- Spinal disease

Содержание
- 2. Upper vs. Lower Motor Neuron Upper motor neuron lesion Motor cortex internal capsule brainstem spinal cord
- 3. Basic Features of Spinal Cord Disease UMN findings below the lesion Hyperreflexia and Babinski’s Sensory and
- 4. History Onset Acute, subacute, chronic Symptoms Pain Weakness Sensory Autonomic Past history Family history
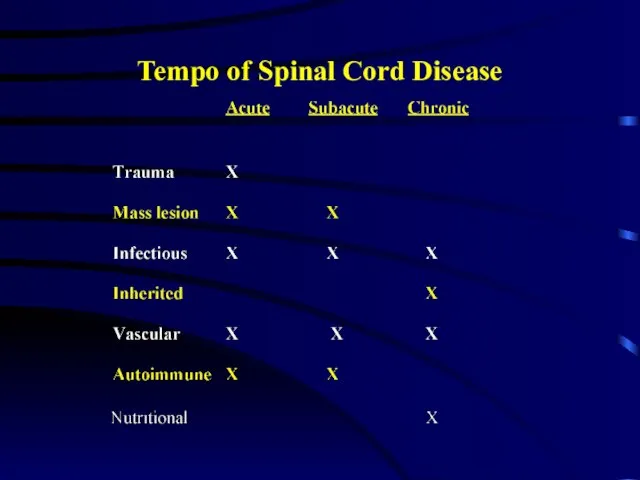
- 5. Tempo of Spinal Cord Disease
- 6. Motor Exam Strength - helps to localize the lesion Upper cervical Quadriplegia with impaired respiration Lower
- 7. Sensory Exam Establish a sensory level Dermatomes Nipples: T4-5 Umbilicus: T8-9 Posterior columns Vibration Joint position
- 8. Autonomic disturbances Neurogenic bladder Urgency, incontinence, retention Bowel dysfunction Constipation more frequent than incontinence With a
- 9. Investigation of Spinal Cord Disease Radiographic exams Plain films Myelography CT scan with myelography MRI Spinal
- 10. Etiology of Spinal Cord Disease
- 11. Traumatic Spinal Cord Disease 10,000 new spinal cord injuries per year MVA, sports injuries the most
- 12. Tumors Metastatic or primary Extramedullary Extradural - most common Bony - breast, prostate Intradural - very
- 13. B12 Deficiency Subacute combined degeneration of the cord B12 deficiency malabsorption of B12 secondary to pernicious
- 14. Transverse myelitis Inflammation of the spinal cord Post-infectious Post-vaccinial Multiple sclerosis Pain at level of lesion
- 15. Infections Involving the Spinal Cord Polio only the anterior horn cells are infected Tabes dorsalis dorsal
- 16. Multiple Sclerosis Demyelination is the underlying pathology Cord disease can be presenting feature of MS or
- 17. Vascular Diseases of the Spinal Cord Infarcts Anterior spinal artery infarct from atherosclerosis, during surgery in
- 18. Vascular Diseases of the Spinal Cord, cont Arteriovenous malformation (AVM) and venous angiomas Both occur in
- 19. Other Disease of the Spinal Cord Hereditary spastic paraparesis Usually autosomal dominant Infectious process of the
- 20. Classical spinal cord syndromes Anterior spinal artery infarct Brown Sequard syndrome Syringomyelia Conus medullaris/caude equina lesions
- 21. Brown Sequard Syndrome Cord hemisection Trauma or tumor Dissociated sensory loss loss of pain and temperature
- 22. Syringomyelia Fluid filled cavitation in the center of the cord Cervical cord most common site Loss
- 24. Скачать презентацию
Слайд 3Basic Features of Spinal Cord Disease
UMN findings below the lesion
Hyperreflexia and Babinski’s
Sensory
Basic Features of Spinal Cord Disease
UMN findings below the lesion
Hyperreflexia and Babinski’s
Sensory
Слайд 4History
Onset
Acute, subacute, chronic
Symptoms
Pain
Weakness
Sensory
Autonomic
Past history
Family history
History
Onset
Acute, subacute, chronic
Symptoms
Pain
Weakness
Sensory
Autonomic
Past history
Family history
Слайд 5Tempo of Spinal Cord Disease
Tempo of Spinal Cord Disease
Слайд 6Motor Exam
Strength - helps to localize the lesion
Upper cervical
Quadriplegia with impaired respiration
Lower
Motor Exam
Strength - helps to localize the lesion
Upper cervical
Quadriplegia with impaired respiration
Lower
Слайд 7Sensory Exam
Establish a sensory level
Dermatomes
Nipples: T4-5
Umbilicus: T8-9
Posterior columns
Vibration
Joint position sense (proprioception)
Spinothalamic tracts
Pain
Temperature
Sensory Exam
Establish a sensory level
Dermatomes
Nipples: T4-5
Umbilicus: T8-9
Posterior columns
Vibration
Joint position sense (proprioception)
Spinothalamic tracts
Pain
Temperature
Слайд 8Autonomic disturbances
Neurogenic bladder
Urgency, incontinence, retention
Bowel dysfunction
Constipation more frequent than incontinence
With a high
Autonomic disturbances
Neurogenic bladder
Urgency, incontinence, retention
Bowel dysfunction
Constipation more frequent than incontinence
With a high
Слайд 9Investigation of Spinal Cord Disease
Radiographic exams
Plain films
Myelography
CT scan with myelography
MRI
Spinal tap
If you
Investigation of Spinal Cord Disease
Radiographic exams
Plain films
Myelography
CT scan with myelography
MRI
Spinal tap
If you
Слайд 10Etiology of Spinal Cord Disease
Etiology of Spinal Cord Disease
Слайд 11Traumatic Spinal Cord Disease
10,000 new spinal cord injuries per year
MVA, sports injuries
Traumatic Spinal Cord Disease
10,000 new spinal cord injuries per year
MVA, sports injuries
Слайд 12Tumors
Metastatic or primary
Extramedullary
Extradural - most common
Bony - breast, prostate
Intradural - very rare
Meninges
Tumors
Metastatic or primary
Extramedullary
Extradural - most common
Bony - breast, prostate
Intradural - very rare
Meninges
Слайд 13B12 Deficiency
Subacute combined degeneration of the cord
B12 deficiency
malabsorption of B12 secondary to
B12 Deficiency
Subacute combined degeneration of the cord
B12 deficiency
malabsorption of B12 secondary to
Слайд 14Transverse myelitis
Inflammation of the spinal cord
Post-infectious
Post-vaccinial
Multiple sclerosis
Pain at level of lesion
Transverse myelitis
Inflammation of the spinal cord
Post-infectious
Post-vaccinial
Multiple sclerosis
Pain at level of lesion
Слайд 15Infections Involving the Spinal Cord
Polio
only the anterior horn cells are infected
Tabes dorsalis
dorsal
Infections Involving the Spinal Cord
Polio
only the anterior horn cells are infected
Tabes dorsalis
dorsal
Слайд 16Multiple Sclerosis
Demyelination is the underlying pathology
Cord disease can be presenting feature of
Multiple Sclerosis
Demyelination is the underlying pathology
Cord disease can be presenting feature of
Слайд 17Vascular Diseases of the Spinal Cord
Infarcts
Anterior spinal artery infarct
from atherosclerosis, during surgery
Vascular Diseases of the Spinal Cord
Infarcts
Anterior spinal artery infarct
from atherosclerosis, during surgery
Слайд 18Vascular Diseases of the Spinal Cord, cont
Arteriovenous malformation (AVM) and venous angiomas
Both
Vascular Diseases of the Spinal Cord, cont
Arteriovenous malformation (AVM) and venous angiomas
Both
Слайд 19Other Disease of the Spinal Cord
Hereditary spastic paraparesis
Usually autosomal dominant
Infectious process of
Other Disease of the Spinal Cord
Hereditary spastic paraparesis
Usually autosomal dominant
Infectious process of
Слайд 20Classical spinal cord syndromes
Anterior spinal artery infarct
Brown Sequard syndrome
Syringomyelia
Conus medullaris/caude equina lesions
Classical spinal cord syndromes
Anterior spinal artery infarct
Brown Sequard syndrome
Syringomyelia
Conus medullaris/caude equina lesions
Слайд 21Brown Sequard Syndrome
Cord hemisection
Trauma or tumor
Dissociated sensory loss
loss of pain and temperature
Brown Sequard Syndrome
Cord hemisection
Trauma or tumor
Dissociated sensory loss
loss of pain and temperature
Слайд 22Syringomyelia
Fluid filled cavitation in the center of the cord
Cervical cord most common
Syringomyelia
Fluid filled cavitation in the center of the cord
Cervical cord most common
 Проект:«Права и обязанности членов семьи»
Проект:«Права и обязанности членов семьи» Презентация на тему Свойства корня n-ой степени (11 класс)
Презентация на тему Свойства корня n-ой степени (11 класс) КМРСО г.Красноярск Солянкина Наталья Леонидовна Голубева Людмила Матвеевна Центр мониторинга качества образования ККИПКиППРО
КМРСО г.Красноярск Солянкина Наталья Леонидовна Голубева Людмила Матвеевна Центр мониторинга качества образования ККИПКиППРО Презентация на тему Обычаи и традиции русского народа
Презентация на тему Обычаи и традиции русского народа Система управления персоналом
Система управления персоналом Презентация на тему Великобритания: конец Викторианской эпохи
Презентация на тему Великобритания: конец Викторианской эпохи  Основные ценности городского сообщества Тольятти Докладчик: Иглин В.Б. Школа № 93. Автозаводской район Тольятти 26 декабря 2010 год
Основные ценности городского сообщества Тольятти Докладчик: Иглин В.Б. Школа № 93. Автозаводской район Тольятти 26 декабря 2010 год Лекция №10-11 (Метод Тестирования) (1)
Лекция №10-11 (Метод Тестирования) (1) Уголок потребителя
Уголок потребителя Защита Отечества — священный долг
Защита Отечества — священный долг Монархи-2017
Монархи-2017 Архитектурные элементы здания
Архитектурные элементы здания Консалтинг-центр по НИДШ
Консалтинг-центр по НИДШ Экстремизм - угроза обществу
Экстремизм - угроза обществу Прямое и переносное значение слов
Прямое и переносное значение слов Фоторяд "Дети войны"
Фоторяд "Дети войны" Инструменты, механизмы, приспособления и инвентарь для выполнения штукатурных работ
Инструменты, механизмы, приспособления и инвентарь для выполнения штукатурных работ Александр Сергеевич Пушкин
Александр Сергеевич Пушкин ОСНОВНЫЕ КОМПОНЕНТЫ И УЗЛЫ ЭЛЕКТРОННЫХ УСТРОЙСТВ
ОСНОВНЫЕ КОМПОНЕНТЫ И УЗЛЫ ЭЛЕКТРОННЫХ УСТРОЙСТВ  Методы селекции растений 11 класс
Методы селекции растений 11 класс Музей Ф.М. Достоевского
Музей Ф.М. Достоевского  Альбом «МОЯ СЕМЬЯ»
Альбом «МОЯ СЕМЬЯ» Метеоролог
Метеоролог Каменный лес
Каменный лес Развивающая эстетика – новый предмет в школьном образовании
Развивающая эстетика – новый предмет в школьном образовании Революционное народничество: идеология, практика, последствия.
Революционное народничество: идеология, практика, последствия. 5 этап командный 15.12.2011ТУРНИРкоманд или индивидуальных участников 9-11 классов по решению «монстров С6»
5 этап командный 15.12.2011ТУРНИРкоманд или индивидуальных участников 9-11 классов по решению «монстров С6» Презентация на тему Храмы России
Презентация на тему Храмы России