- Ventilator Discontinuation: The evidence base and best practice

Содержание
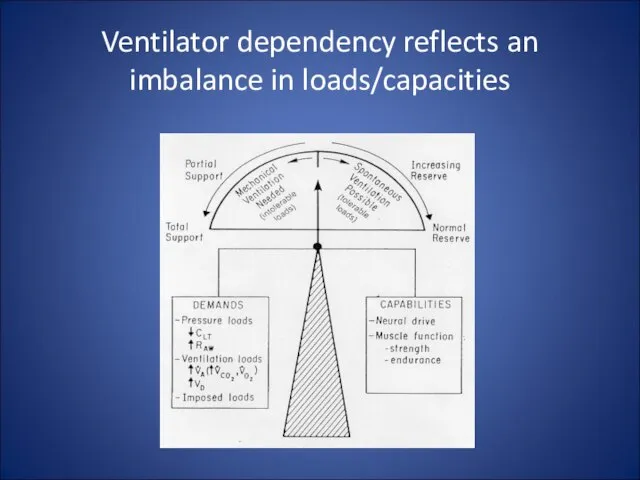
- 2. Ventilator dependency reflects an imbalance in loads/capacities
- 3. Ventilator dependency can also be iatrogenic Failure to recognize discontinuation potential Imposed loading: insufficient support insensitive/unresponsive
- 4. The Ventilator Discontinuation Process - EBM Projects AHCPR - McMaster comprehensive evidence based review 5000 papers
- 5. The Ventilator Discontinuation Process - EBM Projects ACCP/SCCM/AARC Task Force Organized May 1999 Used McMaster report
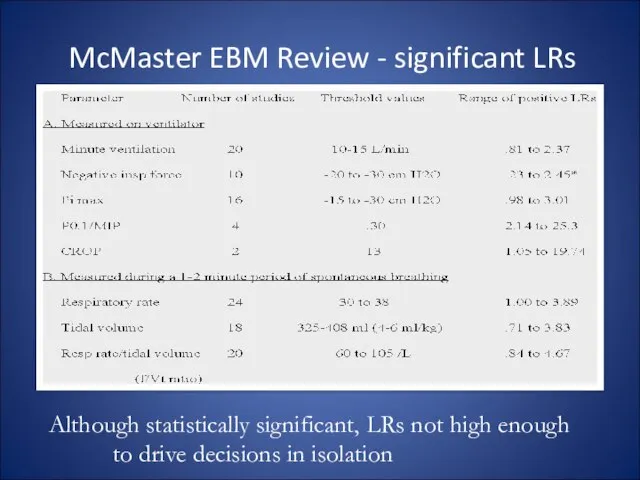
- 6. McMaster EBM Review - significant LRs Although statistically significant, LRs not high enough to drive decisions
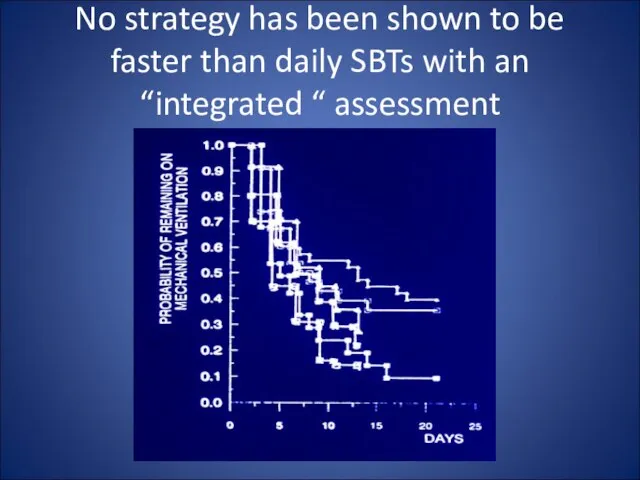
- 7. No strategy has been shown to be faster than daily SBTs with an “integrated “ assessment
- 8. ACCP/SCCM/AARC EBM Guidelines Criteria for considering vent discontinuation: stability/reversal of respiratory failure P/F > 150-200, PEEP
- 9. ACCP/SCCM/AARC EBM Guidelines SBT is most effective way of assessing d/c potential: 5 cm H2O PS,
- 10. ET tube removal requires ability to protect airway Cough is essential Cough velocity (>1 l/sec) White
- 11. Routine daily SBTs shortens weaning NEJM 1996;335:1864
- 12. ACCP/SCCM/AARC EBM Guidelines For patients who fail the SBT: Search for reversible causes
- 13. In between the daily SBT: Address the reversible aspects of load/capabilities imbalance: Loads: improve mechanics (edema,
- 14. ACCP/SCCM/AARC EBM Guidelines For patients who fail the SBT: Search for reversible causes Repeat SBTs q
- 15. In between daily SBTs Properly load the muscles: “Normalize” amount of load avoid atrophy, avoid fatigue
- 16. Practical aspects of “normalized”, comfortable loading Triggering - max sensitivity, “balance” PEEPi with applied PEEP Pressure/flow
- 17. Newer approaches to improving synchrony Proportional assist ventilation Pressure and flow driven by sensed pt flow
- 18. ACCP/SCCM/AARC EBM Guidelines For patients who fail the SBT: Search for reversible causes Repeat SBTs q
- 19. ACCP/SCCM/AARC EBM Guidelines For patients who fail the SBT: Search for reversible causes Repeat SBTs q
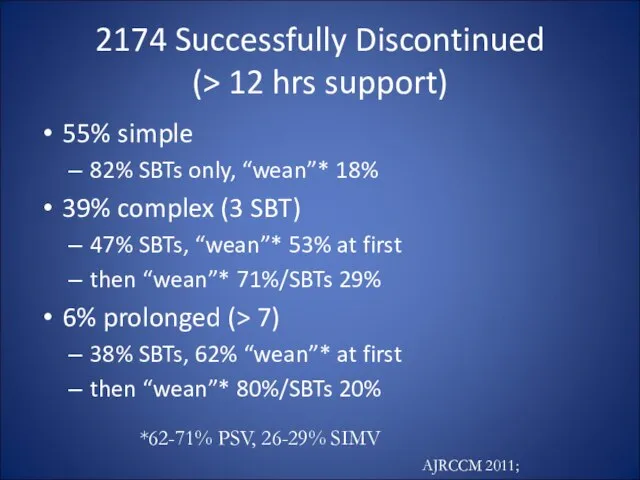
- 20. 2174 Successfully Discontinued (> 12 hrs support) 55% simple 82% SBTs only, “wean”* 18% 39% complex
- 21. Can weaning be automated? Assumes that gradual support reductions help – evidence supporting this is weak
- 22. Volume Support (VS, ASV) Adjusts pressure to targeted tidal volume In theory: As patient recovers, bigger
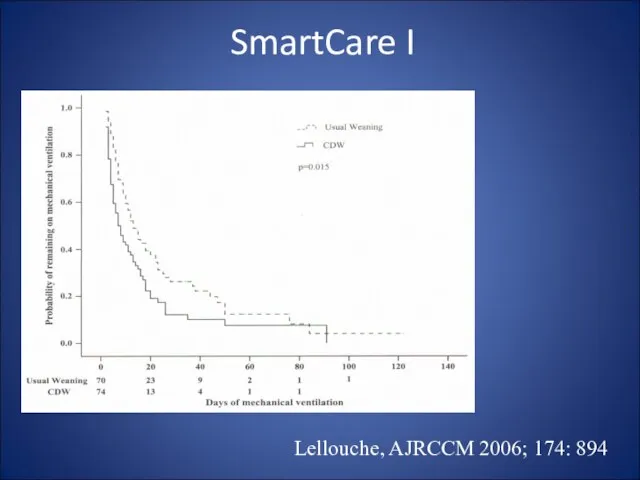
- 23. Lellouche, AJRCCM 2006; 174: 894 SmartCare I
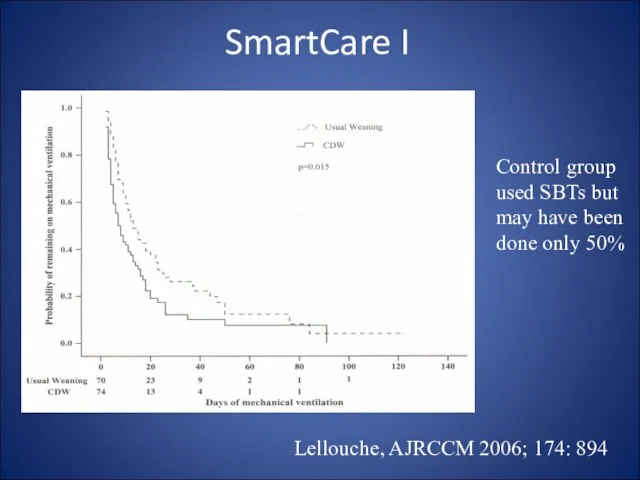
- 24. Lellouche, AJRCCM 2006; 174: 894 Control group used SBTs but may have been done only 50%
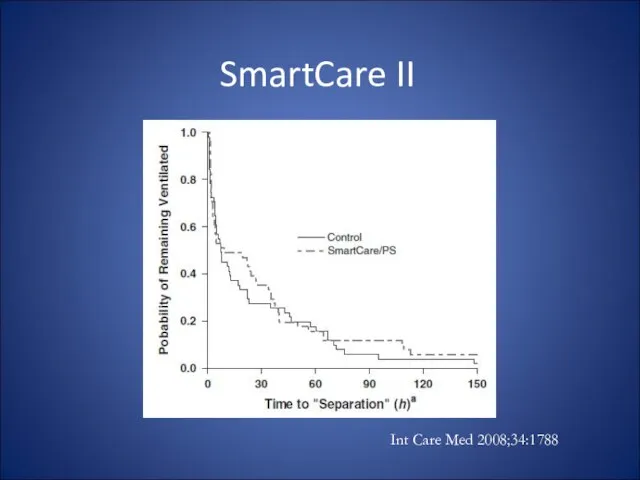
- 25. Int Care Med 2008;34:1788 SmartCare II
- 26. So is there a role for automatic PS reductions? No evidence that says this facilitates muscle
- 28. NIV and Vent Discontinuation: Two Scenarios The failed/borderline SBT but good airway protection Supportive evidence, especially
- 30. Скачать презентацию
Слайд 3Ventilator dependency can also be iatrogenic
Failure to recognize discontinuation potential
Imposed loading:
insufficient support
insensitive/unresponsive
Ventilator dependency can also be iatrogenic
Failure to recognize discontinuation potential
Imposed loading:
insufficient support
insensitive/unresponsive
Слайд 4The Ventilator Discontinuation Process - EBM Projects
AHCPR - McMaster comprehensive evidence based
The Ventilator Discontinuation Process - EBM Projects
AHCPR - McMaster comprehensive evidence based
Слайд 5The Ventilator Discontinuation Process - EBM Projects
ACCP/SCCM/AARC Task Force
Organized May 1999
Used McMaster
The Ventilator Discontinuation Process - EBM Projects
ACCP/SCCM/AARC Task Force
Organized May 1999
Used McMaster
Слайд 6McMaster EBM Review - significant LRs
Although statistically significant, LRs not high enough
McMaster EBM Review - significant LRs
Although statistically significant, LRs not high enough
Слайд 7No strategy has been shown to be faster than daily SBTs with
No strategy has been shown to be faster than daily SBTs with
Слайд 8ACCP/SCCM/AARC EBM Guidelines
Criteria for considering vent discontinuation:
stability/reversal of respiratory failure
P/F > 150-200,
ACCP/SCCM/AARC EBM Guidelines
Criteria for considering vent discontinuation:
stability/reversal of respiratory failure
P/F > 150-200,
Слайд 9ACCP/SCCM/AARC EBM Guidelines
SBT is most effective way of assessing d/c potential:
5 cm
ACCP/SCCM/AARC EBM Guidelines
SBT is most effective way of assessing d/c potential:
5 cm
Слайд 10ET tube removal requires ability to protect airway
Cough is essential
Cough velocity (>1
ET tube removal requires ability to protect airway
Cough is essential
Cough velocity (>1
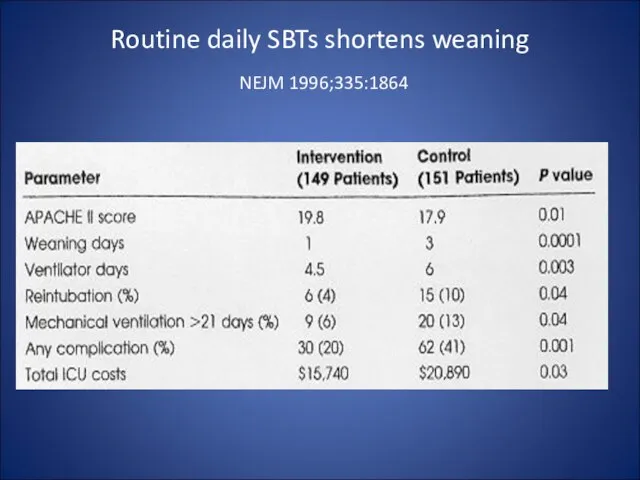
Слайд 11Routine daily SBTs shortens weaning
NEJM 1996;335:1864
Routine daily SBTs shortens weaning
NEJM 1996;335:1864
Слайд 12ACCP/SCCM/AARC EBM Guidelines
For patients who fail the SBT:
Search for reversible causes
ACCP/SCCM/AARC EBM Guidelines
For patients who fail the SBT:
Search for reversible causes
Слайд 13In between the daily SBT:
Address the reversible aspects of load/capabilities imbalance:
Loads:
improve
In between the daily SBT:
Address the reversible aspects of load/capabilities imbalance:
Loads:
improve
Слайд 14ACCP/SCCM/AARC EBM Guidelines
For patients who fail the SBT:
Search for reversible causes
Repeat SBTs
ACCP/SCCM/AARC EBM Guidelines
For patients who fail the SBT:
Search for reversible causes
Repeat SBTs
Слайд 15In between daily SBTs
Properly load the muscles:
“Normalize” amount of load
avoid atrophy, avoid
In between daily SBTs
Properly load the muscles:
“Normalize” amount of load
avoid atrophy, avoid
Слайд 16Practical aspects of “normalized”, comfortable loading
Triggering - max sensitivity, “balance” PEEPi with
Practical aspects of “normalized”, comfortable loading
Triggering - max sensitivity, “balance” PEEPi with
Слайд 17Newer approaches to improving synchrony
Proportional assist ventilation
Pressure and flow driven by sensed
Newer approaches to improving synchrony
Proportional assist ventilation
Pressure and flow driven by sensed
Слайд 18ACCP/SCCM/AARC EBM Guidelines
For patients who fail the SBT:
Search for reversible causes
Repeat SBTs
ACCP/SCCM/AARC EBM Guidelines
For patients who fail the SBT:
Search for reversible causes
Repeat SBTs
Слайд 19ACCP/SCCM/AARC EBM Guidelines
For patients who fail the SBT:
Search for reversible causes
Repeat SBTs
ACCP/SCCM/AARC EBM Guidelines
For patients who fail the SBT:
Search for reversible causes
Repeat SBTs
Слайд 202174 Successfully Discontinued
(> 12 hrs support)
55% simple
82% SBTs only, “wean”* 18%
39% complex
2174 Successfully Discontinued
(> 12 hrs support)
55% simple
82% SBTs only, “wean”* 18%
39% complex
Слайд 21Can weaning be automated?
Assumes that gradual support reductions help – evidence supporting
Can weaning be automated?
Assumes that gradual support reductions help – evidence supporting
Слайд 22Volume Support (VS, ASV)
Adjusts pressure to targeted tidal volume
In theory:
As patient recovers,
Volume Support (VS, ASV)
Adjusts pressure to targeted tidal volume
In theory:
As patient recovers,
Слайд 23Lellouche, AJRCCM 2006; 174: 894
SmartCare I
Lellouche, AJRCCM 2006; 174: 894
SmartCare I
Слайд 24Lellouche, AJRCCM 2006; 174: 894
Control group
used SBTs but
may have been
done
Lellouche, AJRCCM 2006; 174: 894
Control group
used SBTs but
may have been
done
Слайд 25Int Care Med 2008;34:1788
SmartCare II
Int Care Med 2008;34:1788
SmartCare II
Слайд 26So is there a role for automatic PS reductions?
No evidence that says
So is there a role for automatic PS reductions?
No evidence that says

Слайд 28NIV and Vent Discontinuation:
Two Scenarios
The failed/borderline SBT but good airway protection
Supportive evidence,
NIV and Vent Discontinuation:
Two Scenarios
The failed/borderline SBT but good airway protection
Supportive evidence,
 Согласный звук [й]
Согласный звук [й] Влади́мир Луки́ч Боровиковский
Влади́мир Луки́ч Боровиковский Презентация ко дню учителя
Презентация ко дню учителя Название кофейни Coffee Smile
Название кофейни Coffee Smile Jels
Jels Игра в волейбол. Тест
Игра в волейбол. Тест 26e646f73e9ee9e1 (1)
26e646f73e9ee9e1 (1) Работа выполнена в рамках проекта «Повышение квалификаций различных категорий работников образования и формирование у них базов
Работа выполнена в рамках проекта «Повышение квалификаций различных категорий работников образования и формирование у них базов Презентация на тему О птицах зимой окружающий мир
Презентация на тему О птицах зимой окружающий мир Презентация на тему Мучные изделия
Презентация на тему Мучные изделия Бер өн менән генә айырылған һүҙҙәр уйла
Бер өн менән генә айырылған һүҙҙәр уйла Программа развития МОУ «СОШ №3»
Программа развития МОУ «СОШ №3» реклама
реклама Земля – планета Солнечной системы
Земля – планета Солнечной системы Что такое хобби
Что такое хобби "Почва- зеркало ландшафта"
"Почва- зеркало ландшафта" Процессоры фирм Intel и AMD
Процессоры фирм Intel и AMD Налоговый режим для компаний ИТ сектора
Налоговый режим для компаний ИТ сектора Экономические потребности, блага и ресурсы. Экономический выбор
Экономические потребности, блага и ресурсы. Экономический выбор Объединенный брифинг по метео и аэронавигационной информации
Объединенный брифинг по метео и аэронавигационной информации Файл и файловые системы
Файл и файловые системы Соглашения о сотрудничестве заключены со многими предприятиями и учреждениями, в том числе:
Соглашения о сотрудничестве заключены со многими предприятиями и учреждениями, в том числе: Марафон продающих текстов
Марафон продающих текстов декоративное
декоративное Как изменялись способы движения в ходе эволюции животного мира
Как изменялись способы движения в ходе эволюции животного мира Презентация по английскому Интерактивная мозаика
Презентация по английскому Интерактивная мозаика Начало раздробления Древнерусского государства
Начало раздробления Древнерусского государства Infectious process
Infectious process