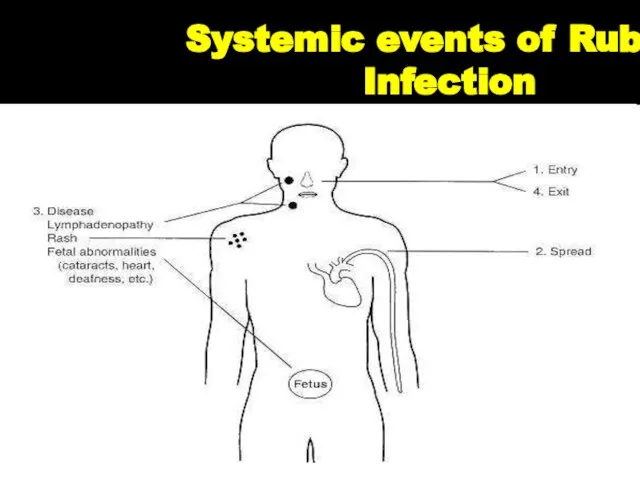
- 19. Systemic events of Rubella Infection
- 20. Adults and children: swollen glands or lymph nodes (may persist for up to a week) fever
- 21. Other manifestations and complications May produce transient Arthritis, in women in particular. Serious complications are Thrombocytopenia
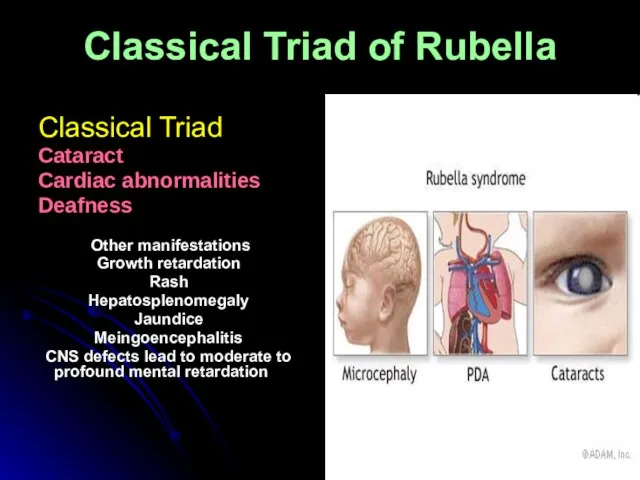
- 22. Classical Triad of Rubella Classical Triad Cataract Cardiac abnormalities Deafness Other manifestations Growth retardation Rash Hepatosplenomegaly
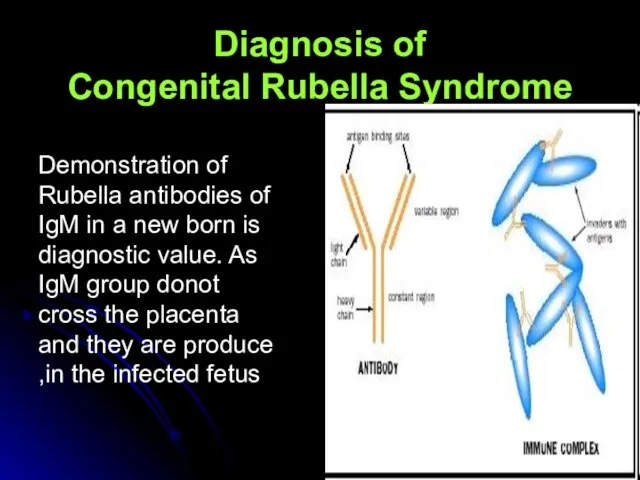
- 23. Diagnosis of Congenital Rubella Syndrome Demonstration of Rubella antibodies of IgM in a new born is
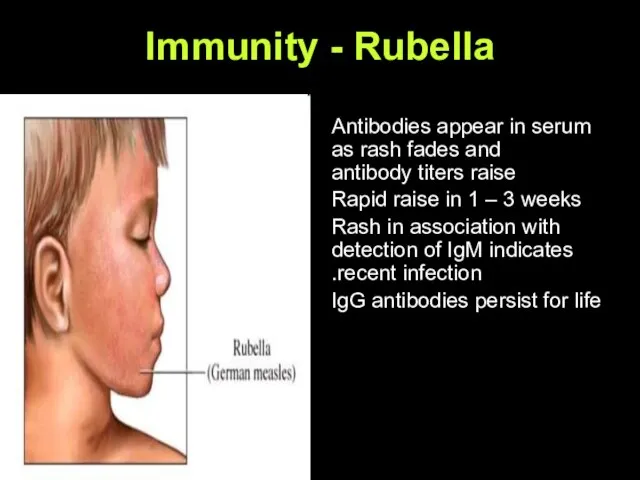
- 24. Immunity - Rubella Antibodies appear in serum as rash fades and antibody titers raise Rapid raise
- 25. Immunity - Protects One attack of Rubella infection, protects for life Immune mothers transfer antibodies to
- 26. Treatment, Prevention, Control No specific treatment is available CRS can be prevented by effective immunization of
- 27. MMR Vaccine The MMR vaccine is a mixture of three live attenuated viruses is a mixture
- 28. Chickenpox-varicella
- 29. Etiology Chickenpox and zoster are caused by varicella -zoster virus . (VZV) ,an enveloped ,double stranded
- 30. Etiology cont… After resolution of chickenpox,the virus persists in latent phase in the dorsal root ganglia
- 31. The Stages of Chickenpox Incubation Period Usually (14-17 days) Prodrome (1 – 3 days) Vesicles Pustules
- 32. Clinical Features Mild prodrome (fever, malaise) for 1-2 days Successive crops (2-4 days) of pruritic vesicles
- 35. NEONATAL CHICKENPOX. Birth within 1 wk before or after the onset of maternal varicella frequently results
- 36. Damage to Sensory Nerves. Cicatricial skin lesions Hypopigmentation.Damage to Optic Stalk and Lens Vesicle.Microphthalmia.Cataracts.Chorioretinitis.optic atrophy.Damage to
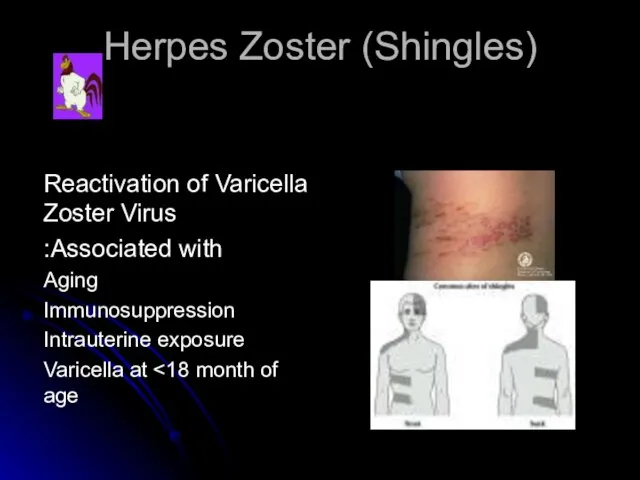
- 38. Herpes Zoster (Shingles) Reactivation of Varicella Zoster Virus Associated with: Aging Immunosuppression Intrauterine exposure Varicella at
- 40. Groups at Increased Risk of Complications Normal Adults Immunocompromised persons Newborns with maternal rash onset within
- 41. Can you get chickenpox more than once? Yes But it is uncommon to do so. For
- 42. What Complications Result From Varicella? The most common complications are: Bacterial infections of the skin and
- 43. What home treatments are available for chickenpox? Fingernails trimmed short Calamine lotion and Aveeno (oatmeal) baths
- 44. Varicella Vaccine Recommendations Routine vaccination at 12 to 18 months of age Recommended for all susceptible
- 45. Zoster Following Vaccination Most cases in children Risk from wild virus 4 to 5 times higher
- 46. Varicella Zoster Immune Globulin (VZIG) May modify or prevent disease if given Indications: Immunocompromised persons Newborn
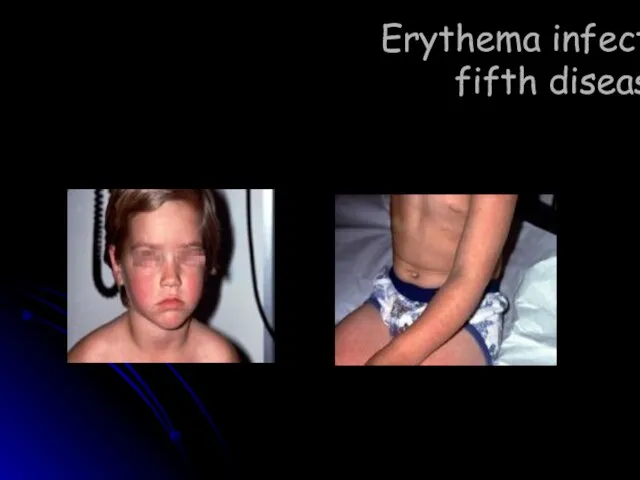
- 47. Erythema infectiosum fifth disease
- 48. Erythema infectiosum fifth disease: Caused by human parvovirus B19. In children between three and 12 years
- 49. Erythema infectiosum
- 50. The incubation period is usually 7-10 days but can be 4-21 days. The mechanism producing the
- 51. Roseola infantum
- 52. Background Roseola infantum is the sixth of the traditional exanthems of childhood. The condition is an
- 53. Causes: HHV-6 was identified as the etiologic agent in 1988. This large, double-stranded (DNA) virus is
- 54. Mortality/Morbidity: Roseola is usually a self-limited illness with no sequelae. The major morbidity associated with roseola
- 55. History: Most cases present within the first 2 years of life, with peak occurrence in infants
- 56. Medication : To date, no controlled antiviral trials exist against HHV-6.. Prevention : Because of the
- 58. Scarlet Fever
- 59. Scarlet fever Is an exotoxinIs an exotoxin-mediated disease caused by Group A streptococcal infectionIs an exotoxin-mediated
- 60. Clinical manifestation Scarlet fever generally has a 1- to 4-days incubation period. Emergence of the illness
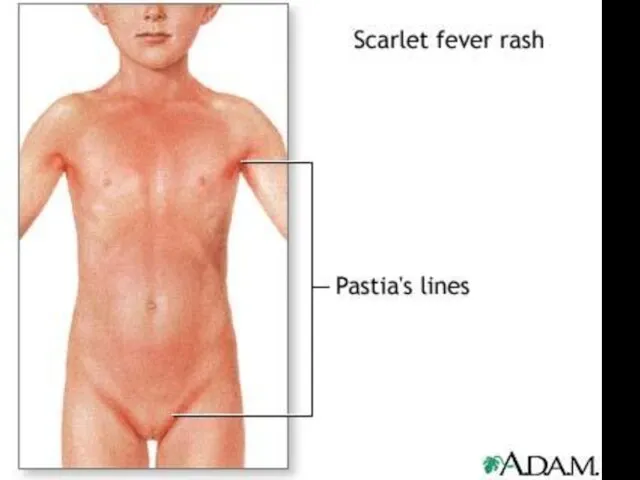
- 61. Skin rash scarlatina generally starts on the chest, axilla , and behind the ears worse in
- 65. Complications arise from suppurative complications such as; *peritonsillar abscess, *sinusitis, *bronchopneumonia, *and meningitis, or problems associated
- 66. Desquamation, one of the most distinctive features of scarlet fever, begins 7-10 days after resolution of
- 68. Lab Studies: 1. Throat culture remains the “gold standard” for confirmation of group A streptococcal upper
- 69. treatment penicillin Pediatric Dose 12 year: Administer as in adults Adult Dose 250 mg PO tid/qid
- 70. TOXIC SHOCK SYNDROME AND SCALDED SKIN SYNDROME Staphylococcus aureus exotoxins responsible for classic toxic shock syndrome
- 73. Coxsackie viruses and other enteroviruses Hand-foot-and-mouth disease: the children develop fever and rash. The rash includes
- 74. Hand-Foot-Mouth Disease Enteroviruses coxsackieviruses A and B echoviruses Vesicular lesions, may be petechial Associated with aseptic
- 76. Infectious Mononucleosis Acute, self limited illness Epstein-Barr virus Oral transmission – incubation 30-50 days Fever, fatigue,
- 77. Impetigo Superficial infection of the dermis Two types: Impetigo contagiosa Bullous impetigo Etiology Group A ß
- 79. Rocky Mountain Spotted Fever Most common rickettsial infection in US Abrupt fever, headache, and myalgia Rash
- 81. Periorbital- Orbital Cellulitis S. aureus, S. pneumoniae, and HIB CBC, blood culture, CT LP? IV antibiotics
- 83. Kawasaki Syndrome Unknown etiology Peak incidence 18-24 months Clinical findings: Fever for at least five days
- 85. Erythema Toxicum Neonatorum Impressive title - harmless skin condition Erythematous macule with a central tiny papule,
- 87. Miliaria Prickly heat, sweat rash Many red macules with central papules, vesicles or pustules are present.
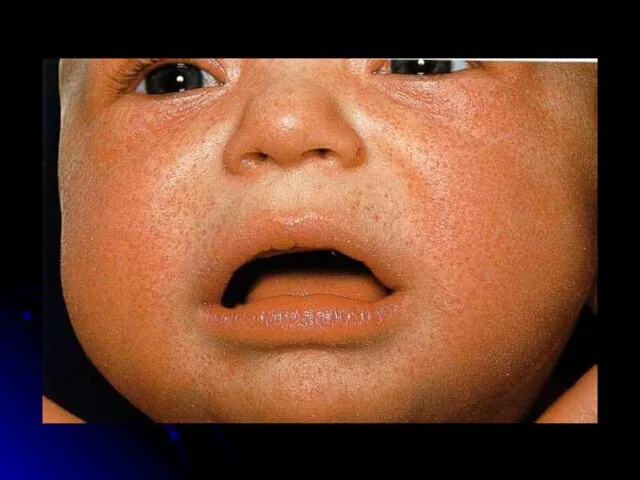
- 89. Infantile Atopic Dermatitis Cause is unknown Red, itchy papules and plaques that ooze and crust Sites
- 91. Eczema- Treatment Avoidance or elimination of predisposing factors Hydration and lubrication of dry skin Anti-pruritic agents
- 92. Seborrheic Dermatitis Common, generally self-limiting Its cause remains ill-understood There is a genetic predisposition Most frequent
- 95. Seborrheic Dermatitis-Treatment Anti-seborrheic shampoo Topical steroids
- 96. Cytomegalovirus (CMV) Most common congenital viral infection ~40,000 infants per year in the U.S. Mild, self
- 97. Clinical Manifestations 90% are asymptomatic at birth! Up to 15% develop symptoms later, notably sensorineural hearing
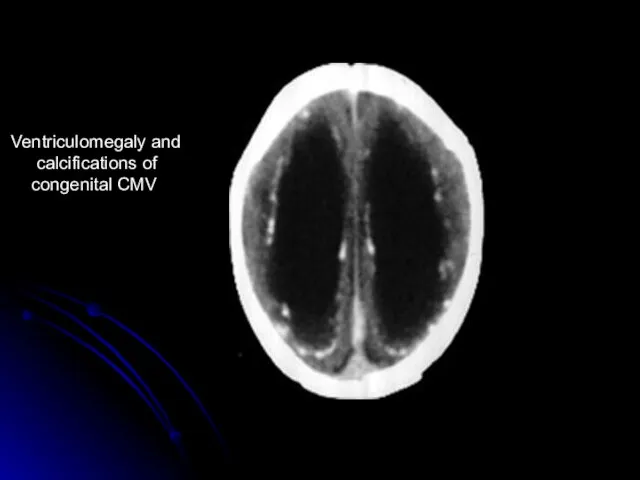
- 98. Ventriculomegaly and calcifications of congenital CMV
- 99. Diagnosis Maternal IgG shows only past infection Infection common – this is useless Viral isolation from
- 101. Скачать презентацию
Слайд 3Exanthema
Measles.
Rubella.
Scarlet fever
Chicken pox.
Erythema infectiosum.
Roseola infantum.
Exanthema
Measles.
Rubella.
Scarlet fever
Chicken pox.
Erythema infectiosum.
Roseola infantum.
Слайд 4Historically, exanthems in children have been numbered in the order they were
Historically, exanthems in children have been numbered in the order they were
Слайд 5Measles
Measles

Слайд 6Measles
Measles, also known as rubeola, is a disease, is a disease caused
Measles
Measles, also known as rubeola, is a disease, is a disease caused
Слайд 7Symptoms
fever for at least three days, 40° Celsius.
Three Cs—coughs—cough, coryzas—cough, coryza
Symptoms
fever for at least three days, 40° Celsius.
Three Cs—coughs—cough, coryzas—cough, coryza
Слайд 8DIAGNOSIS
A detailed history. vaccination history, contact history, and travel history.
Clinical diagnosis of
DIAGNOSIS
A detailed history. vaccination history, contact history, and travel history.
Clinical diagnosis of
Слайд 10Measles
Measles
Measles
Measles

Слайд 11TREATMENT
No specific therapy for measles .
Adequate hydration and antipyretics.
Avoid strong light :photophobia.
IV
TREATMENT
No specific therapy for measles .
Adequate hydration and antipyretics.
Avoid strong light :photophobia.
IV
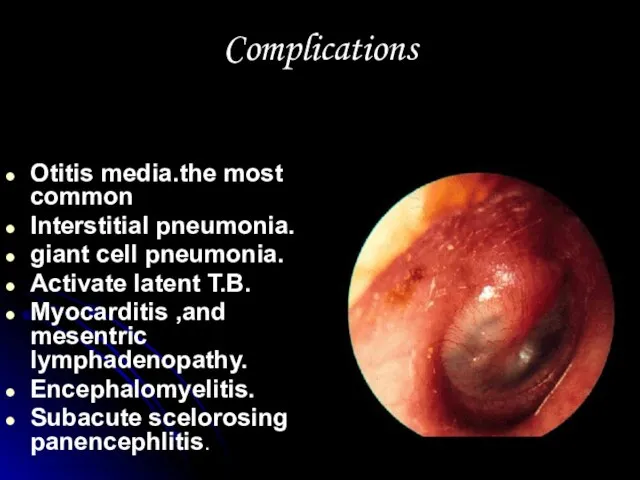
Слайд 12Complications
Otitis media.the most common
Interstitial pneumonia.
giant cell pneumonia.
Activate latent T.B.
Myocarditis ,and mesentric
Complications
Otitis media.the most common
Interstitial pneumonia.
giant cell pneumonia.
Activate latent T.B.
Myocarditis ,and mesentric
Слайд 13Prognosis
Death due to bronchopneumonia or encephlitis,and subacute scelorosing panencephlitis.
Mortality rate is 15%with
Prognosis
Death due to bronchopneumonia or encephlitis,and subacute scelorosing panencephlitis.
Mortality rate is 15%with
Слайд 14Prevention & vaccination
MMR vaccine
first dose 12 to 15 months
Prevention & vaccination
MMR vaccine
first dose 12 to 15 months
Слайд 15Rubella
German measles
Three days measles
Rubella
German measles
Three days measles

Слайд 16Rubella
( German Measles )
Rubella is also called as 3 day Measles or
Rubella
( German Measles )
Rubella is also called as 3 day Measles or
Слайд 17Rubella Virus
Rubella virus are
ss – RNA virus
Diameter 50 – 70
Rubella Virus
Rubella virus are
ss – RNA virus
Diameter 50 – 70
Слайд 18Clinical findings
Malaise
Low grade fever
Morbilliform rash
Rash starts on Face Extremities
Rarely lasts more
Clinical findings
Malaise
Low grade fever
Morbilliform rash
Rash starts on Face Extremities
Rarely lasts more
Слайд 19Systemic events of Rubella Infection
Systemic events of Rubella Infection
Слайд 20Adults and children:
swollen glands or lymph nodes (may persist for up to
Adults and children:
swollen glands or lymph nodes (may persist for up to
Слайд 21Other manifestations and complications
May produce transient Arthritis, in women in particular.
Serious complications
Other manifestations and complications
May produce transient Arthritis, in women in particular.
Serious complications

Слайд 22Classical Triad of Rubella
Classical Triad
Cataract
Cardiac abnormalities
Deafness
Other manifestations
Growth retardation
Classical Triad of Rubella
Classical Triad
Cataract
Cardiac abnormalities
Deafness
Other manifestations
Growth retardation
Слайд 23Diagnosis of
Congenital Rubella Syndrome
Demonstration of Rubella antibodies of IgM in a new
Diagnosis of
Congenital Rubella Syndrome
Demonstration of Rubella antibodies of IgM in a new
Слайд 24Immunity - Rubella
Antibodies appear in serum as rash fades and antibody titers
Immunity - Rubella
Antibodies appear in serum as rash fades and antibody titers
Слайд 25Immunity - Protects
One attack of Rubella infection, protects for life
Immune mothers transfer
Immunity - Protects
One attack of Rubella infection, protects for life
Immune mothers transfer
Слайд 26Treatment, Prevention, Control
No specific treatment is available
CRS can be prevented by effective
Treatment, Prevention, Control
No specific treatment is available
CRS can be prevented by effective
Слайд 27MMR Vaccine
The MMR vaccine is a mixture of three live attenuated viruses
MMR Vaccine
The MMR vaccine is a mixture of three live attenuated viruses
Слайд 28Chickenpox-varicella
Chickenpox-varicella

Слайд 29Etiology
Chickenpox and zoster are caused by varicella -zoster virus .
(VZV) ,an enveloped
Etiology
Chickenpox and zoster are caused by varicella -zoster virus .
(VZV) ,an enveloped
Слайд 30Etiology cont…
After resolution of chickenpox,the virus persists in latent phase in the
Etiology cont…
After resolution of chickenpox,the virus persists in latent phase in the
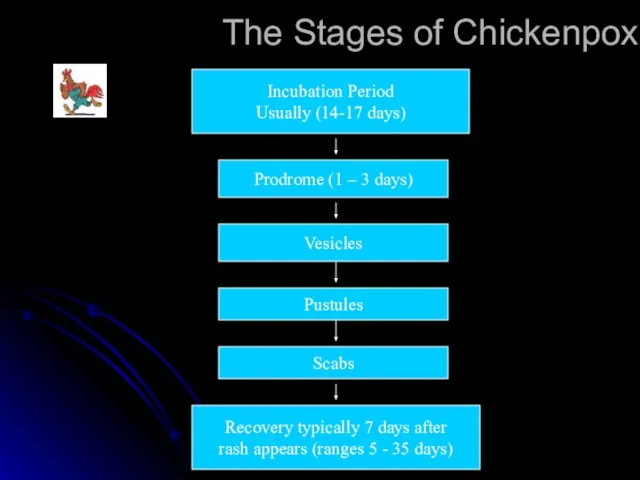
Слайд 31The Stages of Chickenpox
Incubation Period
Usually (14-17 days)
Prodrome (1 – 3 days)
Vesicles
Pustules
The Stages of Chickenpox
Incubation Period
Usually (14-17 days)
Prodrome (1 – 3 days)
Vesicles
Pustules
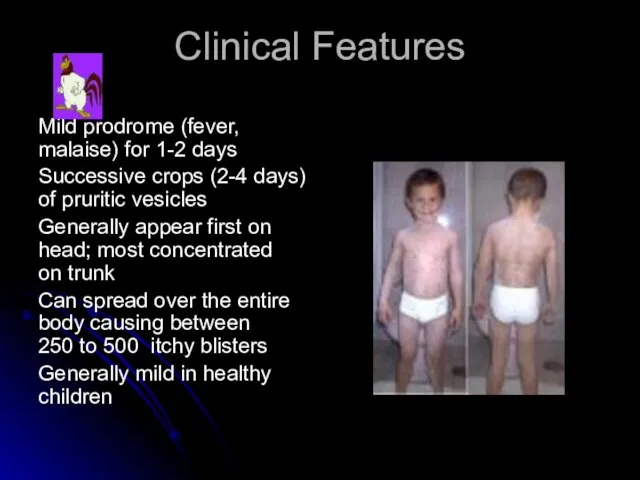
Слайд 32Clinical Features
Mild prodrome (fever, malaise) for 1-2 days
Successive crops (2-4 days) of
Clinical Features
Mild prodrome (fever, malaise) for 1-2 days
Successive crops (2-4 days) of


Слайд 35NEONATAL CHICKENPOX.
Birth within 1 wk before or after the onset of
NEONATAL CHICKENPOX.
Birth within 1 wk before or after the onset of
Слайд 36
Damage to Sensory Nerves. Cicatricial skin lesions
Hypopigmentation.Damage to Optic Stalk and
Damage to Sensory Nerves. Cicatricial skin lesions
Hypopigmentation.Damage to Optic Stalk and

Слайд 38Herpes Zoster (Shingles)
Reactivation of Varicella Zoster Virus
Associated with:
Aging
Immunosuppression
Intrauterine exposure
Varicella at <18
Herpes Zoster (Shingles)
Reactivation of Varicella Zoster Virus
Associated with:
Aging
Immunosuppression
Intrauterine exposure
Varicella at <18

Слайд 40Groups at Increased Risk of Complications
Normal Adults
Immunocompromised persons
Newborns with maternal rash onset
Groups at Increased Risk of Complications
Normal Adults
Immunocompromised persons
Newborns with maternal rash onset
Слайд 41Can you get chickenpox more than once?
Yes
But it is uncommon to
Can you get chickenpox more than once?
Yes
But it is uncommon to
Слайд 42What Complications Result From Varicella?
The most common complications are:
Bacterial infections of
What Complications Result From Varicella?
The most common complications are:
Bacterial infections of

Слайд 43What home treatments are available for chickenpox?
Fingernails trimmed short
Calamine lotion and
What home treatments are available for chickenpox?
Fingernails trimmed short
Calamine lotion and
Слайд 44Varicella Vaccine Recommendations
Routine vaccination at 12 to 18 months of age
Recommended for
Varicella Vaccine Recommendations
Routine vaccination at 12 to 18 months of age
Recommended for
Слайд 45Zoster Following Vaccination
Most cases in children
Risk from wild virus 4 to 5
Zoster Following Vaccination
Most cases in children
Risk from wild virus 4 to 5
Слайд 46Varicella Zoster Immune Globulin (VZIG)
May modify or prevent disease if given <96
Varicella Zoster Immune Globulin (VZIG)
May modify or prevent disease if given <96
Слайд 47Erythema infectiosum
fifth disease
Erythema infectiosum
fifth disease
Слайд 48Erythema infectiosum fifth disease:
Caused by human parvovirus B19.
In children between
Erythema infectiosum fifth disease:
Caused by human parvovirus B19.
In children between
Слайд 49Erythema infectiosum
Erythema infectiosum

Слайд 50The incubation period is usually 7-10 days but can be 4-21 days.
The incubation period is usually 7-10 days but can be 4-21 days.
Слайд 51Roseola infantum
Roseola infantum

Слайд 52Background
Roseola infantum is the sixth of the traditional exanthems of childhood.
Background
Roseola infantum is the sixth of the traditional exanthems of childhood.
Слайд 53Causes:
HHV-6 was identified as the etiologic agent in 1988.
This large, double-stranded (DNA)
Causes:
HHV-6 was identified as the etiologic agent in 1988.
This large, double-stranded (DNA)
Слайд 54Mortality/Morbidity:
Roseola is usually a self-limited illness with no sequelae.
The major morbidity
Mortality/Morbidity:
Roseola is usually a self-limited illness with no sequelae.
The major morbidity
Слайд 55History:
Most cases present within the first 2 years of life, with peak
History:
Most cases present within the first 2 years of life, with peak
Слайд 56 Medication :
To date, no controlled antiviral trials exist against HHV-6..
Prevention :
Medication :
To date, no controlled antiviral trials exist against HHV-6..
Prevention :

Слайд 58Scarlet Fever
Scarlet Fever

Слайд 59Scarlet fever
Is an exotoxinIs an exotoxin-mediated disease caused by Group A streptococcal
Scarlet fever
Is an exotoxinIs an exotoxin-mediated disease caused by Group A streptococcal
Слайд 60Clinical manifestation
Scarlet fever generally has a 1- to 4-days incubation period.
Emergence of
Clinical manifestation
Scarlet fever generally has a 1- to 4-days incubation period.
Emergence of
Слайд 61Skin rash scarlatina
generally starts on the chest, axilla , and behind the
Skin rash scarlatina
generally starts on the chest, axilla , and behind the


Слайд 65Complications
arise from suppurative complications such as;
*peritonsillar abscess,
*sinusitis,
*bronchopneumonia,
*and meningitis,
Complications
arise from suppurative complications such as;
*peritonsillar abscess,
*sinusitis,
*bronchopneumonia,
*and meningitis,
Слайд 66Desquamation, one of the most distinctive features of scarlet fever, begins 7-10
Desquamation, one of the most distinctive features of scarlet fever, begins 7-10

Слайд 68Lab Studies:
1. Throat culture remains the “gold standard” for confirmation of
Lab Studies:
1. Throat culture remains the “gold standard” for confirmation of
Слайд 69treatment
penicillin
Pediatric Dose
<12 year: 25-50 mg/kg/d PO divided tid/qid; not to exceed 3
treatment
penicillin
Pediatric Dose
<12 year: 25-50 mg/kg/d PO divided tid/qid; not to exceed 3
Слайд 70TOXIC SHOCK SYNDROME AND SCALDED SKIN SYNDROME
Staphylococcus aureus exotoxins responsible for classic
TOXIC SHOCK SYNDROME AND SCALDED SKIN SYNDROME
Staphylococcus aureus exotoxins responsible for classic


Слайд 73Coxsackie viruses and other enteroviruses
Hand-foot-and-mouth disease: the children develop fever and
Coxsackie viruses and other enteroviruses
Hand-foot-and-mouth disease: the children develop fever and
Слайд 74Hand-Foot-Mouth Disease
Enteroviruses
coxsackieviruses A and B
echoviruses
Vesicular lesions, may be petechial
Associated with aseptic
Hand-Foot-Mouth Disease
Enteroviruses
coxsackieviruses A and B
echoviruses
Vesicular lesions, may be petechial
Associated with aseptic

Слайд 76Infectious Mononucleosis
Acute, self limited illness
Epstein-Barr virus
Oral transmission – incubation 30-50 days
Fever, fatigue,
Infectious Mononucleosis
Acute, self limited illness
Epstein-Barr virus
Oral transmission – incubation 30-50 days
Fever, fatigue,
Слайд 77Impetigo
Superficial infection of the dermis
Two types:
Impetigo contagiosa
Bullous impetigo
Etiology
Group A ß hemolytic
Impetigo
Superficial infection of the dermis
Two types:
Impetigo contagiosa
Bullous impetigo
Etiology
Group A ß hemolytic


Слайд 79Rocky Mountain Spotted Fever
Most common rickettsial infection in US
Abrupt fever, headache, and
Rocky Mountain Spotted Fever
Most common rickettsial infection in US
Abrupt fever, headache, and

Слайд 81Periorbital- Orbital Cellulitis
S. aureus, S. pneumoniae, and HIB
CBC, blood culture, CT
LP?
IV
Periorbital- Orbital Cellulitis
S. aureus, S. pneumoniae, and HIB
CBC, blood culture, CT
LP?
IV

Слайд 83Kawasaki Syndrome
Unknown etiology
Peak incidence 18-24 months
Clinical findings:
Fever for at least five days
Conjunctivitis
Polymorphous
Kawasaki Syndrome
Unknown etiology
Peak incidence 18-24 months
Clinical findings:
Fever for at least five days
Conjunctivitis
Polymorphous

Слайд 85Erythema Toxicum Neonatorum
Impressive title - harmless skin condition
Erythematous macule with a central
Erythema Toxicum Neonatorum
Impressive title - harmless skin condition
Erythematous macule with a central

Слайд 87Miliaria
Prickly heat, sweat rash
Many red macules with central papules, vesicles or
Miliaria
Prickly heat, sweat rash
Many red macules with central papules, vesicles or
Слайд 89Infantile Atopic Dermatitis
Cause is unknown
Red, itchy papules and plaques that ooze and
Infantile Atopic Dermatitis
Cause is unknown
Red, itchy papules and plaques that ooze and

Слайд 91Eczema- Treatment
Avoidance or elimination of predisposing factors
Hydration and lubrication of dry skin
Anti-pruritic
Eczema- Treatment
Avoidance or elimination of predisposing factors
Hydration and lubrication of dry skin
Anti-pruritic
Слайд 92Seborrheic Dermatitis
Common, generally self-limiting
Its cause remains ill-understood
There is a genetic predisposition
Most
Seborrheic Dermatitis
Common, generally self-limiting
Its cause remains ill-understood
There is a genetic predisposition
Most


Слайд 95Seborrheic Dermatitis-Treatment
Anti-seborrheic shampoo
Topical steroids
Seborrheic Dermatitis-Treatment
Anti-seborrheic shampoo
Topical steroids
Слайд 96Cytomegalovirus (CMV)
Most common congenital viral infection
~40,000 infants per year in the U.S.
Mild,
Cytomegalovirus (CMV)
Most common congenital viral infection
~40,000 infants per year in the U.S.
Mild,
Слайд 97Clinical Manifestations
90% are asymptomatic at birth!
Up to 15% develop symptoms later, notably
Clinical Manifestations
90% are asymptomatic at birth!
Up to 15% develop symptoms later, notably
Слайд 98Ventriculomegaly and calcifications of congenital CMV
Ventriculomegaly and calcifications of congenital CMV
Слайд 99Diagnosis
Maternal IgG shows only past infection
Infection common – this is useless
Viral isolation
Diagnosis
Maternal IgG shows only past infection
Infection common – this is useless
Viral isolation
 Название проекта:
Название проекта: Техника выполнения прыжка через короткую скакалку
Техника выполнения прыжка через короткую скакалку Песочное рисование
Песочное рисование Безопасность в сети Интернет
Безопасность в сети Интернет Как помочь ребенку готовить домашнее задание
Как помочь ребенку готовить домашнее задание Культурология. Типология культурной деятельности людей
Культурология. Типология культурной деятельности людей zagadki-ctvetov
zagadki-ctvetov 26.09.22 Фізичне тіло. Матеріал. Речовина. Молекула. Атом
26.09.22 Фізичне тіло. Матеріал. Речовина. Молекула. Атом Бычкова Карина , ученица 9 класса МБОУ Троснянской СОШ
Бычкова Карина , ученица 9 класса МБОУ Троснянской СОШ Презентация на тему США в период монополистического капитализма
Презентация на тему США в период монополистического капитализма Формирование УУД на уроках физической культуры в 5-ых классах при введении ФГОС
Формирование УУД на уроках физической культуры в 5-ых классах при введении ФГОС Салон магазин Интерьер
Салон магазин Интерьер Openstat – универсальная метка
Openstat – универсальная метка Особенности эксплуатации скважин на форсированных режимах работы. Особенности эксплуатации малодебитных скважин
Особенности эксплуатации скважин на форсированных режимах работы. Особенности эксплуатации малодебитных скважин Воскресная школа Наши родители помогают нам учиться. Класс Выбирай истину (4-7 лет)
Воскресная школа Наши родители помогают нам учиться. Класс Выбирай истину (4-7 лет) Деятельность в социально-гуманитарной сфере
Деятельность в социально-гуманитарной сфере Роль знаков препинания в письменной речи
Роль знаков препинания в письменной речи Использование ИКТ в начальной школе. Работа с одаренными детьми
Использование ИКТ в начальной школе. Работа с одаренными детьми Факультет иностранных языков
Факультет иностранных языков ВКР: Управление ценовой политикой предприятия
ВКР: Управление ценовой политикой предприятия Organizatsia
Organizatsia Рисуем яхту
Рисуем яхту Игровые технологии как условие повышения эффективности процесса физического воспитания школьников
Игровые технологии как условие повышения эффективности процесса физического воспитания школьников Всегда ли правы мы- родители?
Всегда ли правы мы- родители? Принцесса Уникитти
Принцесса Уникитти Божья верность
Божья верность 20140110_rekreatsionnye_resursy_kamchatki
20140110_rekreatsionnye_resursy_kamchatki Построение чертежа выкройки
Построение чертежа выкройки