- Neoplasms of the Nose and Paranasal Sinus

Содержание
- 2. Neoplasms of Nose and Paranasal Sinuses Very rare 3% Delay in diagnosis due to similarity to
- 3. Neoplasms of Nose and Paranasal Sinuses Multimodality treatment Orbital Preservation Minimally invasive surgical techniques
- 4. Epidemiology Predominately of older males Exposure: Wood, nickel-refining processes Industrial fumes, leather tanning Cigarette and Alcohol
- 5. Location Maxillary sinus 70% Ethmoid sinus 20% Sphenoid 3% Frontal 1%
- 6. Presentation Oral symptoms: 25-35% Pain, trismus, alveolar ridge fullness, erosion Nasal findings: 50% Obstruction, epistaxis, rhinorrhea
- 7. Radiography CT Bony erosion Limitations with periorbita involvement MRI 94 -98% correlation with surgical findings Inflammation/retained
- 8. Benign Lesions Papillomas Osteomas Fibrous Dysplasia Neurogenic tumors
- 9. Papilloma Vestibular papillomas Schneiderian papillomas derived from schneiderian mucosa (squamous) Fungiform: 50%, nasal septum Cylindrical: 3%,
- 10. Inverted Papilloma 4% of sinonasal tumors Site of Origin: lateral nasal wall Unilateral Malignant degeneration in
- 11. Inverted Papilloma Resection Initially via transnasal resection: 50-80% recurrence Medial Maxillectomy via lateral rhinotomy: Gold Standard
- 12. Osteomas Benign slow growing tumors of mature bone Location: Frontal, ethmoids, maxillary sinuses When obstructing mucosal
- 13. Fibrous dysplasia Dysplastic transformation of normal bone with collagen, fibroblasts, and osteoid material Monostotic vs Polyostotic
- 14. Neurogenic tumors 4% are found within the paranasal sinuses Schwannomas Neurofibromas Treatment via surgical resection Neurogenic
- 15. Malignant lesions Squamous cell carcinoma Adenoid cystic carcinoma Mucoepidermoid carcinoma Adenocarcinoma Hemangiopericytoma Melanoma Olfactory neuroblastoma Osteogenic
- 16. Squamous cell carcinoma Most common tumor (80%) Location: Maxillary sinus (70%) Nasal cavity (20%) 90% have
- 17. Treatment 88% present in advanced stages (T3/T4) Surgical resection with postoperative radiation Complex 3-D anatomy makes
- 18. Adenoid Cystic Carcinoma 3rd most common site is the nose/paranasal sinuses Perineural spread Anterograde and retrograde
- 19. Mucoepidermoid Carcinoma Extremely rare Widespread local invasion makes resection difficult, therefore radiation is often indicated
- 20. Adenocarcinoma 2nd most common malignant tumor in the maxillary and ethmoid sinuses Present most often in
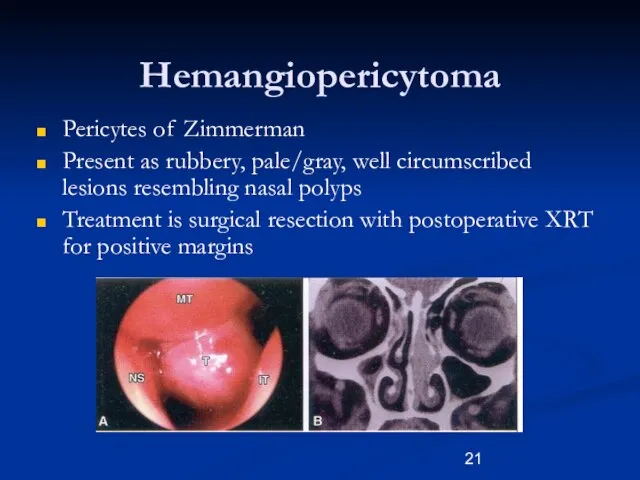
- 21. Hemangiopericytoma Pericytes of Zimmerman Present as rubbery, pale/gray, well circumscribed lesions resembling nasal polyps Treatment is
- 22. Melanoma 0.5- 1.5% of melanoma originates from the nasal cavity and paranasal sinus. Anterior Septum: most
- 23. Olfactory Neuroblastoma Esthesioneuroblastoma Originate from stem cells of neural crest origin that differentiate into olfactory sensory
- 24. Olfactory Neuroblastoma Esthesioneuroblastoma UCLA Staging system T1: Tumor involving nasal cavity and/or paranasal sinus, excluding the
- 25. Olfactory Neuroblastoma Esthesioneuroblastoma Aggressive behavior Local failure: 50-75% Metastatic disease develops in 20-30% Treatment: En bloc
- 26. Sarcomas Osteogenic Sarcoma Most common primary malignancy of bone. Mandible > Maxilla Sunray radiographic appearance Fibrosarcoma
- 27. Rhabdomyosarcoma Most common paranasal sinus malignancy in children Non-orbital, parameningeal Triple therapy is often necessary Aggressive
- 28. Lymphoma Non-Hodgkins type Treatment is by radiation, with or without chemotherapy Survival drops to 10% for
- 29. Sinonasal Undifferentiated Carcinoma Aggressive locally destructive lesion Dependent on pathological differentiation from melanoma, lymphoma, and olfactory
- 30. Metastatic Tumors Renal cell carcinoma is the most common Palliative treatment only
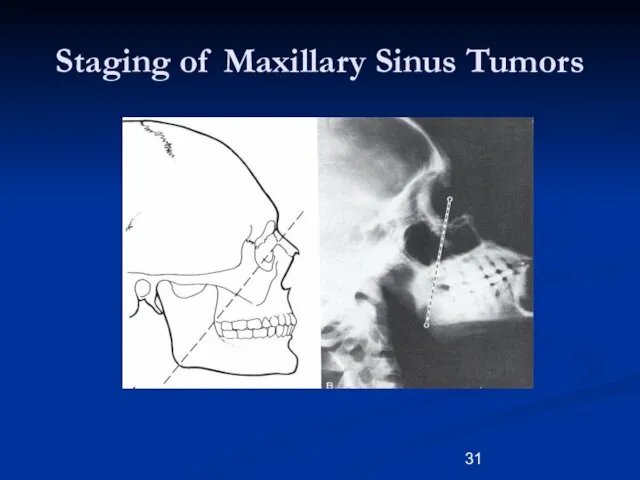
- 31. Staging of Maxillary Sinus Tumors
- 32. Staging of Maxillary Sinus Tumors T1: limited to antral mucosa without bony erosion T2: erosion or
- 33. Surgery Unresectable tumors: Superior extension: frontal lobes Lateral extension: cavernous sinus Posterior extension: prevertebral fascia Bilateral
- 34. Surgery Surgical approaches: Endoscopic Lateral rhinotomy Transoral/transpalatal Midfacial degloving Weber-Fergusson Combined craniofacial approach Extent of resection
- 35. Tracheostomy 130 maxillectomies only 7.7% required tracheostomy Of those not receiving tracheostomy during surgery, only 0.9%
- 36. Treatment of the Orbit Before 1970’s orbital exenteration was included in the radical resection Preoperative radiation
- 37. Current indications for orbital exenteration Involvement of the orbital apex Involvement of the extraocular muscles Involvement
- 38. Conclusions Neoplasms of the nose and paranasal sinus are very rare and require a high index
- 40. Скачать презентацию
Слайд 3Neoplasms of Nose and Paranasal Sinuses
Multimodality treatment
Orbital Preservation
Minimally invasive surgical techniques
Neoplasms of Nose and Paranasal Sinuses
Multimodality treatment
Orbital Preservation
Minimally invasive surgical techniques
Слайд 4
Epidemiology
Predominately of older males
Exposure:
Wood, nickel-refining processes
Industrial fumes, leather tanning
Cigarette and Alcohol
Epidemiology
Predominately of older males
Exposure:
Wood, nickel-refining processes
Industrial fumes, leather tanning
Cigarette and Alcohol
Слайд 5Location
Maxillary sinus
70%
Ethmoid sinus
20%
Sphenoid
3%
Frontal
1%
Location
Maxillary sinus
70%
Ethmoid sinus
20%
Sphenoid
3%
Frontal
1%
Слайд 6Presentation
Oral symptoms: 25-35%
Pain, trismus, alveolar ridge fullness, erosion
Nasal findings: 50%
Obstruction, epistaxis, rhinorrhea
Ocular
Presentation
Oral symptoms: 25-35%
Pain, trismus, alveolar ridge fullness, erosion
Nasal findings: 50%
Obstruction, epistaxis, rhinorrhea
Ocular
Слайд 7Radiography
CT
Bony erosion
Limitations with periorbita involvement
MRI
94 -98% correlation with surgical findings
Inflammation/retained secretions: low
Radiography
CT
Bony erosion
Limitations with periorbita involvement
MRI
94 -98% correlation with surgical findings
Inflammation/retained secretions: low
Слайд 8Benign Lesions
Papillomas
Osteomas
Fibrous Dysplasia
Neurogenic tumors
Benign Lesions
Papillomas
Osteomas
Fibrous Dysplasia
Neurogenic tumors
Слайд 9Papilloma
Vestibular papillomas
Schneiderian papillomas derived from schneiderian mucosa (squamous)
Fungiform: 50%, nasal septum
Cylindrical: 3%,
Papilloma
Vestibular papillomas
Schneiderian papillomas derived from schneiderian mucosa (squamous)
Fungiform: 50%, nasal septum
Cylindrical: 3%,
Слайд 10Inverted Papilloma
4% of sinonasal tumors
Site of Origin: lateral nasal wall
Unilateral
Malignant degeneration in
Inverted Papilloma
4% of sinonasal tumors
Site of Origin: lateral nasal wall
Unilateral
Malignant degeneration in
Слайд 11Inverted Papilloma
Resection
Initially via transnasal resection:
50-80% recurrence
Medial Maxillectomy via lateral rhinotomy:
Gold Standard
10-20%
Endoscopic medial
Inverted Papilloma
Resection
Initially via transnasal resection:
50-80% recurrence
Medial Maxillectomy via lateral rhinotomy:
Gold Standard
10-20%
Endoscopic medial
Слайд 12Osteomas
Benign slow growing tumors of mature bone
Location:
Frontal, ethmoids, maxillary sinuses
When obstructing mucosal
Osteomas
Benign slow growing tumors of mature bone
Location:
Frontal, ethmoids, maxillary sinuses
When obstructing mucosal
Слайд 13Fibrous dysplasia
Dysplastic transformation of normal bone with collagen, fibroblasts, and osteoid material
Monostotic
Fibrous dysplasia
Dysplastic transformation of normal bone with collagen, fibroblasts, and osteoid material
Monostotic
Слайд 14Neurogenic tumors
4% are found within the paranasal sinuses
Schwannomas
Neurofibromas
Treatment via surgical resection
Neurogenic Sarcomas
Neurogenic tumors
4% are found within the paranasal sinuses
Schwannomas
Neurofibromas
Treatment via surgical resection
Neurogenic Sarcomas
Слайд 15Malignant lesions
Squamous cell carcinoma
Adenoid cystic carcinoma
Mucoepidermoid carcinoma
Adenocarcinoma
Hemangiopericytoma
Melanoma
Olfactory neuroblastoma
Osteogenic sarcoma, fibrosarcoma, chondrosarcoma, rhabdomyosarcoma
Lymphoma
Metastatic
Malignant lesions
Squamous cell carcinoma
Adenoid cystic carcinoma
Mucoepidermoid carcinoma
Adenocarcinoma
Hemangiopericytoma
Melanoma
Olfactory neuroblastoma
Osteogenic sarcoma, fibrosarcoma, chondrosarcoma, rhabdomyosarcoma
Lymphoma
Metastatic
Слайд 16Squamous cell carcinoma
Most common tumor (80%)
Location:
Maxillary sinus (70%)
Nasal cavity (20%)
90% have local
Squamous cell carcinoma
Most common tumor (80%)
Location:
Maxillary sinus (70%)
Nasal cavity (20%)
90% have local
Слайд 17Treatment
88% present in advanced stages (T3/T4)
Surgical resection with postoperative radiation
Complex 3-D anatomy
Treatment
88% present in advanced stages (T3/T4)
Surgical resection with postoperative radiation
Complex 3-D anatomy
Слайд 18Adenoid Cystic Carcinoma
3rd most common site is the nose/paranasal sinuses
Perineural spread
Anterograde and
Adenoid Cystic Carcinoma
3rd most common site is the nose/paranasal sinuses
Perineural spread
Anterograde and
Слайд 19Mucoepidermoid Carcinoma
Extremely rare
Widespread local invasion makes resection difficult, therefore radiation is often
Mucoepidermoid Carcinoma
Extremely rare
Widespread local invasion makes resection difficult, therefore radiation is often
Слайд 20Adenocarcinoma
2nd most common malignant tumor in the maxillary and ethmoid sinuses
Present most
Adenocarcinoma
2nd most common malignant tumor in the maxillary and ethmoid sinuses
Present most
Слайд 21Hemangiopericytoma
Pericytes of Zimmerman
Present as rubbery, pale/gray, well circumscribed lesions resembling nasal polyps
Treatment
Hemangiopericytoma
Pericytes of Zimmerman
Present as rubbery, pale/gray, well circumscribed lesions resembling nasal polyps
Treatment
Слайд 22Melanoma
0.5- 1.5% of melanoma originates from the nasal cavity and paranasal sinus.
Anterior
Melanoma
0.5- 1.5% of melanoma originates from the nasal cavity and paranasal sinus.
Anterior
Слайд 23Olfactory Neuroblastoma
Esthesioneuroblastoma
Originate from stem cells of neural crest origin that differentiate into
Olfactory Neuroblastoma
Esthesioneuroblastoma
Originate from stem cells of neural crest origin that differentiate into
Слайд 24Olfactory Neuroblastoma
Esthesioneuroblastoma
UCLA Staging system
T1: Tumor involving nasal cavity and/or paranasal sinus, excluding
Olfactory Neuroblastoma
Esthesioneuroblastoma
UCLA Staging system
T1: Tumor involving nasal cavity and/or paranasal sinus, excluding
Слайд 25Olfactory Neuroblastoma
Esthesioneuroblastoma
Aggressive behavior
Local failure: 50-75%
Metastatic disease develops in 20-30%
Treatment:
En bloc surgical resection
Olfactory Neuroblastoma
Esthesioneuroblastoma
Aggressive behavior
Local failure: 50-75%
Metastatic disease develops in 20-30%
Treatment:
En bloc surgical resection
Слайд 26Sarcomas
Osteogenic Sarcoma
Most common primary malignancy of bone.
Mandible > Maxilla
Sunray radiographic appearance
Fibrosarcoma
Chondrosarcoma
Sarcomas
Osteogenic Sarcoma
Most common primary malignancy of bone.
Mandible > Maxilla
Sunray radiographic appearance
Fibrosarcoma
Chondrosarcoma
Слайд 27Rhabdomyosarcoma
Most common paranasal sinus malignancy in children
Non-orbital, parameningeal
Triple therapy is often necessary
Aggressive
Rhabdomyosarcoma
Most common paranasal sinus malignancy in children
Non-orbital, parameningeal
Triple therapy is often necessary
Aggressive
Слайд 28Lymphoma
Non-Hodgkins type
Treatment is by radiation, with or without chemotherapy
Survival drops to 10%
Lymphoma
Non-Hodgkins type
Treatment is by radiation, with or without chemotherapy
Survival drops to 10%
Слайд 29Sinonasal Undifferentiated Carcinoma
Aggressive locally destructive lesion
Dependent on pathological differentiation from melanoma, lymphoma,
Sinonasal Undifferentiated Carcinoma
Aggressive locally destructive lesion
Dependent on pathological differentiation from melanoma, lymphoma,
Слайд 30Metastatic Tumors
Renal cell carcinoma is the most common
Palliative treatment only
Metastatic Tumors
Renal cell carcinoma is the most common
Palliative treatment only
Слайд 31Staging of Maxillary Sinus Tumors
Staging of Maxillary Sinus Tumors
Слайд 32Staging of Maxillary Sinus Tumors
T1: limited to antral mucosa without bony erosion
T2:
Staging of Maxillary Sinus Tumors
T1: limited to antral mucosa without bony erosion
T2:
Слайд 33Surgery
Unresectable tumors:
Superior extension: frontal lobes
Lateral extension: cavernous sinus
Posterior extension: prevertebral fascia
Bilateral optic
Surgery
Unresectable tumors:
Superior extension: frontal lobes
Lateral extension: cavernous sinus
Posterior extension: prevertebral fascia
Bilateral optic
Слайд 34Surgery
Surgical approaches:
Endoscopic
Lateral rhinotomy
Transoral/transpalatal
Midfacial degloving
Weber-Fergusson
Combined craniofacial approach
Extent of resection
Medial maxillectomy
Inferior maxillectomy
Total maxillectomy
Surgery
Surgical approaches:
Endoscopic
Lateral rhinotomy
Transoral/transpalatal
Midfacial degloving
Weber-Fergusson
Combined craniofacial approach
Extent of resection
Medial maxillectomy
Inferior maxillectomy
Total maxillectomy
Слайд 35Tracheostomy
130 maxillectomies only 7.7% required tracheostomy
Of those not receiving tracheostomy during surgery,
Tracheostomy
130 maxillectomies only 7.7% required tracheostomy
Of those not receiving tracheostomy during surgery,
Слайд 36Treatment of the Orbit
Before 1970’s orbital exenteration was included in the radical
Treatment of the Orbit
Before 1970’s orbital exenteration was included in the radical
Слайд 37Current indications for orbital exenteration
Involvement of the orbital apex
Involvement of the extraocular
Current indications for orbital exenteration
Involvement of the orbital apex
Involvement of the extraocular
Слайд 38Conclusions
Neoplasms of the nose and paranasal sinus are very rare and require
Conclusions
Neoplasms of the nose and paranasal sinus are very rare and require
 Электронное декларирование Подготовила: Межуева Дарья
Электронное декларирование Подготовила: Межуева Дарья Организационный план
Организационный план Ты стала большой
Ты стала большой Создание Единой нормативно-справочной информации по материально-техническим ресурсам в крупных компаниях. Актуальность, Шаги, Пр
Создание Единой нормативно-справочной информации по материально-техническим ресурсам в крупных компаниях. Актуальность, Шаги, Пр ОЦЕНКА ПЕРСОНАЛА В КОМПАНИИ
ОЦЕНКА ПЕРСОНАЛА В КОМПАНИИ Игровые технологии в процессе занятий физической культурой
Игровые технологии в процессе занятий физической культурой Evolution 9- сделано для профессионального фотографадополнение в линейке суперпопулярных рюкзаков Evolution 6 и Evolution 8
Evolution 9- сделано для профессионального фотографадополнение в линейке суперпопулярных рюкзаков Evolution 6 и Evolution 8 Психологические особенности детей с нарушениями речи
Психологические особенности детей с нарушениями речи Решение иррациональных уравнений (11 класс)
Решение иррациональных уравнений (11 класс) Кто такой турист
Кто такой турист Презентация на тему Баргузинский заповедник
Презентация на тему Баргузинский заповедник carevna__-lyagushka (1)
carevna__-lyagushka (1) Рациональное питание. Диеты
Рациональное питание. Диеты Русская матрешка 1 - 4 класс
Русская матрешка 1 - 4 класс ШКОЛЬНОЕ МЕТОДИЧЕСКОЕ ОБЪЕДИНЕНИЕ
ШКОЛЬНОЕ МЕТОДИЧЕСКОЕ ОБЪЕДИНЕНИЕ Астероиды - малые планеты
Астероиды - малые планеты Современные материалы в интерьере
Современные материалы в интерьере Путешествие на планету Математика
Путешествие на планету Математика После троянской войны беженцы отплыли от берегов Трои
После троянской войны беженцы отплыли от берегов Трои Что такое радуга?
Что такое радуга? Герои родного района
Герои родного района Формирование учебно-познавательной компетенции через овладение приемами действия в нестандартной ситуациях
Формирование учебно-познавательной компетенции через овладение приемами действия в нестандартной ситуациях «Весь мир у нас в руках, мы звезды континентов», - поют герои легендарного мюзикла «Бременские музыканты». А вместе с ними отлично п
«Весь мир у нас в руках, мы звезды континентов», - поют герои легендарного мюзикла «Бременские музыканты». А вместе с ними отлично п Фотодело. Маски. Торговые центры. Новый год
Фотодело. Маски. Торговые центры. Новый год Презентация на тему Диагностика метапредметных и предметных результатов с учетом требований ФГОС нового поколения
Презентация на тему Диагностика метапредметных и предметных результатов с учетом требований ФГОС нового поколения День семьи любви и верности
День семьи любви и верности Приключения «Ю»-класса...
Приключения «Ю»-класса... Презентация на тему Зороастризм
Презентация на тему Зороастризм