- ANTIBIOTICS

Содержание
- 2. SOME GENERAL PRINCIPLES Antibiotics can be naturally produced, semi-synthetic, or synthetic substances Designed to have as
- 3. EXAMPLES OF SELECTIVE ACTION Penicillin on bacterial cell wall (organisms without cell wall won’t be inhibited
- 4. ANTIBIOTICS ACTING ON CELL WALL OF BACTERIA Beta lactams: Penicillins, cephalosporins, carbapenems, monobactam Glycopeptides: Vancomycin, teicoplanin
- 5. THE IDEAL ANTIBIOTIC?:PENICILLIN Narrow spectrum Bactericidal Very selective mode of action Low serum protein binding Widely
- 6. THE DEVELOPMENT OF THE BETA LACTAMS Benzylenicillin and early cephalosporins mainly active against gram positive bacteria
- 7. BENZYLPENICILLIN: MAIN INDICATIONS Strep pyogenes sepsis (from sore throat to fasciitis) Pneumococcal pneumonia, meningitis Meningococcal meningitis,
- 8. Broader spectrum penicillins Ampicillin, amoxycillin cover most organisms hit by penicillin but also Esch coli, some
- 9. Organisms producing TEM1beta lactamase Haemophilus influenzae Neisseria gonorrhoeae Bacteroides fragilis Staph aureus Esch coli
- 10. Carbapenems Imipenem, meropenem: have a very broad spectrum activity against gram-negative bacteria, anaerobes, streps Now used
- 11. PENICILLIN IS GENERALLY VERY SAFE BUT…. Allergic reactions not uncommon-rashes Most severe reaction being anaphylaxis A
- 12. What antibiotics can be used in penicillin allergy? Macrolides: erythromycin, clarithromycin (mainly gram positive cover) Quinolones:
- 13. REMEMBER WHAT THE OTHER BETA LACTAMS ARE: All penicillins: ampicillin, augmentin, piperacillin, cloxacillin Cephalosporins: cefuroxime, cefotaxime,
- 14. CLOXACILLIN Narrow spectrum: Staph aureus (MSSA) Stable to TEM1 beta lactamase Similar antibiotics are methicillin, nafcillin
- 15. Cephalosporins: main uses Cefuroxime: surgical prophylaxis Cefotaxime/ceftriaxone: meningitis nosocomial infections excluding Pseudomonal, Ceftazidime: nosocomial infections including
- 16. Problems with antibiotic resistance: how does it happen? Some bacteria are naturally resistant to particular antibiotics
- 17. Current major antibiotic resistance problems: community infections Respiratory tract: penicillin resistance in pneumococcus (5-10%) Gastrointestinal: quinolone
- 18. Current major resistance problems: hospital infections MRSA: current strains are often multiply-antibiotic resistant VISA/GISA: intermediate resistance
- 19. Other major antibiotic groups: aminoglycosides Gentamicin, amikacin (tobramycin, streptomycin) Mainly active against gram negative bacteria Mainly
- 20. How we give aminoglycosides For serious nosocomial infections: “extended interval” or once daily dosing 5 or
- 21. Some indications and limitations of particular antibiotics
- 22. Community acquired pneumonia Pneumococcus (and H influenzae) are most likely: therefore ampicillin, amoxycillin or augmentin Severe
- 23. Community acquired urinary infections Ampicillin, amoxycillin, augmentin Oral cephalosporin: cephradine Trimethroprim Nalidixic acid Nitrofurantoin Ciprofloxacin Mecillinam
- 24. Skin and soft tissue infections Cellulitis ? Streptococcal: penicillin or augmentin Infected eczema ? Staphylococccal/mixed: penicillin+flucloxacillin
- 25. Where there is deep-seated infection: bone, abscess Need an antibiotic with good tissue and phagocyte penetration
- 26. Why do we use combination therapy? When treating serious infection empirically we want to cover a
- 27. Factors to consider when prescribing an antibiotic Any history of allergy, toxicity? Is it appropriate for
- 28. Some other antibiotics occasionally used Co-trimoxazole (Stenotrophomonas) Chloramphenicol (typhoid fever, meningitis) Colistin (resistant Pseudomonas) topical Neomycin:
- 30. Скачать презентацию
Слайд 2SOME GENERAL PRINCIPLES
Antibiotics can be naturally produced, semi-synthetic, or synthetic substances
Designed to
SOME GENERAL PRINCIPLES
Antibiotics can be naturally produced, semi-synthetic, or synthetic substances
Designed to
Слайд 3EXAMPLES OF SELECTIVE ACTION
Penicillin on bacterial cell wall (organisms without cell wall
EXAMPLES OF SELECTIVE ACTION
Penicillin on bacterial cell wall (organisms without cell wall
Слайд 4ANTIBIOTICS ACTING ON CELL WALL OF BACTERIA
Beta lactams:
Penicillins, cephalosporins, carbapenems, monobactam
Glycopeptides:
Vancomycin, teicoplanin
ANTIBIOTICS ACTING ON CELL WALL OF BACTERIA
Beta lactams:
Penicillins, cephalosporins, carbapenems, monobactam
Glycopeptides:
Vancomycin, teicoplanin
Слайд 5THE IDEAL ANTIBIOTIC?:PENICILLIN
Narrow spectrum
Bactericidal
Very selective mode of action
Low serum protein binding
Widely distributed
THE IDEAL ANTIBIOTIC?:PENICILLIN
Narrow spectrum
Bactericidal
Very selective mode of action
Low serum protein binding
Widely distributed
Слайд 6THE DEVELOPMENT OF THE BETA LACTAMS
Benzylenicillin and early cephalosporins mainly active against
THE DEVELOPMENT OF THE BETA LACTAMS
Benzylenicillin and early cephalosporins mainly active against
Слайд 7BENZYLPENICILLIN: MAIN INDICATIONS
Strep pyogenes sepsis (from sore throat to fasciitis)
Pneumococcal pneumonia, meningitis
Meningococcal
BENZYLPENICILLIN: MAIN INDICATIONS
Strep pyogenes sepsis (from sore throat to fasciitis)
Pneumococcal pneumonia, meningitis
Meningococcal
Слайд 8Broader spectrum penicillins
Ampicillin, amoxycillin cover most organisms hit by penicillin but also
Broader spectrum penicillins
Ampicillin, amoxycillin cover most organisms hit by penicillin but also
Слайд 9Organisms producing TEM1beta lactamase
Haemophilus influenzae
Neisseria gonorrhoeae
Bacteroides fragilis
Staph aureus
Esch coli
Organisms producing TEM1beta lactamase
Haemophilus influenzae
Neisseria gonorrhoeae
Bacteroides fragilis
Staph aureus
Esch coli
Слайд 10Carbapenems
Imipenem, meropenem: have a very broad spectrum activity against gram-negative bacteria, anaerobes,
Carbapenems
Imipenem, meropenem: have a very broad spectrum activity against gram-negative bacteria, anaerobes,
Слайд 11PENICILLIN IS GENERALLY VERY SAFE BUT….
Allergic reactions not uncommon-rashes
Most severe reaction being
PENICILLIN IS GENERALLY VERY SAFE BUT….
Allergic reactions not uncommon-rashes
Most severe reaction being
Слайд 12What antibiotics can be used in penicillin allergy?
Macrolides: erythromycin, clarithromycin
(mainly gram positive
What antibiotics can be used in penicillin allergy?
Macrolides: erythromycin, clarithromycin
(mainly gram positive
Слайд 13REMEMBER WHAT THE OTHER BETA LACTAMS ARE:
All penicillins: ampicillin, augmentin, piperacillin, cloxacillin
Cephalosporins:
REMEMBER WHAT THE OTHER BETA LACTAMS ARE:
All penicillins: ampicillin, augmentin, piperacillin, cloxacillin
Cephalosporins:
Слайд 14CLOXACILLIN
Narrow spectrum: Staph aureus (MSSA)
Stable to TEM1 beta lactamase
Similar antibiotics are methicillin,
CLOXACILLIN
Narrow spectrum: Staph aureus (MSSA)
Stable to TEM1 beta lactamase
Similar antibiotics are methicillin,
Слайд 15Cephalosporins: main uses
Cefuroxime: surgical prophylaxis
Cefotaxime/ceftriaxone: meningitis nosocomial infections excluding Pseudomonal,
Ceftazidime: nosocomial
Cephalosporins: main uses
Cefuroxime: surgical prophylaxis
Cefotaxime/ceftriaxone: meningitis nosocomial infections excluding Pseudomonal,
Ceftazidime: nosocomial
Слайд 16Problems with antibiotic resistance: how does it happen?
Some bacteria are naturally resistant
Problems with antibiotic resistance: how does it happen?
Some bacteria are naturally resistant
Слайд 17Current major antibiotic resistance problems: community infections
Respiratory tract: penicillin resistance in pneumococcus
Current major antibiotic resistance problems: community infections
Respiratory tract: penicillin resistance in pneumococcus
Слайд 18Current major resistance problems: hospital infections
MRSA: current strains are often multiply-antibiotic resistant
VISA/GISA:
Current major resistance problems: hospital infections
MRSA: current strains are often multiply-antibiotic resistant
VISA/GISA:
Слайд 19Other major antibiotic groups: aminoglycosides
Gentamicin, amikacin (tobramycin, streptomycin)
Mainly active against gram negative
Other major antibiotic groups: aminoglycosides
Gentamicin, amikacin (tobramycin, streptomycin)
Mainly active against gram negative
Слайд 20How we give aminoglycosides
For serious nosocomial infections: “extended interval” or once daily
How we give aminoglycosides
For serious nosocomial infections: “extended interval” or once daily
Слайд 21Some indications and limitations of particular antibiotics
Some indications and limitations of particular antibiotics
Слайд 22Community acquired pneumonia
Pneumococcus (and H influenzae) are most likely: therefore ampicillin, amoxycillin
Community acquired pneumonia
Pneumococcus (and H influenzae) are most likely: therefore ampicillin, amoxycillin
Слайд 23Community acquired urinary infections
Ampicillin, amoxycillin, augmentin
Oral cephalosporin: cephradine
Trimethroprim
Nalidixic acid
Nitrofurantoin
Ciprofloxacin
Mecillinam
Community acquired urinary infections
Ampicillin, amoxycillin, augmentin
Oral cephalosporin: cephradine
Trimethroprim
Nalidixic acid
Nitrofurantoin
Ciprofloxacin
Mecillinam
Слайд 24Skin and soft tissue infections
Cellulitis ? Streptococcal: penicillin or augmentin
Infected eczema ?
Skin and soft tissue infections
Cellulitis ? Streptococcal: penicillin or augmentin
Infected eczema ?
Слайд 25Where there is deep-seated infection: bone, abscess
Need an antibiotic with good tissue
Where there is deep-seated infection: bone, abscess
Need an antibiotic with good tissue
Слайд 26Why do we use combination therapy?
When treating serious infection empirically we want
Why do we use combination therapy?
When treating serious infection empirically we want
Слайд 27Factors to consider when prescribing an antibiotic
Any history of allergy, toxicity?
Is it
Factors to consider when prescribing an antibiotic
Any history of allergy, toxicity?
Is it
Слайд 28Some other antibiotics occasionally used
Co-trimoxazole (Stenotrophomonas)
Chloramphenicol (typhoid fever, meningitis)
Colistin (resistant Pseudomonas) topical
Neomycin:
Some other antibiotics occasionally used
Co-trimoxazole (Stenotrophomonas)
Chloramphenicol (typhoid fever, meningitis)
Colistin (resistant Pseudomonas) topical
Neomycin:
 6. Участие граждан в политической жизни
6. Участие граждан в политической жизни Смешанные числа
Смешанные числа Разработка кольцевых маршрутов движения автотранспорта
Разработка кольцевых маршрутов движения автотранспорта Сетчатый орнамент. Maстер-класс преподавателя ИЗО
Сетчатый орнамент. Maстер-класс преподавателя ИЗО Тема урока: «Культура речи в профессиональной деятельности человека»
Тема урока: «Культура речи в профессиональной деятельности человека»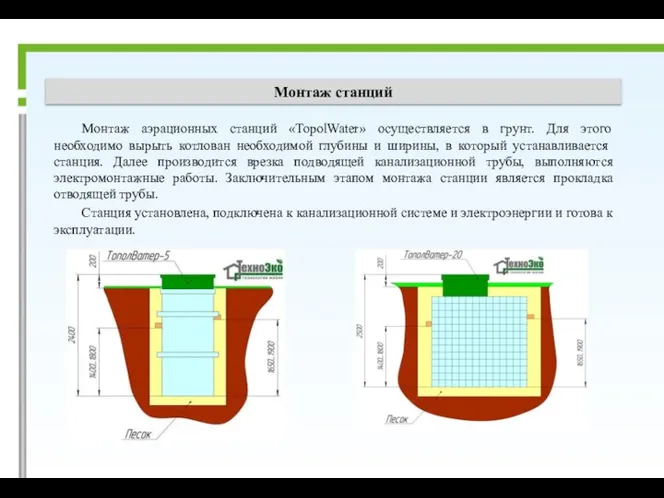 Монтаж станций
Монтаж станций Научно-производственная фирма Шар. Новые полимерные материалы
Научно-производственная фирма Шар. Новые полимерные материалы Презентация на тему Социалистическая индустриализация. Итоги первых пятилеток
Презентация на тему Социалистическая индустриализация. Итоги первых пятилеток  Особенностипродвиженияженских товаровв Интернете
Особенностипродвиженияженских товаровв Интернете А. И. Солженицын (1918-2008)
А. И. Солженицын (1918-2008) Народы, языки и религии
Народы, языки и религии Новогоднее мероприятие в стиле «Русские гуляния»
Новогоднее мероприятие в стиле «Русские гуляния» Совещание МО
Совещание МО Проект остановки транспорта. Окупаемость остановок при помощи рекламы
Проект остановки транспорта. Окупаемость остановок при помощи рекламы Россия и НАТО: реальность и перспективы взаимодействия
Россия и НАТО: реальность и перспективы взаимодействия Школа молодого педагога Специфика ведения школьной документации начального общего образования
Школа молодого педагога Специфика ведения школьной документации начального общего образования Задание по хозяйству
Задание по хозяйству Группа компаний DIGSEE
Группа компаний DIGSEE Боевые искусства Древней Руси
Боевые искусства Древней Руси Презентация на тему Влага в атмосфере
Презентация на тему Влага в атмосфере  macroeconomics
macroeconomics  Бизнес в Польше под ключ. Помощь для получения лизинга
Бизнес в Польше под ключ. Помощь для получения лизинга Масленица (1-8 класс)
Масленица (1-8 класс) Финикийские мореплаватели
Финикийские мореплаватели Бизнес-задача
Бизнес-задача Архитектура православного храма. Символика
Архитектура православного храма. Символика Системы мотивации и стимулирования персонала
Системы мотивации и стимулирования персонала Окислительно-восстановительные реакции
Окислительно-восстановительные реакции