- Congenital heart diseases

Содержание
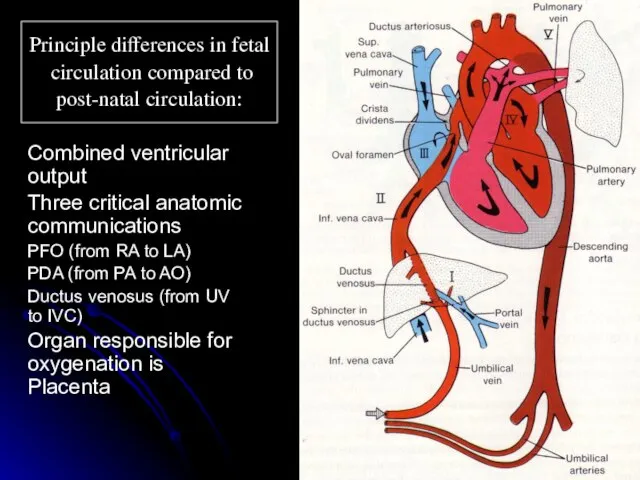
- 2. Principle differences in fetal circulation compared to post-natal circulation: Combined ventricular output Three critical anatomic communications
- 3. CARDIAC EVALUATION History Infants feeding difficulties Easily fatigued Sweating while feeding Tachypnea Poor weight gain Older
- 4. CARDIAC EVALUATION Physical examination HR , RR Assess adequate growth Upper/lower BP Rales Hepatomegaly Cyanosis/clubbing
- 5. CARDIAC EVALUATION Diagnostic tests Chest X-ray ECG Echocardiography Others: MRI ,cardiac catheterization , angiography, exercise testing.
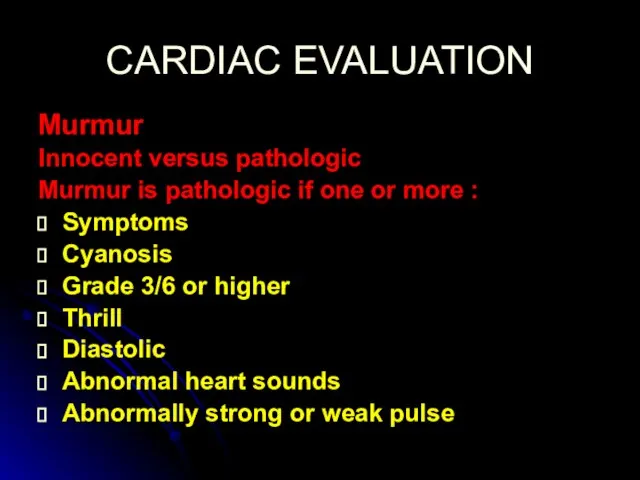
- 7. CARDIAC EVALUATION Murmur Innocent versus pathologic Murmur is pathologic if one or more : Symptoms Cyanosis
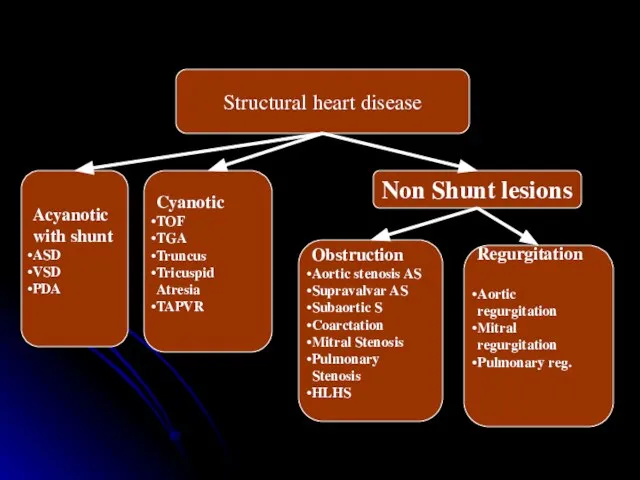
- 8. Structural heart disease Acyanotic with shunt ASD VSD PDA Cyanotic TOF TGA Truncus Tricuspid Atresia TAPVR
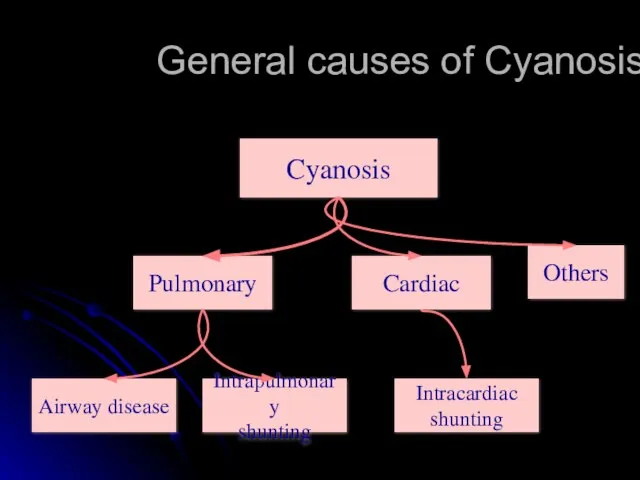
- 10. General causes of Cyanosis Pulmonary Cardiac Others Airway disease Intrapulmonary shunting Intracardiac shunting Cyanosis
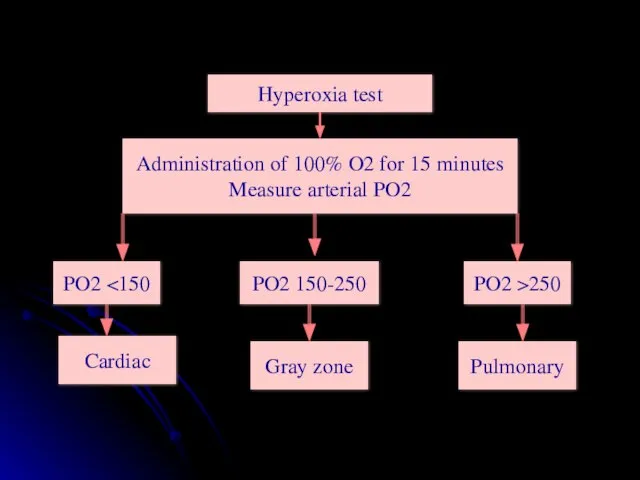
- 11. Hyperoxia test Administration of 100% O2 for 15 minutes Measure arterial PO2 PO2 PO2 >250 PO2
- 12. Left to Right shunt Portion of fully oxygenated pulmonary venous blood bypassing the systemic flow and
- 13. Left to right shunts Physiologic effect of the shunt is dependent on three factors: Location of
- 14. Congenital Heart Lesions that INCREASE Pulmonary Arterial Blood Flow Atrial Septal Defect Complete Atrioventricular Canal Ventricular
- 15. Congenital Heart Disease ACYANOTIC CONGENITAL HEART DISEASE Left to right shunts Ventricular septal defect (VSD) Most
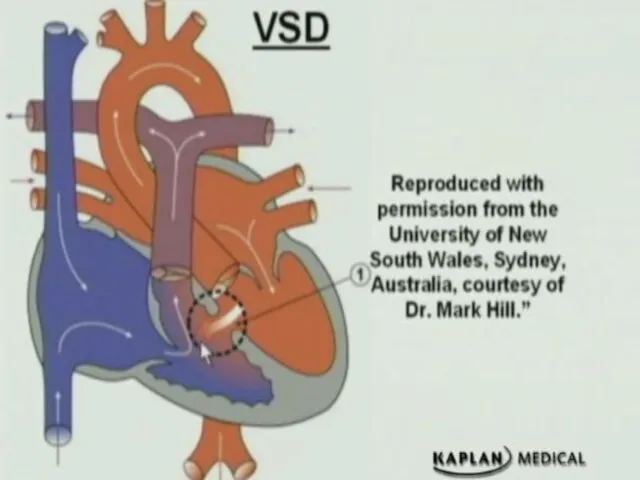
- 16. Congenital Heart Disease
- 17. Ventricular septal defect (VSD) Clinical findings Asymptomatic if small defect with normal pulmonary artery pressure (most)
- 18. Types of VSD Perimembranous (conoventricular defect) Commonest type of VSD Defect is under the aortic valve?
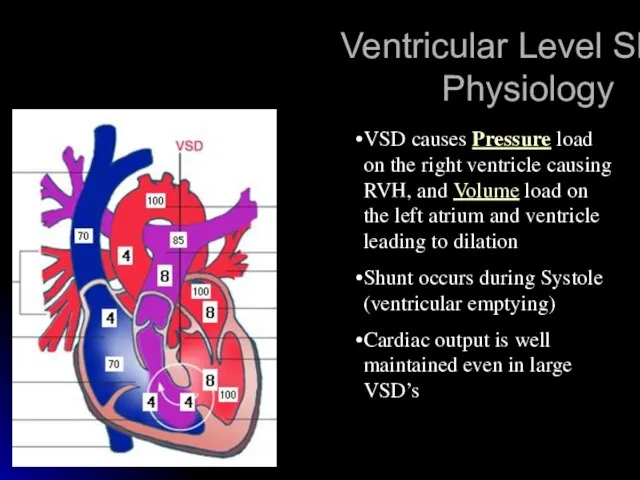
- 19. Ventricular Level Shunt: Physiology VSD causes Pressure load on the right ventricle causing RVH, and Volume
- 20. Diagnostic studies ECG: (beyond infancy) Left axis deviation LVH Left atrial dilation Northwest (superior) axis in
- 21. Management No restriction from activity No SBE prophylaxis (the newer guidelines) Spontaneous closure is common in
- 22. Ventricular septal defect (VSD) Complications Large defects lead to HF, failure to thrive Endocarditis Pulmonary hypertension
- 23. Atrial Septal Defect Acyanotic; asymptomatic, or dyspnea on exertion. Right ventricular lift. Fixed, widely split second
- 24. Types of ASD Ostium secundum ASD: Commonest type Deficiency of septum primum Can be one defect
- 25. Atrial Level Shunt: Physiology ASD causes volume load on the right atrium, and right ventricle leading
- 26. Examination Normal in young infants Prominent RV heave Wide, fixed S2 Ejection systolic murmur Diastolic rumble
- 27. Atrial spetal defect Treatment Most in term infants close spontaneously; symptoms often do not appear until
- 28. Management No restriction from activity No SBE prophylaxis No medications Observation for spontaneous closure if secundum
- 29. Atrial Septal Defect
- 30. Atrial Septal Defect
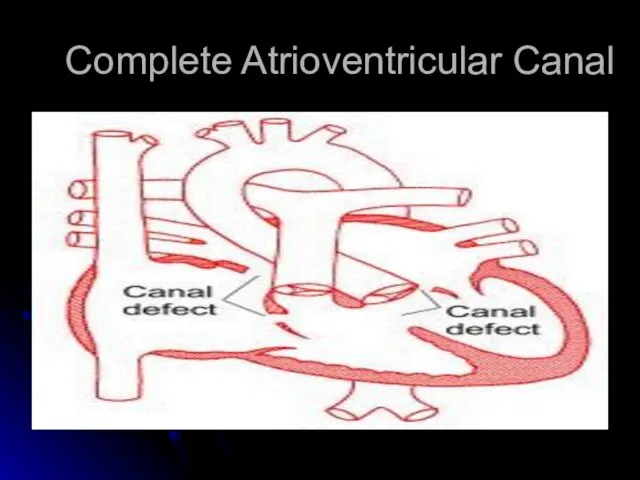
- 31. Complete Atrioventricular Canal
- 32. Complete Atrioventricular Canal Heart failure common in infancy. Cardiomegaly, blowing pansystolic murmur, other variable murmurs. Deficiencies
- 33. Complete Atrioventricular Canal Partial and complete AV canal defects frequently accompany Down’s syndrome. Early surgical correction.
- 34. Congenital Heart Disease Patent Ductus Arteriosus (PDA) results when the ductus arteriosus fails to close;this leads
- 35. Patent Ductus Arteriosis Murmur usually systolic, sometimes continuous, “machinery” Poor feeding, respiratory distress, and frequent respiratory
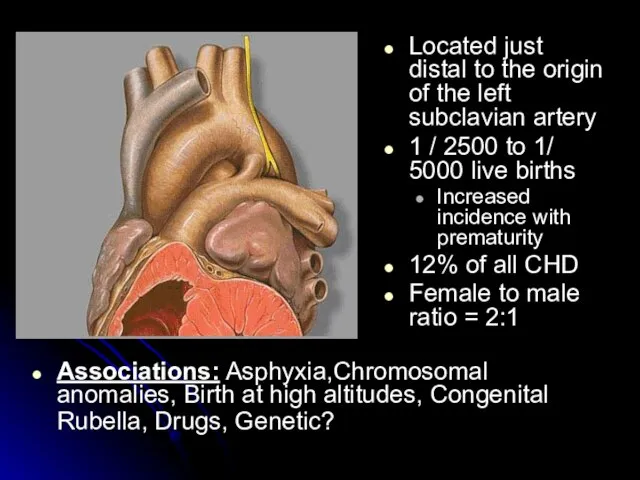
- 36. Located just distal to the origin of the left subclavian artery 1 / 2500 to 1/
- 37. Normal postnatal closure Functional closure Usually occurs within the first 24 hours Stimulated by: High pO2
- 38. Patent Ductus Arteriosus (PDA) Presentation If small – possibly no symptoms If large –heart failure, a
- 39. Management Asymptomatic PDA’s require no treatment before age of 1 year, elective closure can usually be
- 40. Cyanotic heart disease (right to left shunt)
- 41. CYANOTIC CONGENITAL HEART DISEASE Common cyanotic heart disease ( 5 Ts & a P ) Tetralogy
- 42. Congenital Heart Lesions that DECREASE Pulmonary Arterial Blood Flow Tetralogy of Fallot Transposition of the Great
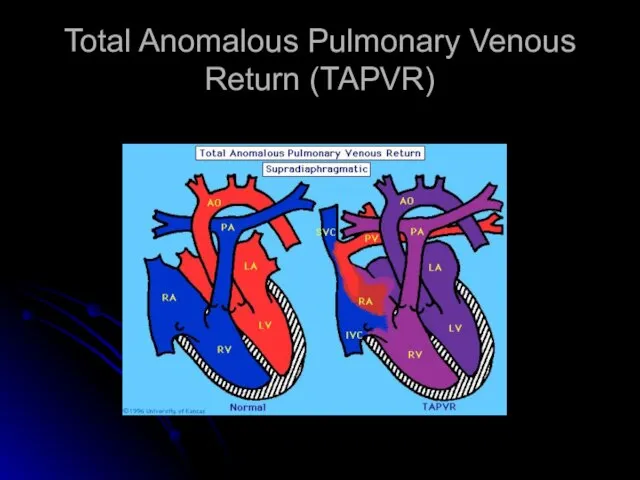
- 43. Total Anomalous Pulmonary Venous Connection Pulmonary veins do not make a direct connection with the left
- 44. Total Anomalous Pulmonary Venous Connection Diagnosis by cardiac catherization or echocardiography. Operative repair in all cases.
- 45. Total Anomalous Pulmonary Venous Return (TAPVR)
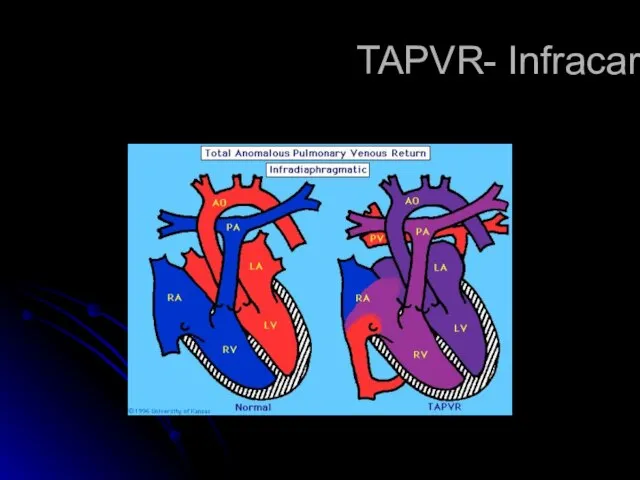
- 46. TAPVR- Infracardiac
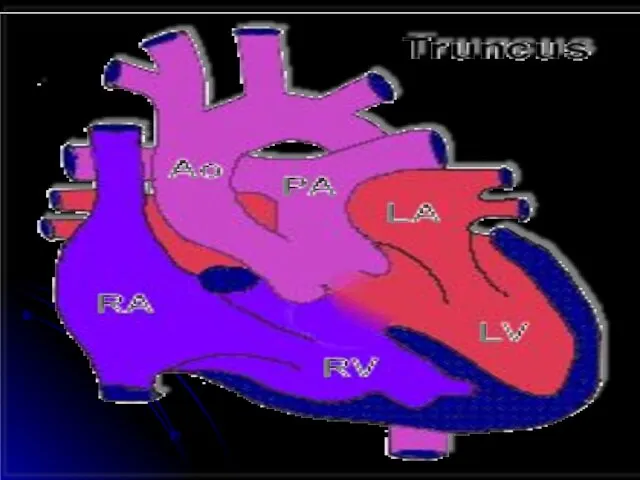
- 48. Truncus Arteriosus Single large vessel overrides the ventricular septum and distributes all the blood ejected from
- 49. Truncus Arteriosus Corrective operation with a valved conduit between right ventricle and pulmonary vessels. Conduit will
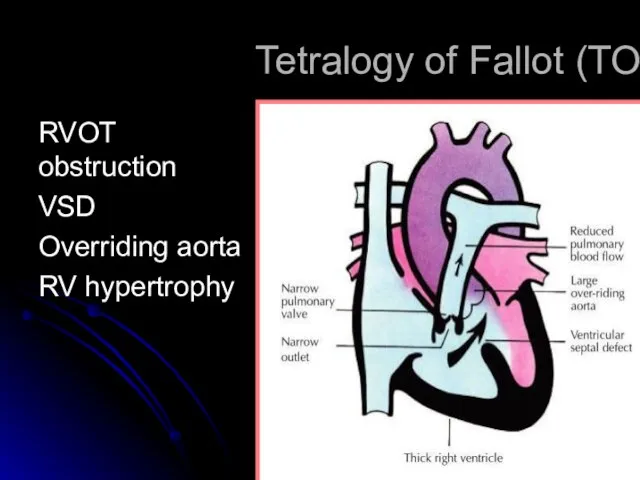
- 51. Tetralogy of Fallot (TOF) RVOT obstruction VSD Overriding aorta RV hypertrophy
- 52. Tetralogy of Fallot Addition of an atrial septal defect falls in the category of Pentalogy of
- 53. Clinical Features Asymptomatic infant with murmur is very common in the usual TOF patients Murmur of
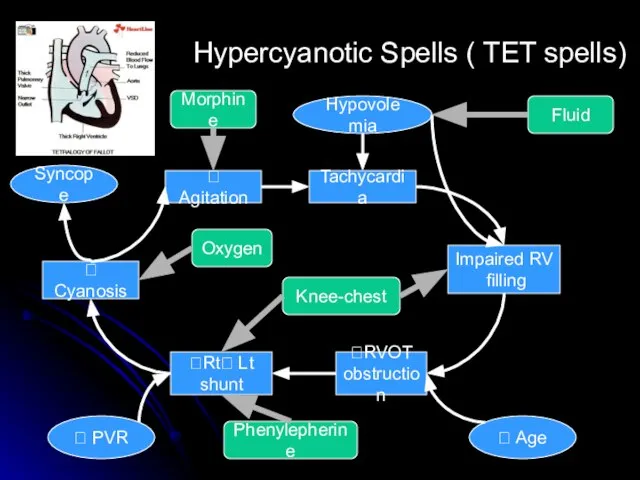
- 54. Tachycardia Impaired RV filling ?RVOT obstruction ?Rt? Lt shunt ? Agitation Hypovolemia ? Age ? PVR
- 55. Tetralogy of Fallot Diagnosis Chest X-ray: Boot-shaped heart, dark lung fields ECG: right axis deviation, RVH
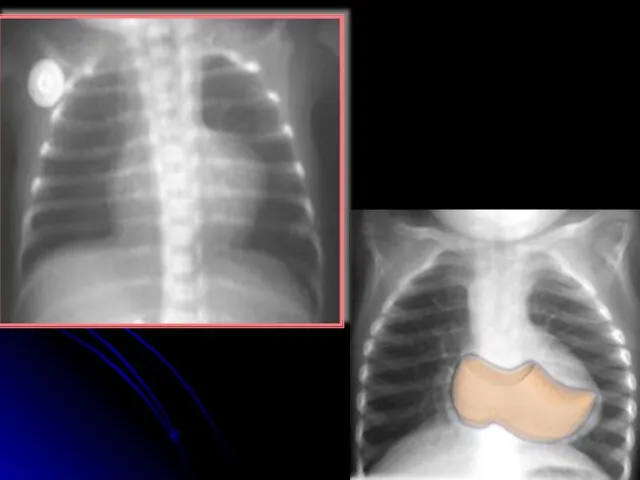
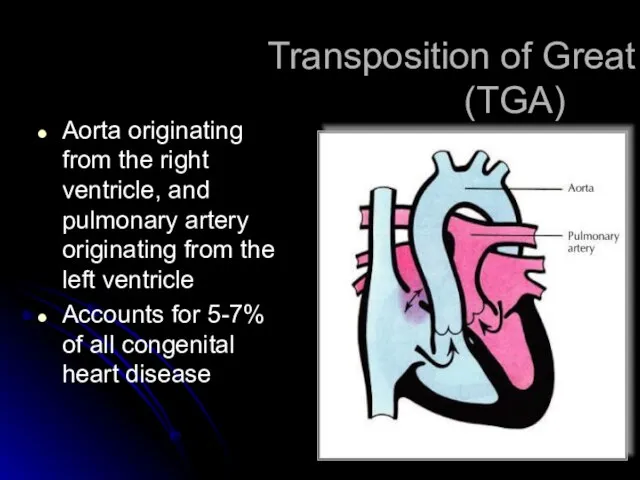
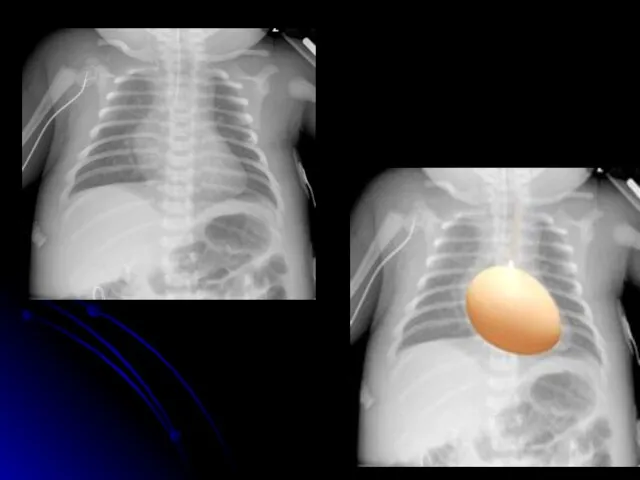
- 57. Transposition of Great Areries (TGA) Aorta originating from the right ventricle, and pulmonary artery originating from
- 58. TGA Survival is dependent on the presence of mixing between the pulmonary and systemic circulation Atrial
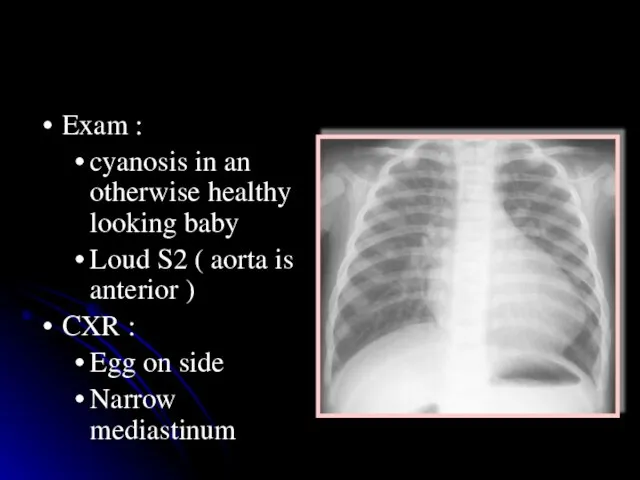
- 59. TGA Exam : cyanosis in an otherwise healthy looking baby Loud S2 ( aorta is anterior
- 61. Transposition of the Great Arteries (TGA) Management • prostaglandin E1 (PGE1) infusion to keep ductus open
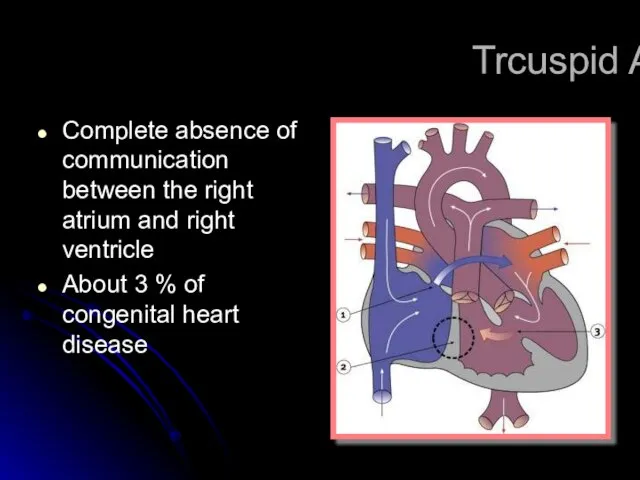
- 62. Trcuspid Atresia Complete absence of communication between the right atrium and right ventricle About 3 %
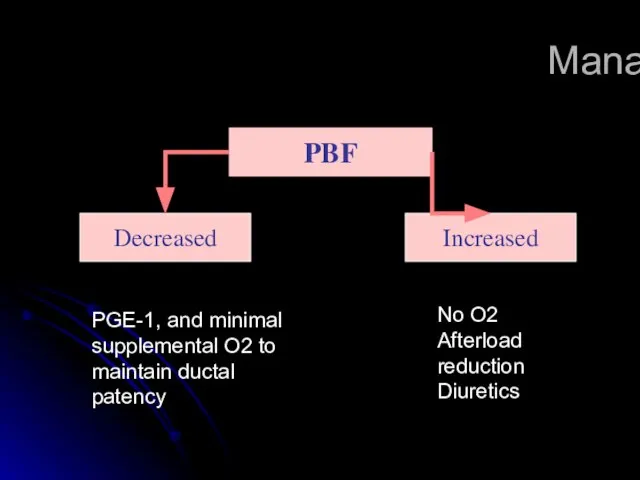
- 63. Management PBF Decreased Increased PGE-1, and minimal supplemental O2 to maintain ductal patency No O2 Afterload
- 64. Tricuspid Atresia Repair consists of shunt from right atrium to pulmonary artery or rudimentary right ventricle
- 65. Ebstein’s Anomaly Septal and posterior leaflets of the tricuspid valve are small and deformed, usually displaced
- 66. Ebstein’s Anomaly Right heart failure in half of patients. Operative repair with tricuspid valve replacement.
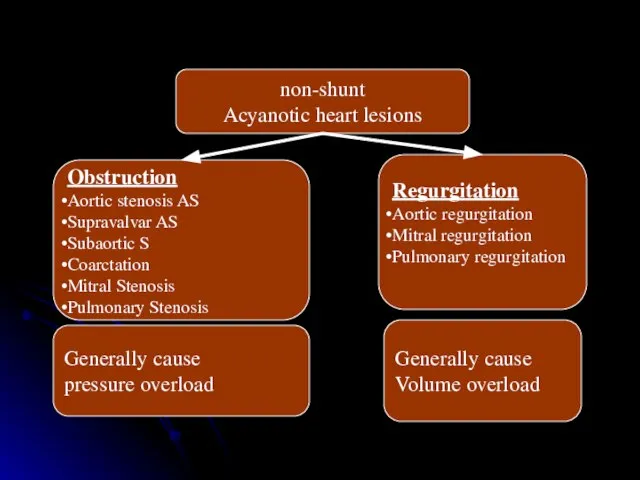
- 68. non-shunt Acyanotic heart lesions Obstruction Aortic stenosis AS Supravalvar AS Subaortic S Coarctation Mitral Stenosis Pulmonary
- 69. Coarctation of the Aorta Males twice as frequently as females. 98% of all coarctations at segment
- 70. Coarctation of the Aorta Absent or weak femoral pulses. Systolic pressure higher in upper extremities than
- 72. Coarctation of the Aorta Older child if milder “juxtaductal” – 90% turner syndrome. May hear murmur
- 75. Coarctation of the Aorta Diagnostic tests Chest X-ray Notching of inferior border of ribs Poststenotic dilatation
- 77. Coarctation of the Aorta Management: Neonats : PGE1 balloon arterioplasty or surgical correction after stabilization Older
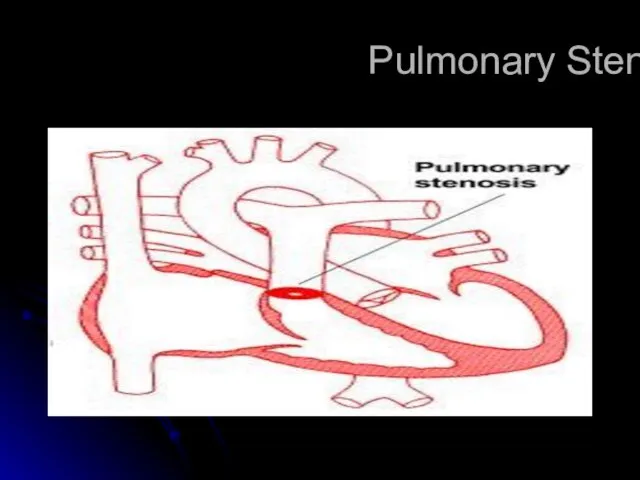
- 78. Pulmonary Stenosis
- 79. Pulmonary Stenosis No symptoms in mild or moderately severe lesions. Cyanosis and right-sided heart failure in
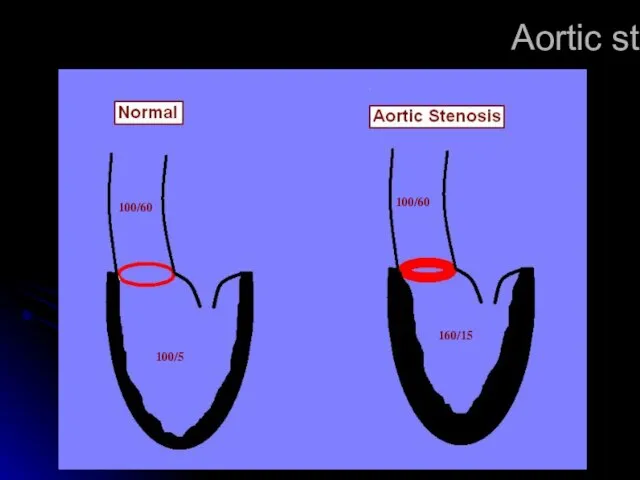
- 80. Aortic stenosis 100/60 100/5 100/60 160/15
- 81. Aortic Stenosis Valvular Aortic Stenosis Subaortic Stenosis Supravalvular Aortic Stenosis Asymmetric Septal Hypertrophy (Idiopathic Hypertrophic Subaortic
- 82. Valvular Aortic Stenosis Most common type, usually asymptomatic in children. May cause severe heart failure in
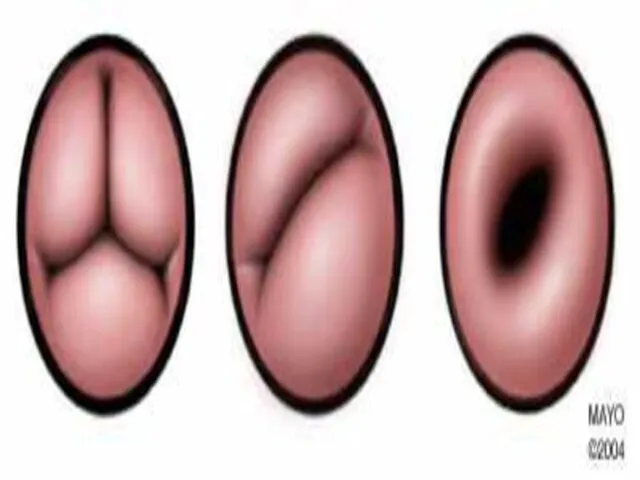
- 84. Valvular Aortic Stenosis Predominantly in males Thickened, fibrotic, malformed aortic leaflets. Fused commissures Bicuspid aortic valve.
- 85. Congenital malformations syndrome with CHD Down syndrome >>>endocardil cushion defect , VSD and ASD Trisomy 18
- 86. Di George syndrome >>aortic arch anomalies Alagille syndrome >> periphral pulmonary stenosis , supravalvular aortic stenosis
- 87. Polycystic kidney disease >> mitral prolapse Diabetes >>hypertrophic cardiomyopathy ,VSD,TGA Kartagner syndrome >> dextrocardia Noonan syndrome
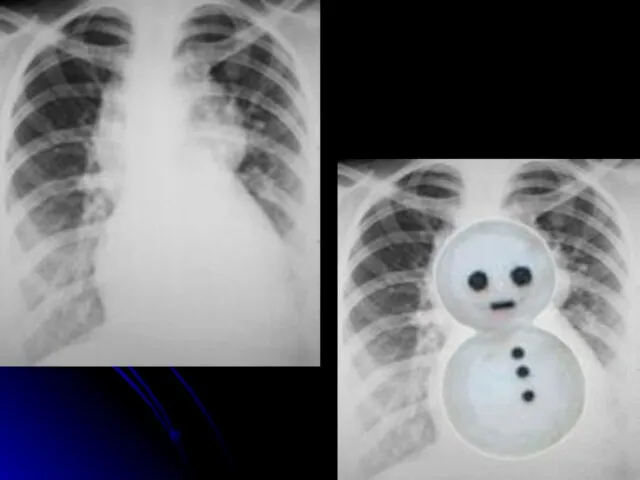
- 88. CXR finding with CHD Figure of 8 ( snowman ) >> total anomalous Boot shape >>>
- 89. Causes of heart failure In neonatal period >>CoA , hypoplastic left heart , sever aortic stenosis
- 91. Скачать презентацию
Слайд 2
Principle differences in fetal
circulation compared to
post-natal circulation:
Combined ventricular output
Three
Principle differences in fetal
circulation compared to
post-natal circulation:
Combined ventricular output
Three
Слайд 3CARDIAC EVALUATION
History
Infants
feeding difficulties
Easily fatigued
Sweating while feeding
Tachypnea
Poor weight gain
Older
CARDIAC EVALUATION
History
Infants
feeding difficulties
Easily fatigued
Sweating while feeding
Tachypnea
Poor weight gain
Older
Слайд 4CARDIAC EVALUATION
Physical examination
HR , RR
Assess adequate growth
Upper/lower BP
Rales
Hepatomegaly
Cyanosis/clubbing
CARDIAC EVALUATION
Physical examination
HR , RR
Assess adequate growth
Upper/lower BP
Rales
Hepatomegaly
Cyanosis/clubbing
Слайд 5CARDIAC EVALUATION
Diagnostic tests
Chest X-ray
ECG
Echocardiography
Others: MRI ,cardiac catheterization , angiography, exercise testing.
CARDIAC EVALUATION
Diagnostic tests
Chest X-ray
ECG
Echocardiography
Others: MRI ,cardiac catheterization , angiography, exercise testing.
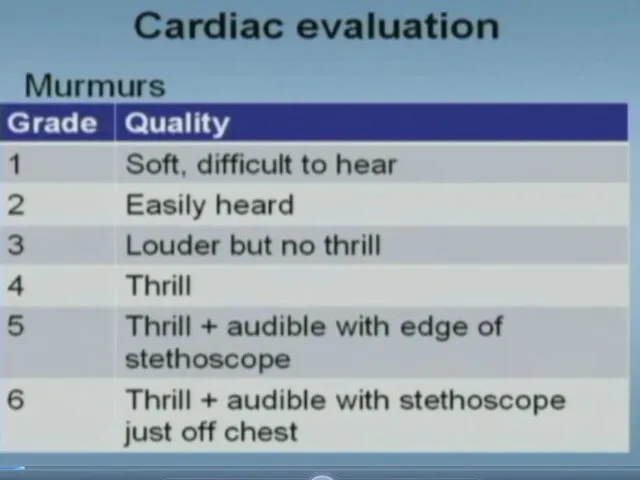
Слайд 7CARDIAC EVALUATION
Murmur
Innocent versus pathologic
Murmur is pathologic if one or more :
Symptoms
Cyanosis
Grade
CARDIAC EVALUATION
Murmur
Innocent versus pathologic
Murmur is pathologic if one or more :
Symptoms
Cyanosis
Grade
Слайд 8Structural heart disease
Acyanotic
with shunt
ASD
VSD
PDA
Cyanotic
TOF
TGA
Truncus
Tricuspid Atresia
TAPVR
Non Shunt lesions
Obstruction
Aortic stenosis AS
Supravalvar AS
Subaortic S
Coarctation
Mitral
Structural heart disease
Acyanotic
with shunt
ASD
VSD
PDA
Cyanotic
TOF
TGA
Truncus
Tricuspid Atresia
TAPVR
Non Shunt lesions
Obstruction
Aortic stenosis AS
Supravalvar AS
Subaortic S
Coarctation
Mitral
Слайд 10General causes of Cyanosis
Pulmonary
Cardiac
Others
Airway disease
Intrapulmonary
shunting
Intracardiac
shunting
Cyanosis
General causes of Cyanosis
Pulmonary
Cardiac
Others
Airway disease
Intrapulmonary
shunting
Intracardiac
shunting
Cyanosis
Слайд 11Hyperoxia test
Administration of 100% O2 for 15 minutes
Measure arterial PO2
PO2 <150
PO2 >250
PO2
Hyperoxia test
Administration of 100% O2 for 15 minutes
Measure arterial PO2
PO2 <150
PO2 >250
PO2
Слайд 12Left to Right shunt
Portion of fully oxygenated pulmonary venous blood bypassing the
Left to Right shunt
Portion of fully oxygenated pulmonary venous blood bypassing the
Слайд 13Left to right shunts
Physiologic effect of the shunt is dependent on three
Left to right shunts
Physiologic effect of the shunt is dependent on three
Слайд 14Congenital Heart Lesions that INCREASE Pulmonary Arterial Blood Flow
Atrial Septal Defect
Complete Atrioventricular
Congenital Heart Lesions that INCREASE Pulmonary Arterial Blood Flow
Atrial Septal Defect
Complete Atrioventricular
Слайд 15Congenital Heart Disease
ACYANOTIC CONGENITAL HEART DISEASE
Left to right shunts
Ventricular septal defect (VSD)
Most
Congenital Heart Disease
ACYANOTIC CONGENITAL HEART DISEASE
Left to right shunts
Ventricular septal defect (VSD)
Most
Слайд 16Congenital Heart Disease
Congenital Heart Disease
Слайд 17Ventricular septal defect (VSD)
Clinical findings
Asymptomatic if small defect with normal pulmonary artery
Ventricular septal defect (VSD)
Clinical findings
Asymptomatic if small defect with normal pulmonary artery
Слайд 18Types of VSD
Perimembranous (conoventricular defect)
Commonest type of VSD
Defect is under the aortic
Types of VSD
Perimembranous (conoventricular defect)
Commonest type of VSD
Defect is under the aortic
Слайд 19Ventricular Level Shunt: Physiology
VSD causes Pressure load on the right ventricle causing
Ventricular Level Shunt: Physiology
VSD causes Pressure load on the right ventricle causing
Слайд 20Diagnostic studies
ECG: (beyond infancy)
Left axis deviation
LVH
Left atrial dilation
Northwest (superior) axis in AV
Diagnostic studies
ECG: (beyond infancy)
Left axis deviation
LVH
Left atrial dilation
Northwest (superior) axis in AV
Слайд 21Management
No restriction from activity
No SBE prophylaxis (the newer guidelines)
Spontaneous closure is common
Management
No restriction from activity
No SBE prophylaxis (the newer guidelines)
Spontaneous closure is common
Слайд 22
Ventricular septal defect (VSD)
Complications
Large defects lead to HF, failure to thrive
Endocarditis
Ventricular septal defect (VSD)
Complications
Large defects lead to HF, failure to thrive
Endocarditis
Слайд 23Atrial Septal Defect
Acyanotic; asymptomatic, or dyspnea on exertion.
Right ventricular lift.
Fixed, widely split
Atrial Septal Defect
Acyanotic; asymptomatic, or dyspnea on exertion.
Right ventricular lift.
Fixed, widely split
Слайд 24Types of ASD
Ostium secundum ASD:
Commonest type
Deficiency of septum primum
Can be one
Types of ASD
Ostium secundum ASD:
Commonest type
Deficiency of septum primum
Can be one
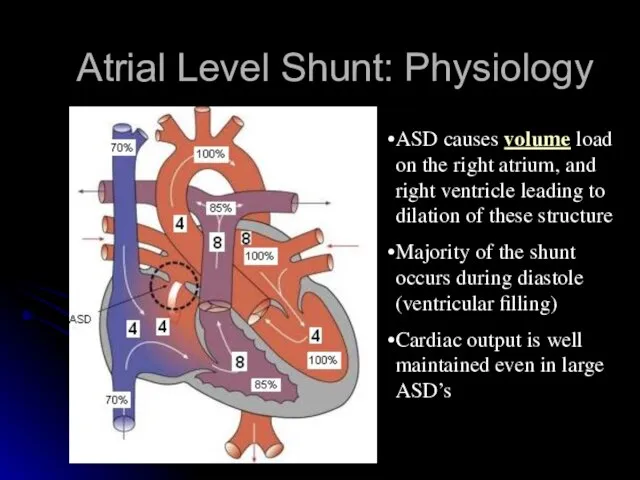
Слайд 25Atrial Level Shunt: Physiology
ASD causes volume load on the right atrium, and
Atrial Level Shunt: Physiology
ASD causes volume load on the right atrium, and
Слайд 26Examination
Normal in young infants
Prominent RV heave
Wide, fixed S2
Ejection systolic murmur
Diastolic rumble
Examination
Normal in young infants
Prominent RV heave
Wide, fixed S2
Ejection systolic murmur
Diastolic rumble
Слайд 27Atrial spetal defect
Treatment
Most in term infants close spontaneously; symptoms often do
Atrial spetal defect
Treatment
Most in term infants close spontaneously; symptoms often do
Слайд 28Management
No restriction from activity
No SBE prophylaxis
No medications
Observation for spontaneous closure if secundum
Management
No restriction from activity
No SBE prophylaxis
No medications
Observation for spontaneous closure if secundum
Слайд 29Atrial Septal Defect
Atrial Septal Defect
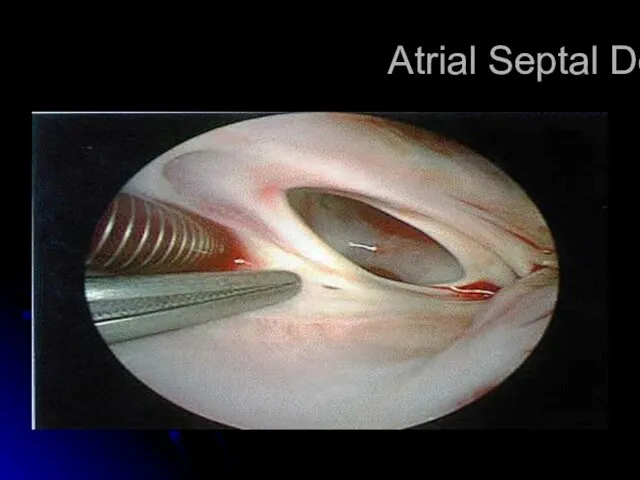
Слайд 30Atrial Septal Defect
Atrial Septal Defect

Слайд 31Complete Atrioventricular Canal
Complete Atrioventricular Canal
Слайд 32Complete Atrioventricular Canal
Heart failure common in infancy.
Cardiomegaly, blowing pansystolic murmur, other variable
Complete Atrioventricular Canal
Heart failure common in infancy.
Cardiomegaly, blowing pansystolic murmur, other variable
Слайд 33Complete Atrioventricular Canal
Partial and complete AV canal defects frequently accompany Down’s syndrome.
Early
Complete Atrioventricular Canal
Partial and complete AV canal defects frequently accompany Down’s syndrome.
Early
Слайд 34Congenital Heart Disease
Patent Ductus Arteriosus (PDA)
results when the ductus arteriosus fails
Congenital Heart Disease
Patent Ductus Arteriosus (PDA)
results when the ductus arteriosus fails
Слайд 35Patent Ductus Arteriosis
Murmur usually systolic, sometimes continuous, “machinery”
Poor feeding, respiratory distress, and
Patent Ductus Arteriosis
Murmur usually systolic, sometimes continuous, “machinery”
Poor feeding, respiratory distress, and
Слайд 36Located just distal to the origin of the left subclavian artery
1 /
Located just distal to the origin of the left subclavian artery
1 /
Слайд 37Normal postnatal closure
Functional closure
Usually occurs within the first 24 hours
Stimulated by:
High
Normal postnatal closure
Functional closure
Usually occurs within the first 24 hours
Stimulated by:
High
Слайд 38Patent Ductus Arteriosus (PDA)
Presentation
If small – possibly no symptoms
If large –heart
Patent Ductus Arteriosus (PDA)
Presentation
If small – possibly no symptoms
If large –heart
Слайд 39Management
Asymptomatic PDA’s require no treatment before age of 1 year, elective closure
Management
Asymptomatic PDA’s require no treatment before age of 1 year, elective closure
Слайд 40Cyanotic heart disease (right to left shunt)
Cyanotic heart disease (right to left shunt)

Слайд 41CYANOTIC CONGENITAL HEART DISEASE
Common cyanotic heart disease ( 5 Ts & a
CYANOTIC CONGENITAL HEART DISEASE
Common cyanotic heart disease ( 5 Ts & a
Слайд 42Congenital Heart Lesions that DECREASE Pulmonary Arterial Blood Flow
Tetralogy of Fallot
Transposition of
Congenital Heart Lesions that DECREASE Pulmonary Arterial Blood Flow
Tetralogy of Fallot
Transposition of
Слайд 43Total Anomalous Pulmonary Venous Connection
Pulmonary veins do not make a direct connection
Total Anomalous Pulmonary Venous Connection
Pulmonary veins do not make a direct connection
Слайд 44Total Anomalous Pulmonary Venous Connection
Diagnosis by cardiac catherization or echocardiography.
Operative repair in
Total Anomalous Pulmonary Venous Connection
Diagnosis by cardiac catherization or echocardiography.
Operative repair in
Слайд 45Total Anomalous Pulmonary Venous Return (TAPVR)
Total Anomalous Pulmonary Venous Return (TAPVR)
Слайд 46TAPVR- Infracardiac
TAPVR- Infracardiac
Слайд 48Truncus Arteriosus
Single large vessel overrides the ventricular septum and distributes all the
Truncus Arteriosus
Single large vessel overrides the ventricular septum and distributes all the
Слайд 49Truncus Arteriosus
Corrective operation with a valved conduit between right ventricle and pulmonary
Truncus Arteriosus
Corrective operation with a valved conduit between right ventricle and pulmonary
Слайд 51Tetralogy of Fallot (TOF)
RVOT obstruction
VSD
Overriding aorta
RV hypertrophy
Tetralogy of Fallot (TOF)
RVOT obstruction
VSD
Overriding aorta
RV hypertrophy
Слайд 52Tetralogy of Fallot
Addition of an atrial septal defect falls in the category
Tetralogy of Fallot
Addition of an atrial septal defect falls in the category
Слайд 53Clinical Features
Asymptomatic infant with murmur is very common in the usual TOF
Clinical Features
Asymptomatic infant with murmur is very common in the usual TOF
Слайд 54Tachycardia
Impaired RV
filling
?RVOT
obstruction
?Rt? Lt
shunt
? Agitation
Hypovolemia
? Age
? PVR
Hypercyanotic Spells ( TET
Tachycardia
Impaired RV
filling
?RVOT
obstruction
?Rt? Lt
shunt
? Agitation
Hypovolemia
? Age
? PVR
Hypercyanotic Spells ( TET
Слайд 55Tetralogy of Fallot
Diagnosis
Chest X-ray: Boot-shaped heart, dark lung fields
ECG: right axis
Tetralogy of Fallot
Diagnosis
Chest X-ray: Boot-shaped heart, dark lung fields
ECG: right axis
Слайд 57Transposition of Great Areries (TGA)
Aorta originating from the right ventricle, and pulmonary
Transposition of Great Areries (TGA)
Aorta originating from the right ventricle, and pulmonary
Слайд 58TGA
Survival is dependent on the presence of mixing between the pulmonary and
TGA
Survival is dependent on the presence of mixing between the pulmonary and
Слайд 59TGA
Exam :
cyanosis in an otherwise healthy looking baby
Loud S2 ( aorta
TGA
Exam :
cyanosis in an otherwise healthy looking baby
Loud S2 ( aorta
Слайд 61
Transposition of the Great Arteries (TGA)
Management
• prostaglandin E1 (PGE1) infusion to keep
Transposition of the Great Arteries (TGA)
Management
• prostaglandin E1 (PGE1) infusion to keep
Слайд 62Trcuspid Atresia
Complete absence of communication between the right atrium and right ventricle
About
Trcuspid Atresia
Complete absence of communication between the right atrium and right ventricle
About
Слайд 63Management
PBF
Decreased
Increased
PGE-1, and minimal supplemental O2 to maintain ductal patency
No O2
Afterload reduction
Diuretics
Management
PBF
Decreased
Increased
PGE-1, and minimal supplemental O2 to maintain ductal patency
No O2
Afterload reduction
Diuretics
Слайд 64Tricuspid Atresia
Repair consists of shunt from right atrium to pulmonary artery or
Tricuspid Atresia
Repair consists of shunt from right atrium to pulmonary artery or

Слайд 65Ebstein’s Anomaly
Septal and posterior leaflets of the tricuspid valve are small and
Ebstein’s Anomaly
Septal and posterior leaflets of the tricuspid valve are small and
Слайд 66Ebstein’s Anomaly
Right heart failure in half of patients.
Operative repair with tricuspid valve
Ebstein’s Anomaly
Right heart failure in half of patients.
Operative repair with tricuspid valve
Слайд 68non-shunt
Acyanotic heart lesions
Obstruction
Aortic stenosis AS
Supravalvar AS
Subaortic S
Coarctation
Mitral Stenosis
Pulmonary Stenosis
Regurgitation
Aortic regurgitation
Mitral regurgitation
Pulmonary regurgitation
Generally
non-shunt
Acyanotic heart lesions
Obstruction
Aortic stenosis AS
Supravalvar AS
Subaortic S
Coarctation
Mitral Stenosis
Pulmonary Stenosis
Regurgitation
Aortic regurgitation
Mitral regurgitation
Pulmonary regurgitation
Generally
Слайд 69Coarctation of the Aorta
Males twice as frequently as females.
98% of all coarctations
Coarctation of the Aorta
Males twice as frequently as females.
98% of all coarctations
Слайд 70Coarctation of the Aorta
Absent or weak femoral pulses.
Systolic pressure higher in upper
Coarctation of the Aorta
Absent or weak femoral pulses.
Systolic pressure higher in upper
Слайд 72
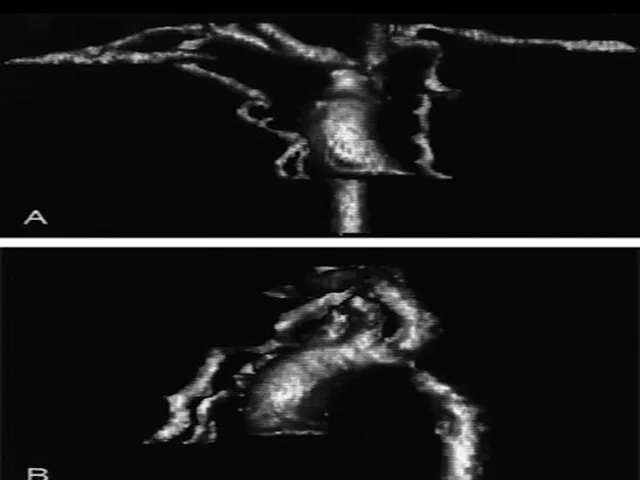
Coarctation of the Aorta
Older child if milder “juxtaductal” – 90% turner syndrome.
May
Coarctation of the Aorta
Older child if milder “juxtaductal” – 90% turner syndrome.
May

Слайд 75
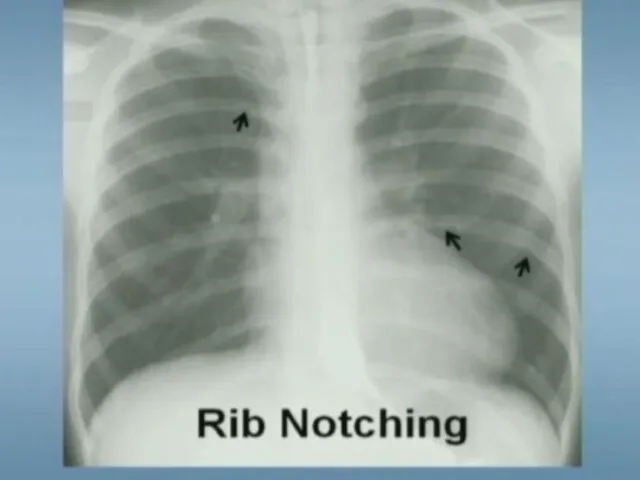
Coarctation of the Aorta
Diagnostic tests
Chest X-ray
Notching of inferior border of ribs
Poststenotic
Coarctation of the Aorta
Diagnostic tests
Chest X-ray
Notching of inferior border of ribs
Poststenotic
Слайд 77
Coarctation of the Aorta
Management:
Neonats :
PGE1
balloon arterioplasty or surgical correction after
Coarctation of the Aorta
Management:
Neonats :
PGE1
balloon arterioplasty or surgical correction after
Слайд 78Pulmonary Stenosis
Pulmonary Stenosis
Слайд 79Pulmonary Stenosis
No symptoms in mild or moderately severe lesions.
Cyanosis and right-sided heart
Pulmonary Stenosis
No symptoms in mild or moderately severe lesions.
Cyanosis and right-sided heart
Слайд 80Aortic stenosis
100/60
100/5
100/60
160/15
Aortic stenosis
100/60
100/5
100/60
160/15
Слайд 81Aortic Stenosis
Valvular Aortic Stenosis
Subaortic Stenosis
Supravalvular Aortic Stenosis
Asymmetric Septal Hypertrophy (Idiopathic Hypertrophic Subaortic
Aortic Stenosis
Valvular Aortic Stenosis
Subaortic Stenosis
Supravalvular Aortic Stenosis
Asymmetric Septal Hypertrophy (Idiopathic Hypertrophic Subaortic
Слайд 82Valvular Aortic Stenosis
Most common type, usually asymptomatic in children.
May cause severe heart
Valvular Aortic Stenosis
Most common type, usually asymptomatic in children.
May cause severe heart
Слайд 84Valvular Aortic Stenosis
Predominantly in males
Thickened, fibrotic, malformed aortic leaflets.
Fused commissures
Bicuspid aortic valve.
Valvular Aortic Stenosis
Predominantly in males
Thickened, fibrotic, malformed aortic leaflets.
Fused commissures
Bicuspid aortic valve.
Слайд 85Congenital malformations syndrome with CHD
Down syndrome >>>endocardil cushion defect , VSD and
Congenital malformations syndrome with CHD
Down syndrome >>>endocardil cushion defect , VSD and
Слайд 86Di George syndrome >>aortic arch anomalies
Alagille syndrome >> periphral pulmonary stenosis
Di George syndrome >>aortic arch anomalies
Alagille syndrome >> periphral pulmonary stenosis
Слайд 87Polycystic kidney disease >> mitral prolapse
Diabetes >>hypertrophic cardiomyopathy ,VSD,TGA
Kartagner syndrome >>
Polycystic kidney disease >> mitral prolapse
Diabetes >>hypertrophic cardiomyopathy ,VSD,TGA
Kartagner syndrome >>
Слайд 88CXR finding with CHD
Figure of 8 ( snowman ) >> total
CXR finding with CHD
Figure of 8 ( snowman ) >> total
Слайд 89Causes of heart failure
In neonatal period >>CoA , hypoplastic left heart
Causes of heart failure
In neonatal period >>CoA , hypoplastic left heart
 Black English (Афроамериканский английский )
Black English (Афроамериканский английский ) Презентация на тему Корень. Родственные слова. Два признака родственных слов
Презентация на тему Корень. Родственные слова. Два признака родственных слов Презентация на тему Русские народные танцы (8 класс)
Презентация на тему Русские народные танцы (8 класс) Первые блюда. Супы
Первые блюда. Супы «Загрязнение атмосферного воздуха посёлка «Магистральный» выбросами автотранспорта и влияние отработанных газовна здоровье
«Загрязнение атмосферного воздуха посёлка «Магистральный» выбросами автотранспорта и влияние отработанных газовна здоровье  Создание рабочих мест
Создание рабочих мест С:ЕНКО MEN
С:ЕНКО MEN Традиции модернизма в искусстве 2-й пол. ХХ века
Традиции модернизма в искусстве 2-й пол. ХХ века Многогранники в живой природе
Многогранники в живой природе Sale 30% Bestia
Sale 30% Bestia ВЫСТУПЛЕНИЕ ПЕРВОГО ВИЦЕ-ПРЕЗИДЕНТА ОАО «РЖД»В.Н.МОРОЗОВА на VII Международной конференции «Рынок транспортных услуг: взаимодейс
ВЫСТУПЛЕНИЕ ПЕРВОГО ВИЦЕ-ПРЕЗИДЕНТА ОАО «РЖД»В.Н.МОРОЗОВА на VII Международной конференции «Рынок транспортных услуг: взаимодейс Эффективный нападающий удар в волейболе
Эффективный нападающий удар в волейболе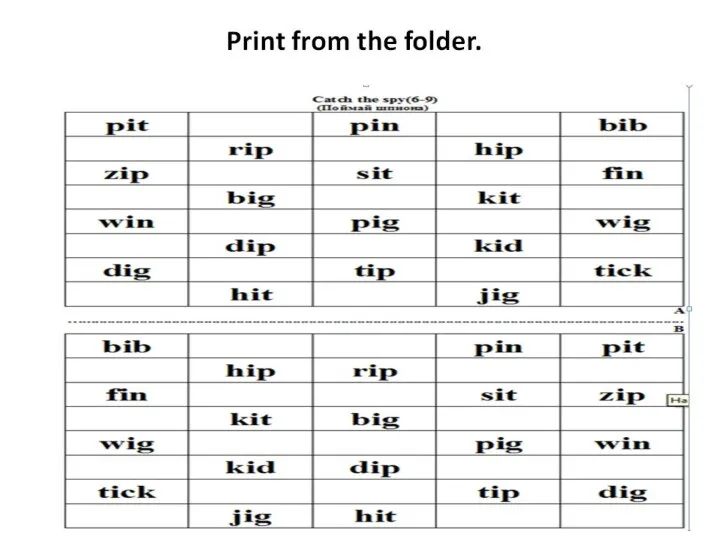 Print from the folder
Print from the folder Шаровая Молния.
Шаровая Молния. МОУ Голицынская СОШ №1 Презентация на тему : «Александр Невский – Патриот Земли Русской»
МОУ Голицынская СОШ №1 Презентация на тему : «Александр Невский – Патриот Земли Русской» Отделение дополнительного образования детей ГОУ школы №20
Отделение дополнительного образования детей ГОУ школы №20 Это мы, здравствуйте! 6 «Б» класс
Это мы, здравствуйте! 6 «Б» класс Потребности и способности
Потребности и способности a4c02c41e02991ba9d4f7fdd7cfefa1c
a4c02c41e02991ba9d4f7fdd7cfefa1c Собрание родителей и обучающихся 11 классов
Собрание родителей и обучающихся 11 классов Анализ и оценка организационных структур управления
Анализ и оценка организационных структур управления Органы государственной власти по Конституции 1918 г
Органы государственной власти по Конституции 1918 г Азбука потребителя
Азбука потребителя Совещание с грузоотправителями Калининградской железной дороги
Совещание с грузоотправителями Калининградской железной дороги Орудия труда
Орудия труда Полупроводниковые приборы
Полупроводниковые приборы Презентация на тему Гора Рашмор
Презентация на тему Гора Рашмор Программы государственной поддержки малого предпринимательства на селе в Республике Карелия
Программы государственной поддержки малого предпринимательства на селе в Республике Карелия