- Penetrating Neck Trauma

Содержание
- 2. Introduction 5-10% of all trauma Overall mortality rate as high as 11% Major vessel injury fatal
- 3. Historical Perspective/ pre WW I Ligation of the major vessels described as early as 1522 by
- 4. Historical / post WW II Mandatory exploration of all penetrating neck wounds, through the platysma Fogelman
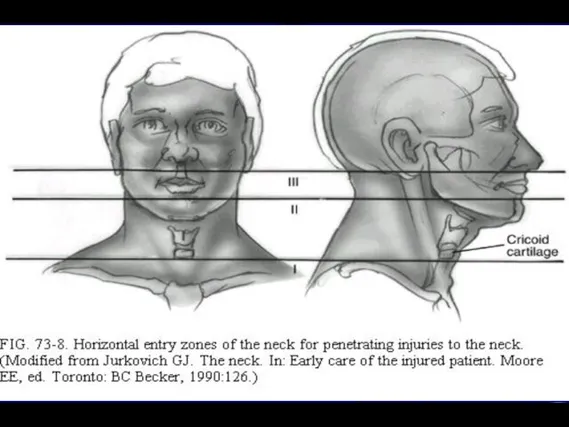
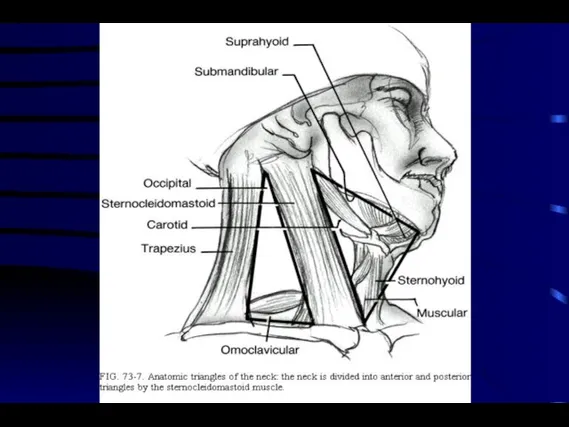
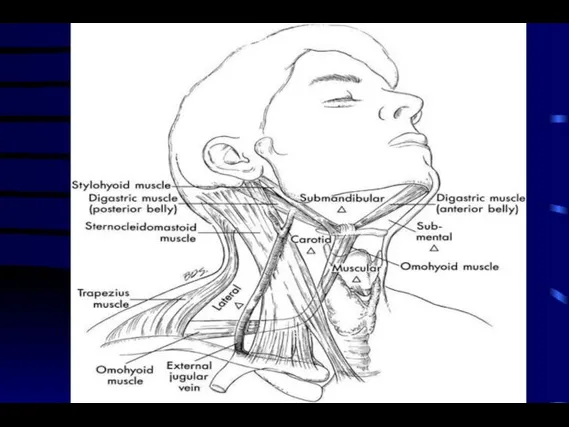
- 6. Anatomy/Zone I Bound superiorly by the cricoid and inferiorly by the sternum and clavicles Contains the
- 7. Anatomy/Zone II Bound inferiorly by the cricoid and superiorly by the angle of the mandible Contains
- 8. Anatomy/Zone III Lies above the angle of the mandible Contains the internal and external carotid arteries,
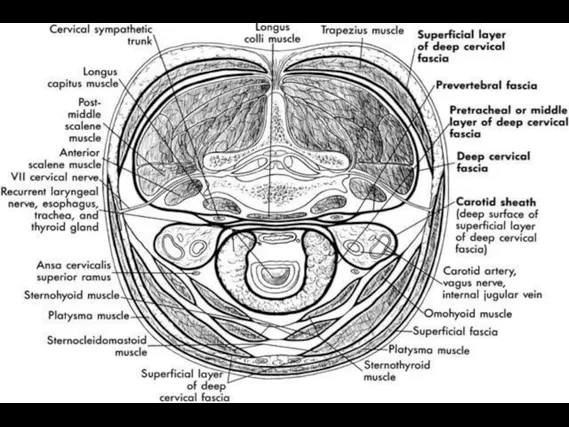
- 9. Fascial Layers Superficial cervical fascia - platysma Deep cervical fascia Investing: sternocleidomastoid muscle, trapezius muscle Pretracheal:
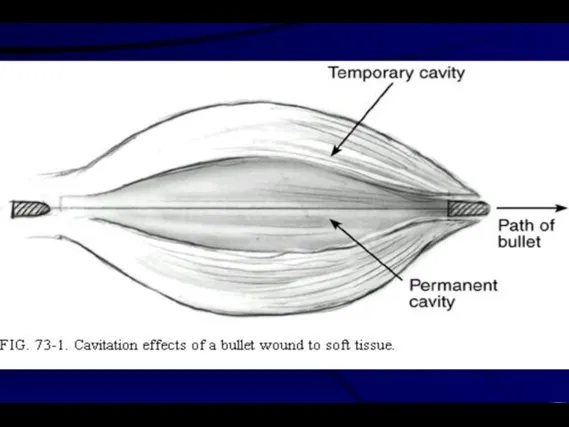
- 13. Ballistics Over 95% of penetrating neck wounds are from guns and knives, remainder from motor vehicle,
- 14. Ballistic cont... Muzzle velocity less than 1000 ft/s ( 610 m/s ) is considered low velocity
- 15. Ballistic cont. Injuries inflicted with high power rifles, shotguns at less than 20 feet, and .357
- 18. Stabilization/Airway Established Airway be prepared to obtain an airway emergently intubation or cricothyrotomy beware of cutting
- 19. Breathing Zone I injuries with concomitant thoracic injuries pneumothorax hemopneumothorax tension pneumothorax
- 20. Circulation Bleeding should be controlled by pressure Do not clamp blindly or probe the wound depths
- 21. History Obtain from EMS witnesses, patient Mechanisms of injury - stab wounds, gunshot wound, high-energy, low-energy,
- 22. Physical Examination Thorough head and neck exam using palpation and stethoscope to search for thrills and
- 23. Radiographs CXR - inspiratory/expiratory films to assess for phrenic nerve injury, look for pneumothorax Cervical spine
- 24. Preoperative Preparation Surgeon and staff ready for emergent/urgent tracheotomy Gentle cleansing of wound, betadine paint only
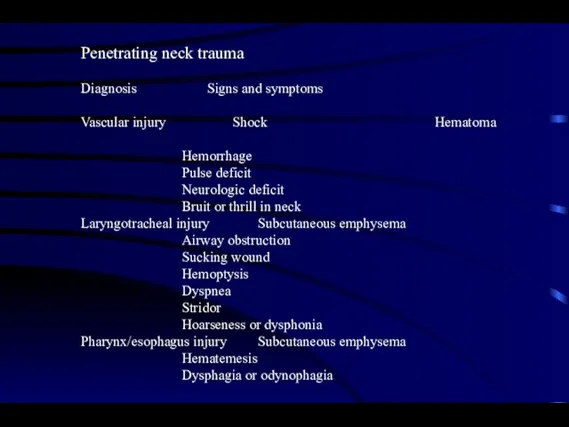
- 25. Penetrating neck trauma Diagnosis Signs and symptoms Vascular injury Shock Hematoma Hemorrhage Pulse deficit Neurologic deficit
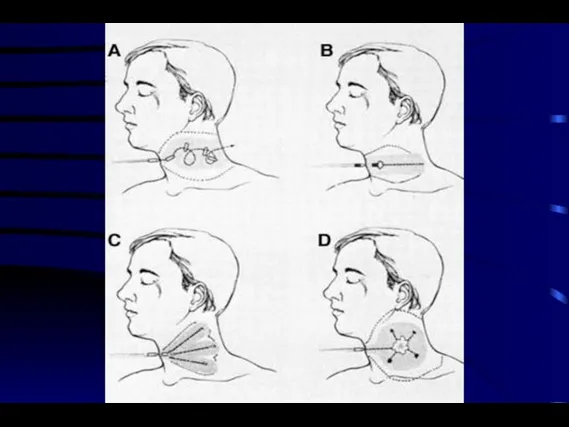
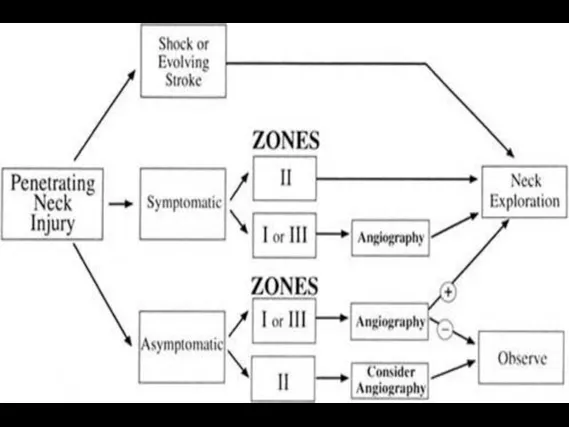
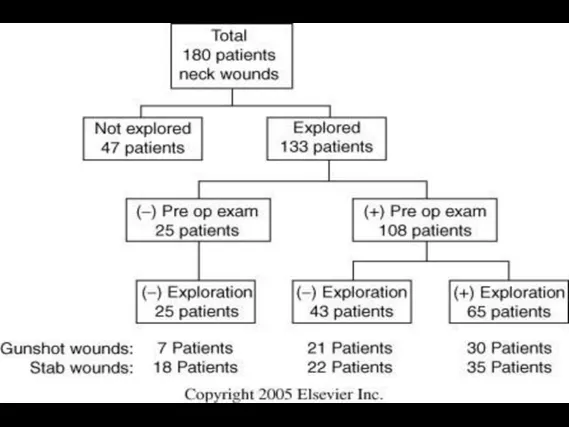
- 26. Exploration vs. Observation Many experts have adopted a policy of selective exploration Decreased number of negative
- 29. Site/Zone I Adequate exposure for exploration and repair may require sternotomy, clavicle resection, or thoracotomy High
- 30. Site/Zone II Few injuries will escape clinical examination Most carotid injuries occur here Adjunctive studies, except
- 31. Site/Zone III High rate of vascular injury, often multiple Often difficult to obtain proximal and distal
- 32. Clinical Setting Observation requires admission to an intensive care unit where serial examination can be performed
- 33. Pharyngo Esophageal Gastrografin swallow followed by Barium if negative Flexible ± rigid esophagoscopy Invert the mucosal
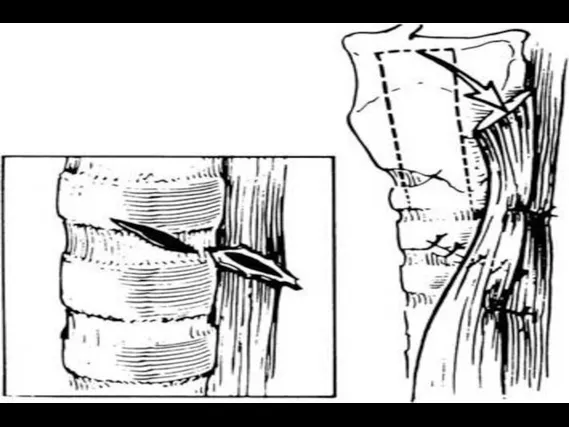
- 35. Airway DL where laryngeal injury is suspected Mucosal tears are closed with absorbable sutures Cover raw
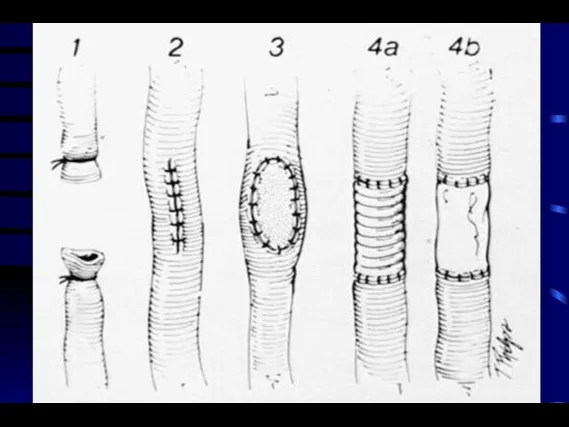
- 36. Vascular The subclavian and internal jugular veins can be ligated without adverse effect Major arteries should
- 39. Vascular cont. When tension is required, vein grafts from the sphenous or internal jugular are interposed
- 41. Conclusions Maintain a healthy respect for apparently minor neck wounds because of potential fatal outcome for
- 45. Скачать презентацию
Слайд 3Historical Perspective/ pre WW I
Ligation of the major vessels described as early
Historical Perspective/ pre WW I
Ligation of the major vessels described as early
Слайд 4Historical / post WW II
Mandatory exploration of all penetrating neck wounds, through
Historical / post WW II
Mandatory exploration of all penetrating neck wounds, through
Слайд 6Anatomy/Zone I
Bound superiorly by the cricoid and inferiorly by the sternum and
Anatomy/Zone I
Bound superiorly by the cricoid and inferiorly by the sternum and
Слайд 7Anatomy/Zone II
Bound inferiorly by the cricoid and superiorly by the angle of
Anatomy/Zone II
Bound inferiorly by the cricoid and superiorly by the angle of
Слайд 8Anatomy/Zone III
Lies above the angle of the mandible
Contains the internal and external
Anatomy/Zone III
Lies above the angle of the mandible
Contains the internal and external
Слайд 9Fascial Layers
Superficial cervical fascia - platysma
Deep cervical fascia
Investing: sternocleidomastoid muscle, trapezius muscle
Pretracheal:
Fascial Layers
Superficial cervical fascia - platysma
Deep cervical fascia
Investing: sternocleidomastoid muscle, trapezius muscle
Pretracheal:
Слайд 13Ballistics
Over 95% of penetrating neck wounds are from guns and knives, remainder
Ballistics
Over 95% of penetrating neck wounds are from guns and knives, remainder
Слайд 14Ballistic cont...
Muzzle velocity less than 1000 ft/s ( 610 m/s ) is
Ballistic cont...
Muzzle velocity less than 1000 ft/s ( 610 m/s ) is
Слайд 15Ballistic cont.
Injuries inflicted with high power rifles, shotguns at less than 20
Ballistic cont.
Injuries inflicted with high power rifles, shotguns at less than 20
Слайд 18Stabilization/Airway
Established Airway
be prepared to obtain an airway emergently
intubation or cricothyrotomy
beware of cutting
Stabilization/Airway
Established Airway
be prepared to obtain an airway emergently
intubation or cricothyrotomy
beware of cutting
Слайд 19Breathing
Zone I injuries with concomitant thoracic injuries
pneumothorax
hemopneumothorax
tension pneumothorax
Breathing
Zone I injuries with concomitant thoracic injuries
pneumothorax
hemopneumothorax
tension pneumothorax
Слайд 20Circulation
Bleeding should be controlled by pressure
Do not clamp blindly or probe the
Circulation
Bleeding should be controlled by pressure
Do not clamp blindly or probe the
Слайд 21History
Obtain from EMS witnesses, patient
Mechanisms of injury - stab wounds, gunshot wound,
History
Obtain from EMS witnesses, patient
Mechanisms of injury - stab wounds, gunshot wound,
Слайд 22Physical Examination
Thorough head and neck exam using palpation and stethoscope to search
Physical Examination
Thorough head and neck exam using palpation and stethoscope to search
Слайд 23Radiographs
CXR - inspiratory/expiratory films to assess for phrenic nerve injury, look for
Radiographs
CXR - inspiratory/expiratory films to assess for phrenic nerve injury, look for
Слайд 24Preoperative Preparation
Surgeon and staff ready for emergent/urgent tracheotomy
Gentle cleansing of wound, betadine
Preoperative Preparation
Surgeon and staff ready for emergent/urgent tracheotomy
Gentle cleansing of wound, betadine
Слайд 25Penetrating neck trauma
Diagnosis Signs and symptoms
Vascular injury Shock Hematoma
Hemorrhage
Pulse deficit
Neurologic
Diagnosis Signs and symptoms
Vascular injury Shock Hematoma
Hemorrhage
Pulse deficit
Neurologic
Слайд 26Exploration vs. Observation
Many experts have adopted a policy of selective exploration
Decreased number
Exploration vs. Observation
Many experts have adopted a policy of selective exploration
Decreased number
Слайд 29Site/Zone I
Adequate exposure for exploration and repair may require sternotomy, clavicle resection,
Site/Zone I
Adequate exposure for exploration and repair may require sternotomy, clavicle resection,
Слайд 30Site/Zone II
Few injuries will escape clinical examination
Most carotid injuries occur here
Adjunctive
Site/Zone II
Few injuries will escape clinical examination
Most carotid injuries occur here
Adjunctive
Слайд 31Site/Zone III
High rate of vascular injury, often multiple
Often difficult to obtain proximal
Site/Zone III
High rate of vascular injury, often multiple
Often difficult to obtain proximal
Слайд 32Clinical Setting
Observation requires admission to an intensive care unit where serial examination
Clinical Setting
Observation requires admission to an intensive care unit where serial examination
Слайд 33Pharyngo Esophageal
Gastrografin swallow followed by Barium if negative
Flexible ± rigid esophagoscopy
Invert the
Pharyngo Esophageal
Gastrografin swallow followed by Barium if negative
Flexible ± rigid esophagoscopy
Invert the
Слайд 35Airway
DL where laryngeal injury is suspected
Mucosal tears are closed with absorbable sutures
Airway
DL where laryngeal injury is suspected
Mucosal tears are closed with absorbable sutures
Слайд 36Vascular
The subclavian and internal jugular veins can be ligated without adverse effect
Major
Vascular
The subclavian and internal jugular veins can be ligated without adverse effect
Major

Слайд 39Vascular cont.
When tension is required, vein grafts from the sphenous or internal
Vascular cont.
When tension is required, vein grafts from the sphenous or internal
Слайд 41Conclusions
Maintain a healthy respect for apparently minor neck wounds because of potential
Conclusions
Maintain a healthy respect for apparently minor neck wounds because of potential
 Финансы в экономике
Финансы в экономике Дополнительное телематическое оборудование в авто Remoto
Дополнительное телематическое оборудование в авто Remoto The sights of America
The sights of America 98696487
98696487 Собака динго
Собака динго Презентация на тему Этическая основа культуры
Презентация на тему Этическая основа культуры Влияние воды и водных процедур на здоровье человека
Влияние воды и водных процедур на здоровье человека 제5과. 말하기
제5과. 말하기 Создавать видимость активной работы Минимизировать ответственность и риски Сохранить хорошую мину Получать большую зарплату КАК
Создавать видимость активной работы Минимизировать ответственность и риски Сохранить хорошую мину Получать большую зарплату КАК Химия атмосферы и поверхности.
Химия атмосферы и поверхности. Насилие в произведениях искусства
Насилие в произведениях искусства Основы мировых религиозных культур « Вся культура – из храма» Дж. Фрэзер Автор: д.и.н., доцент Сушко А.В. Омск – 2012.
Основы мировых религиозных культур « Вся культура – из храма» Дж. Фрэзер Автор: д.и.н., доцент Сушко А.В. Омск – 2012. Что изучает история Древнего мира (5 класс)
Что изучает история Древнего мира (5 класс) Алесь Разанау
Алесь Разанау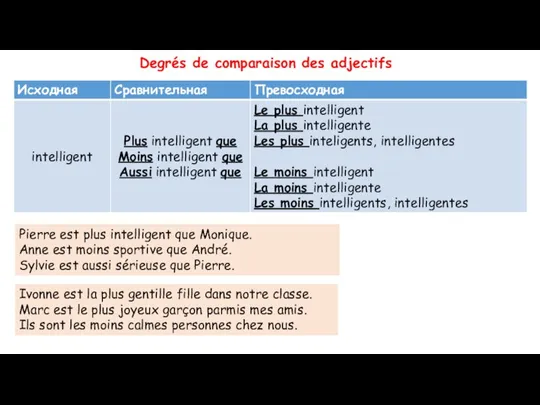 8Г2_2022-10-12_урок 11_devoir (1)
8Г2_2022-10-12_урок 11_devoir (1) Первая постановка комедии «Ревизор»
Первая постановка комедии «Ревизор» Гипоталамус
Гипоталамус  Современная концепция управления проектом
Современная концепция управления проектом Маковельская Инна Николаевна
Маковельская Инна Николаевна Соотношение финансового права и финансового законодательства
Соотношение финансового права и финансового законодательства Организация наставничества на государственной гражданской службе
Организация наставничества на государственной гражданской службе Федорко Надежда Никифоровна
Федорко Надежда Никифоровна Present simple versus present continuous
Present simple versus present continuous Почему кошки так называются?
Почему кошки так называются? Фонетика (урок-повторение, 6 класс)
Фонетика (урок-повторение, 6 класс) Особые образовательные потребности
Особые образовательные потребности Уважаемые преподаватели, аспиранты и студенты РГЭУ (РИНХ)! Представляем вам новую специальную литературу (учебники и монографии),
Уважаемые преподаватели, аспиранты и студенты РГЭУ (РИНХ)! Представляем вам новую специальную литературу (учебники и монографии), Работа со списками. Колонки. Буквица. Стили
Работа со списками. Колонки. Буквица. Стили