- DOC-20221021-WA0014

Содержание
- 2. INFLAMMATORY BOWEL DISEASE Refers to two chronic diseases of unknown etiology that cause inflammation of the
- 3. INTRODUCTION Ulcerative colitis is an idiopathic form of acute and chronic ulcero-inflammatory colitis affecting chiefly the
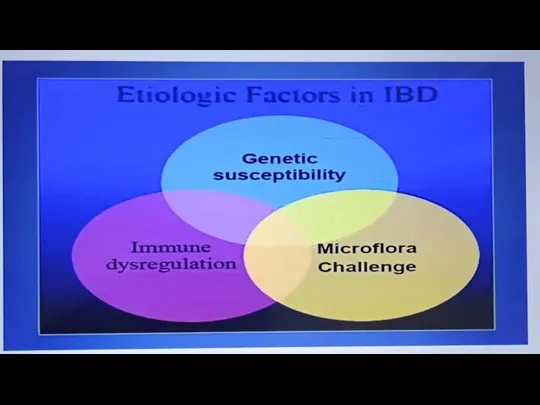
- 5. ETIOLOGY 1 Genetic factors. Genetic factors are implicated in the etiopathogenesis of IBD is supported by
- 6. 2. Immunologic factors. Defective immunologic regulation in IBD has been shown to play significant role in
- 7. 3. Exogenous factors. In addition to role of genetic factors and deranged T-cell mediated immunity, a
- 8. Ii) Psychosocial factors: It has been observed that individuals who are unduly sensitive, dependent on others
- 10. RISE OF INCIDENCE IN IBD IN INDIA Familial aggregation Nicotine Consumption Oral Contraceptives • Dietary Habits-Refined
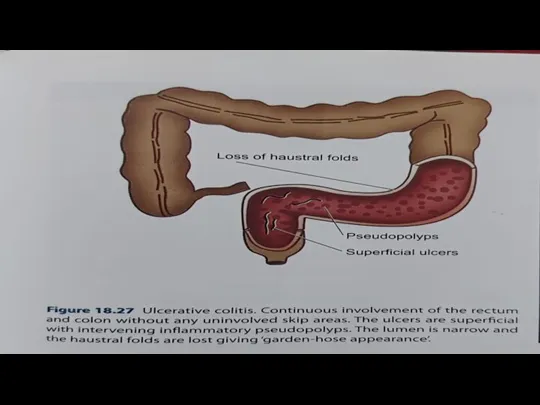
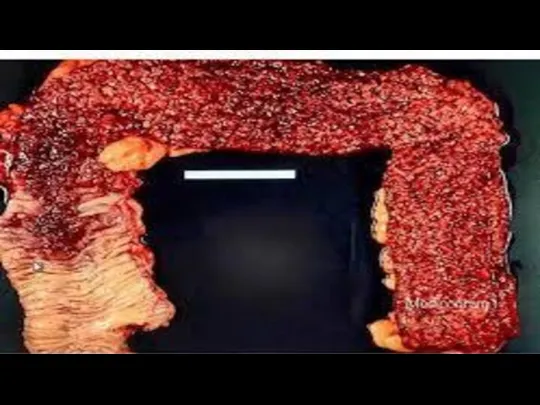
- 11. MORPHOLOGY Mucosa shows linear and superficial ulcers, usually not penetrating the muscular layer. The intervening intact
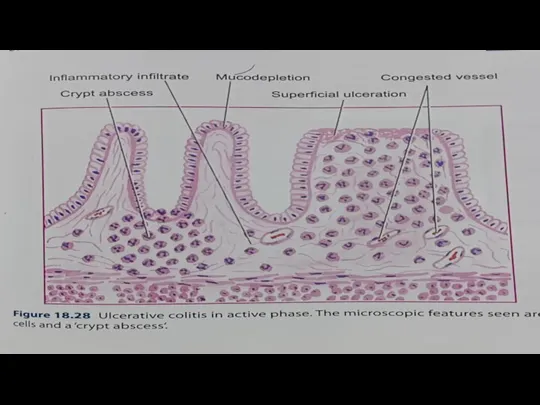
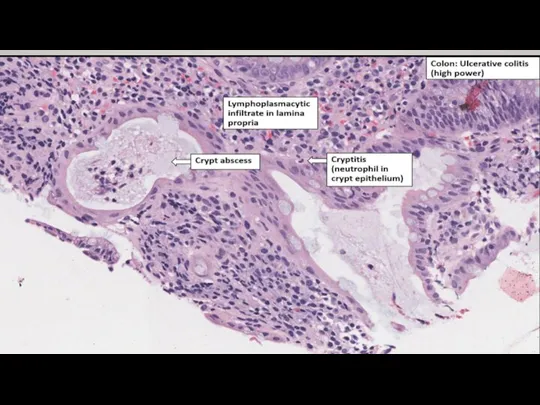
- 14. CHARACTERISTICS FORM OF CHRONIC COLITIS ACCORDING TO BIOPSY 1Crypt distortion, cryptitis and focal accumulations of neutrophils
- 15. 4 Goblet cells are markedly diminished in cases of activedisease. 5. Areas of mucosal regeneration and
- 18. SYMPTOMS Rectal bleeding and tenesmus are universallypresent. Diarrhea and abdominal pain are more frequent with proximal
- 19. COMPLICATIONS 1. Toxic megacolon (Fulminant colitis) is the acute fulminating colitis in which the affected colon
- 23. Скачать презентацию
Слайд 3INTRODUCTION
Ulcerative colitis is an idiopathic form of acute and chronic ulcero-inflammatory
INTRODUCTION
Ulcerative colitis is an idiopathic form of acute and chronic ulcero-inflammatory
Слайд 5ETIOLOGY
1 Genetic factors. Genetic factors are implicated in the etiopathogenesis of
ETIOLOGY
1 Genetic factors. Genetic factors are implicated in the etiopathogenesis of
Слайд 62. Immunologic factors. Defective immunologic regulation in IBD has been shown to
2. Immunologic factors. Defective immunologic regulation in IBD has been shown to
Слайд 73. Exogenous factors. In addition to role of genetic factors and deranged
3. Exogenous factors. In addition to role of genetic factors and deranged
Слайд 8Ii) Psychosocial factors: It has been observed that individuals who are unduly
Ii) Psychosocial factors: It has been observed that individuals who are unduly
Слайд 10RISE OF INCIDENCE IN IBD IN INDIA
Familial aggregation
Nicotine Consumption
Oral Contraceptives
• Dietary
RISE OF INCIDENCE IN IBD IN INDIA
Familial aggregation
Nicotine Consumption
Oral Contraceptives
• Dietary
Слайд 11MORPHOLOGY
Mucosa shows linear and superficial ulcers, usually not penetrating the muscular
MORPHOLOGY
Mucosa shows linear and superficial ulcers, usually not penetrating the muscular
Слайд 14CHARACTERISTICS FORM OF CHRONIC COLITIS ACCORDING TO BIOPSY
1Crypt distortion, cryptitis and
CHARACTERISTICS FORM OF CHRONIC COLITIS ACCORDING TO BIOPSY
1Crypt distortion, cryptitis and
Слайд 154 Goblet cells are markedly diminished in cases of activedisease.
5. Areas of
4 Goblet cells are markedly diminished in cases of activedisease.
5. Areas of
Слайд 18SYMPTOMS
Rectal bleeding and tenesmus are universallypresent.
Diarrhea and abdominal pain are more
SYMPTOMS
Rectal bleeding and tenesmus are universallypresent.
Diarrhea and abdominal pain are more
Слайд 19COMPLICATIONS
1. Toxic megacolon (Fulminant colitis) is the acute fulminating colitis in
COMPLICATIONS
1. Toxic megacolon (Fulminant colitis) is the acute fulminating colitis in
 Презентация на тему И.З. Зуриков Зима
Презентация на тему И.З. Зуриков Зима Канапе в ассортименте
Канапе в ассортименте МОУ СОШ № 10
МОУ СОШ № 10 Жесты судей в волейболе
Жесты судей в волейболе Рекламное агенство
Рекламное агенство Интернет-площадка для бизнеса Ау!
Интернет-площадка для бизнеса Ау! Изучение механизмов и их работа Тема 3.12: Датчик наклона и Рычаг
Изучение механизмов и их работа Тема 3.12: Датчик наклона и Рычаг Презентация на тему Японская поэзия
Презентация на тему Японская поэзия ИКТ на уроках химии
ИКТ на уроках химии Стипендии и гранты имени Сафи Утебаева
Стипендии и гранты имени Сафи Утебаева Кацусика Хокусай – художник Японии
Кацусика Хокусай – художник Японии СССР накануне Великой Отечественной войны
СССР накануне Великой Отечественной войны ВВП
ВВП Еженедельный Отчет Отдела клиентского опыта по СЕБ,
Еженедельный Отчет Отдела клиентского опыта по СЕБ, Презентация про мое имя.
Презентация про мое имя. Доклад «Взаимодействие рынка труда и рынка образовательных услуг в сфере высшей школы в Российской Федерации» Княгинин В. Н., ди
Доклад «Взаимодействие рынка труда и рынка образовательных услуг в сфере высшей школы в Российской Федерации» Княгинин В. Н., ди Предвыборная программа кандидата в студенческий совет
Предвыборная программа кандидата в студенческий совет РЕЗУЛЬТАТЫ СЕССИИ
РЕЗУЛЬТАТЫ СЕССИИ http://bezpeka-service.com.ua/
http://bezpeka-service.com.ua/ Услуги в сфере строительства и управления недвижимостью ООО АУСТЕНА
Услуги в сфере строительства и управления недвижимостью ООО АУСТЕНА Самостоятельная работа по словообразованию
Самостоятельная работа по словообразованию Былина о Садко и Морском царе. Океан-море синее, Н.А. Римский – Корсаков
Былина о Садко и Морском царе. Океан-море синее, Н.А. Римский – Корсаков Занятия гимнастикой. Группы мышц и способы их развития
Занятия гимнастикой. Группы мышц и способы их развития Прибор для охраны газо- и нефтепроводов, военных и гражданских объектов
Прибор для охраны газо- и нефтепроводов, военных и гражданских объектов Итоги развития Волгоградского государственного университета в 2004 г. и задачи на 2005 г.презентация доклада ректора ВолГУ, д. э. н., п
Итоги развития Волгоградского государственного университета в 2004 г. и задачи на 2005 г.презентация доклада ректора ВолГУ, д. э. н., п НРАВСТВЕННЫЕ БЕСЕДЫ СОКРОВИЩА МУДРОСТИ
НРАВСТВЕННЫЕ БЕСЕДЫ СОКРОВИЩА МУДРОСТИ Твои любимые блюда
Твои любимые блюда Наполеон и наполеонизм в художественной культуре
Наполеон и наполеонизм в художественной культуре