- Traumatic shock

Содержание
- 2. The traumatic shock. The prehospital management. The blood replacement in trauma patients. Professor of the department
- 3. Specificity of battle trauma The bleeding is the cause of death in 50%. The management of
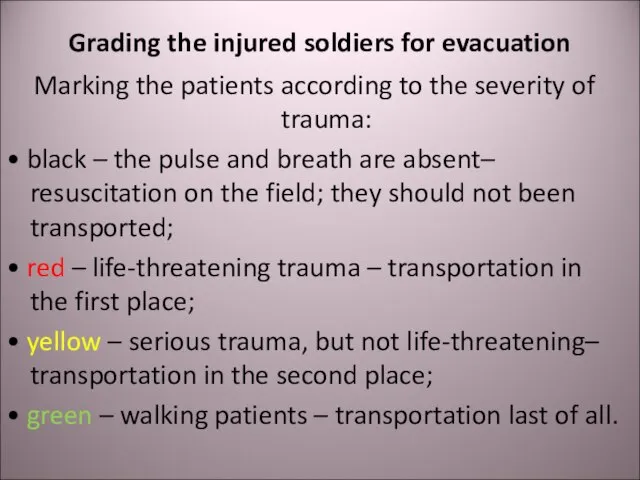
- 4. Grading the injured soldiers for evacuation Marking the patients according to the severity of trauma: •
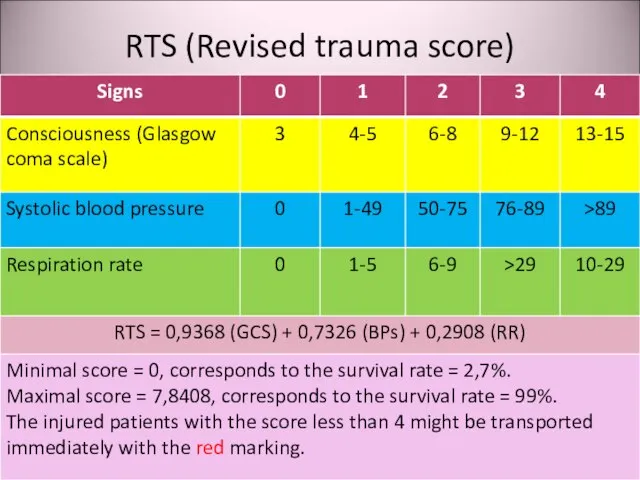
- 5. RTS (Revised trauma score)
- 6. Shock Acute hemodynamic instability, which leads to organ dysfunction due to poor perfusion, with poor oxygen
- 7. Causes of traumatic shock Hypovolemia due to bleeding or dehydration in burned patients; Cardiac failure due
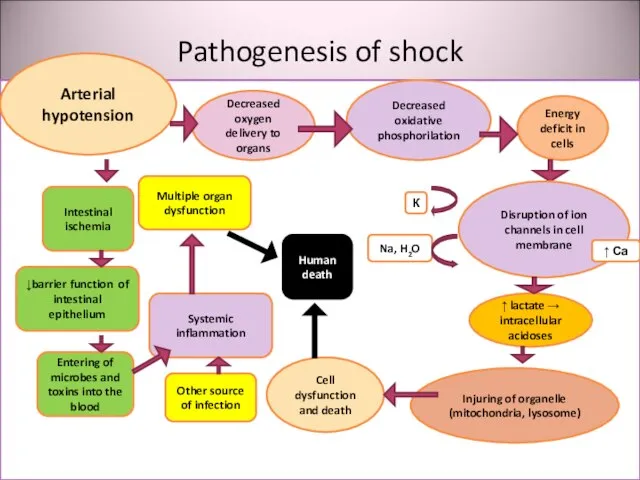
- 8. Pathogenesis of shock утрата Arterial hypotension Decreased oxygen delivery to organs Decreased oxidative phosphorilation Energy deficit
- 9. Clinical signs of shock Paleness Tachycardia Breathlessness Oliguria → anuria Impairment of consciousness Decreased blood pressure
- 10. Stages of shock Compensated: the perfusion of vital organs (brain, lungs, heart) is maintained due to
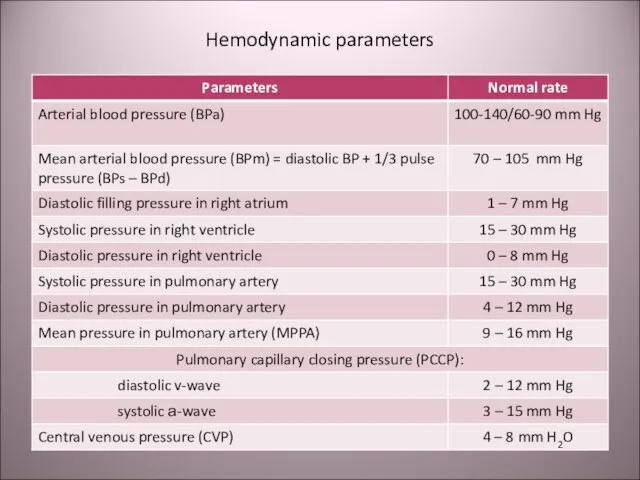
- 11. Hemodynamic parameters
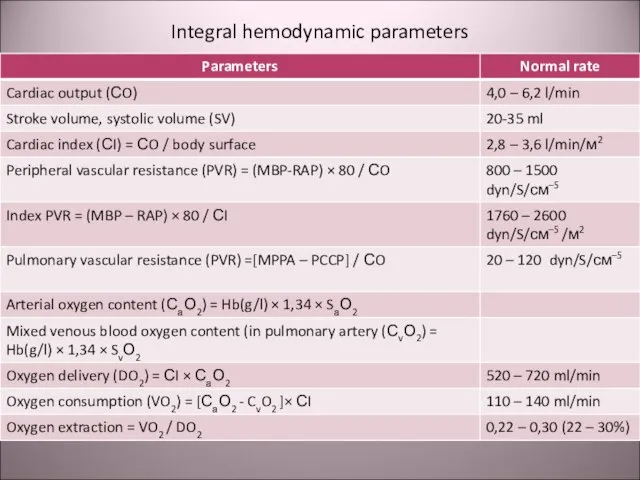
- 12. Integral hemodynamic parameters
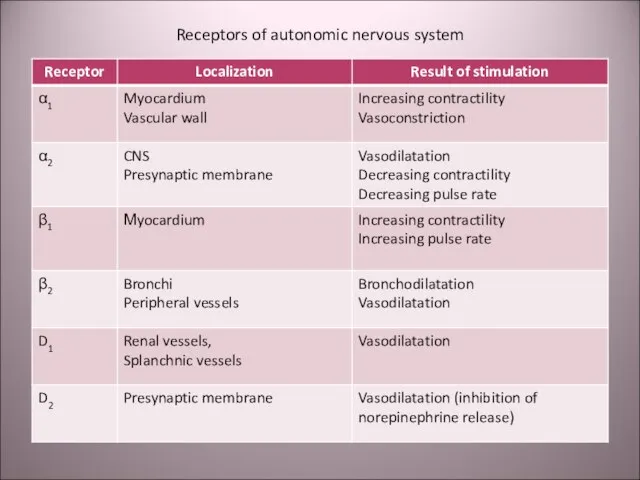
- 13. Receptors of autonomic nervous system
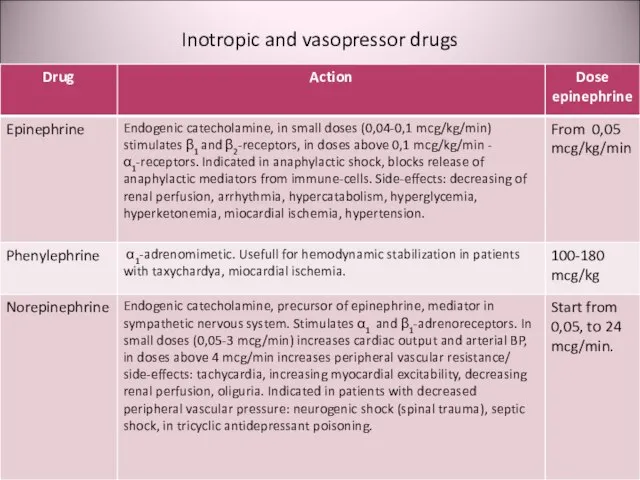
- 14. Inotropic and vasopressor drugs
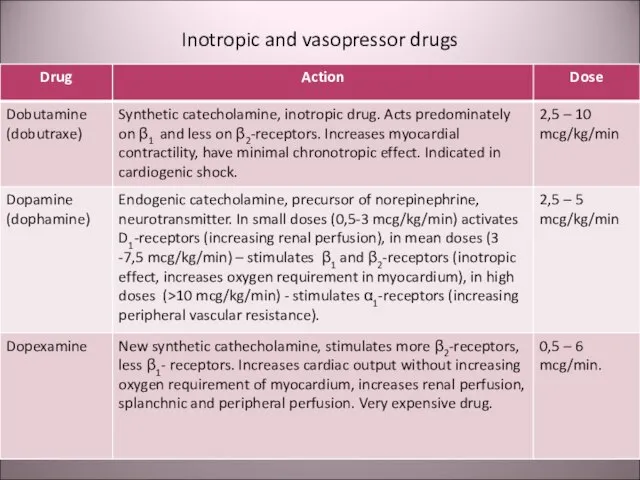
- 15. Inotropic and vasopressor drugs
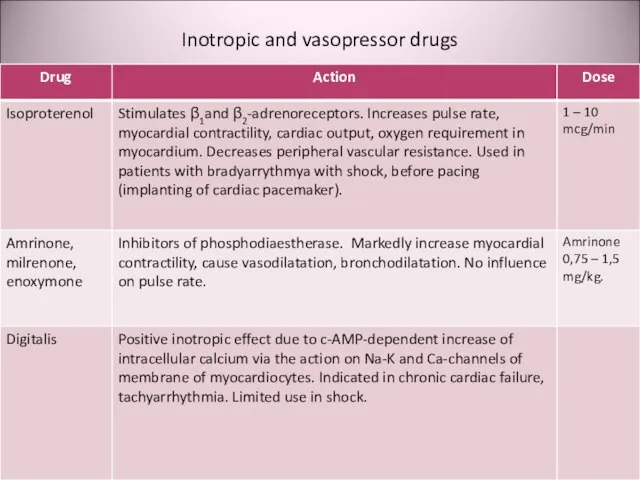
- 16. Inotropic and vasopressor drugs
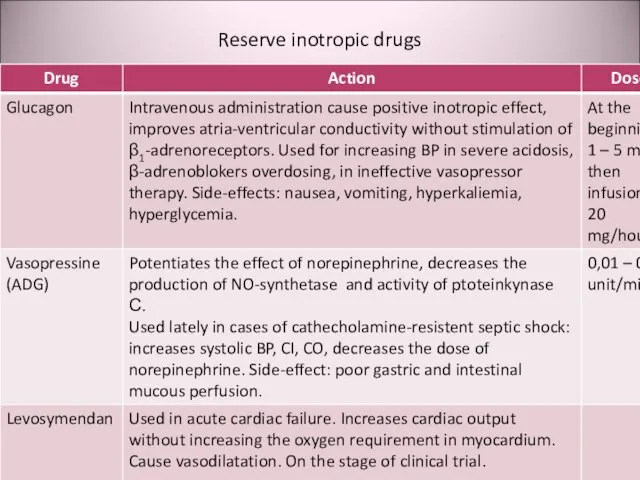
- 17. Reserve inotropic drugs
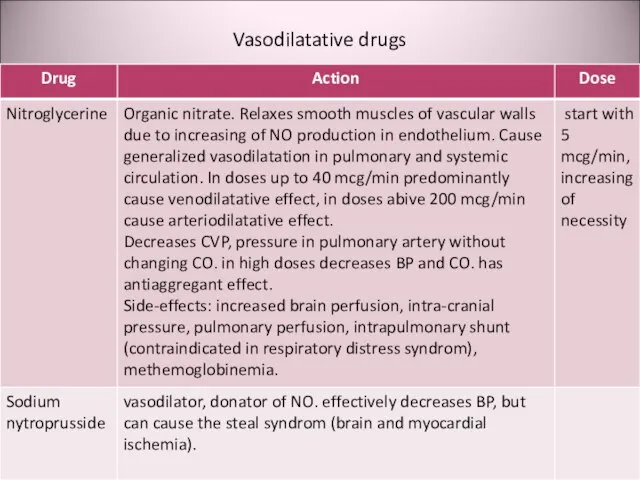
- 18. Vasodilatative drugs
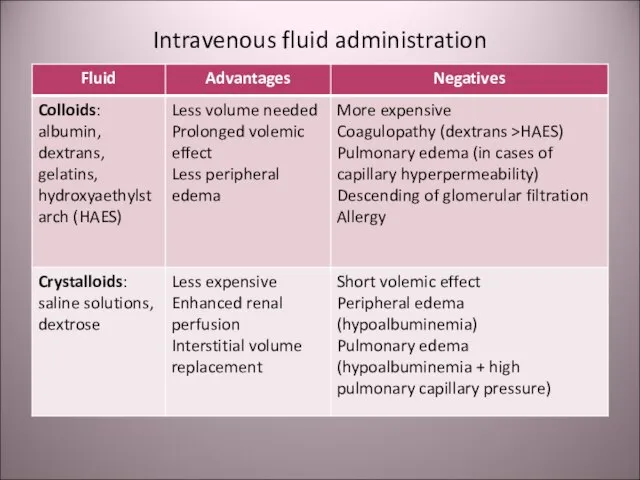
- 19. Intravenous fluid administration
- 20. Cristalloides Normal saline (isotonic 0,9% NaCl). Balanced electrolyte solutions: Ringer‘s lactate, sterofundyne, e.g. Hypertonic NaCl (from
- 21. Synthetic colloides Dextrans: Poliglucine, Reopoliglucine Gelatins: Helafusine, e.g. Hydroxyaethylstarchs (HAES): Haecodez, Refortan, Stabizol, Voluven, Tetrastarch, e.g.
- 22. Polyhydric alcohol solutions: Sorbilact, Reosorbilact, Xylite Crystalloid solutions. Volemic effect is short. Advantages: Energy supply without
- 23. Polivinylpirrolidones: peristoy, haemodez The first synthetic colloides. Repeated administration can lead to depression of reticule-endothelial system
- 24. Perfluorocarbons: Perftoran («blue blood»). The positive effects were exaggerated and did not confirmed in medical practice.
- 25. Blood preparations Whole blood Packed red blood cells Fresh frozen plasma (FFP) Cryoprecipitate Platelets Albumin
- 26. Hemorrhagic shock Cause – blood loss. Hemodynamic changes: Decreased volume of blood circulation, central venous pressure
- 27. Response to the blood loss Sympathetic activation: centralization of blood circulation, discharge of blood from spleen,
- 28. Classification of blood loss severity (American Association of Surgeons)
- 29. At the prehospital stage Algover‘s shock index is useful for evaluating the volume of blood loss:
- 30. Nomogram for calculating the blood volume deficit (Blutvolumendefizit [mL] – right vertical axis) according to the
- 31. Shock index: Is not informative in young children and old patients due to the age differences
- 32. Hemorrhagic shock Laboratory dates: Hb ↓. Ht ↓. Lactate ↑. Diuresis ↓. рН ↓.
- 33. Prehospital management of hemorrhagic shock Venous access – canulation of 2-3 veins; Crystalloid / colloid infusion;
- 34. Infusion rate in continuous bleeding If the bleeding is not stopped the infusion rate must provide
- 35. War – epidemic trauma In the ІІ word war all countries use the blood transfusion. But
- 36. Change of field doctrine On the basis of understanding the pathophisiology of traumatic shock as the
- 37. Change of doctrine The “liberal” regiment of crystalloid infusion gave rise to doubt in early 1990-th.
- 38. Step-by-step in replacement of blood loss At the first stage: saline cristalloids in restrictive regiment (for
- 39. “Damage control” In XX century wars (in Persian Gulf 1990-1991 and in Vietnam 1961-1973) 24% of
- 40. “Damage control” For surgeons it means the physiological correction, but not anatomical correction. This includes stop
- 41. Complete surgical correction Complete surgical correction may be provided in 1-2 days after the stabilization of
- 42. Thank you for your attention! Questions?
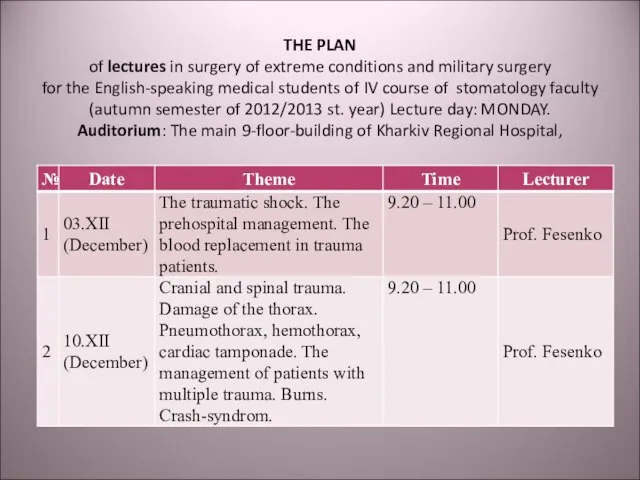
- 43. THE PLAN of lectures in surgery of extreme conditions and military surgery for the English-speaking medical
- 44. THE PLAN of practical classes in surgery of extreme conditions and military surgery for the English-speaking
- 46. Скачать презентацию
Слайд 3Specificity of battle trauma
The bleeding is the cause of death in 50%.
Specificity of battle trauma
The bleeding is the cause of death in 50%.
Слайд 4Grading the injured soldiers for evacuation
Marking the patients according to the severity
Grading the injured soldiers for evacuation
Marking the patients according to the severity
Слайд 5RTS (Revised trauma score)
RTS (Revised trauma score)
Слайд 6Shock
Acute hemodynamic instability, which leads to organ dysfunction due to poor
Shock
Acute hemodynamic instability, which leads to organ dysfunction due to poor
Слайд 7Causes of traumatic shock
Hypovolemia due to bleeding or dehydration in burned patients;
Cardiac
Causes of traumatic shock
Hypovolemia due to bleeding or dehydration in burned patients;
Cardiac
Слайд 8Pathogenesis of shock
утрата
Arterial hypotension
Decreased oxygen delivery to organs
Decreased oxidative phosphorilation
Energy deficit in
Pathogenesis of shock
утрата
Arterial hypotension
Decreased oxygen delivery to organs
Decreased oxidative phosphorilation
Energy deficit in
Слайд 9Clinical signs of shock
Paleness
Tachycardia
Breathlessness
Oliguria → anuria
Impairment of consciousness
Decreased blood
Clinical signs of shock
Paleness
Tachycardia
Breathlessness
Oliguria → anuria
Impairment of consciousness
Decreased blood
Слайд 10Stages of shock
Compensated: the perfusion of vital organs (brain, lungs, heart) is
Stages of shock
Compensated: the perfusion of vital organs (brain, lungs, heart) is
Слайд 11Hemodynamic parameters
Hemodynamic parameters
Слайд 12Integral hemodynamic parameters
Integral hemodynamic parameters
Слайд 13Receptors of autonomic nervous system
Receptors of autonomic nervous system
Слайд 14Inotropic and vasopressor drugs
Inotropic and vasopressor drugs
Слайд 15Inotropic and vasopressor drugs
Inotropic and vasopressor drugs
Слайд 16Inotropic and vasopressor drugs
Inotropic and vasopressor drugs
Слайд 17Reserve inotropic drugs
Reserve inotropic drugs
Слайд 18Vasodilatative drugs
Vasodilatative drugs
Слайд 19Intravenous fluid administration
Intravenous fluid administration
Слайд 20Cristalloides
Normal saline (isotonic 0,9% NaCl).
Balanced electrolyte solutions: Ringer‘s lactate, sterofundyne, e.g.
Hypertonic
Cristalloides
Normal saline (isotonic 0,9% NaCl).
Balanced electrolyte solutions: Ringer‘s lactate, sterofundyne, e.g.
Hypertonic
Слайд 21Synthetic colloides
Dextrans: Poliglucine, Reopoliglucine
Gelatins: Helafusine, e.g.
Hydroxyaethylstarchs (HAES): Haecodez, Refortan, Stabizol, Voluven, Tetrastarch,
Synthetic colloides
Dextrans: Poliglucine, Reopoliglucine
Gelatins: Helafusine, e.g.
Hydroxyaethylstarchs (HAES): Haecodez, Refortan, Stabizol, Voluven, Tetrastarch,
Слайд 22Polyhydric alcohol solutions: Sorbilact, Reosorbilact, Xylite
Crystalloid solutions.
Volemic effect is short.
Advantages:
Polyhydric alcohol solutions: Sorbilact, Reosorbilact, Xylite
Crystalloid solutions.
Volemic effect is short.
Advantages:
Слайд 23Polivinylpirrolidones: peristoy, haemodez
The first synthetic colloides.
Repeated administration can lead to depression
Polivinylpirrolidones: peristoy, haemodez
The first synthetic colloides.
Repeated administration can lead to depression
Слайд 24Perfluorocarbons: Perftoran («blue blood»).
The positive effects were exaggerated and did not confirmed
Perfluorocarbons: Perftoran («blue blood»).
The positive effects were exaggerated and did not confirmed
Слайд 25Blood preparations
Whole blood
Packed red blood cells
Fresh frozen plasma (FFP)
Cryoprecipitate
Platelets
Albumin
Blood preparations
Whole blood
Packed red blood cells
Fresh frozen plasma (FFP)
Cryoprecipitate
Platelets
Albumin
Слайд 26Hemorrhagic shock
Cause – blood loss.
Hemodynamic changes:
Decreased volume of blood circulation, central
Hemorrhagic shock
Cause – blood loss.
Hemodynamic changes:
Decreased volume of blood circulation, central
Слайд 27Response to the blood loss
Sympathetic activation: centralization of blood circulation, discharge of
Response to the blood loss
Sympathetic activation: centralization of blood circulation, discharge of
Слайд 28Classification of blood loss severity
(American Association of Surgeons)
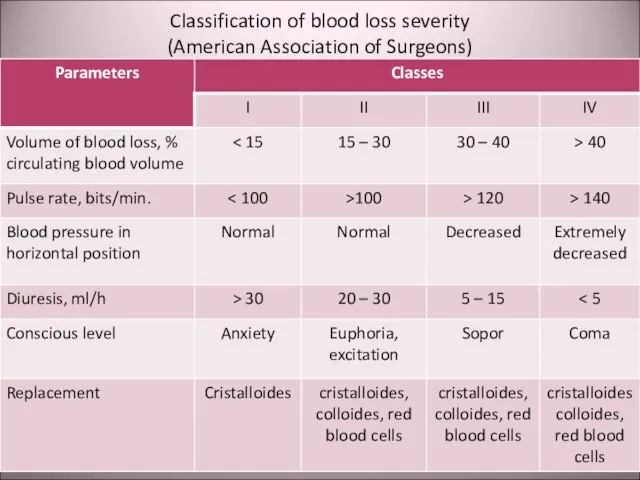
Classification of blood loss severity
(American Association of Surgeons)
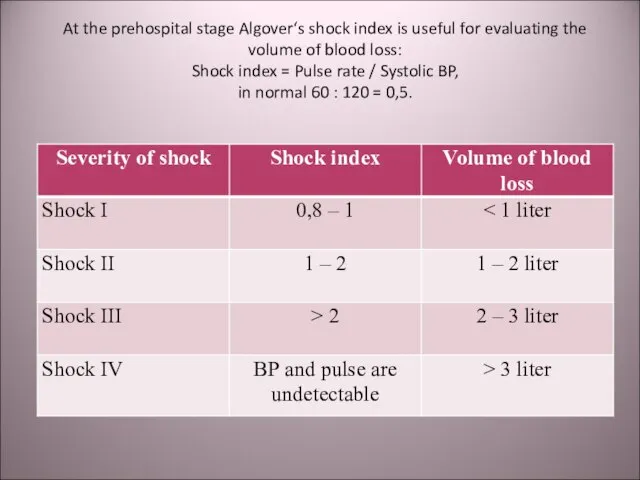
Слайд 29At the prehospital stage Algover‘s shock index is useful for evaluating the
At the prehospital stage Algover‘s shock index is useful for evaluating the
Слайд 30Nomogram for calculating the blood volume deficit (Blutvolumendefizit [mL] – right vertical
Nomogram for calculating the blood volume deficit (Blutvolumendefizit [mL] – right vertical
![Nomogram for calculating the blood volume deficit (Blutvolumendefizit [mL] – right vertical](/_ipx/f_webp&q_80&fit_contain&s_1440x1080/imagesDir/jpg/381760/slide-29.jpg)
Слайд 31Shock index:
Is not informative in young children and old patients due to
Shock index:
Is not informative in young children and old patients due to
Слайд 32Hemorrhagic shock
Laboratory dates:
Hb ↓.
Ht ↓.
Lactate ↑.
Diuresis ↓.
рН ↓.
Hemorrhagic shock
Laboratory dates:
Hb ↓.
Ht ↓.
Lactate ↑.
Diuresis ↓.
рН ↓.
Слайд 33Prehospital management of hemorrhagic shock
Venous access – canulation of 2-3 veins;
Crystalloid /
Prehospital management of hemorrhagic shock
Venous access – canulation of 2-3 veins;
Crystalloid /
Слайд 34Infusion rate in continuous bleeding
If the bleeding is not stopped the infusion
Infusion rate in continuous bleeding
If the bleeding is not stopped the infusion
Слайд 35War – epidemic trauma
In the ІІ word war all countries use the
War – epidemic trauma
In the ІІ word war all countries use the
Слайд 36Change of field doctrine
On the basis of understanding the pathophisiology of traumatic
Change of field doctrine
On the basis of understanding the pathophisiology of traumatic
Слайд 37Change of doctrine
The “liberal” regiment of crystalloid infusion gave rise to doubt
Change of doctrine
The “liberal” regiment of crystalloid infusion gave rise to doubt
Слайд 38Step-by-step in replacement of blood loss
At the first stage: saline cristalloids in
Step-by-step in replacement of blood loss
At the first stage: saline cristalloids in
Слайд 39“Damage control”
In XX century wars (in Persian Gulf 1990-1991 and in Vietnam
“Damage control”
In XX century wars (in Persian Gulf 1990-1991 and in Vietnam
Слайд 40“Damage control”
For surgeons it means the physiological correction, but not anatomical correction.
“Damage control”
For surgeons it means the physiological correction, but not anatomical correction.
Слайд 41Complete surgical correction
Complete surgical correction may be provided in 1-2 days after
Complete surgical correction
Complete surgical correction may be provided in 1-2 days after
Слайд 42
Thank you for your attention!
Questions?
Thank you for your attention!
Questions?

Слайд 43THE PLAN
of lectures in surgery of extreme conditions and military surgery
for
THE PLAN of lectures in surgery of extreme conditions and military surgery for
Слайд 44
THE PLAN
of practical classes in surgery of extreme conditions and military surgery
THE PLAN of practical classes in surgery of extreme conditions and military surgery
 Презентация на тему Программирование ветвящихся алгоритмов Условный оператор
Презентация на тему Программирование ветвящихся алгоритмов Условный оператор  Презентация на тему Упражнения для расслабления мышц
Презентация на тему Упражнения для расслабления мышц  Различия между магистерской диссертацией и бизнес проектом
Различия между магистерской диссертацией и бизнес проектом Ожоговая болезнь
Ожоговая болезнь ДЕНЬ ПОБЕДЫ Наглядно – дидактическое пособие, издательство «Мозаика-Синтез» 900igr.net.
ДЕНЬ ПОБЕДЫ Наглядно – дидактическое пособие, издательство «Мозаика-Синтез» 900igr.net. Нитраты и организм человека
Нитраты и организм человека СОВРЕМЕННАЯ ПОЧТАИ INTERNET
СОВРЕМЕННАЯ ПОЧТАИ INTERNET С Рождеством Христовым!
С Рождеством Христовым! Заработная плата – 2021
Заработная плата – 2021 Собор Парижской Богоматери
Собор Парижской Богоматери МЕТОДЫ ПОВЫШЕНИЯ ЭФФЕКТИВНОСТИ ЖЕЛЕЗНОДОРОЖНЫХ ПЕРЕВОЗОК ЗЕРНОВЫХ ГРУЗОВ
МЕТОДЫ ПОВЫШЕНИЯ ЭФФЕКТИВНОСТИ ЖЕЛЕЗНОДОРОЖНЫХ ПЕРЕВОЗОК ЗЕРНОВЫХ ГРУЗОВ Разработка четырехканального импульсного преобразователя на базе микроконтроллера STM32
Разработка четырехканального импульсного преобразователя на базе микроконтроллера STM32 урок по теме: "Логарифмическая функция, её свойства и график"
урок по теме: "Логарифмическая функция, её свойства и график" Научные основы современного машиностроения
Научные основы современного машиностроения www.AnCom.ru
www.AnCom.ru У у
У у Создание многоуровневого списка
Создание многоуровневого списка Абсцесс и гангрена легких
Абсцесс и гангрена легких Роль имения Спасское-Лутовиново в жизни и творчестве И.С. Тургенева
Роль имения Спасское-Лутовиново в жизни и творчестве И.С. Тургенева Управление образования Исполнительного комитета города Набережные Челны Республики ТатарстанМуниципальное образовательное уч
Управление образования Исполнительного комитета города Набережные Челны Республики ТатарстанМуниципальное образовательное уч ЭФФЕКТИВНОСТЬ ДЕЯТЕЛЬНОСТИ РУКОВОДЯЩИХ КАДРОВ ОВД И ЕЕ ОЦЕНКА
ЭФФЕКТИВНОСТЬ ДЕЯТЕЛЬНОСТИ РУКОВОДЯЩИХ КАДРОВ ОВД И ЕЕ ОЦЕНКА Язвенный Колит
Язвенный Колит Management
Management Александр Родченко
Александр Родченко Цивилизация Инков
Цивилизация Инков Действия сотрудников полиции по предупреждению и пресечению групповых нарушений общественного порядка
Действия сотрудников полиции по предупреждению и пресечению групповых нарушений общественного порядка От пера к компьютеру
От пера к компьютеру Жесты рук
Жесты рук