- Objectives

Содержание
- 2. Introduction
- 4. Definitions & Terminology Fertility: the capacity to reproduce or the state of being fertile. Fecundability: the
- 5. Definitions & Terminology Infertility: one year of unprotected coitus without conception. Primary infertility: couple who has
- 6. Epidemiology Fecundability rate in the general reproductive-aged population is fairly constant and is approximately 0.22 per
- 7. Fecundability 20-25% of couples will conceive/cycle. 50% should conceive after 3-4 months. 95% should conceive after
- 8. Infertility Affects 1 in 6 married couples of childbearing age Primary infertility : 58.6%. Secondary infertility:
- 9. Etiology of Infertility
- 10. Requirements for Normal Reproduction Release of a normal preovulatory oocyte. Production of adequate spermatozoa. Normal transport
- 11. Female Factor Infertility Female factor infertility can be divided into several categories: Cervical factor infertility Uterine
- 12. Cervical factor infertility Account for 5-10% of infertility. Can be caused by: Cervical stenosis Abnormalities of
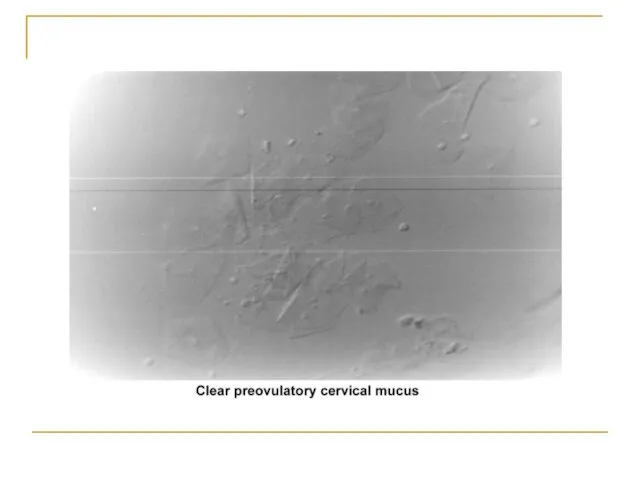
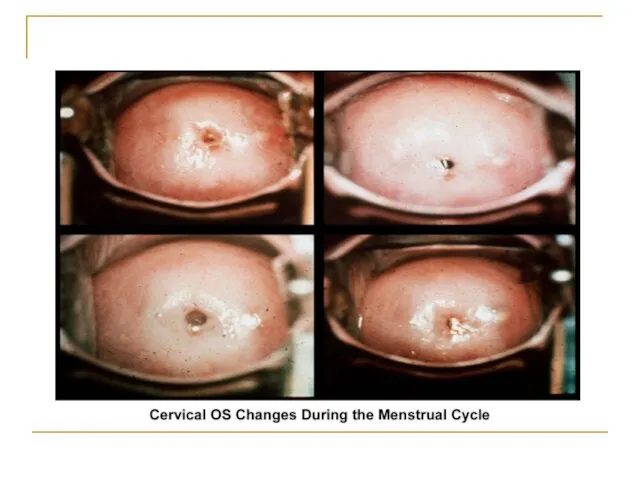
- 13. Cervical mucus production and characteristics It changes according to the estrogen concentration during the late follicular
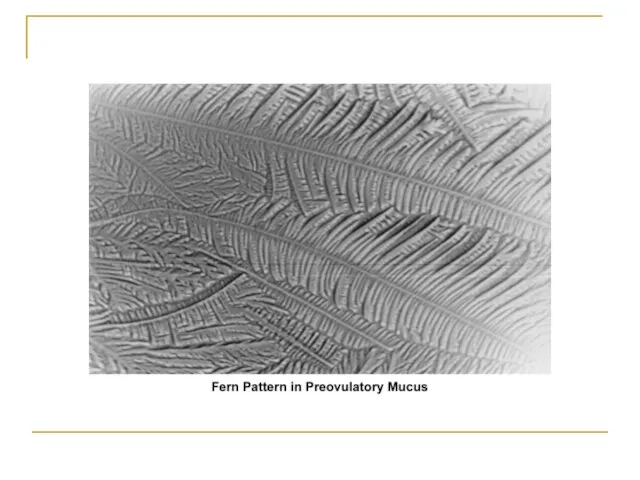
- 15. Cont,,, Secretion ↑ in mid follicular phase and reaches its maximum 24-48h before ovulation. Water and
- 17. Cont,,, The mucus organizes itself, forming multiple microchannels so the spermatozoa can travel through. Spermatozoa simultaneously
- 18. Cont,,, Mucus secretion may be altered by hormonal changes and medications, especially drugs like clomiphene citrate,
- 19. Cont,,, Cervical stenosis can cause infertility by blocking the passage of sperm from the cervix to
- 21. Uterine factor infertility May be associated with primary infertility or with pregnancy wastage and premature delivery.
- 22. Congenital defects The full spectrum of congenital/müllerian abnormalities varies from: Total absence of the uterus and
- 23. The most common uterine malformations observed during the past 40 years were drug induced. From the
- 24. Ddiethylstilbestrol (DES) DES was found to be responsible for inducing malformations of the uterine cervix, irregularities
- 25. Premature delivery has been associated with cervical incompetence. Unicornuate uterus associated with a blind horn, and
- 26. Acquired defects Endometritis associated with a traumatic delivery, dilatation and curettage, intrauterine device, or any instrumentation
- 27. Cont,,, Placental polyps may develop from placental remains. Intrauterine and submucosal fibroids are very common, affecting
- 28. Ovarian factor infertility Ovulatory dysfunction is defined as an alteration in the frequency and duration of
- 29. Tubal factors infertility Abnormalities or damage to the fallopian tube interferes with fertility and is responsible
- 30. Other tubal factors associated with infertility are either congenital or acquired. Congenital absence of the fallopian
- 31. Advanced age The prevalence of infertility rises dramatically as age increases. Fertility decreases with marriage duration
- 32. Peritoneal Factor Infertility Pelvic inflammatory disease Associated with gonorrhea and chlamydia infection . The rate of
- 33. Endometriosis Remains an enigmatic disease that affects women during their reproductive years. The evolution of the
- 35. Approach To Infertility and Evaluation of Infertile Couple
- 36. General Guidance on Evaluation of Infertility Infertility is a problem that involves both partners. The consultation
- 37. History Type of infertility (primary or secondary) Detailed history of previous pregnancies Specific questions: Frequency of
- 38. Female: menstrual history frequency patterns since menarche.
- 39. Male: semen analysis results history of impotence premature ejaculation change in libido history of testicular trauma
- 40. Ask the couple about: surgical contraception weight changes Lifestyle exercise medical treatment Smoking
- 41. Physical Body Mass Index skin evaluation of hair distribution Malformed face or limbs (congenital abnormalities) visual
- 42. Comprehensive Evaluation of Infertility Cervical factors Uterine factors Tubal and peritoneal factors Ovarian factors
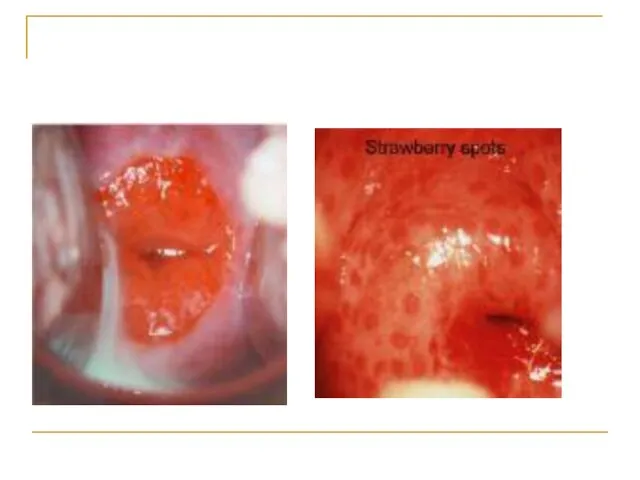
- 44. Cervical factors Congenital: Severe stenosis Inflammatory: chronic cervicitis Neoplastic causes: Cervical polyp or cervical fibroid. Cervical
- 46. Cervical factors The postcoital test: evaluating the amount of spermatozoa and its motility within the cervical
- 47. Uterine factors Congenital causes: Uterine aplasia, hypoplasia, septate uterus. Inflammatory causes: Tuberculous endometritis. Neoplastic causes: Fibroid
- 48. HSG pelvic ultrasonography Hysteroscopy MRI
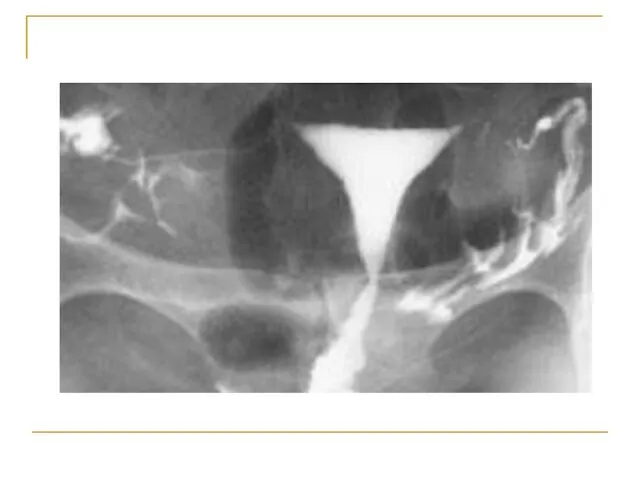
- 49. Hysterosalpingogram To evaluate: endocervical canal diameter and configuration of the internal os endometrial cavity uterine/tubal junction
- 50. The HSG should be performed during the early follicular phase. At this time, the endometrium is
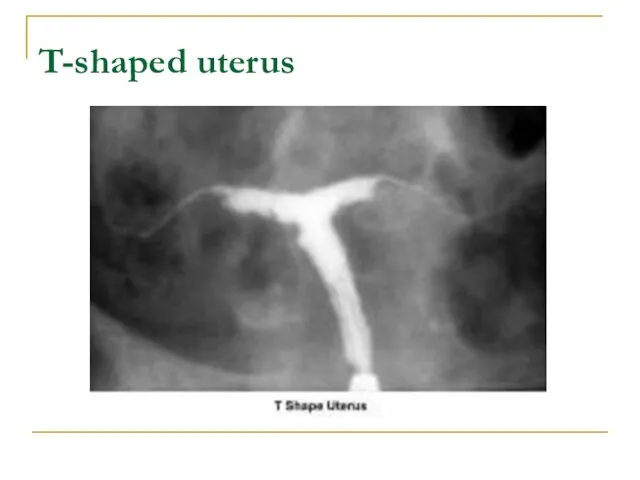
- 52. T-shaped uterus
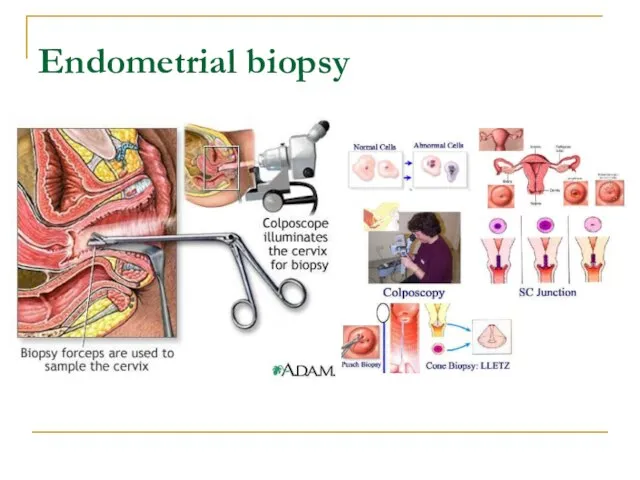
- 53. Endometrial biopsy
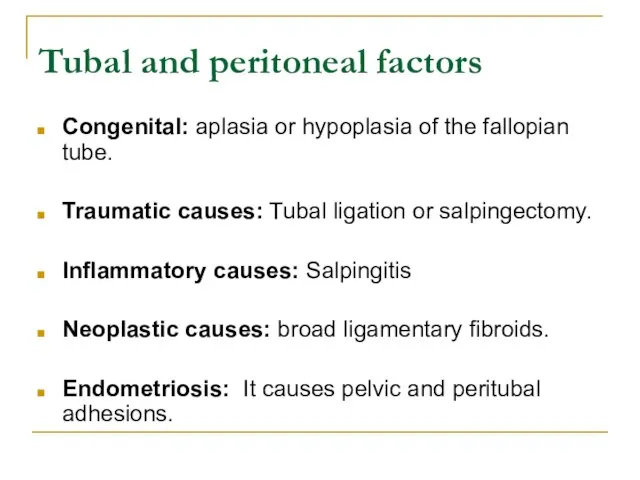
- 54. Tubal and peritoneal factors Congenital: aplasia or hypoplasia of the fallopian tube. Traumatic causes: Tubal ligation
- 55. Laparoscopy hysterosalpingogram
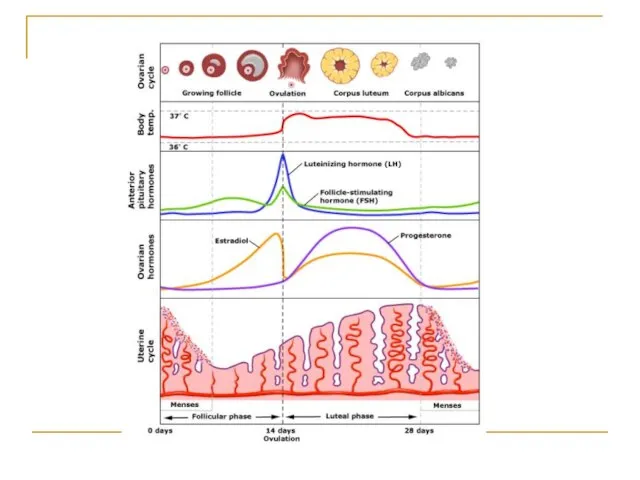
- 57. Ovarian factors Menstrual history Basal body temperature Hormone levels Blood levels of the hormone progesterone are
- 60. Evaluation of the Male Partner Semen analysis: The basic semen analysis assesses sperm concentration motility Morphology
- 61. Volume - 2-5 mL pH level - 7.2-7.8 Sperm concentration - 20 million or greater Motility
- 62. Interpretation of semen analysis Azoospermia indicates absence of sperm Oligozoospermia indicates a concentration of fewer than
- 63. Kruger criteria If the initial semen analysis is abnormal, the clinician will often request an additional
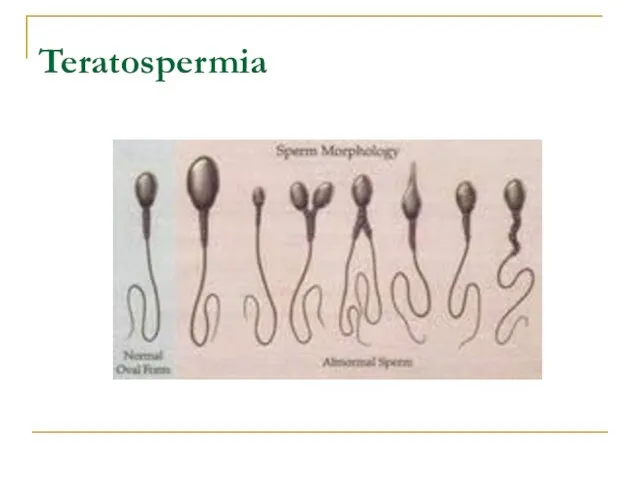
- 64. Teratospermia
- 65. Blood tests: to measure total testosterone, LH , FSH and prolactin may be ordered. Genetic tests:
- 66. Other tests If a blockage in the reproductive tract is suspected, a transrectal ultrasound test may
- 67. Infertility Treatment
- 68. Treatment of infertility depends on the cause, diagnosis, duration of infertility, age of the partners and
- 69. Restoring fertility: These approaches can involve steps related to the male or to the female, or
- 70. Treatment for men General sexual problems: Addressing impotence or premature ejaculation can improve fertility. Treatment for
- 71. Treatment for women Stimulating ovulation with fertility drugs: Fertility drugs are the main treatment for women
- 72. Commonly used fertility drugs include: Clomiphene citrate (Clomid, Serophene): Taken orally and stimulates ovulation in women
- 73. Human menopausal gonadotropin, or hMG (Repronex): This is an injected medication is for women who do
- 74. Follicle-stimulating hormone, or FSH (Gonal-F, Follistim, Bravelle): FSH works by stimulating the ovaries to mature egg
- 75. Gonadotropin-releasing hormone (Gn-RH) analogs: This treatment is for women with irregular ovulatory cycles or who ovulate
- 76. Letrozole (Femara): A class of medications called aromatase inhibitors, which are approved for treatment of advanced
- 77. Metformin (Glucophage): Oral drug taken to boost ovulation. It is used when insulin resistance is a
- 78. Bromocriptine: This medication is for women whose ovulation cycles are irregular due to elevated levels of
- 79. Fertility drugs and the risk of multiple pregnancies: Injectable fertility drugs increase the chance of multiple
- 80. The greater the number of fetuses, the higher the risk of premature labor. Babies born prematurely
- 81. If a woman requires an HCG injection to trigger ovulation, and ultrasound exams show that too
- 82. Surgery Depending on the cause, surgery may be a treatment option for infertility. Blockages or other
- 83. Assisted reproductive technology (ART)
- 84. Assisted reproductive technology (ART) ART has revolutionized the treatment of infertility. An ART health team includes
- 85. In Vitro Fertilization
- 86. Historical Perspective The first successful human IVF attempt resulted in the 1978 delivery of Louise Brown
- 87. Definition: In Vitro Fertilization is commonly referred to as IVF. It is the process of fertilization
- 88. When the IVF procedure is successful, the process is combined with a procedure known as embryo
- 89. Indications: Failed other treatments Tubal damage Significant male factor Absent uterus Carriers of genetic diseases Family
- 90. Method: There are basically five steps in the IVF and embryo transfer process which include the
- 91. 1. Ovarian stimulation Treatment cycles are typically started on the third day of menstruation. It consists
- 92. Typically approximately 10 days of injections will be necessary. Spontaneous ovulation during the cycle is typically
- 93. 2. Egg retrieval When follicular maturation is judged to be adequate, human chorionic gonadotropin (hCG) is
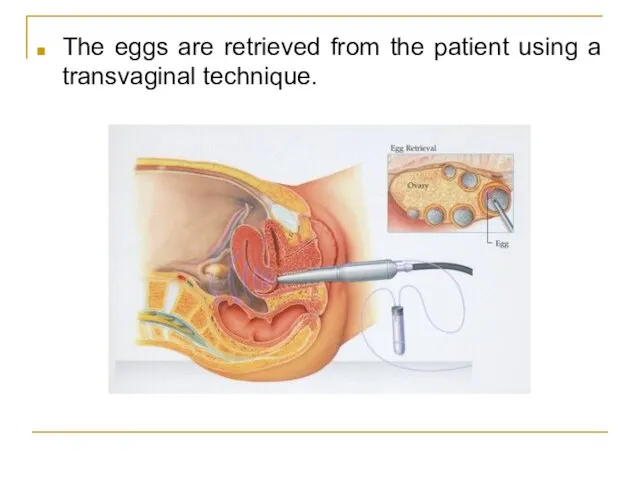
- 94. The eggs are retrieved from the patient using a transvaginal technique.
- 95. Through this needle follicles can be aspirated, and the follicular fluid is handed to the IVF
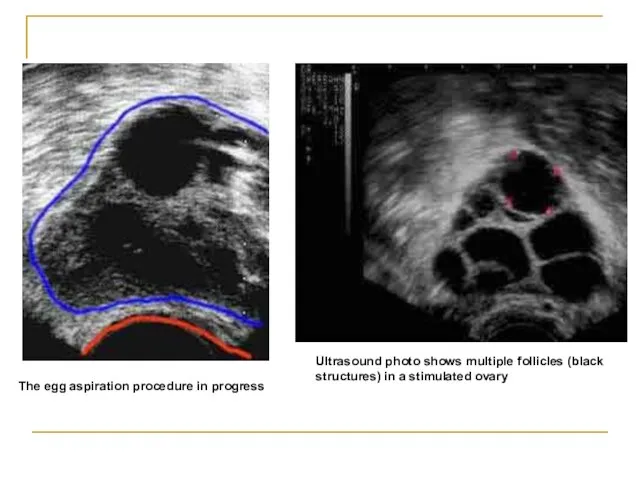
- 96. Ultrasound photo shows multiple follicles (black structures) in a stimulated ovary The egg aspiration procedure in
- 97. 3. Fertilization In the laboratory, the identified eggs are stripped of surrounding cells and prepared for
- 98. In most cases, the egg will be fertilized by that time and the fertilized egg will
- 99. Picture of IVF egg showing fertilization process
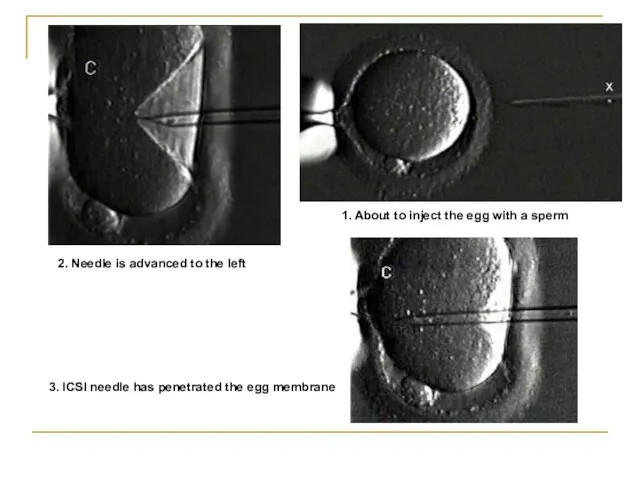
- 100. 1. About to inject the egg with a sperm 2. Needle is advanced to the left
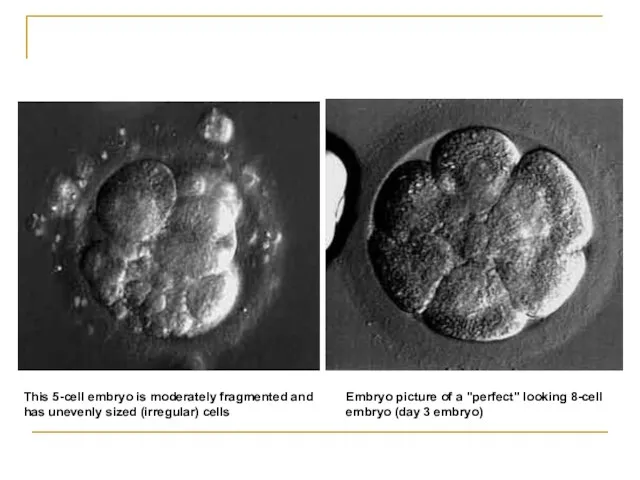
- 101. 4. Selection Typically, embryos that have reached the 6-8 cell stage are transferred three days after
- 102. Embryo picture of a "perfect" looking 8-cell embryo (day 3 embryo) This 5-cell embryo is moderately
- 103. 5. Embryo transfer Embryos are graded by the embryologist based on the number of cells, evenness
- 104. In countries such as the UK, Australia and New Zealand, a maximum of two embryos are
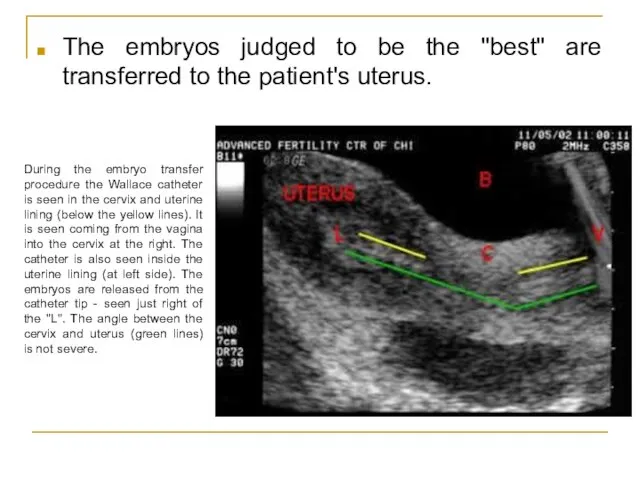
- 105. The embryos judged to be the "best" are transferred to the patient's uterus. During the embryo
- 106. What Happens to the Other Embryos? Freeze Embryos Donate For Research/Stem Cells Embryo Adoption Discard!
- 107. Pregnancy Rates For IVF, it is the percentage of all attempts that lead to pregnancy. With
- 108. Complications The major complication of IVF is the risk of multiple births. Multiple births are related
- 109. A double blind, randomized study followed IVF pregnancies that resulted in 73 infants (33 boys and
- 110. Another risk of ovarian stimulation is the development of ovarian hyperstimulation syndrome. In 2008, an analysis
- 111. Special IVF Procedures PGD PGD (Preimplantation Genetic Diagnosis) can be performed on embryos before the embryo
- 112. Special IVF Procedures ZIFT In the process of ZIFT (Zygote Intrafallopian Transfer), eggs are removed from
- 113. References: Hacker & Moore's Essentials of Obstetrics and Gynecology www.emedicine.medscape.com/article/274143-overview http://www.mayoclinic.com/health/infertility/ds00310 UpToDate www.ncbi.org http://en.wikipedia.org/wiki/Infertility
- 115. Скачать презентацию
Слайд 4Definitions & Terminology
Fertility: the capacity to reproduce or the state of
Definitions & Terminology
Fertility: the capacity to reproduce or the state of
Слайд 5Definitions & Terminology
Infertility: one year of unprotected coitus without conception.
Primary infertility:
Definitions & Terminology
Infertility: one year of unprotected coitus without conception.
Primary infertility:
Слайд 6Epidemiology
Fecundability rate in the general reproductive-aged population is fairly constant and is
Epidemiology
Fecundability rate in the general reproductive-aged population is fairly constant and is
Слайд 7Fecundability
20-25% of couples will conceive/cycle.
50% should conceive after 3-4 months.
95% should conceive
Fecundability
20-25% of couples will conceive/cycle.
50% should conceive after 3-4 months.
95% should conceive
Слайд 8Infertility
Affects 1 in 6 married couples of childbearing age
Primary infertility :
Infertility
Affects 1 in 6 married couples of childbearing age
Primary infertility :
Слайд 9Etiology of Infertility
Etiology of Infertility
Слайд 10Requirements for Normal Reproduction
Release of a normal preovulatory oocyte.
Production of
Requirements for Normal Reproduction
Release of a normal preovulatory oocyte.
Production of
Слайд 11Female Factor Infertility
Female factor infertility can be divided into several categories:
Female Factor Infertility
Female factor infertility can be divided into several categories:
Слайд 12Cervical factor infertility
Account for 5-10% of infertility.
Can be caused by:
Cervical stenosis
Abnormalities
Cervical factor infertility
Account for 5-10% of infertility.
Can be caused by:
Cervical stenosis
Abnormalities
Слайд 13Cervical mucus production and characteristics
It changes according to the estrogen concentration during
Cervical mucus production and characteristics
It changes according to the estrogen concentration during
Слайд 15Cont,,,
Secretion ↑ in mid follicular phase and reaches its maximum 24-48h before
Cont,,,
Secretion ↑ in mid follicular phase and reaches its maximum 24-48h before
Слайд 17Cont,,,
The mucus organizes itself, forming multiple microchannels so the spermatozoa can travel
Cont,,,
The mucus organizes itself, forming multiple microchannels so the spermatozoa can travel
Слайд 18Cont,,,
Mucus secretion may be altered by hormonal changes and medications, especially drugs
Cont,,,
Mucus secretion may be altered by hormonal changes and medications, especially drugs
Слайд 19Cont,,,
Cervical stenosis can cause infertility by blocking the passage of sperm from
Cont,,,
Cervical stenosis can cause infertility by blocking the passage of sperm from
Слайд 21Uterine factor infertility
May be associated with primary infertility or with pregnancy wastage
Uterine factor infertility
May be associated with primary infertility or with pregnancy wastage
Слайд 22Congenital defects
The full spectrum of congenital/müllerian abnormalities varies from:
Total absence of
Congenital defects
The full spectrum of congenital/müllerian abnormalities varies from:
Total absence of
Слайд 23The most common uterine malformations observed during the past 40 years were
Слайд 24Ddiethylstilbestrol (DES)
DES was found to be responsible for inducing malformations of the
Ddiethylstilbestrol (DES)
DES was found to be responsible for inducing malformations of the
Слайд 25Premature delivery has been associated with cervical incompetence.
Unicornuate uterus associated with a
Premature delivery has been associated with cervical incompetence.
Unicornuate uterus associated with a
Слайд 26Acquired defects
Endometritis associated with a traumatic delivery, dilatation and curettage, intrauterine device,
Acquired defects
Endometritis associated with a traumatic delivery, dilatation and curettage, intrauterine device,
Слайд 27Cont,,,
Placental polyps may develop from placental remains.
Intrauterine and submucosal fibroids are very
Cont,,,
Placental polyps may develop from placental remains.
Intrauterine and submucosal fibroids are very
Слайд 28Ovarian factor infertility
Ovulatory dysfunction is defined as an alteration in the frequency
Ovarian factor infertility
Ovulatory dysfunction is defined as an alteration in the frequency
Слайд 29Tubal factors infertility
Abnormalities or damage to the fallopian tube interferes with fertility
Tubal factors infertility
Abnormalities or damage to the fallopian tube interferes with fertility
Слайд 30Other tubal factors associated with infertility are either congenital or acquired.
Congenital
Other tubal factors associated with infertility are either congenital or acquired.
Congenital
Слайд 31Advanced age
The prevalence of infertility rises dramatically as age increases.
Fertility decreases with
Advanced age
The prevalence of infertility rises dramatically as age increases.
Fertility decreases with
Слайд 32Peritoneal Factor Infertility
Pelvic inflammatory disease
Associated with gonorrhea and chlamydia infection .
The rate
Peritoneal Factor Infertility
Pelvic inflammatory disease
Associated with gonorrhea and chlamydia infection .
The rate
Слайд 33Endometriosis
Remains an enigmatic disease that affects women during their reproductive years.
The evolution
Endometriosis
Remains an enigmatic disease that affects women during their reproductive years.
The evolution
Слайд 35Approach To Infertility and Evaluation of Infertile Couple
Слайд 36General Guidance on Evaluation of Infertility
Infertility is a problem that involves both
General Guidance on Evaluation of Infertility
Infertility is a problem that involves both
Слайд 37History
Type of infertility (primary or secondary)
Detailed history of previous pregnancies
Specific questions:
Frequency of
History
Type of infertility (primary or secondary)
Detailed history of previous pregnancies
Specific questions:
Frequency of
Слайд 38Female:
menstrual history
frequency
patterns since menarche.
Female:
menstrual history
frequency
patterns since menarche.
Слайд 39Male:
semen analysis results
history of impotence
premature ejaculation
change in libido
history of testicular trauma
Infections
Male:
semen analysis results
history of impotence
premature ejaculation
change in libido
history of testicular trauma
Infections
Слайд 40Ask the couple about:
surgical contraception
weight changes
Lifestyle
exercise
medical treatment
Smoking
Ask the couple about:
surgical contraception
weight changes
Lifestyle
exercise
medical treatment
Smoking
Слайд 41Physical
Body Mass Index
skin
evaluation of hair distribution
Malformed face or limbs (congenital abnormalities)
visual
Physical
Body Mass Index
skin
evaluation of hair distribution
Malformed face or limbs (congenital abnormalities)
visual
Слайд 42Comprehensive Evaluation of Infertility
Cervical factors
Uterine factors
Tubal and peritoneal factors
Ovarian factors
Comprehensive Evaluation of Infertility
Cervical factors
Uterine factors
Tubal and peritoneal factors
Ovarian factors
Слайд 44Cervical factors
Congenital: Severe stenosis
Inflammatory: chronic cervicitis
Neoplastic causes: Cervical polyp or cervical
Cervical factors
Congenital: Severe stenosis
Inflammatory: chronic cervicitis
Neoplastic causes: Cervical polyp or cervical
Слайд 46Cervical factors
The postcoital test: evaluating the amount of spermatozoa and its motility
Cervical factors
The postcoital test: evaluating the amount of spermatozoa and its motility
Слайд 47Uterine factors
Congenital causes: Uterine aplasia, hypoplasia, septate uterus.
Inflammatory causes: Tuberculous endometritis.
Uterine factors
Congenital causes: Uterine aplasia, hypoplasia, septate uterus.
Inflammatory causes: Tuberculous endometritis.
Слайд 48HSG
pelvic ultrasonography
Hysteroscopy
MRI
HSG
pelvic ultrasonography
Hysteroscopy
MRI
Слайд 49Hysterosalpingogram
To evaluate:
endocervical canal
diameter and configuration of the internal os
endometrial cavity
uterine/tubal junction
diameter, location,
Hysterosalpingogram
To evaluate:
endocervical canal
diameter and configuration of the internal os
endometrial cavity
uterine/tubal junction
diameter, location,
Слайд 50The HSG should be performed during the early follicular phase.
At this time,
The HSG should be performed during the early follicular phase.
At this time,
Слайд 52T-shaped uterus
T-shaped uterus
Слайд 53Endometrial biopsy
Endometrial biopsy
Слайд 54Tubal and peritoneal factors
Congenital: aplasia or hypoplasia of the fallopian tube.
Traumatic
Tubal and peritoneal factors
Congenital: aplasia or hypoplasia of the fallopian tube.
Traumatic
Слайд 55Laparoscopy
hysterosalpingogram
Laparoscopy
hysterosalpingogram
Слайд 57Ovarian factors
Menstrual history
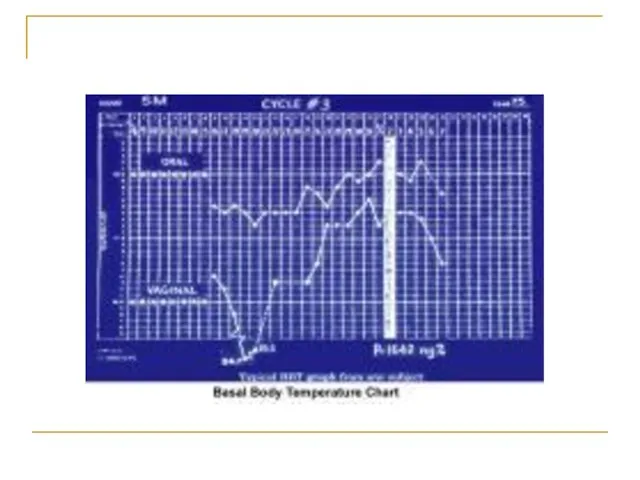
Basal body temperature
Hormone levels
Blood levels of the hormone progesterone are
Ovarian factors
Menstrual history
Basal body temperature
Hormone levels
Blood levels of the hormone progesterone are
Слайд 60Evaluation of the Male Partner
Semen analysis:
The basic semen analysis assesses
sperm concentration
motility
Morphology
viability.
Evaluation of the Male Partner
Semen analysis:
The basic semen analysis assesses
sperm concentration
motility
Morphology
viability.
Слайд 61Volume - 2-5 mL
pH level - 7.2-7.8
Sperm concentration - 20 million or
pH level - 7.2-7.8
Sperm concentration - 20 million or
Слайд 62Interpretation of semen analysis
Azoospermia indicates absence of sperm
Oligozoospermia indicates a concentration of
Interpretation of semen analysis
Azoospermia indicates absence of sperm
Oligozoospermia indicates a concentration of
Слайд 63Kruger criteria
If the initial semen analysis is abnormal, the clinician will often
Kruger criteria
If the initial semen analysis is abnormal, the clinician will often
Слайд 64Teratospermia
Teratospermia
Слайд 65Blood tests: to measure total testosterone, LH , FSH and prolactin may
Blood tests: to measure total testosterone, LH , FSH and prolactin may
Слайд 66Other tests
If a blockage in the reproductive tract is suspected, a transrectal
Other tests
If a blockage in the reproductive tract is suspected, a transrectal
Слайд 67Infertility Treatment
Слайд 68Treatment of infertility depends on the cause, diagnosis, duration of infertility, age
Treatment of infertility depends on the cause, diagnosis, duration of infertility, age
Слайд 69Restoring fertility: These approaches can involve steps related to the male or
Restoring fertility: These approaches can involve steps related to the male or
Слайд 70Treatment for men
General sexual problems: Addressing impotence or premature ejaculation can
Treatment for men
General sexual problems: Addressing impotence or premature ejaculation can
Слайд 71Treatment for women
Stimulating ovulation with fertility drugs:
Fertility drugs are the main treatment
Treatment for women
Stimulating ovulation with fertility drugs:
Fertility drugs are the main treatment
Слайд 72Commonly used fertility drugs include:
Clomiphene citrate (Clomid, Serophene):
Taken orally and stimulates
Commonly used fertility drugs include:
Clomiphene citrate (Clomid, Serophene):
Taken orally and stimulates
Слайд 73Human menopausal gonadotropin, or hMG (Repronex):
This is an injected medication is for
Human menopausal gonadotropin, or hMG (Repronex):
This is an injected medication is for
Слайд 74Follicle-stimulating hormone, or FSH (Gonal-F, Follistim, Bravelle):
FSH works by stimulating the ovaries
Follicle-stimulating hormone, or FSH (Gonal-F, Follistim, Bravelle):
FSH works by stimulating the ovaries
Слайд 75Gonadotropin-releasing hormone (Gn-RH) analogs:
This treatment is for women with irregular ovulatory cycles
Gonadotropin-releasing hormone (Gn-RH) analogs:
This treatment is for women with irregular ovulatory cycles
Слайд 76Letrozole (Femara):
A class of medications called aromatase inhibitors, which are approved for
Letrozole (Femara):
A class of medications called aromatase inhibitors, which are approved for
Слайд 77Metformin (Glucophage):
Oral drug taken to boost ovulation.
It is used when insulin resistance
Metformin (Glucophage):
Oral drug taken to boost ovulation.
It is used when insulin resistance
Слайд 78Bromocriptine:
This medication is for women whose ovulation cycles are irregular due to
Bromocriptine:
This medication is for women whose ovulation cycles are irregular due to
Слайд 79Fertility drugs and the risk of multiple pregnancies:
Injectable fertility drugs increase the
Fertility drugs and the risk of multiple pregnancies:
Injectable fertility drugs increase the
Слайд 80The greater the number of fetuses, the higher the risk of premature
The greater the number of fetuses, the higher the risk of premature
Слайд 81If a woman requires an HCG injection to trigger ovulation, and ultrasound
If a woman requires an HCG injection to trigger ovulation, and ultrasound
Слайд 82Surgery
Depending on the cause, surgery may be a treatment option for infertility.
Surgery
Depending on the cause, surgery may be a treatment option for infertility.
Слайд 83Assisted reproductive technology (ART)
Assisted reproductive technology (ART)
Слайд 84Assisted reproductive technology (ART)
ART has revolutionized the treatment of infertility.
An ART health
Assisted reproductive technology (ART)
ART has revolutionized the treatment of infertility.
An ART health
Слайд 85In Vitro Fertilization
In Vitro Fertilization
Слайд 86Historical Perspective
The first successful human IVF attempt resulted in the 1978 delivery
Historical Perspective
The first successful human IVF attempt resulted in the 1978 delivery
Слайд 87Definition:
In Vitro Fertilization is commonly referred to as IVF.
It is the
Definition:
In Vitro Fertilization is commonly referred to as IVF.
It is the
Слайд 88When the IVF procedure is successful, the process is combined with a
When the IVF procedure is successful, the process is combined with a
Слайд 89Indications:
Failed other treatments
Tubal damage
Significant male factor
Absent uterus
Carriers of genetic diseases
Family Balancing
Cancer patients
Indications:
Failed other treatments
Tubal damage
Significant male factor
Absent uterus
Carriers of genetic diseases
Family Balancing
Cancer patients
Слайд 90Method:
There are basically five steps in the IVF and embryo transfer process
Method:
There are basically five steps in the IVF and embryo transfer process
Слайд 911. Ovarian stimulation
Treatment cycles are typically started on the third day of
1. Ovarian stimulation
Treatment cycles are typically started on the third day of
Слайд 92Typically approximately 10 days of injections will be necessary.
Spontaneous ovulation during
Typically approximately 10 days of injections will be necessary.
Spontaneous ovulation during
Слайд 932. Egg retrieval
When follicular maturation is judged to be adequate, human chorionic
2. Egg retrieval
When follicular maturation is judged to be adequate, human chorionic
Слайд 94The eggs are retrieved from the patient using a transvaginal technique.
The eggs are retrieved from the patient using a transvaginal technique.
Слайд 95Through this needle follicles can be aspirated, and the follicular fluid is
Through this needle follicles can be aspirated, and the follicular fluid is
Слайд 96Ultrasound photo shows multiple follicles (black structures) in a stimulated ovary
The egg
Ultrasound photo shows multiple follicles (black structures) in a stimulated ovary
The egg
Слайд 973. Fertilization
In the laboratory, the identified eggs are stripped of surrounding cells
3. Fertilization
In the laboratory, the identified eggs are stripped of surrounding cells
Слайд 98In most cases, the egg will be fertilized by that time and
In most cases, the egg will be fertilized by that time and
Слайд 99Picture of IVF egg showing fertilization process
Picture of IVF egg showing fertilization process
Слайд 1001. About to inject the egg with a sperm
2. Needle is
1. About to inject the egg with a sperm
2. Needle is
Слайд 1014. Selection
Typically, embryos that have reached the 6-8 cell stage are transferred
4. Selection
Typically, embryos that have reached the 6-8 cell stage are transferred
Слайд 102Embryo picture of a "perfect" looking 8-cell embryo (day 3 embryo)
This 5-cell
Embryo picture of a "perfect" looking 8-cell embryo (day 3 embryo)
This 5-cell
Слайд 1035. Embryo transfer
Embryos are graded by the embryologist based on the number
5. Embryo transfer
Embryos are graded by the embryologist based on the number
Слайд 104In countries such as the UK, Australia and New Zealand, a maximum
In countries such as the UK, Australia and New Zealand, a maximum
Слайд 105The embryos judged to be the "best" are transferred to the patient's
The embryos judged to be the "best" are transferred to the patient's
Слайд 106What Happens to the Other Embryos?
Freeze Embryos
Donate For Research/Stem Cells
Embryo Adoption
Discard!
What Happens to the Other Embryos?
Freeze Embryos
Donate For Research/Stem Cells
Embryo Adoption
Discard!
Слайд 107Pregnancy Rates
For IVF, it is the percentage of all attempts that lead
Pregnancy Rates
For IVF, it is the percentage of all attempts that lead
Слайд 108Complications
The major complication of IVF is the risk of multiple births.
Multiple births
Complications
The major complication of IVF is the risk of multiple births.
Multiple births
Слайд 109A double blind, randomized study followed IVF pregnancies that resulted in 73
A double blind, randomized study followed IVF pregnancies that resulted in 73
Слайд 110Another risk of ovarian stimulation is the development of ovarian hyperstimulation syndrome.
In
Another risk of ovarian stimulation is the development of ovarian hyperstimulation syndrome.
In
Слайд 111Special IVF Procedures
PGD
PGD (Preimplantation Genetic Diagnosis) can be performed on embryos before
Special IVF Procedures
PGD
PGD (Preimplantation Genetic Diagnosis) can be performed on embryos before
Слайд 112Special IVF Procedures
ZIFT
In the process of ZIFT (Zygote Intrafallopian Transfer), eggs are
Special IVF Procedures
ZIFT
In the process of ZIFT (Zygote Intrafallopian Transfer), eggs are
Слайд 113References:
Hacker & Moore's Essentials of Obstetrics and Gynecology
www.emedicine.medscape.com/article/274143-overview
http://www.mayoclinic.com/health/infertility/ds00310
UpToDate
www.ncbi.org
http://en.wikipedia.org/wiki/Infertility
References:
Hacker & Moore's Essentials of Obstetrics and Gynecology
www.emedicine.medscape.com/article/274143-overview
http://www.mayoclinic.com/health/infertility/ds00310
UpToDate
www.ncbi.org
http://en.wikipedia.org/wiki/Infertility
 Political systems of the world and the Nenets autonomous okrug
Political systems of the world and the Nenets autonomous okrug АРЕНДА БЕТОНОНАСОСОВ
АРЕНДА БЕТОНОНАСОСОВ Презентация на тему В экваториальном лесу Южной Америки
Презентация на тему В экваториальном лесу Южной Америки Работа с бумагой
Работа с бумагой Большая китайская панда
Большая китайская панда Совещание с Дистрибьюторами г.Москва в рамках регионального совещания в г.Москва
Совещание с Дистрибьюторами г.Москва в рамках регионального совещания в г.Москва Крестики – нолики
Крестики – нолики Реконструкция Политехнического музея
Реконструкция Политехнического музея Блюдо из птицы
Блюдо из птицы Е.Л. Николаева Президент НАМИКС
Е.Л. Николаева Президент НАМИКС Казачество
Казачество 3. Types of Computer
3. Types of Computer Курс «Взаимодействие с заинтересованными сторонами и планирование деятельности в соответствии со стандартом AA1000 SES»
Курс «Взаимодействие с заинтересованными сторонами и планирование деятельности в соответствии со стандартом AA1000 SES» Эскиз
Эскиз «Оценивание программ и политик: методология и применение» - от межфакультетского семинара (2004-2005) к общегородскому коллоквиуму И
«Оценивание программ и политик: методология и применение» - от межфакультетского семинара (2004-2005) к общегородскому коллоквиуму И Мастер-класс Рисование пластилином картин
Мастер-класс Рисование пластилином картин Комплекс по сжижению, хранению и отгрузке СПГ в районе КС Портовая (Ленинградская область)
Комплекс по сжижению, хранению и отгрузке СПГ в районе КС Портовая (Ленинградская область) Новое похождения выпускников, или удивительное путешествие по океану знаний
Новое похождения выпускников, или удивительное путешествие по океану знаний Режимы электроэнергетических систем
Режимы электроэнергетических систем ратцель
ратцель Сравнительный анализ стандартов по географии 8-9 классы
Сравнительный анализ стандартов по географии 8-9 классы Зачем нам нужны растения?
Зачем нам нужны растения? Автоматическое повторное включение
Автоматическое повторное включение ИССЛЕДОВАНИЕ ТЕКСТОВ, ВЫПОЛНЕННЫХ «ПЕЧАТНЫМ» ПОЧЕРКОМ
ИССЛЕДОВАНИЕ ТЕКСТОВ, ВЫПОЛНЕННЫХ «ПЕЧАТНЫМ» ПОЧЕРКОМ МАОУ СОШ №91
МАОУ СОШ №91 Р-даы олданыстаы мырышты-орасынды байыту
Р-даы олданыстаы мырышты-орасынды байыту Детство без границ. Юбилею школы Горького посвящается
Детство без границ. Юбилею школы Горького посвящается Паремии
Паремии