- Pneumonia in children

Содержание
- 2. Pneumonia – polyetiological infectious disease of respiratory system lower parts with alveolar exudation which is confirmed
- 3. Etiologic Agents
- 4. Etiologic Agents Neonates and Young Infants Pneumonia in neonates can manifest as early-onset disease (within the
- 5. Etiologic Agents infants, Children, and Adolescents Viruses account for approximately 14% to 35% of childhood CAPbut
- 6. Etiologic Agents infants, Children, and Adolescents Mycoplasma pneumoniae and Chlamydophila pneumoniae Bacterial Pathogens S. pneumoniaeis the
- 7. Pathogenesis and Pathology
- 8. The pulmonary defense mechanisms Physical barriers of the respiratory tract include the presence of hairs in
- 9. The pulmonary defense mechanisms Mucociliary transport moves normally aspirated oropharyngeal flora and particulate matter up the
- 10. Pneumonia is inflammatory process developed after entry of infectious agent in respiratory portions of airway tract.
- 11. There are 4 ways of pulmonary contamination with pathogens: 1. Aspiration of oropharyngeal contents (microaspiration in
- 12. Pathogenesis of acute pneumonia First – contamination with microorganisms, inflammatory obstruction of upper respiratory ways, disorder
- 13. Pathogenesis of acute pneumonia Third – alteration of not only pathogen but of own organism including
- 14. Pathogenesis of acute pneumonia Fifth – development of respiratory insufficiency and non-respiratory pulmonary functions. Sixth –
- 15. Viruses affection Viral respiratory infections can lead to bronchiolitis, interstitial pneumonia, or parenchymal infection, with overlapping
- 16. Bacteria affection Five pathologic patterns are seen with bacterial pneumonia: 1)parenchymal inflammation of a lobe or
- 17. Stages of lobar pneumonia 1. In the first stage, which occurs within 24 hours of infection,
- 18. Classification
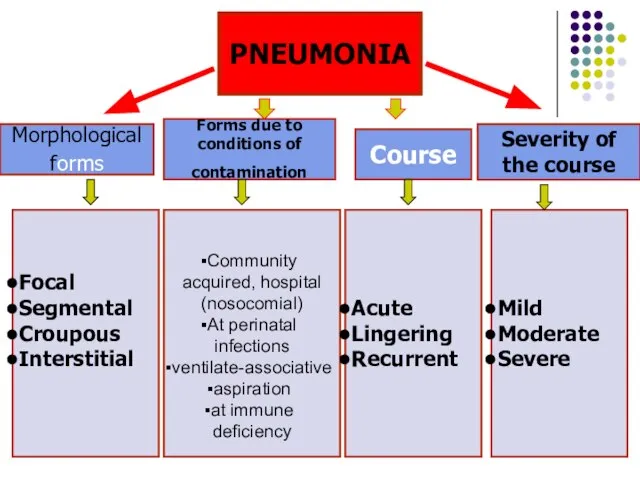
- 19. PNEUMONIA Morphological forms Forms due to conditions of contamination Course Severity of the course Focal Segmental
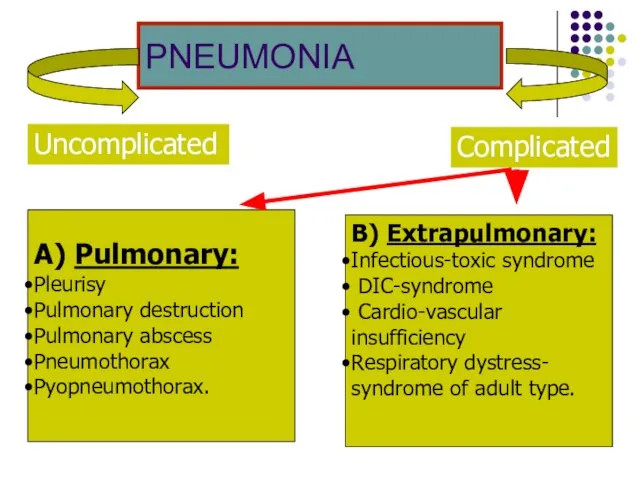
- 20. PNEUMONIA Complicated Uncomplicated А) Pulmonary: Pleurisy Pulmonary destruction Pulmonary abscess Pneumothorax Pyopneumothorax. B) Extrapulmonary: Infectious-toxic syndrome
- 21. Clinical symptoms
- 22. Main signs of pneumonia Symptoms of intoxication, fever Cough (recently started) Tachypnoea Dyspnoea Chest wall retractions
- 23. Pneumonia indications in children younger 5 years of age: Nasal flaring (before 12 months) Oxygen saturation
- 24. Clinical symptoms Newborn and neonates present with: Grunting Poor feeding Irritability or lethargy Tachypnoea sometimes Fever
- 25. Clinical symptoms Infants present with: Cough (the most common symptom after the first four weeks) Tachypnoea
- 26. Clinical symptoms Toddlers/pre-school children: Again, preceding URTI is common Cough is the most common symptom Fever
- 27. Clinical symptoms Older children: There will be additional symptoms to those above More expressive and articulate
- 28. Criteria for Respiratory Distress in Children With Pneumonia Tachypnea: RR breaths/minute >50 for age 3–11 months
- 29. Criteria for CAP Severity of illness Major criteria Invasive mechanical ventilation Fluid refractory shock Acute need
- 30. Percussion & auscultation Local physical signs of pneumonia (shortening of percussion sound in the zone of
- 31. X-ray study Pneumonia diagnosis always includes detecting patchy infiltrative changes in the lung parenchyma with other
- 32. X-ray study used If the diagnosis is questionable This is repeated episode The patient is ill
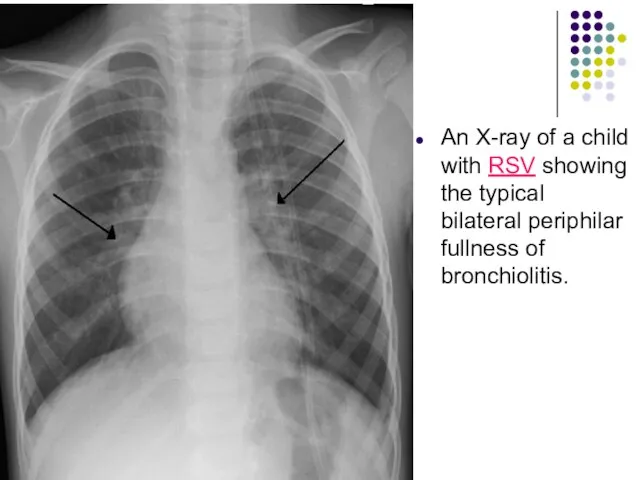
- 33. An X-ray of a child with RSV showing the typical bilateral periphilar fullness of bronchiolitis.
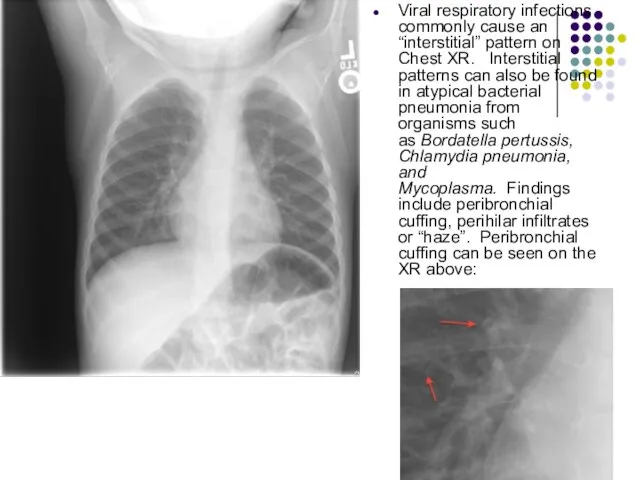
- 34. Viral respiratory infections commonly cause an “interstitial” pattern on Chest XR. Interstitial patterns can also be
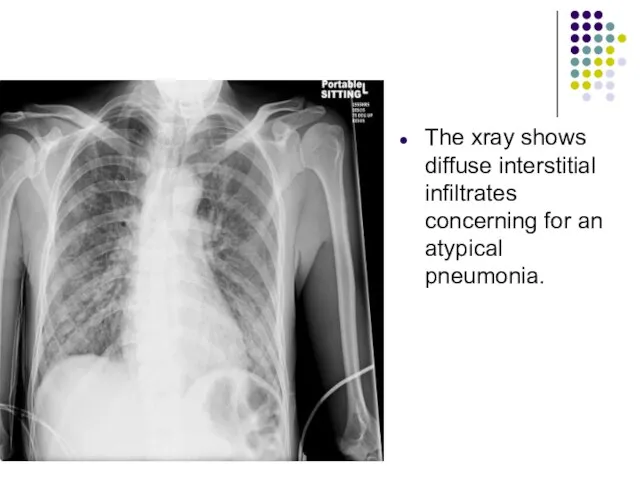
- 35. The xray shows diffuse interstitial infiltrates concerning for an atypical pneumonia.
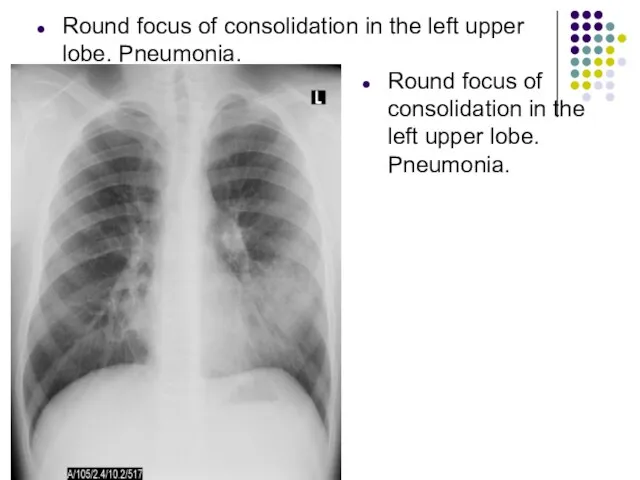
- 36. Round focus of consolidation in the left upper lobe. Pneumonia. Round focus of consolidation in the
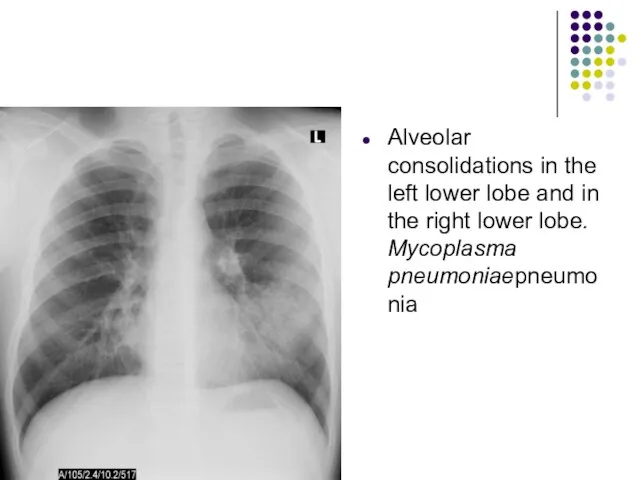
- 37. Alveolar consolidations in the left lower lobe and in the right lower lobe. Mycoplasma pneumoniaepneumonia
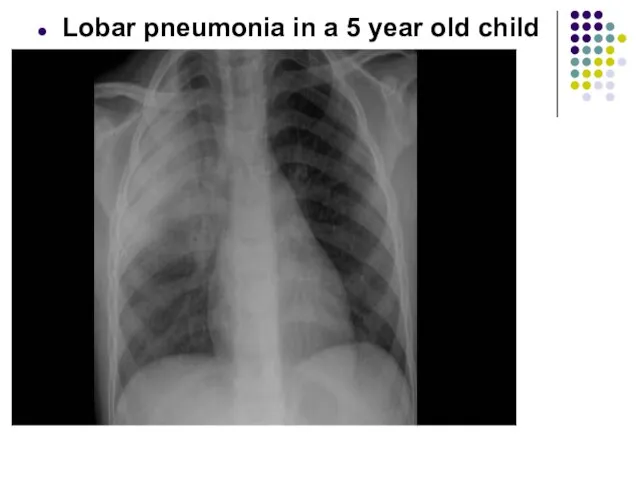
- 38. Lobar pneumonia in a 5 year old child
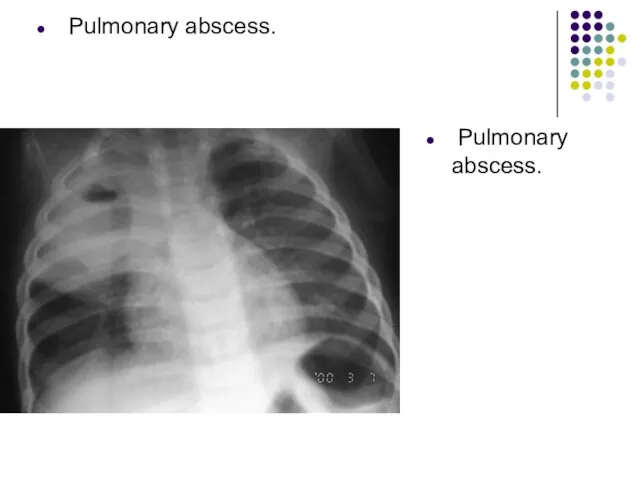
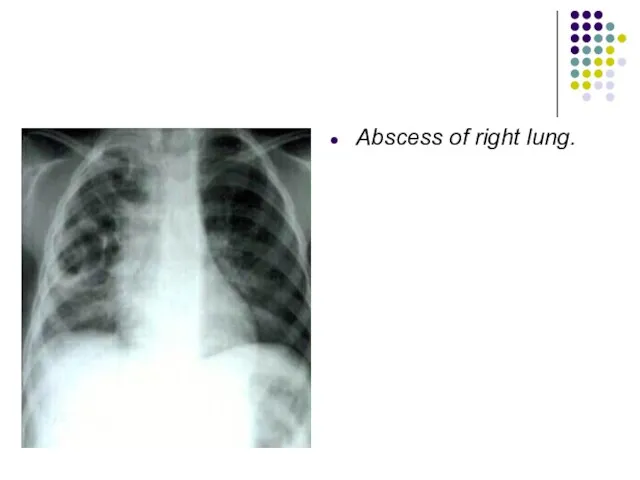
- 39. Pulmonary abscess. Pulmonary abscess.
- 40. Abscess of right lung.
- 41. Sputum Gram Stain and Culture Sputum is rarely produced in children younger than 10 years, and
- 42. Rapid antigen tests are available for RSV, parainfluenza 1, 2, and 3, influenza A and B,
- 43. Serologic testing for IgM or an increase in IgG titers may be performed for Mycoplasma and
- 44. The complete blood count Complete Blood Cell Count may help in determining if an infection is
- 45. Acute-phase reactants erythrocytesedimentation rate (ESR) C-reactive protein (CRP)concentration serum procalcitonin concentration
- 46. Oxygen saturation should be assessed by pulse oximetry in children with respiratory distress, significant tachypnea, or
- 47. Classification of hypoxaemia There are two ways of classifying hypoxaemia in children: (i) WHO classification and
- 48. Clinical picture of focal pneumonia In children of pre-school and school age: Respiratory complaints, symptoms of
- 50. Clinical picture of segmental pneumonia: First variant: -course is favourable, sometimes they aren’t diagnosed because local
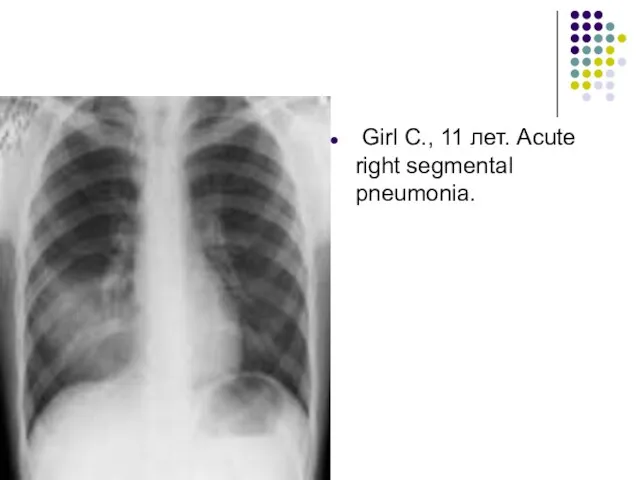
- 51. Girl С., 11 лет. Acute right segmental pneumonia.
- 52. Clinical picture of segmental pneumonia: Second variant: -similar to clinical picture of croupous pneumonia with abrupt
- 53. Clinical picture of croupous pneumonia Onset is abrupt, temperature 39-40°, headache, severe disorders of general condition,
- 54. Mycoplasma pneumoniae Vague and slow-onset history over a few days or weeks of constitutional upset, fever,
- 55. Chlamydophila pneumoniae Gradual onset, which may show improvement before worsening again; incubation period is 3-4 weeks.Initial
- 56. Legionella pneumophila This tends to be the most severe of the pneumonias due to atypical pathogens.
- 57. Hospital-acquired pneumonia This is defined as a new infection of lung parenchyma appearing more than 48
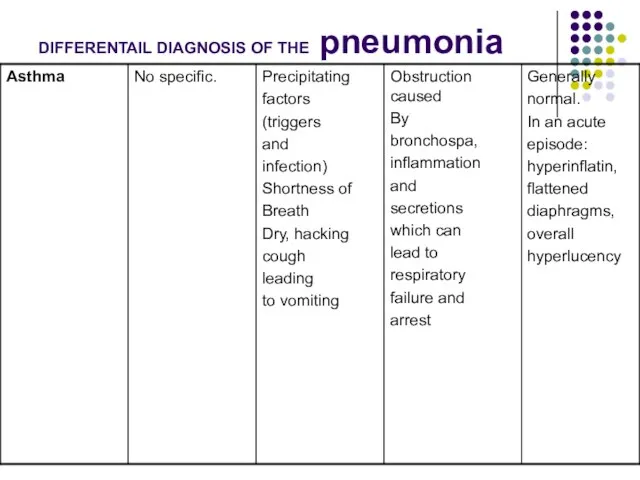
- 58. DIFFERENTAIL DIAGNOSIS OF THE PNEUMONIA Asthma Inhaled foreign body Pneumothorax Cardiac dyspnoea Pneumonitis from other causes:
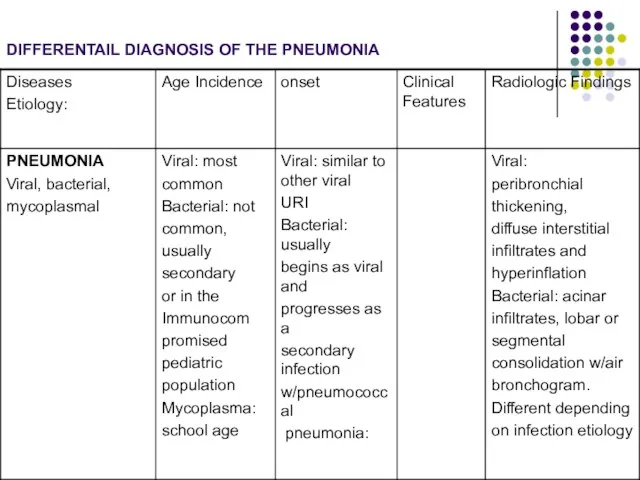
- 59. DIFFERENTAIL DIAGNOSIS OF THE PNEUMONIA
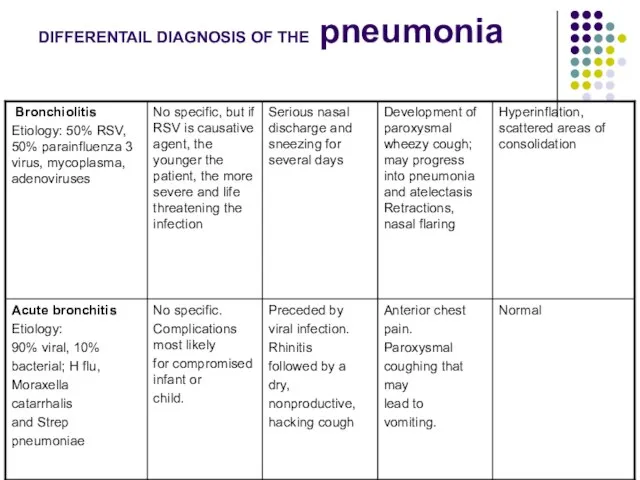
- 60. DIFFERENTAIL DIAGNOSIS OF THE pneumonia
- 61. DIFFERENTAIL DIAGNOSIS OF THE pneumonia
- 62. Algorithm of medical care for a child with pneumonia Health-protective regime Antibiotic therapy. Oxygen-therapy Liquidation of
- 63. Anti-Infective Therapy Should Be Provided to a Child With Suspected CAP ( outpatient) Amoxicillin should be
- 64. Anti-Infective Therapy Should Be Provided to a Child With Suspected CAP ( outpatient) Macrolide antibiotics should
- 65. Preparations of other groups Lincomycin30-60mg/kg oral 10-20mg/kg oral Clindamycin20-40mg/kg oral 10-25mg/kg, i/m, i/v Rifampicin10-20mg/kg oral 10-20mg/kg,
- 66. Preparations of other groups Carbepenems: Imipenem (Tienam) Meropenem 60 mg/kg, i/v Monobactams Aztreonam120-150 mg/kg, i/v Aminoglycosides
- 67. Anti-Infective Therapy Should Be Provided to a Child With Suspected CAP ( outpatient) Influenza antiviral therapy
- 68. Indications for hospital admission 1. Hypoxaemia (oxygen saturation 2. Toxic appearance 3. Respiratory rate >70/minute, or
- 69. Anti-Infective Therapy Should Be Provided to a Child With Suspected CAP ( inpatient) Ampicillin or penicillin
- 70. Anti-Infective Therapy Should Be Provided to a Child With Suspected CAP ( inpatient) Empiric therapy with
- 71. Anti-Infective Therapy Should Be Provided to a Child With Suspected CAP ( inpatient) Empiric combination therapy
- 72. Anti-Infective Therapy Should Be Provided to a Child With Suspected CAP ( inpatient) Vancomycin or clindamycin
- 73. Management of atypical pneumonia Macrolides, such as erythromycin, clarithromycin and azithromycin, have been shown to be
- 74. Indications for oxygen therapy 1. Hypoxaemia (oxygen saturation 2. Central cyanosis 3. Severe lower chest-wall in-drawing
- 75. oxygen therapy a) To ensure free airway, optimization of ventilation (throwing head back, the output of
- 76. Methods of oxygen administration Nasal prongs: are recommended for most children. Nasal prongs give a maximum
- 77. Methods of oxygen administration Headbox: oxygen is well tolerated by young infants. Headbox oxygen requires no
- 78. Antipyretics and analgesics drugs Children with CAP are generally pyrexial and may also have some pain,
- 79. Indications for the use of antipyretics and analgesics in CAP Rectal temperature >39 Celsius There is
- 80. Antipyretics and analgesics drugs The most appropriate agent is paracetamol at a dose of 15 mg/kg/dose
- 81. Liquidation of cardiac, vascular insufficiency strophanthin– 0,05% for children till 1 y.o. 0,1-0,15 ml 1-2 time
- 82. Acute vascular insufficiency Stream i/V prednsolon 2 mg/ kg or hydrocortison 10-15 mg /kg I/V plasma
- 83. Sudden (acute) pulmonary edema symptoms Extreme shortness of breath or difficulty breathing (dyspnea) that worsens when
- 84. Prevention of lung edema oxygen therapy use antifoam drugs (inhalation 30 % C2H5OH 30 - 40
- 85. Anticonvulsion therapy Deacresing hypoxia and Deacresing edema of brain Furosemid i/v 2-3 mg/kg Deacresing excitability –0,5
- 86. Liquidation of toxicity: albumin, plasma, Haemodesum 5-10 ml/kg/day. Correction of acid-alkaline balance: 4% solution of sodium
- 87. Intravenous fluids Intravenous fluids must be used with great care and with caution, and only if
- 88. Indications for I/V fluid Shock Inability to tolerate enteral feeds Sepsis Severe dehydration Gross electrolyte imbalance
- 89. Calorie requirements Adequate nutrition is of particular concern, especially when there are underlying factors such as
- 90. Enteral feeds Children with pneumonia should be encouraged to feed orally unless there are indications for
- 91. Chest physiotherapy postural drainage, percussion of the chest deep breathing exercises should be routinely performed in
- 92. Apparatus physiotherapy during the acute clinical manifestations of acute pneumonia is contrindicated. With the normalization of
- 93. Mucolytic agents Anti-tussive remedies are not recommended as they cause suppression of cough and interfere with
- 94. Compositions of cough mixtures available Category A - Only Antitussive F - Expectorant + Antitussive B
- 95. Postural drainage: There is no evidence for the use of a head-down position for postural drainage.
- 96. Electrophoresis
- 97. Ultraviolet irradiation therapy
- 98. Apparatus for UHF-therapy «UHF 30-2» The apparatus is intended for therapeutic effect on the patient by
- 99. Single-channel laser therapy apparatus that generates the red and infrared radiation, with an open modular system
- 100. Ultrasound therapy apparatus BTL-4710 Sono Professional
- 101. Complication of pneumonia
- 102. Pulmonary Complication Pleural effusion or empyema Pneumothorax Lung abscess Bronchopleural fistula Necrotizing pneumonia Acute respiratory failure
- 103. Metastatic Complication Meningitis Central nervous system abscess Pericarditis Endocarditis Osteomyelitis Septic arthritis Systemic Complication Systemic inflammatory
- 105. Скачать презентацию
Слайд 2Pneumonia – polyetiological infectious disease of respiratory system lower parts with alveolar
Pneumonia – polyetiological infectious disease of respiratory system lower parts with alveolar
Слайд 3Etiologic Agents
Etiologic Agents
Слайд 4Etiologic Agents
Neonates and Young Infants
Pneumonia in neonates can manifest as early-onset
Etiologic Agents
Neonates and Young Infants
Pneumonia in neonates can manifest as early-onset

Слайд 5Etiologic Agents
infants, Children, and Adolescents
Viruses account for approximately 14% to 35% of
Etiologic Agents
infants, Children, and Adolescents
Viruses account for approximately 14% to 35% of
Слайд 6Etiologic Agents
infants, Children, and Adolescents
Mycoplasma pneumoniae and
Chlamydophila pneumoniae
Bacterial Pathogens
S. pneumoniaeis the single most common
Etiologic Agents
infants, Children, and Adolescents
Mycoplasma pneumoniae and
Chlamydophila pneumoniae
Bacterial Pathogens
S. pneumoniaeis the single most common
Слайд 7Pathogenesis
and Pathology
Pathogenesis
and Pathology
Слайд 8The pulmonary defense mechanisms
Physical barriers of the respiratory tract include the presence
The pulmonary defense mechanisms
Physical barriers of the respiratory tract include the presence
Слайд 9The pulmonary defense mechanisms
Mucociliary transport moves normally aspirated oropharyngeal flora and
The pulmonary defense mechanisms
Mucociliary transport moves normally aspirated oropharyngeal flora and
Слайд 10Pneumonia is inflammatory process developed after entry of infectious agent in respiratory
Pneumonia is inflammatory process developed after entry of infectious agent in respiratory
Слайд 11There are 4 ways of pulmonary contamination with pathogens:
1. Aspiration of oropharyngeal
There are 4 ways of pulmonary contamination with pathogens: 1. Aspiration of oropharyngeal
Слайд 12Pathogenesis of acute pneumonia
First – contamination with microorganisms, inflammatory obstruction of upper
Pathogenesis of acute pneumonia
First – contamination with microorganisms, inflammatory obstruction of upper
Слайд 13Pathogenesis of acute pneumonia
Third – alteration of not only pathogen but of
Pathogenesis of acute pneumonia
Third – alteration of not only pathogen but of
Слайд 14Pathogenesis of acute pneumonia
Fifth – development of respiratory insufficiency and non-respiratory pulmonary
Pathogenesis of acute pneumonia
Fifth – development of respiratory insufficiency and non-respiratory pulmonary
Слайд 15Viruses affection
Viral respiratory infections can lead to bronchiolitis, interstitial pneumonia, or parenchymal
Viruses affection
Viral respiratory infections can lead to bronchiolitis, interstitial pneumonia, or parenchymal
Слайд 16Bacteria affection
Five pathologic patterns are seen with bacterial pneumonia:
1)parenchymal inflammation of
Bacteria affection
Five pathologic patterns are seen with bacterial pneumonia:
1)parenchymal inflammation of
Слайд 17Stages of lobar pneumonia
1. In the first stage, which occurs within 24
Stages of lobar pneumonia
1. In the first stage, which occurs within 24
Слайд 18Classification
Classification
Слайд 19PNEUMONIA
Morphological forms
Forms due to conditions of contamination
Course
Severity of the
PNEUMONIA
Morphological forms
Forms due to conditions of contamination
Course
Severity of the
Слайд 20PNEUMONIA
Complicated
Uncomplicated
А) Pulmonary:
Pleurisy
Pulmonary destruction
Pulmonary abscess
Pneumothorax
Pyopneumothorax.
B) Extrapulmonary:
Infectious-toxic syndrome
DIC-syndrome
Cardio-vascular insufficiency
Respiratory dystress-
syndrome of
PNEUMONIA
Complicated
Uncomplicated
А) Pulmonary:
Pleurisy
Pulmonary destruction
Pulmonary abscess
Pneumothorax
Pyopneumothorax.
B) Extrapulmonary:
Infectious-toxic syndrome
DIC-syndrome
Cardio-vascular insufficiency
Respiratory dystress-
syndrome of
Слайд 21Clinical symptoms
Clinical symptoms

Слайд 22Main signs of pneumonia
Symptoms of intoxication, fever
Cough (recently started)
Tachypnoea
Dyspnoea
Chest wall retractions
Nasal flaring
Percustory
Main signs of pneumonia
Symptoms of intoxication, fever
Cough (recently started)
Tachypnoea
Dyspnoea
Chest wall retractions
Nasal flaring
Percustory
Слайд 23Pneumonia indications in children younger 5 years of age:
Nasal flaring (before 12
Pneumonia indications in children younger 5 years of age:
Nasal flaring (before 12
Слайд 24Clinical symptoms
Newborn and neonates present with:
Grunting
Poor feeding
Irritability or lethargy
Tachypnoea sometimes
Fever (but neonates may
Clinical symptoms
Newborn and neonates present with:
Grunting
Poor feeding
Irritability or lethargy
Tachypnoea sometimes
Fever (but neonates may
Слайд 25Clinical symptoms
Infants present with:
Cough (the most common symptom after the first four weeks)
Tachypnoea
Clinical symptoms
Infants present with:
Cough (the most common symptom after the first four weeks)
Tachypnoea
Слайд 26Clinical symptoms
Toddlers/pre-school children:
Again, preceding URTI is common
Cough is the most common symptom
Fever
Clinical symptoms
Toddlers/pre-school children:
Again, preceding URTI is common
Cough is the most common symptom
Fever
Слайд 27Clinical symptoms
Older children:
There will be additional symptoms to those above
More expressive and
Clinical symptoms
Older children:
There will be additional symptoms to those above
More expressive and
Слайд 28Criteria for Respiratory Distress in Children With
Pneumonia
Tachypnea: RR breaths/minute
>50 for age 3–11
Criteria for Respiratory Distress in Children With
Pneumonia
Tachypnea: RR breaths/minute
>50 for age 3–11
Слайд 29Criteria for CAP Severity of illness
Major criteria
Invasive mechanical ventilation
Fluid refractory shock
Acute need
Criteria for CAP Severity of illness
Major criteria
Invasive mechanical ventilation
Fluid refractory shock
Acute need
Слайд 30Percussion & auscultation
Local physical signs of pneumonia (shortening of percussion sound in
Percussion & auscultation
Local physical signs of pneumonia (shortening of percussion sound in
Слайд 31X-ray study
Pneumonia diagnosis always includes detecting patchy infiltrative changes in the lung
X-ray study
Pneumonia diagnosis always includes detecting patchy infiltrative changes in the lung
Слайд 32X-ray study used
If the diagnosis is questionable
This is repeated episode
The patient is
X-ray study used
If the diagnosis is questionable
This is repeated episode
The patient is
Слайд 33An X-ray of a child with RSV showing the typical bilateral periphilar fullness of bronchiolitis.
An X-ray of a child with RSV showing the typical bilateral periphilar fullness of bronchiolitis.
Слайд 34Viral respiratory infections commonly cause an “interstitial” pattern on Chest XR. Interstitial
Viral respiratory infections commonly cause an “interstitial” pattern on Chest XR. Interstitial
Слайд 35The xray shows diffuse interstitial infiltrates concerning for an atypical pneumonia.
The xray shows diffuse interstitial infiltrates concerning for an atypical pneumonia.
Слайд 36Round focus of consolidation in the left upper lobe. Pneumonia.
Round focus
Round focus of consolidation in the left upper lobe. Pneumonia.
Round focus
Слайд 37Alveolar consolidations in the left lower lobe and in the right lower
Alveolar consolidations in the left lower lobe and in the right lower
Слайд 38Lobar pneumonia in a 5 year old child
Lobar pneumonia in a 5 year old child
Слайд 39 Pulmonary abscess.
Pulmonary abscess.
Pulmonary abscess.
Pulmonary abscess.
Слайд 40Abscess of right lung.
Abscess of right lung.
Слайд 41Sputum Gram Stain and Culture
Sputum is rarely produced in children younger than
Sputum Gram Stain and Culture
Sputum is rarely produced in children younger than
Слайд 42Rapid antigen tests
are available for RSV, parainfluenza 1, 2, and 3, influenza
Rapid antigen tests
are available for RSV, parainfluenza 1, 2, and 3, influenza
Слайд 43Serologic testing
for IgM or an increase in IgG titers may be performed
Serologic testing
for IgM or an increase in IgG titers may be performed
Слайд 44The complete blood count
Complete Blood Cell Count may help in determining if
The complete blood count
Complete Blood Cell Count may help in determining if
Слайд 45Acute-phase reactants
erythrocytesedimentation rate (ESR)
C-reactive protein (CRP)concentration
serum procalcitonin concentration
Acute-phase reactants
erythrocytesedimentation rate (ESR)
C-reactive protein (CRP)concentration
serum procalcitonin concentration
Слайд 46Oxygen saturation
should be assessed by pulse oximetry in children with respiratory distress,
Oxygen saturation
should be assessed by pulse oximetry in children with respiratory distress,
Слайд 47Classification of hypoxaemia
There are two ways of classifying hypoxaemia in children: (i)
Classification of hypoxaemia
There are two ways of classifying hypoxaemia in children: (i)
Слайд 48Clinical picture of focal pneumonia
In children of pre-school and school age:
Clinical picture of focal pneumonia
In children of pre-school and school age:

Слайд 50Clinical picture of segmental pneumonia:
First variant:
-course is favourable, sometimes they aren’t diagnosed
Clinical picture of segmental pneumonia:
First variant: -course is favourable, sometimes they aren’t diagnosed
Слайд 51 Girl С., 11 лет. Acute right segmental pneumonia.
Girl С., 11 лет. Acute right segmental pneumonia.
Слайд 52Clinical picture of segmental pneumonia:
Second variant:
-similar to clinical picture of croupous pneumonia
Clinical picture of segmental pneumonia:
Second variant: -similar to clinical picture of croupous pneumonia
Слайд 53Clinical picture of croupous pneumonia
Onset is abrupt, temperature 39-40°, headache, severe
Clinical picture of croupous pneumonia
Onset is abrupt, temperature 39-40°, headache, severe
Слайд 54Mycoplasma pneumoniae
Vague and slow-onset history over a few days or weeks of
Mycoplasma pneumoniae
Vague and slow-onset history over a few days or weeks of
Слайд 55Chlamydophila pneumoniae
Gradual onset, which may show improvement before worsening
again; incubation period
Chlamydophila pneumoniae
Gradual onset, which may show improvement before worsening
again; incubation period
Слайд 56Legionella pneumophila
This tends to be the most severe of the pneumonias due
Legionella pneumophila
This tends to be the most severe of the pneumonias due
Слайд 57Hospital-acquired pneumonia
This is defined as a new infection of lung parenchyma appearing
Hospital-acquired pneumonia
This is defined as a new infection of lung parenchyma appearing
Слайд 58DIFFERENTAIL DIAGNOSIS OF THE PNEUMONIA
Asthma
Inhaled foreign body
Pneumothorax
Cardiac dyspnoea
Pneumonitis from other causes:
Extrinsic allergic
DIFFERENTAIL DIAGNOSIS OF THE PNEUMONIA
Asthma
Inhaled foreign body
Pneumothorax
Cardiac dyspnoea
Pneumonitis from other causes:
Extrinsic allergic
Слайд 59DIFFERENTAIL DIAGNOSIS OF THE PNEUMONIA
DIFFERENTAIL DIAGNOSIS OF THE PNEUMONIA
Слайд 60DIFFERENTAIL DIAGNOSIS OF THE pneumonia
DIFFERENTAIL DIAGNOSIS OF THE pneumonia
Слайд 61DIFFERENTAIL DIAGNOSIS OF THE pneumonia
DIFFERENTAIL DIAGNOSIS OF THE pneumonia
Слайд 62Algorithm of medical care for a child with pneumonia
Health-protective regime
Antibiotic therapy.
Oxygen-therapy
Liquidation
Algorithm of medical care for a child with pneumonia
Health-protective regime
Antibiotic therapy.
Oxygen-therapy
Liquidation
Слайд 63Anti-Infective Therapy Should Be Provided to a Child
With Suspected CAP ( outpatient)
Anti-Infective Therapy Should Be Provided to a Child
With Suspected CAP ( outpatient)
Слайд 64Anti-Infective Therapy Should Be Provided to a Child
With Suspected CAP ( outpatient)
Anti-Infective Therapy Should Be Provided to a Child
With Suspected CAP ( outpatient)
Слайд 65Preparations of other groups
Lincomycin30-60mg/kg oral 10-20mg/kg oral
Clindamycin20-40mg/kg oral 10-25mg/kg, i/m, i/v
Rifampicin10-20mg/kg oral 10-20mg/kg, i/m, i/v
Preparations of other groups
Lincomycin30-60mg/kg oral 10-20mg/kg oral
Clindamycin20-40mg/kg oral 10-25mg/kg, i/m, i/v
Rifampicin10-20mg/kg oral 10-20mg/kg, i/m, i/v
Слайд 66Preparations of other groups
Carbepenems:
Imipenem (Tienam) Meropenem 60 mg/kg, i/v
Monobactams
Aztreonam120-150 mg/kg, i/v
Aminoglycosides
Gentamicin 5 mg/kg, i/m, i/v
Amicacin 15-20 mg/kg, i/v
Preparations of other groups
Carbepenems:
Imipenem (Tienam) Meropenem 60 mg/kg, i/v
Monobactams
Aztreonam120-150 mg/kg, i/v
Aminoglycosides
Gentamicin 5 mg/kg, i/m, i/v
Amicacin 15-20 mg/kg, i/v
Слайд 67Anti-Infective Therapy Should Be Provided to a Child With Suspected CAP (
Anti-Infective Therapy Should Be Provided to a Child With Suspected CAP (
Слайд 68Indications for hospital admission
1. Hypoxaemia (oxygen saturation <90% in room air at
Indications for hospital admission
1. Hypoxaemia (oxygen saturation <90% in room air at
Слайд 69Anti-Infective Therapy Should Be Provided to a Child
With Suspected CAP ( inpatient)
Ampicillin
Anti-Infective Therapy Should Be Provided to a Child
With Suspected CAP ( inpatient)
Ampicillin
Слайд 70Anti-Infective Therapy Should Be Provided to a Child
With Suspected CAP ( inpatient)
Empiric
Anti-Infective Therapy Should Be Provided to a Child
With Suspected CAP ( inpatient)
Empiric
Слайд 71Anti-Infective Therapy Should Be Provided to a Child With Suspected CAP (
Anti-Infective Therapy Should Be Provided to a Child With Suspected CAP (
Слайд 72Anti-Infective Therapy Should Be Provided to a Child With Suspected CAP (
Anti-Infective Therapy Should Be Provided to a Child With Suspected CAP (
Слайд 73Management of atypical pneumonia
Macrolides, such as erythromycin, clarithromycin and azithromycin, have been
Management of atypical pneumonia
Macrolides, such as erythromycin, clarithromycin and azithromycin, have been
Слайд 74Indications for oxygen therapy
1. Hypoxaemia (oxygen saturation <90% in room air at
Indications for oxygen therapy
1. Hypoxaemia (oxygen saturation <90% in room air at
Слайд 75oxygen therapy
a) To ensure free airway, optimization of ventilation (throwing head back,
oxygen therapy
a) To ensure free airway, optimization of ventilation (throwing head back,
Слайд 76Methods of oxygen administration
Nasal prongs: are recommended for most children. Nasal prongs
Methods of oxygen administration
Nasal prongs: are recommended for most children. Nasal prongs
Слайд 77Methods of oxygen administration
Headbox: oxygen is well tolerated by young infants. Headbox
Methods of oxygen administration
Headbox: oxygen is well tolerated by young infants. Headbox
Слайд 78Antipyretics and analgesics drugs
Children with CAP are generally pyrexial and may also
Antipyretics and analgesics drugs
Children with CAP are generally pyrexial and may also
Слайд 79Indications for the use of antipyretics and analgesics in CAP
Rectal temperature
Indications for the use of antipyretics and analgesics in CAP
Rectal temperature
Слайд 80Antipyretics and analgesics drugs
The most appropriate agent is paracetamol at a dose
Antipyretics and analgesics drugs
The most appropriate agent is paracetamol at a dose
Слайд 81Liquidation of cardiac, vascular insufficiency
strophanthin– 0,05% for children till 1 y.o. 0,1-0,15
Liquidation of cardiac, vascular insufficiency
strophanthin– 0,05% for children till 1 y.o. 0,1-0,15
Слайд 82Acute vascular insufficiency
Stream i/V prednsolon 2 mg/ kg or hydrocortison 10-15 mg
Acute vascular insufficiency
Stream i/V prednsolon 2 mg/ kg or hydrocortison 10-15 mg
Слайд 83Sudden (acute) pulmonary edema symptoms
Extreme shortness of breath or difficulty breathing (dyspnea)
Sudden (acute) pulmonary edema symptoms
Extreme shortness of breath or difficulty breathing (dyspnea)
Слайд 84Prevention of lung edema
oxygen therapy
use antifoam drugs (inhalation 30 % C2H5OH
Prevention of lung edema
oxygen therapy
use antifoam drugs (inhalation 30 % C2H5OH
Слайд 85Anticonvulsion therapy
Deacresing hypoxia and
Deacresing edema of brain Furosemid i/v 2-3 mg/kg
Deacresing excitability
Anticonvulsion therapy
Deacresing hypoxia and
Deacresing edema of brain Furosemid i/v 2-3 mg/kg
Deacresing excitability
Слайд 86Liquidation of toxicity: albumin, plasma, Haemodesum 5-10 ml/kg/day.
Correction of acid-alkaline balance: 4% solution
Liquidation of toxicity: albumin, plasma, Haemodesum 5-10 ml/kg/day.
Correction of acid-alkaline balance: 4% solution
Слайд 87Intravenous fluids
Intravenous fluids must be used with great care and with caution,
Intravenous fluids
Intravenous fluids must be used with great care and with caution,
Слайд 88Indications for I/V fluid
Shock
Inability to tolerate enteral feeds
Sepsis
Severe dehydration
Indications for I/V fluid
Shock
Inability to tolerate enteral feeds
Sepsis
Severe dehydration
Слайд 89Calorie requirements
Adequate nutrition is of particular concern, especially when there are
Calorie requirements
Adequate nutrition is of particular concern, especially when there are
Слайд 90Enteral feeds
Children with pneumonia should be encouraged to feed orally unless there
Enteral feeds
Children with pneumonia should be encouraged to feed orally unless there
Слайд 91Chest physiotherapy
postural drainage,
percussion of the chest
deep breathing exercises should be
Chest physiotherapy
postural drainage,
percussion of the chest
deep breathing exercises should be
Слайд 92Apparatus physiotherapy
during the acute clinical manifestations of acute pneumonia is contrindicated. With the
Apparatus physiotherapy
during the acute clinical manifestations of acute pneumonia is contrindicated. With the
Слайд 93Mucolytic agents
Anti-tussive remedies are not recommended as they cause suppression of
Mucolytic agents
Anti-tussive remedies are not recommended as they cause suppression of
Слайд 94Compositions of cough mixtures available
Category
A - Only Antitussive F - Expectorant +
Compositions of cough mixtures available
Category
A - Only Antitussive F - Expectorant +
Слайд 95Postural drainage: There is no evidence for the use of a head-down
Postural drainage: There is no evidence for the use of a head-down
Слайд 96 Electrophoresis
Electrophoresis
Слайд 97Ultraviolet irradiation therapy
Ultraviolet irradiation therapy

Слайд 98Apparatus for UHF-therapy «UHF 30-2» The apparatus is intended for therapeutic effect on the patient by ultra
Apparatus for UHF-therapy «UHF 30-2» The apparatus is intended for therapeutic effect on the patient by ultra
Слайд 99Single-channel laser therapy apparatus that generates the red and infrared radiation, with
Single-channel laser therapy apparatus that generates the red and infrared radiation, with
Слайд 100Ultrasound therapy apparatus BTL-4710 Sono Professional
Ultrasound therapy apparatus BTL-4710 Sono Professional

Слайд 101Complication of pneumonia
Complication of pneumonia
Слайд 102Pulmonary Complication
Pleural effusion or empyema
Pneumothorax
Lung abscess
Bronchopleural fistula
Necrotizing pneumonia
Acute respiratory failure
Pulmonary Complication
Pleural effusion or empyema
Pneumothorax
Lung abscess
Bronchopleural fistula
Necrotizing pneumonia
Acute respiratory failure
Слайд 103Metastatic Complication
Meningitis
Central nervous system abscess
Pericarditis
Endocarditis
Osteomyelitis
Septic arthritis
Systemic Complication
Systemic inflammatory response syndrome or
Metastatic Complication
Meningitis
Central nervous system abscess
Pericarditis
Endocarditis
Osteomyelitis
Septic arthritis
Systemic Complication
Systemic inflammatory response syndrome or
 О реализации Федерального закона «О размещении заказов на поставки товаров, выполнение работ, оказание услуг для государственны
О реализации Федерального закона «О размещении заказов на поставки товаров, выполнение работ, оказание услуг для государственны Урок по истории Древнего мира в 5 классе.
Урок по истории Древнего мира в 5 классе. навыки комм в деловых переговорах
навыки комм в деловых переговорах Презентация на тему: Построим дом
Презентация на тему: Построим дом Лингвострановедческий аспект учебника
Лингвострановедческий аспект учебника Расчет точки безубыточности функционирования логистической системы
Расчет точки безубыточности функционирования логистической системы Вкусный крафт. The Bar Botanist
Вкусный крафт. The Bar Botanist Государственный музей изобразительных искусств имени А.С.Пушкина
Государственный музей изобразительных искусств имени А.С.Пушкина Народные ремесла
Народные ремесла Презентация на тему Мальтийский орден
Презентация на тему Мальтийский орден М О Я Р О Д И Н А - Р О С С И Я
М О Я Р О Д И Н А - Р О С С И Я Методы преодоления кризисных явлений в системе образования Смирнов Н.В. профессор кафедры моделирования экономических сис
Методы преодоления кризисных явлений в системе образования Смирнов Н.В. профессор кафедры моделирования экономических сис Экологическое право
Экологическое право Приёмы работы с пластилином
Приёмы работы с пластилином «Металлы»
«Металлы» Что такое техносфера
Что такое техносфера Презентация мероприятий на призы номинаций и кубок Всероссийского общественного объединения ветеранов Боевое братство
Презентация мероприятий на призы номинаций и кубок Всероссийского общественного объединения ветеранов Боевое братство Организация распространения изданий в ИД «АЛТАПРЕСС»
Организация распространения изданий в ИД «АЛТАПРЕСС» Королева Елизавета I
Королева Елизавета I Описание природы. Зима
Описание природы. Зима Развитие платформы интегральной фотоники для телекоммуникационного оборудования
Развитие платформы интегральной фотоники для телекоммуникационного оборудования Белый фосфор
Белый фосфор Структура системы исполнительных органов власти в Российской Федерации
Структура системы исполнительных органов власти в Российской Федерации Репликация, транскрипция
Репликация, транскрипция Информационные технологии в сфере безопасности. Лекция 1. Вводная
Информационные технологии в сфере безопасности. Лекция 1. Вводная Гений Приморья. Ломоносов
Гений Приморья. Ломоносов Мы должны гордиться тем, что живем в одном из красивейших уголков Западной Сибири, с относительно благополучной экологической обс
Мы должны гордиться тем, что живем в одном из красивейших уголков Западной Сибири, с относительно благополучной экологической обс Pridex+. Оценка эффективности деятельности
Pridex+. Оценка эффективности деятельности