- DISORDERS OF THE PARATHYROID GLANDS

Содержание
- 2. Disorders of the Parathyroid Glands Maintenance of calcium, phosphate and magnesium homeostasis is under the influence
- 3. Disorders of the Parathyroid Glands These hormones regulate the flow of minerals in and out of
- 4. Disorders of the Parathyroid Glands The PTH acts directly on the bones and kidneys and indirectly
- 5. Disorders of the Parathyroid Glands Calcitonin is released by the “C” cells (parafollicular cells in the
- 6. Disorders of the Parathyroid Glands Calcitonin is therefore the physiological antagonist of PTH. The two hormones
- 8. Disorders of the Parathyroid Function Primary hyperparathyroidismis due to excessive production of PTH by one or
- 9. Disorders of the Parathyroid Function The cause of primary hyperparathyroidism is unknown. A genetic factor may
- 10. Disorders of the Parathyroid Function The incidence of the disease increases dramatically after the age of
- 11. Disorders of the Parathyroid Function The two major sites of potential complications are the bones and
- 12. Disorders of the Parathyroid Function In skeleton a condition called osteitis fibrosa cystica could occur with
- 13. Disorders of the Parathyroid Function Now a days almost 90% of diagnosed cases in the developed
- 14. Disorders of the Parathyroid Function Other symptoms include muscle weakness, easy fatigability, peptic ulcer disease, pancreatitis,
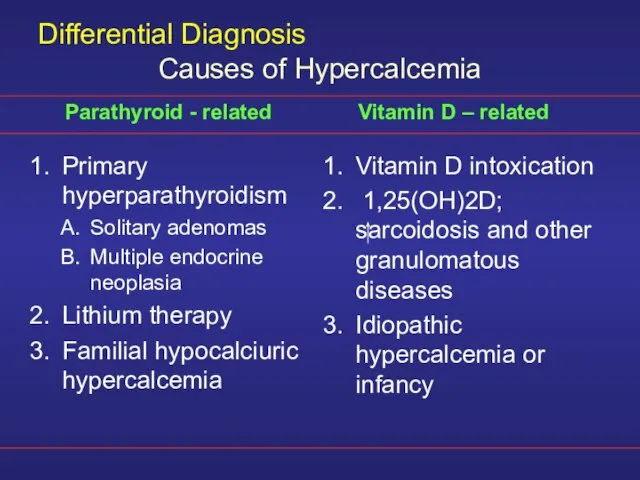
- 15. Differential Diagnosis Primary hyperparathyroidism Solitary adenomas Multiple endocrine neoplasia Lithium therapy Familial hypocalciuric hypercalcemia Vitamin D
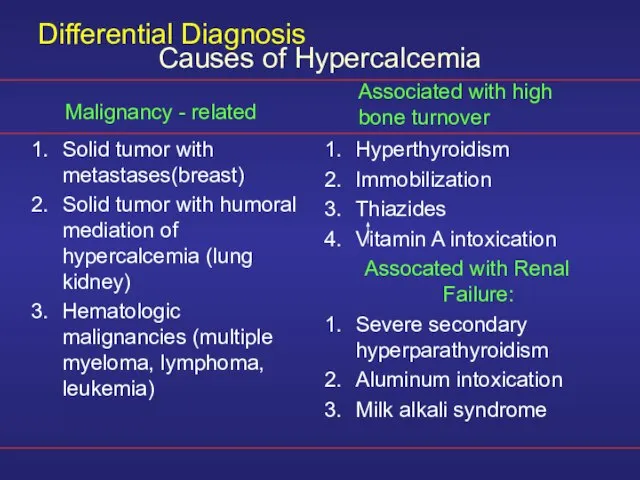
- 16. Differential Diagnosis Solid tumor with metastases(breast) Solid tumor with humoral mediation of hypercalcemia (lung kidney) Hematologic
- 17. Diagnosis The presence of established hypercalcaemia in more than one serum measurement accompanied by elevated immunoreactive
- 18. Diagnosis Serum phosphate is usually low but may be normal. Hypercalcaemia is common and blood alkaline
- 19. Other Diagnostic tests The heypercalcaemic of non-parathyroid origin e.g., vitamin D intoxication, sarcoidosis and lymphoproliferative syndromes
- 20. Other Diagnostic tests The response is unusual in hypercalcaemia secondary to primary hyperparathyroidism and ectopic PTH
- 21. Other Diagnostic tests Plain X-ray of hands can be diagnostic showing subperiosteal bone resorption usually on
- 22. Other Diagnostic tests Ultrasonography MRI CT Thallium 201 – Tehcnichum99m scan (subtraction study) Pre-operative localization of
- 23. Treatment A large proportion of patients have “biochemical” hyperparathyroidism but with prolonged follow up they progress
- 24. Medical Treatment of the hypercalcaemia In acute severe forms the main stay of therapy is adequate
- 25. Other agents Glucocostiroids In hypercalcaemia associated the hematological malignant neoplasms Mythramycin A toxic antibiotics which inhibit
- 26. Other agents Calcitonin Also inhibit osteoclast activity and prevent bone resorption Bisphosphonates They are given intravenously
- 27. Other agents Phosphate Oral phosphate can be used as an antihypercalcaemic agent and is commonly used
- 28. Surgery Surgical treatment should be considered in all cases with established diagnosis of primary hyperparthyroidism. During
- 29. Other Complications Deterioration of renal function Metabolic disturbance e.g. hypomagnesia, pancreatitis, gout or pseudogout
- 30. Secondary hyperparathyroidism An increase in PTH secretion which is adaptive and unrelated to intrinsic disease of
- 31. Major causes of chronic hypocalcemia other than hypoparathyroidism Dietary deficiency of vitamin D or calcium Decreased
- 32. Major causes of chronic hypocalcemia other than parathyroprival hypoparathyroidism States of tissue resistance to vitamin D
- 33. Hypoparathyroidism Deficient secretion of PTH which manifests itself biochemically by hypocalcemia, hyperphospatemia diminished or absent circulating
- 34. Hypoparathyroidism Surgical hypoparathyroidism – the commonest After anterior neck exploration for thyroidectomy, abnormal parathyroid gland removal,
- 35. Hypoparathyroidism Idiopathic hypoparathyroidism A form occuring at an early age (genetic origin) with autosomal recessive mode
- 36. Hypoparathyroidism Idiopathic hypoparathyroidism Circulating antibodies for the parathyroid glands and the adrenals are frequently present. Other
- 37. Hypoparathyroidism Idiopathic hypoparathyroidism The late onset form occurs sporadically without circulating grandular autoantibodies. Functional hypoparathyroidism In
- 38. Hypoparathyroidism Neuromuscular The rate of decrease in serum calcium is the major determinant for the development
- 39. Hypoparathyroidism Neuromuscular Parathesia Tetany Hyperventilation Adrenergic symptoms Convulsion (More common in young people and it can
- 40. Hypoparathyroidism Other clinical manifestation Posterio lenticular cataract Cardiac manifestation: Prolonged QT interval in the ECG Resistance
- 41. Hypoparathyroidism Other clinical manifestation Dental Manifestation Abnormal enamel formation with delayed or absent dental eruption and
- 42. Hypoparathyroidism In the absence of renal failure the presence of hypocalcaemia with hyperphosphataemia is virtually diagnostic
- 43. Hypoparathyroidism The mainstay of treatment is a combination of oral calcium with pharmacological doses of vitamin
- 44. Emergency Treatment for Hypocalcaemic Calcium should be given parenterally till adequate serum calcium level is obtained
- 45. Emergency Treatment for Hypocalcaemic In patients with hyperparathyroidism and severe bone disease who undergo successful parathyroidectomy
- 46. Pseudohypoparathysoidism and Pseudopseudohypoparathyroidism A rare familial disorders with target tissue resistance to PTH. There is hypocalcaemia,
- 48. Скачать презентацию
Слайд 2Disorders of the Parathyroid Glands
Maintenance of calcium, phosphate and magnesium homeostasis is
Disorders of the Parathyroid Glands
Maintenance of calcium, phosphate and magnesium homeostasis is
Слайд 3Disorders of the Parathyroid Glands
These hormones regulate the flow of minerals in
Disorders of the Parathyroid Glands
These hormones regulate the flow of minerals in
Слайд 4Disorders of the Parathyroid Glands
The PTH acts directly on the bones and
Disorders of the Parathyroid Glands
The PTH acts directly on the bones and
Слайд 5Disorders of the Parathyroid Glands
Calcitonin is released by the “C” cells (parafollicular
Disorders of the Parathyroid Glands
Calcitonin is released by the “C” cells (parafollicular
Слайд 6Disorders of the Parathyroid Glands
Calcitonin is therefore the physiological antagonist of PTH.
Disorders of the Parathyroid Glands
Calcitonin is therefore the physiological antagonist of PTH.
Слайд 8Disorders of the Parathyroid Function
Primary hyperparathyroidismis due to excessive production of PTH
Disorders of the Parathyroid Function
Primary hyperparathyroidismis due to excessive production of PTH
Слайд 9Disorders of the Parathyroid Function
The cause of primary hyperparathyroidism is unknown. A
Disorders of the Parathyroid Function
The cause of primary hyperparathyroidism is unknown. A
Слайд 10Disorders of the Parathyroid Function
The incidence of the disease increases dramatically after
Disorders of the Parathyroid Function
The incidence of the disease increases dramatically after
Слайд 11Disorders of the Parathyroid Function
The two major sites of potential complications are
Disorders of the Parathyroid Function
The two major sites of potential complications are
Слайд 12Disorders of the Parathyroid Function
In skeleton a condition called osteitis fibrosa cystica
Disorders of the Parathyroid Function
In skeleton a condition called osteitis fibrosa cystica
Слайд 13Disorders of the Parathyroid Function
Now a days almost 90% of diagnosed cases
Disorders of the Parathyroid Function
Now a days almost 90% of diagnosed cases
Слайд 14Disorders of the Parathyroid Function
Other symptoms include muscle weakness, easy fatigability, peptic
Disorders of the Parathyroid Function
Other symptoms include muscle weakness, easy fatigability, peptic
Слайд 15Differential Diagnosis
Primary hyperparathyroidism
Solitary adenomas
Multiple endocrine neoplasia
Lithium therapy
Familial hypocalciuric hypercalcemia
Vitamin D intoxication
1,25(OH)2D;
Differential Diagnosis
Primary hyperparathyroidism
Solitary adenomas
Multiple endocrine neoplasia
Lithium therapy
Familial hypocalciuric hypercalcemia
Vitamin D intoxication
1,25(OH)2D;
Слайд 16Differential Diagnosis
Solid tumor with metastases(breast)
Solid tumor with humoral mediation of hypercalcemia (lung
Differential Diagnosis
Solid tumor with metastases(breast)
Solid tumor with humoral mediation of hypercalcemia (lung
Слайд 17Diagnosis
The presence of established hypercalcaemia in more than one serum measurement accompanied
Diagnosis
The presence of established hypercalcaemia in more than one serum measurement accompanied
Слайд 18Diagnosis
Serum phosphate is usually low but may be normal. Hypercalcaemia is common
Diagnosis
Serum phosphate is usually low but may be normal. Hypercalcaemia is common
Слайд 19Other Diagnostic tests
The heypercalcaemic of non-parathyroid origin e.g., vitamin D intoxication, sarcoidosis
Other Diagnostic tests
The heypercalcaemic of non-parathyroid origin e.g., vitamin D intoxication, sarcoidosis
Слайд 20Other Diagnostic tests
The response is unusual in hypercalcaemia secondary to primary hyperparathyroidism
Other Diagnostic tests
The response is unusual in hypercalcaemia secondary to primary hyperparathyroidism
Слайд 21Other Diagnostic tests
Plain X-ray of hands can be diagnostic showing subperiosteal bone
Other Diagnostic tests
Plain X-ray of hands can be diagnostic showing subperiosteal bone
Слайд 22Other Diagnostic tests
Ultrasonography
MRI
CT
Thallium 201 – Tehcnichum99m scan (subtraction study)
Pre-operative localization of the
Other Diagnostic tests
Ultrasonography
MRI
CT
Thallium 201 – Tehcnichum99m scan (subtraction study)
Pre-operative localization of the
Слайд 23Treatment
A large proportion of patients have “biochemical” hyperparathyroidism but with prolonged follow
Treatment
A large proportion of patients have “biochemical” hyperparathyroidism but with prolonged follow
Слайд 24Medical Treatment of the hypercalcaemia
In acute severe forms the main stay of
Medical Treatment of the hypercalcaemia
In acute severe forms the main stay of
Слайд 25Other agents
Glucocostiroids
In hypercalcaemia associated the hematological malignant neoplasms
Mythramycin
A toxic antibiotics which inhibit
Other agents
Glucocostiroids
In hypercalcaemia associated the hematological malignant neoplasms
Mythramycin
A toxic antibiotics which inhibit
Слайд 26Other agents
Calcitonin
Also inhibit osteoclast activity and prevent bone resorption
Bisphosphonates
They are given intravenously
Other agents
Calcitonin
Also inhibit osteoclast activity and prevent bone resorption
Bisphosphonates
They are given intravenously
Слайд 27Other agents
Phosphate
Oral phosphate can be used as an antihypercalcaemic agent and is
Other agents
Phosphate
Oral phosphate can be used as an antihypercalcaemic agent and is
Слайд 28Surgery
Surgical treatment should be considered in all cases with established diagnosis of
Surgery
Surgical treatment should be considered in all cases with established diagnosis of
Слайд 29Other Complications
Deterioration of renal function
Metabolic disturbance e.g. hypomagnesia, pancreatitis, gout or pseudogout
Other Complications
Deterioration of renal function
Metabolic disturbance e.g. hypomagnesia, pancreatitis, gout or pseudogout
Слайд 30Secondary hyperparathyroidism
An increase in PTH secretion which is adaptive and unrelated to
Secondary hyperparathyroidism
An increase in PTH secretion which is adaptive and unrelated to
Слайд 31Major causes of chronic hypocalcemia other than hypoparathyroidism
Dietary deficiency of vitamin D
Major causes of chronic hypocalcemia other than hypoparathyroidism
Dietary deficiency of vitamin D
Слайд 32Major causes of chronic hypocalcemia other than parathyroprival hypoparathyroidism
States of tissue resistance
Major causes of chronic hypocalcemia other than parathyroprival hypoparathyroidism
States of tissue resistance
Слайд 33Hypoparathyroidism
Deficient secretion of PTH which manifests itself biochemically by hypocalcemia, hyperphospatemia diminished
Hypoparathyroidism
Deficient secretion of PTH which manifests itself biochemically by hypocalcemia, hyperphospatemia diminished
Слайд 34Hypoparathyroidism
Surgical hypoparathyroidism – the commonest
After anterior neck exploration for thyroidectomy, abnormal parathyroid
Hypoparathyroidism
Surgical hypoparathyroidism – the commonest
After anterior neck exploration for thyroidectomy, abnormal parathyroid
Слайд 35Hypoparathyroidism
Idiopathic hypoparathyroidism
A form occuring at an early age (genetic origin) with autosomal
Hypoparathyroidism
Idiopathic hypoparathyroidism
A form occuring at an early age (genetic origin) with autosomal
Слайд 36Hypoparathyroidism
Idiopathic hypoparathyroidism
Circulating antibodies for the parathyroid glands and the adrenals are frequently
Hypoparathyroidism
Idiopathic hypoparathyroidism
Circulating antibodies for the parathyroid glands and the adrenals are frequently
Слайд 37Hypoparathyroidism
Idiopathic hypoparathyroidism
The late onset form occurs sporadically without circulating grandular autoantibodies.
Functional hypoparathyroidism
In
Hypoparathyroidism
Idiopathic hypoparathyroidism
The late onset form occurs sporadically without circulating grandular autoantibodies.
Functional hypoparathyroidism
In
Слайд 38Hypoparathyroidism
Neuromuscular
The rate of decrease in serum calcium is the major determinant for
Hypoparathyroidism
Neuromuscular
The rate of decrease in serum calcium is the major determinant for
Слайд 39Hypoparathyroidism
Neuromuscular
Parathesia
Tetany
Hyperventilation
Adrenergic symptoms
Convulsion (More common in young people and it can take the
Hypoparathyroidism
Neuromuscular
Parathesia
Tetany
Hyperventilation
Adrenergic symptoms
Convulsion (More common in young people and it can take the
Слайд 40Hypoparathyroidism
Other clinical manifestation
Posterio lenticular cataract
Cardiac manifestation:
Prolonged QT interval in the ECG
Resistance to
Hypoparathyroidism
Other clinical manifestation
Posterio lenticular cataract
Cardiac manifestation:
Prolonged QT interval in the ECG
Resistance to
Слайд 41Hypoparathyroidism
Other clinical manifestation
Dental Manifestation
Abnormal enamel formation with delayed or absent dental eruption
Hypoparathyroidism
Other clinical manifestation
Dental Manifestation
Abnormal enamel formation with delayed or absent dental eruption
Слайд 42Hypoparathyroidism
In the absence of renal failure the presence of hypocalcaemia with hyperphosphataemia
Hypoparathyroidism
In the absence of renal failure the presence of hypocalcaemia with hyperphosphataemia
Слайд 43Hypoparathyroidism
The mainstay of treatment is a combination of oral calcium with pharmacological
Hypoparathyroidism
The mainstay of treatment is a combination of oral calcium with pharmacological
Слайд 44Emergency Treatment for Hypocalcaemic
Calcium should be given parenterally till adequate serum calcium
Emergency Treatment for Hypocalcaemic
Calcium should be given parenterally till adequate serum calcium
Слайд 45Emergency Treatment for Hypocalcaemic
In patients with hyperparathyroidism and severe bone disease who
Emergency Treatment for Hypocalcaemic
In patients with hyperparathyroidism and severe bone disease who
Слайд 46Pseudohypoparathysoidism and Pseudopseudohypoparathyroidism
A rare familial disorders with target tissue resistance to PTH.
Pseudohypoparathysoidism and Pseudopseudohypoparathyroidism
A rare familial disorders with target tissue resistance to PTH.
 Экономика семьи Д/З: § 18, читать
Экономика семьи Д/З: § 18, читать Презентация на тему Синтаксическая синонимия. Открытый урок
Презентация на тему Синтаксическая синонимия. Открытый урок Kazaerostat. Your dreams are real
Kazaerostat. Your dreams are real Анализ методической работы
Анализ методической работы Гигиена девочки. Уход за кожей
Гигиена девочки. Уход за кожей Тренажер лексики
Тренажер лексики Планирование развёртывания полевого магистрального трубопровода
Планирование развёртывания полевого магистрального трубопровода Команда СШОР Русичи г. Орла: ФК Орел – 2008. Для спонсоров и партнеров
Команда СШОР Русичи г. Орла: ФК Орел – 2008. Для спонсоров и партнеров Мониторинг ТВСостояние проектов
Мониторинг ТВСостояние проектов Ochrona pracownikow placowek dyplomatycznych i konsularnych
Ochrona pracownikow placowek dyplomatycznych i konsularnych Акции: продукты гаммы Fusio-Dose
Акции: продукты гаммы Fusio-Dose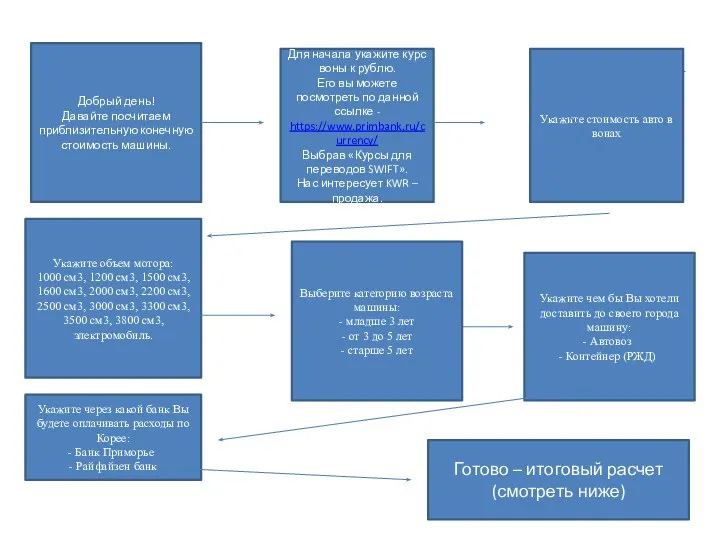 алгоритм
алгоритм 1 апреля – праздник смеха
1 апреля – праздник смеха Особенности кадровой политики в неустойчивых деловых организациях. Тема 5
Особенности кадровой политики в неустойчивых деловых организациях. Тема 5 Циклический алгоритм 6 класс
Циклический алгоритм 6 класс Творческое ассорти
Творческое ассорти Маска, я тебя знаю, или Тайны сценического грима
Маска, я тебя знаю, или Тайны сценического грима Практический опыт использования ИКТ в преподавании биологии 6,8 классы
Практический опыт использования ИКТ в преподавании биологии 6,8 классы Воинский учет в 2022 году
Воинский учет в 2022 году Сила трения в природе
Сила трения в природе Путешествие
Путешествие Создание букета на собственных стеблях без использования каркаса
Создание букета на собственных стеблях без использования каркаса Презентация дидактического материала для работы с одарёнными детьми на уроках литературного чтения ( развитие творческого вообр
Презентация дидактического материала для работы с одарёнными детьми на уроках литературного чтения ( развитие творческого вообр Презентация на тему Русские иконописцы
Презентация на тему Русские иконописцы Компания Commencal
Компания Commencal Сохраним мир живой природы
Сохраним мир живой природы Аудио эксперимент. Гид по генным ключам
Аудио эксперимент. Гид по генным ключам Абсолютные и относительные статистические величины
Абсолютные и относительные статистические величины