- ACUTE CHOLECYSTITIS

Содержание
- 2. Content Anatomy Bile Stone formation & types Acute cholecystitis - Calculus - Acalculus Sign & symptoms
- 3. ANATOMY The gallbladder is located in the right upper quadrant of the abdomen beneath the liver.
- 4. ANATOMY CBD empty into the duodenum at the ampulla of Vater. This is surrounded by the
- 5. ANATOMY Blood supply is from the cystic artery. Celiac A. Hepatic A. Rt. Hepatic A. Cystic
- 6. Nerve Supply : Sympathetic and parasympathetic vagal fibers the celiac plexus. Lymph Drainage: The lymph drains
- 9. Bile Bile produced in the liver is stored in the gallbladder. The function of bile is
- 10. Bile The spiral valves of Heister in the cystic duct prevent bile reflux into the gallbladder.
- 11. Stones formation Imbalance of cholesterol and its solubilizing agents, bile salts and lecithin concentrations If hepatic
- 12. Types of Stones Cholesterol stones Pigment stones Mixed stones
- 13. Cholesterol Stones
- 14. Pigment stones
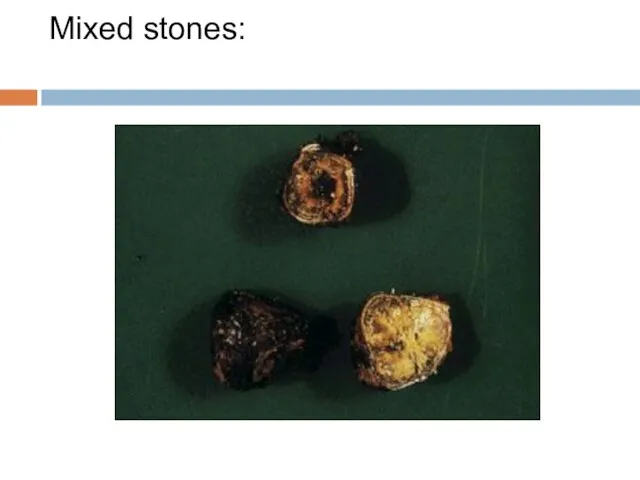
- 15. Mixed stones:
- 16. Acute Cholecystitis
- 17. Acute Cholecystitis Inflammation of the gallbladder, resulting from : Obstruction of cystic duct by gallstone( 80%
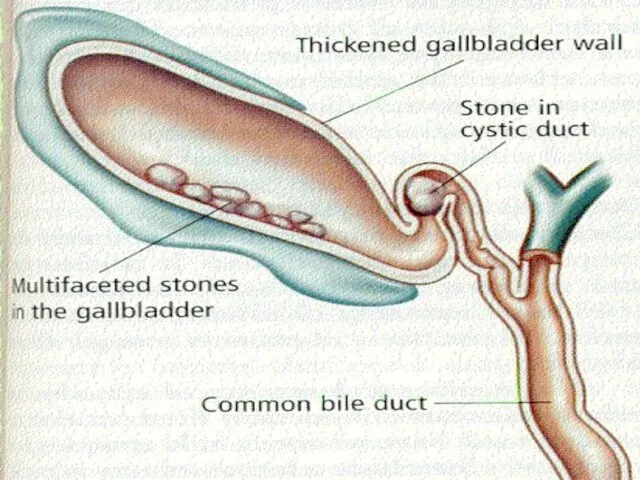
- 18. Acute Cholecystitis Cholecystitis with stones most commonly blocking the cystic duct directly. This leads to inspissation
- 19. Acute Cholecystitis The gallbladder shows congestion, thickening of the wall by edema and mucosal ulceration.
- 21. Pathogenesis:
- 22. Acute cholecystitis without gallstone may occur in a variety of condition it may be due to
- 23. Hx Age 30-60 yrs mostly ♀ Sudden pain in RUQ, often radiate through the back to
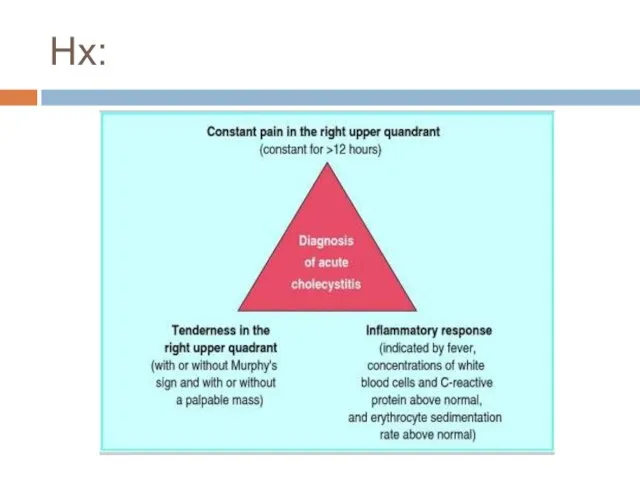
- 24. Hx:
- 25. Signs & Symptoms Anorexia. Low grade fever ( Tachycardia Positive Murphy’s sign Palpable gallbladder (in 1/3
- 26. P/E Pt distressed by pain and lies quitely breathing shallowly. Tachycardia and Pyrexia Tenderness & guarding
- 27. Physical features of enlarged GB It appears from beneath the tip of the Rt. 9th rib
- 28. Differential diagnosis Perforating or penetrating peptic ulcer. Myocardial infraction Pancreatitis Hiatus hernia RLL pneumonia Appendicitis Hepatitis
- 29. Lab Investigations Leukocystosis Mild Hyperbillirubinemia Mild ↑ AST, ALT, ALP Moderate ↑ Lipase & Amylase
- 30. US Distended gallbladder Thickened gallbladdr wall Pericholecystic fluid collection US Murphy’s sign ( + in 98%
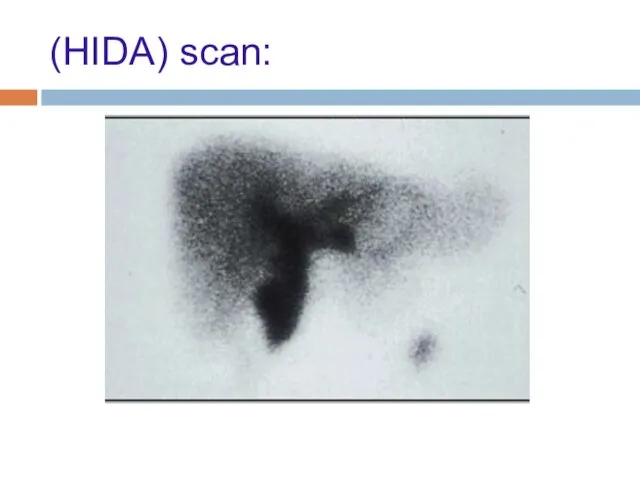
- 31. Biliary scintigraphy (hydroxyiminodiacetic acid) (HIDA) scan: Is the gold standard investigation when the diagnosis remains in
- 32. (HIDA) scan: The patient is given an intravenous injection of radiolabelled hydroxyiminodiacetic acid and then the
- 33. (HIDA) scan:
- 34. Complication - Cholecystentiric fistula formation - Gallstone illeus - Perforation (may cause localized abscess or generalized
- 35. Mx NPO IVF IV Analgesia (pethidine) IV Abx (cefuroxime) NGT Parental Analgesics Optimal Rx is cholecystectomy
- 36. Calot’s Triangle Superiorly: Lower edge of the liver Laterally: Cystic Duct Medially: Common Hepatic Duct
- 37. Acute Cholecystits vs. Billiary Colic Duration, Symptoms ?
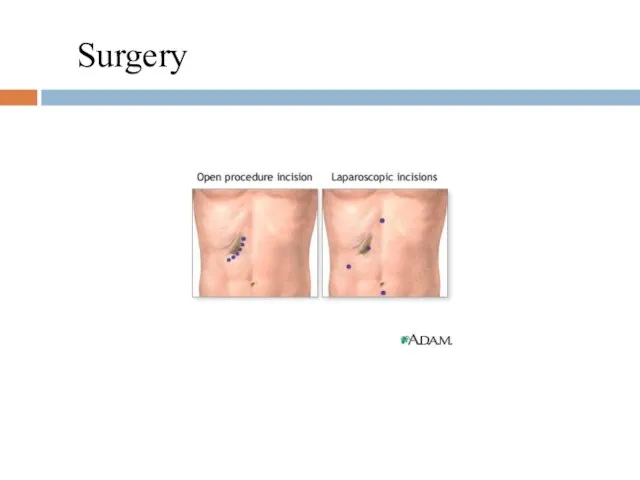
- 38. Surgery
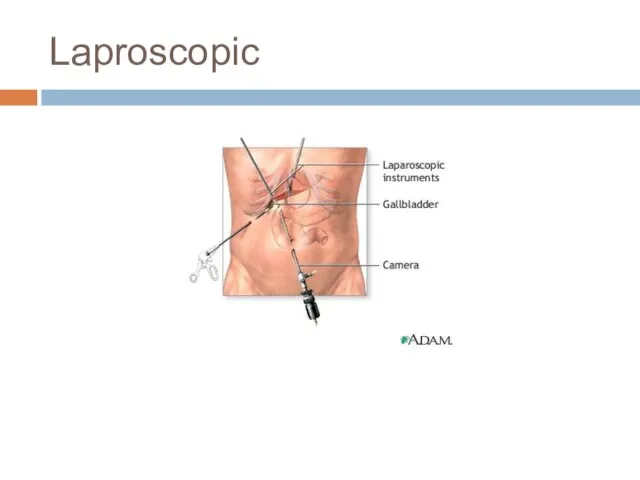
- 39. Laproscopic
- 40. Questions
- 42. Скачать презентацию
Слайд 3ANATOMY
The gallbladder is located in the right upper quadrant of the abdomen
ANATOMY
The gallbladder is located in the right upper quadrant of the abdomen
Слайд 4ANATOMY
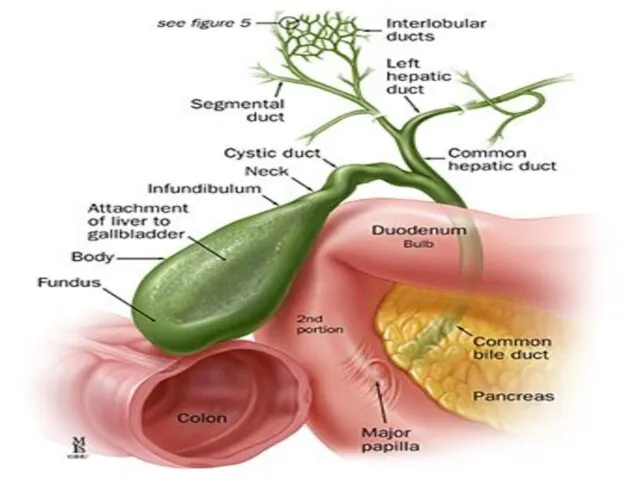
CBD empty into the duodenum at the ampulla of Vater. This
ANATOMY
CBD empty into the duodenum at the ampulla of Vater. This
Слайд 5ANATOMY
Blood supply is from the cystic artery.
Celiac A. Hepatic A. Rt. Hepatic
ANATOMY
Blood supply is from the cystic artery.
Celiac A. Hepatic A. Rt. Hepatic
Слайд 6Nerve Supply :
Sympathetic and parasympathetic vagal fibers
the celiac plexus.
Lymph Drainage:
Nerve Supply :
Sympathetic and parasympathetic vagal fibers
the celiac plexus.
Lymph Drainage:
Слайд 9Bile
Bile produced in the liver is stored in the gallbladder.
The function
Bile
Bile produced in the liver is stored in the gallbladder.
The function
Слайд 10Bile
The spiral valves of Heister in the cystic duct prevent bile
Bile
The spiral valves of Heister in the cystic duct prevent bile
Слайд 11Stones formation
Imbalance of cholesterol and its solubilizing agents, bile salts and lecithin
Stones formation
Imbalance of cholesterol and its solubilizing agents, bile salts and lecithin
Слайд 12Types of Stones
Cholesterol stones
Pigment stones
Mixed stones
Types of Stones
Cholesterol stones
Pigment stones
Mixed stones
Слайд 13Cholesterol Stones
Cholesterol Stones

Слайд 14Pigment stones
Pigment stones

Слайд 15Mixed stones:
Mixed stones:
Слайд 16Acute
Cholecystitis
Acute
Cholecystitis
Слайд 17Acute Cholecystitis
Inflammation of the gallbladder, resulting from :
Obstruction of cystic duct by
Acute Cholecystitis
Inflammation of the gallbladder, resulting from :
Obstruction of cystic duct by
Слайд 18Acute Cholecystitis
Cholecystitis with stones most commonly blocking the cystic duct directly. This
Acute Cholecystitis
Cholecystitis with stones most commonly blocking the cystic duct directly. This
Слайд 19Acute Cholecystitis
The gallbladder shows congestion, thickening of the wall by edema and
Acute Cholecystitis
The gallbladder shows congestion, thickening of the wall by edema and
Слайд 21Pathogenesis:
Pathogenesis:

Слайд 22Acute cholecystitis without gallstone may occur in a variety of condition it
Слайд 23Hx
Age 30-60 yrs
mostly ♀
Sudden pain in RUQ, often radiate through the
Hx
Age 30-60 yrs
mostly ♀
Sudden pain in RUQ, often radiate through the
Слайд 24Hx:
Hx:
Слайд 25Signs & Symptoms
Anorexia.
Low grade fever ( < 38.5 C)
Tachycardia
Positive Murphy’s sign
Palpable
Signs & Symptoms
Anorexia.
Low grade fever ( < 38.5 C)
Tachycardia
Positive Murphy’s sign
Palpable
Слайд 26P/E
Pt distressed by pain and lies quitely breathing shallowly.
Tachycardia and Pyrexia
Tenderness
P/E
Pt distressed by pain and lies quitely breathing shallowly.
Tachycardia and Pyrexia
Tenderness
Слайд 27Physical features of enlarged GB
It appears from beneath the tip of the
Physical features of enlarged GB
It appears from beneath the tip of the
Слайд 28Differential diagnosis
Perforating or penetrating peptic ulcer.
Myocardial infraction
Pancreatitis
Hiatus hernia
RLL pneumonia
Appendicitis
Hepatitis
Differential diagnosis
Perforating or penetrating peptic ulcer.
Myocardial infraction
Pancreatitis
Hiatus hernia
RLL pneumonia
Appendicitis
Hepatitis
Слайд 29Lab Investigations
Leukocystosis
Mild Hyperbillirubinemia
Mild ↑ AST, ALT, ALP
Moderate ↑ Lipase & Amylase
Lab Investigations
Leukocystosis
Mild Hyperbillirubinemia
Mild ↑ AST, ALT, ALP
Moderate ↑ Lipase & Amylase
Слайд 30US
Distended gallbladder
Thickened gallbladdr wall
Pericholecystic fluid collection
US Murphy’s sign ( + in 98%
US
Distended gallbladder
Thickened gallbladdr wall
Pericholecystic fluid collection
US Murphy’s sign ( + in 98%
Слайд 31Biliary scintigraphy (hydroxyiminodiacetic acid) (HIDA) scan:
Is the gold standard investigation
Biliary scintigraphy (hydroxyiminodiacetic acid) (HIDA) scan:
Is the gold standard investigation
Слайд 32(HIDA) scan:
The patient is given an intravenous injection of radiolabelled hydroxyiminodiacetic acid
(HIDA) scan:
The patient is given an intravenous injection of radiolabelled hydroxyiminodiacetic acid
Слайд 33(HIDA) scan:
(HIDA) scan:
Слайд 34Complication
- Cholecystentiric fistula formation
- Gallstone illeus
- Perforation (may cause localized abscess
Complication
- Cholecystentiric fistula formation
- Gallstone illeus
- Perforation (may cause localized abscess
Слайд 35Mx
NPO
IVF
IV Analgesia (pethidine)
IV Abx (cefuroxime)
NGT
Parental Analgesics
Optimal Rx is cholecystectomy within 3 days
Mx
NPO
IVF
IV Analgesia (pethidine)
IV Abx (cefuroxime)
NGT
Parental Analgesics
Optimal Rx is cholecystectomy within 3 days
Слайд 36Calot’s Triangle
Superiorly: Lower edge of the liver
Laterally: Cystic Duct
Medially: Common Hepatic Duct
Calot’s Triangle
Superiorly: Lower edge of the liver
Laterally: Cystic Duct
Medially: Common Hepatic Duct
Слайд 37Acute Cholecystits vs. Billiary Colic
Duration, Symptoms ?
Acute Cholecystits vs. Billiary Colic
Duration, Symptoms ?
Слайд 38
Surgery
Surgery
Слайд 39Laproscopic
Laproscopic
Слайд 40
Questions
Questions
 Political systems of the world and the Nenets autonomous okrug
Political systems of the world and the Nenets autonomous okrug АРЕНДА БЕТОНОНАСОСОВ
АРЕНДА БЕТОНОНАСОСОВ Презентация на тему В экваториальном лесу Южной Америки
Презентация на тему В экваториальном лесу Южной Америки Работа с бумагой
Работа с бумагой Большая китайская панда
Большая китайская панда Совещание с Дистрибьюторами г.Москва в рамках регионального совещания в г.Москва
Совещание с Дистрибьюторами г.Москва в рамках регионального совещания в г.Москва Крестики – нолики
Крестики – нолики Реконструкция Политехнического музея
Реконструкция Политехнического музея Блюдо из птицы
Блюдо из птицы Е.Л. Николаева Президент НАМИКС
Е.Л. Николаева Президент НАМИКС Казачество
Казачество 3. Types of Computer
3. Types of Computer Курс «Взаимодействие с заинтересованными сторонами и планирование деятельности в соответствии со стандартом AA1000 SES»
Курс «Взаимодействие с заинтересованными сторонами и планирование деятельности в соответствии со стандартом AA1000 SES» Эскиз
Эскиз «Оценивание программ и политик: методология и применение» - от межфакультетского семинара (2004-2005) к общегородскому коллоквиуму И
«Оценивание программ и политик: методология и применение» - от межфакультетского семинара (2004-2005) к общегородскому коллоквиуму И Мастер-класс Рисование пластилином картин
Мастер-класс Рисование пластилином картин Комплекс по сжижению, хранению и отгрузке СПГ в районе КС Портовая (Ленинградская область)
Комплекс по сжижению, хранению и отгрузке СПГ в районе КС Портовая (Ленинградская область) Новое похождения выпускников, или удивительное путешествие по океану знаний
Новое похождения выпускников, или удивительное путешествие по океану знаний Режимы электроэнергетических систем
Режимы электроэнергетических систем ратцель
ратцель Сравнительный анализ стандартов по географии 8-9 классы
Сравнительный анализ стандартов по географии 8-9 классы Зачем нам нужны растения?
Зачем нам нужны растения? Автоматическое повторное включение
Автоматическое повторное включение ИССЛЕДОВАНИЕ ТЕКСТОВ, ВЫПОЛНЕННЫХ «ПЕЧАТНЫМ» ПОЧЕРКОМ
ИССЛЕДОВАНИЕ ТЕКСТОВ, ВЫПОЛНЕННЫХ «ПЕЧАТНЫМ» ПОЧЕРКОМ МАОУ СОШ №91
МАОУ СОШ №91 Р-даы олданыстаы мырышты-орасынды байыту
Р-даы олданыстаы мырышты-орасынды байыту Детство без границ. Юбилею школы Горького посвящается
Детство без границ. Юбилею школы Горького посвящается Паремии
Паремии