- Neoplasms of the Nose and Paranasal Sinuses

Содержание
- 2. Sinonasal Neoplasms 3% of aerodigestive malignancies 1% of all malignancies 2 to 1 males Sixth to
- 3. Sinonasal Neoplasms Nasal cavity (benign = malignant) Benign - inverting papilloma Malignant - SCCA Sinuses (malignant)
- 4. Epidemiology Occupational exposure in >40% nickel workers - SCCA hardwood dust & leather tanning - adenoca
- 5. Presentation Similar sx to common problems 6 to 8 month delay in diagnosis Cranial neuropathies &
- 6. Presentation Oral - 30% tooth pain, trismus, palatal fullness, erosion Nasal - 50% obstruction, epistaxis, discharge,
- 7. Advanced Disease Classic Triad facial asymmetry tumor bulge in oral cavity nasal mass All three -
- 8. Diagnosis Physical exam Nasal endoscopy Biopsy Radiography
- 9. Computed Tomography Bone erosion orbit, cribiform plate, fovea, post max sinus wall, PTPF, sphenoid, post wall
- 10. MRI Superior to CT multiplanar no ionizing radiation Inflammatory tissue & secretions - intense T2 Tumor
- 11. Schneiderian Papillomas Fungiform (50%) - septum Cylindrical (3%) - lateral nasal wall Inverting (47%) - lateral
- 12. Inverting Papilloma
- 13. Osteomas Benign, slow-growing 15 to 40 years frontal > ethmoid > maxillary local excision
- 14. Fibrous Dysplasia Normal bone replaced by collagen, fibroblasts, and osteoid material ground-glass appearance treatment? No irradiation
- 15. Neurogenic tumors Schwannomas surface of nerve fibers no malignant degeneration along trigeminal & ANS Neurofibromas within
- 16. SCCA Most common - 80% Max > nasal cavity > ethmoids Males Sixth decade 90% have
- 17. Adenoid Cystic Carcinoma Palate > major salivary glands > sinuses Resistant to tx Multiple recurrences, distant
- 18. Mucoepidermoid Carcinoma rare, widespread local invasion Adenocarcinoma 2nd most common, 5-20% ethmoids occupational exposures
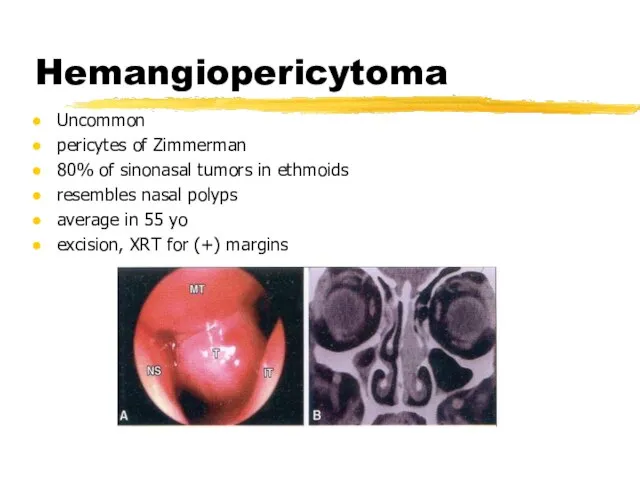
- 19. Hemangiopericytoma Uncommon pericytes of Zimmerman 80% of sinonasal tumors in ethmoids resembles nasal polyps average in
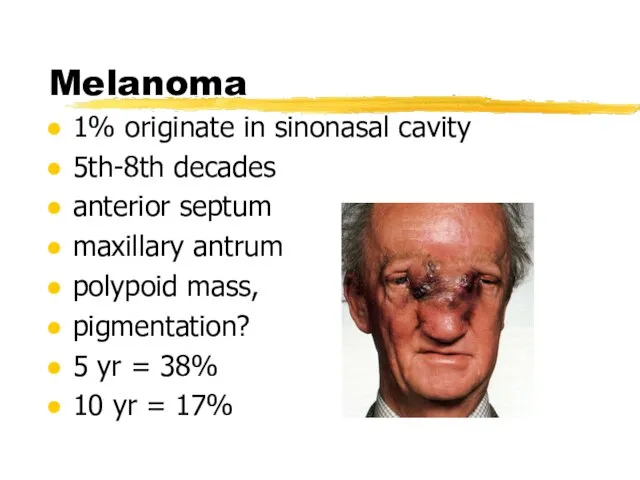
- 20. Melanoma 1% originate in sinonasal cavity 5th-8th decades anterior septum maxillary antrum polypoid mass, pigmentation? 5
- 21. Olfactory Neuroblastoma Neural crest origin no urinary VMA or HVA bimodal distribution at 20 and 50
- 22. Osteogenic Sarcoma most common primary bone tumor only 5% in H & N, mandible most involved
- 23. Chondrosarcoma 3rd-5th decades histologic dx difficult slow erosion of skull base, (+) margins Rhabdomyosarcoma most common
- 24. Lymphoma bimodal presentation NHL irradiation +/- chemo Extramedullary plasmacytoma 40% in paranasal sinuses/nose “benign” must r/o
- 25. Metastatic tumors Renal cell carcinoma lungs breasts urogenital tract gastrointestinal tract Palliation necessary
- 26. Ohngren’s Line Suprastructure Infrastructure
- 27. Staging AJCC - Maxillary sinus carcinoma
- 28. Treatment T3 and T4 60% local recurrence Surgery Irradiation Chemotherapy
- 29. Surgical resection Unresectability (Sisson) extension to frontal lobes invasion of prevertebral fascia bilateral optic nerve involvement
- 30. Surgical resection Endoscopic excision WLE medial maxillectomy total maxillectomy radical maxillectomy +/- exenteration craniofacial resection
- 31. Orbital Preservation Harrison - proptosis, limitation of EOM, bony erosion of orbit = exenteration Conley -
- 32. Orbital preservation UVA - McCary & Levine 50 Gy preop XRT to orbit periorbital bx resect
- 33. Pterygopalatine Fossa 10-20% involvement Som - PTPF invasion = unresectable lesion Craniofacial resection (MCF) Postop XRT
- 34. Neck Dissection Retropharyngeal and jugulodigastric nodes 10% (+) necks neck dissection palpable nodes radiographic evidence of
- 35. Radiation therapy Primary tx only for palliation 10-15% improved 5 year survival XRT = 23% vs.
- 37. Скачать презентацию
Слайд 2Sinonasal Neoplasms
3% of aerodigestive malignancies
1% of all malignancies
2 to 1 males
Sixth to
Sinonasal Neoplasms
3% of aerodigestive malignancies
1% of all malignancies
2 to 1 males
Sixth to
Слайд 3Sinonasal Neoplasms
Nasal cavity (benign = malignant)
Benign - inverting papilloma
Malignant - SCCA
Sinuses (malignant)
SCCA
Maxillary
Sinonasal Neoplasms
Nasal cavity (benign = malignant)
Benign - inverting papilloma
Malignant - SCCA
Sinuses (malignant)
SCCA
Maxillary
Слайд 4Epidemiology
Occupational exposure in >40%
nickel workers - SCCA
hardwood dust & leather tanning -
Epidemiology
Occupational exposure in >40%
nickel workers - SCCA
hardwood dust & leather tanning -
Слайд 5Presentation
Similar sx to common problems
6 to 8 month delay in diagnosis
Cranial neuropathies
Presentation
Similar sx to common problems
6 to 8 month delay in diagnosis
Cranial neuropathies
Слайд 6Presentation
Oral - 30%
tooth pain, trismus, palatal fullness, erosion
Nasal - 50%
obstruction, epistaxis, discharge,
Presentation
Oral - 30%
tooth pain, trismus, palatal fullness, erosion
Nasal - 50%
obstruction, epistaxis, discharge,
Слайд 7Advanced Disease
Classic Triad
facial asymmetry
tumor bulge in oral cavity
nasal mass
All three - 40-60%
One
Advanced Disease
Classic Triad
facial asymmetry
tumor bulge in oral cavity
nasal mass
All three - 40-60%
One
Слайд 8Diagnosis
Physical exam
Nasal endoscopy
Biopsy
Radiography
Diagnosis
Physical exam
Nasal endoscopy
Biopsy
Radiography
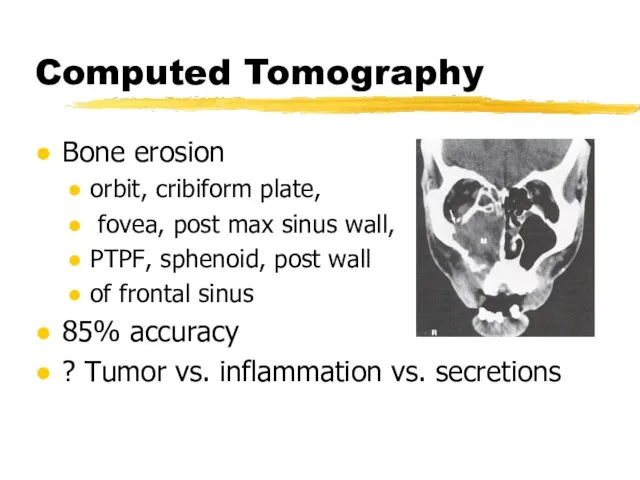
Слайд 9Computed Tomography
Bone erosion
orbit, cribiform plate,
fovea, post max sinus wall,
PTPF, sphenoid,
Computed Tomography
Bone erosion
orbit, cribiform plate,
fovea, post max sinus wall,
PTPF, sphenoid,
Слайд 10MRI
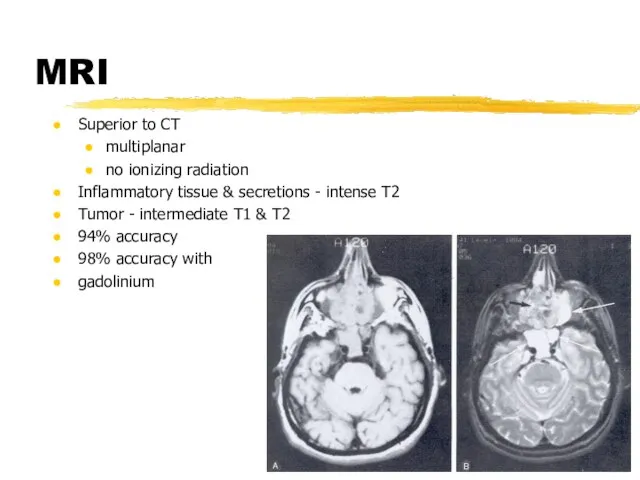
Superior to CT
multiplanar
no ionizing radiation
Inflammatory tissue & secretions - intense T2
Tumor
MRI
Superior to CT
multiplanar
no ionizing radiation
Inflammatory tissue & secretions - intense T2
Tumor
Слайд 11Schneiderian Papillomas
Fungiform (50%) - septum
Cylindrical (3%) - lateral nasal wall
Inverting (47%) -
Schneiderian Papillomas
Fungiform (50%) - septum
Cylindrical (3%) - lateral nasal wall
Inverting (47%) -
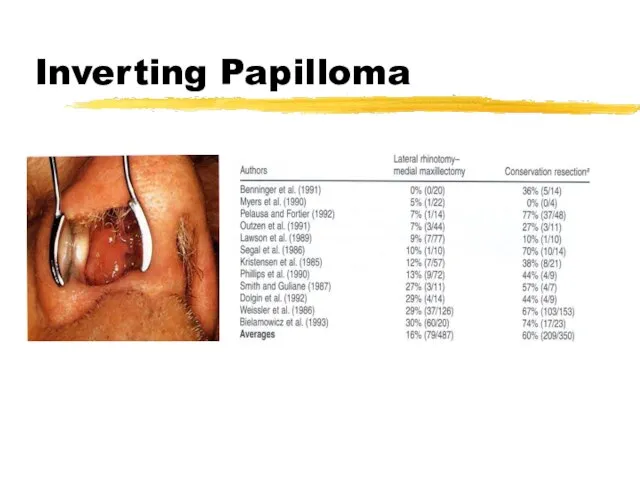
Слайд 12Inverting Papilloma
Inverting Papilloma
Слайд 13Osteomas
Benign, slow-growing
15 to 40 years
frontal > ethmoid > maxillary
local excision
Osteomas
Benign, slow-growing
15 to 40 years
frontal > ethmoid > maxillary
local excision
Слайд 14Fibrous Dysplasia
Normal bone replaced by collagen, fibroblasts, and osteoid material
< 20 years
ground-glass
Fibrous Dysplasia
Normal bone replaced by collagen, fibroblasts, and osteoid material
< 20 years
ground-glass
Слайд 15Neurogenic tumors
Schwannomas
surface of nerve fibers
no malignant degeneration
along trigeminal & ANS
Neurofibromas
within nerve fibers
von
Neurogenic tumors
Schwannomas
surface of nerve fibers
no malignant degeneration
along trigeminal & ANS
Neurofibromas
within nerve fibers
von
Слайд 16SCCA
Most common - 80%
Max > nasal cavity > ethmoids
Males
Sixth decade
90% have eroded
SCCA
Most common - 80%
Max > nasal cavity > ethmoids
Males
Sixth decade
90% have eroded
Слайд 17Adenoid Cystic Carcinoma
Palate > major salivary glands > sinuses
Resistant to tx
Multiple recurrences,
Adenoid Cystic Carcinoma
Palate > major salivary glands > sinuses
Resistant to tx
Multiple recurrences,
Слайд 18Mucoepidermoid Carcinoma
rare, widespread local invasion
Adenocarcinoma
2nd most common, 5-20%
ethmoids
occupational exposures
Mucoepidermoid Carcinoma
rare, widespread local invasion
Adenocarcinoma
2nd most common, 5-20%
ethmoids
occupational exposures
Слайд 19Hemangiopericytoma
Uncommon
pericytes of Zimmerman
80% of sinonasal tumors in ethmoids
resembles nasal polyps
average in 55
Hemangiopericytoma
Uncommon
pericytes of Zimmerman
80% of sinonasal tumors in ethmoids
resembles nasal polyps
average in 55
Слайд 20Melanoma
1% originate in sinonasal cavity
5th-8th decades
anterior septum
maxillary antrum
polypoid mass,
pigmentation?
5 yr =
Melanoma
1% originate in sinonasal cavity
5th-8th decades
anterior septum
maxillary antrum
polypoid mass,
pigmentation?
5 yr =
Слайд 21Olfactory Neuroblastoma
Neural crest origin
no urinary VMA or HVA
bimodal distribution at 20 and
Olfactory Neuroblastoma
Neural crest origin
no urinary VMA or HVA
bimodal distribution at 20 and
Слайд 22Osteogenic Sarcoma
most common primary bone tumor
only 5% in H & N, mandible
Osteogenic Sarcoma
most common primary bone tumor
only 5% in H & N, mandible
Слайд 23Chondrosarcoma
3rd-5th decades
histologic dx difficult
slow erosion of skull base, (+) margins
Rhabdomyosarcoma
most common in
Chondrosarcoma
3rd-5th decades
histologic dx difficult
slow erosion of skull base, (+) margins
Rhabdomyosarcoma
most common in
Слайд 24Lymphoma
bimodal presentation
NHL
irradiation +/- chemo
Extramedullary plasmacytoma
40% in paranasal sinuses/nose
“benign”
must r/o myeloma
excision or irradiation
Lymphoma
bimodal presentation
NHL
irradiation +/- chemo
Extramedullary plasmacytoma
40% in paranasal sinuses/nose
“benign”
must r/o myeloma
excision or irradiation
Слайд 25Metastatic tumors
Renal cell carcinoma
lungs
breasts
urogenital tract
gastrointestinal tract
Palliation necessary
Metastatic tumors
Renal cell carcinoma
lungs
breasts
urogenital tract
gastrointestinal tract
Palliation necessary
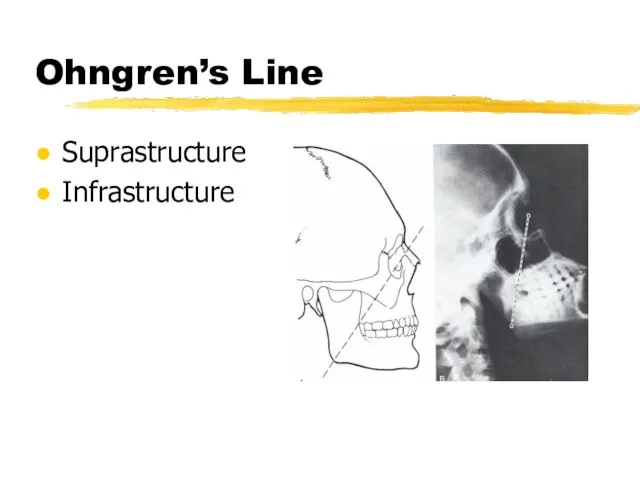
Слайд 26Ohngren’s Line
Suprastructure
Infrastructure
Ohngren’s Line
Suprastructure
Infrastructure
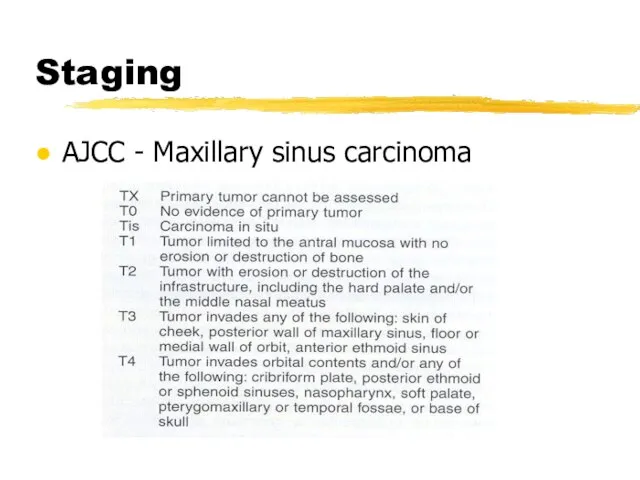
Слайд 27Staging
AJCC - Maxillary sinus carcinoma
Staging
AJCC - Maxillary sinus carcinoma
Слайд 28Treatment
T3 and T4
60% local recurrence
Surgery
Irradiation
Chemotherapy
Treatment
T3 and T4
60% local recurrence
Surgery
Irradiation
Chemotherapy
Слайд 29Surgical resection
Unresectability (Sisson)
extension to frontal lobes
invasion of prevertebral fascia
bilateral optic nerve involvement
cavernous
Surgical resection
Unresectability (Sisson)
extension to frontal lobes
invasion of prevertebral fascia
bilateral optic nerve involvement
cavernous
Слайд 30Surgical resection
Endoscopic excision
WLE
medial maxillectomy
total maxillectomy
radical maxillectomy +/- exenteration
craniofacial resection
Surgical resection
Endoscopic excision
WLE
medial maxillectomy
total maxillectomy
radical maxillectomy +/- exenteration
craniofacial resection
Слайд 31Orbital Preservation
Harrison - proptosis, limitation of EOM, bony erosion of orbit =
Orbital Preservation
Harrison - proptosis, limitation of EOM, bony erosion of orbit =
Слайд 32Orbital preservation
UVA - McCary & Levine
50 Gy preop XRT to orbit
periorbital bx
Orbital preservation
UVA - McCary & Levine
50 Gy preop XRT to orbit
periorbital bx
Слайд 33Pterygopalatine Fossa
10-20% involvement
Som - PTPF invasion = unresectable lesion
Craniofacial resection (MCF)
Postop XRT
Pterygopalatine Fossa
10-20% involvement
Som - PTPF invasion = unresectable lesion
Craniofacial resection (MCF)
Postop XRT
Слайд 34Neck Dissection
Retropharyngeal and jugulodigastric nodes
10% (+) necks
neck dissection
palpable nodes
radiographic evidence of disease
40%
Neck Dissection
Retropharyngeal and jugulodigastric nodes
10% (+) necks
neck dissection
palpable nodes
radiographic evidence of disease
40%
Слайд 35Radiation therapy
Primary tx only for palliation
10-15% improved 5 year survival
XRT = 23%
Radiation therapy
Primary tx only for palliation
10-15% improved 5 year survival
XRT = 23%
 Молодежный сленг 7 класс
Молодежный сленг 7 класс Олег Диващук
Олег Диващук Храмовое искусство Древней Руси.
Храмовое искусство Древней Руси. Город сегодня и завтра. Перспективы развитиясовременной архитектуры
Город сегодня и завтра. Перспективы развитиясовременной архитектуры Техника ручной дуговой сварки
Техника ручной дуговой сварки Эрнст Те?одор Амаде?й Го?фман «Щелкунчик и мышиный король»
Эрнст Те?одор Амаде?й Го?фман «Щелкунчик и мышиный король» Интеллектуально-познавательная игра
Интеллектуально-познавательная игра Мой край – Белгородчина. Цвета флага Белгородской области
Мой край – Белгородчина. Цвета флага Белгородской области Признаки живых организмов
Признаки живых организмов Казачий фольклор
Казачий фольклор «Кукла – как нечто волшебное»
«Кукла – как нечто волшебное» «Мой путь…»
«Мой путь…» Голосовая/факсимильная почта (ГФП)
Голосовая/факсимильная почта (ГФП) Здоровье. Четыре фактора, определяющие состояние индивидуального здоровья
Здоровье. Четыре фактора, определяющие состояние индивидуального здоровья С 8 марта. Пускай живет весна в душе
С 8 марта. Пускай живет весна в душе «Ищу себе маму!»Добрые отзывчивые жители Макушинского района!Вглядитесь в эти грустные глаза детей, ждущих любовь, ласку и тепло
«Ищу себе маму!»Добрые отзывчивые жители Макушинского района!Вглядитесь в эти грустные глаза детей, ждущих любовь, ласку и тепло Великая Отечественная Война
Великая Отечественная Война Чердачные панели. (Тема 4.2)
Чердачные панели. (Тема 4.2) Готовимся к работе по новым Федеральным государственным образовательным стандартам
Готовимся к работе по новым Федеральным государственным образовательным стандартам МОУ МУК № 2 города Костромы
МОУ МУК № 2 города Костромы «О новых подходах к формированию инвестиционного климата в Республике Башкортостан и порядке рассмотрения инвестиционных проек
«О новых подходах к формированию инвестиционного климата в Республике Башкортостан и порядке рассмотрения инвестиционных проек Биография И. С. Тургенева
Биография И. С. Тургенева Кризис 3-х лет или возраст строптивости
Кризис 3-х лет или возраст строптивости Drupal для параноиков: безопасность сайта и системного окружения VPS и выделенных серверов А.Графов
Drupal для параноиков: безопасность сайта и системного окружения VPS и выделенных серверов А.Графов  Лучшие практики разработки: автоматизация сборок и управление кодом в командах
Лучшие практики разработки: автоматизация сборок и управление кодом в командах 02_09_Вопросы_для_вынесения_на_Правление
02_09_Вопросы_для_вынесения_на_Правление Технико-экономическое обоснование проекта
Технико-экономическое обоснование проекта Защита окружающей среды
Защита окружающей среды