- Chronic Obstructive Pulmonary Disease

Содержание
- 2. THE Guideline Global Initiative for Chronic Obstructive Lung Disease (GOLD), World Health Organization (WHO), National Heart,
- 3. Definition of COPD COPD is a preventable and treatable chronic lung disease characterized by airflow limitation
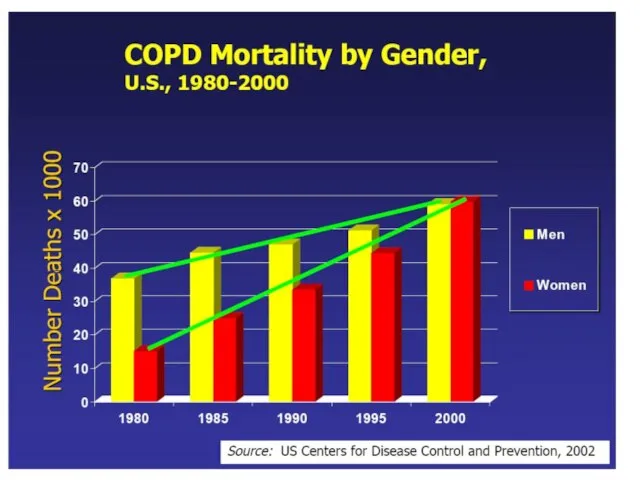
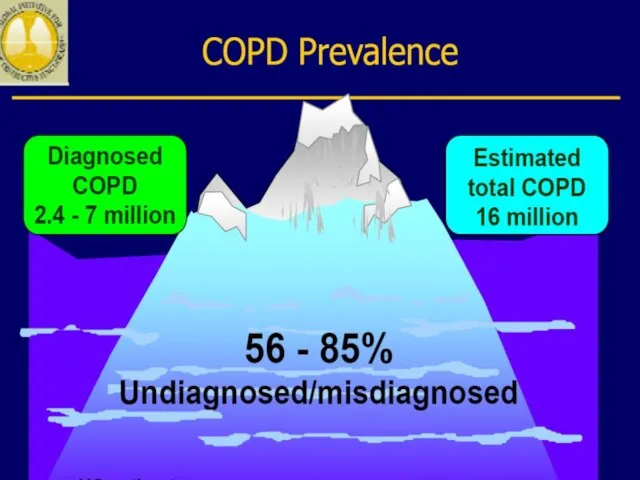
- 4. Epidemiology of COPD 4th leading cause of death in world 4th leading cause of death in
- 5. COPD includes: chronic bronchitis chronic bronchiolitis (small air way disease) Emphysema
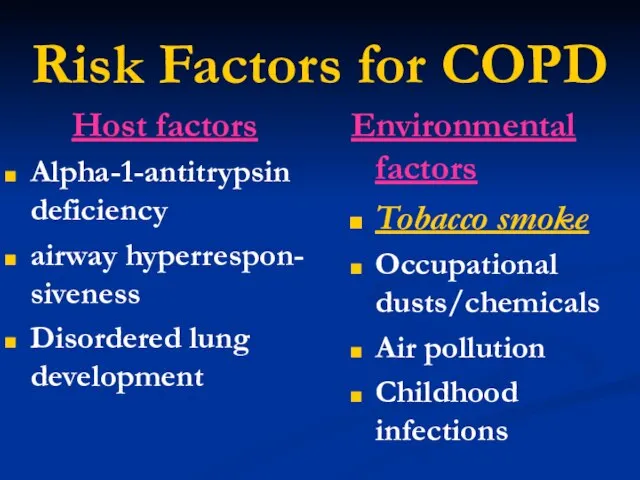
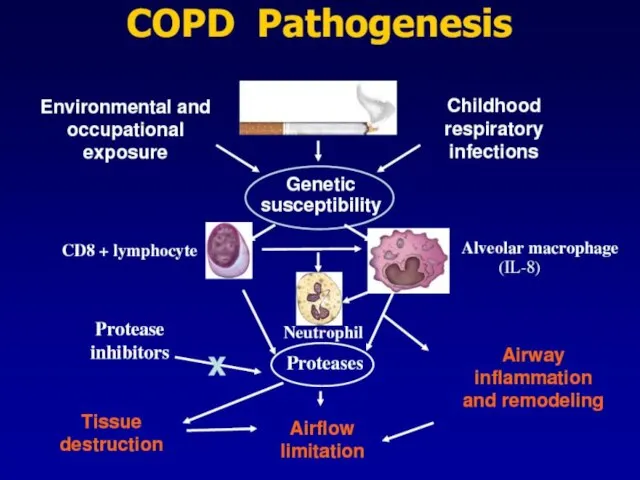
- 8. Risk Factors for COPD Host factors Alpha-1-antitrypsin deficiency airway hyperrespon- siveness Disordered lung development Environmental factors
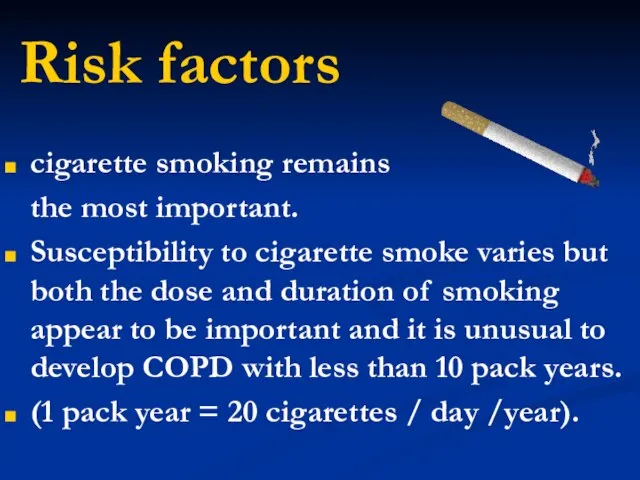
- 10. Risk factors cigarette smoking remains the most important. Susceptibility to cigarette smoke varies but both the
- 11. Alpha-1-antitrypsin deficiency α1-Antitrypsin is a proteinase inhibitor which is produced in the liver, secreted into the
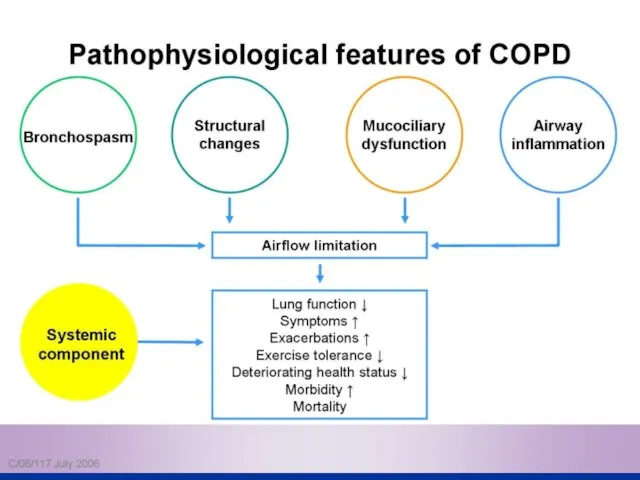
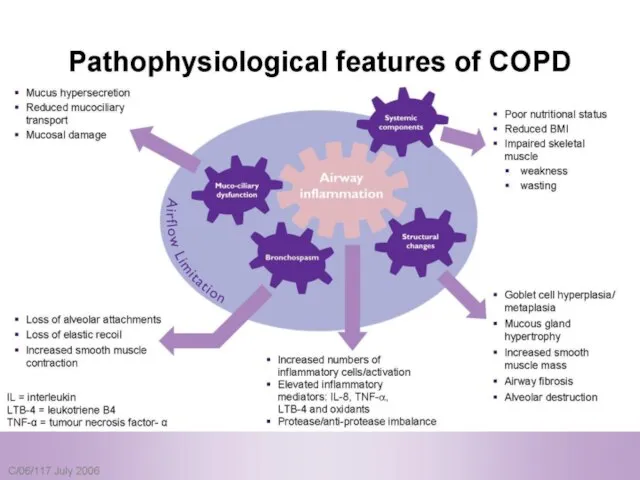
- 12. Pathophysiology COPD has both Pulmonary components Systemic components
- 13. Pulmonary components: Mucus secretion An enlargement of mucous secreting glands and an increasing number of goblet
- 14. Pulmonary components: Premature airway closure leads to gas trapping and hyperinflation → ↓ pulmonary and chest
- 15. Pulmonary components: Flattening of the diaphragmatic muscles and increase horizontal alignment of the intercostals muscles →
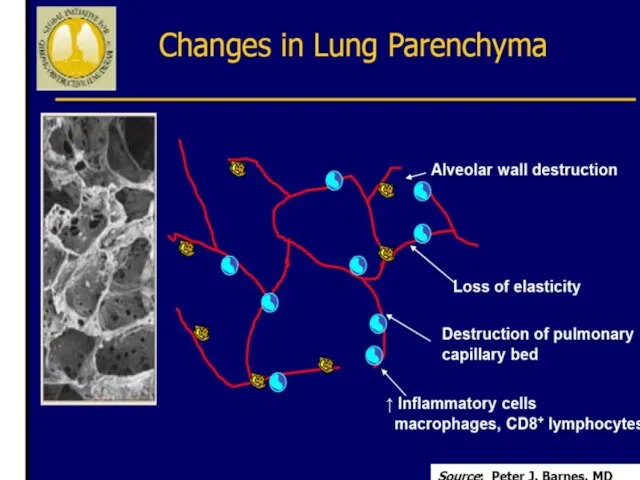
- 16. Pulmonary components: In the alveolar capillary units the unopposed action of proteases and oxidants → destruction
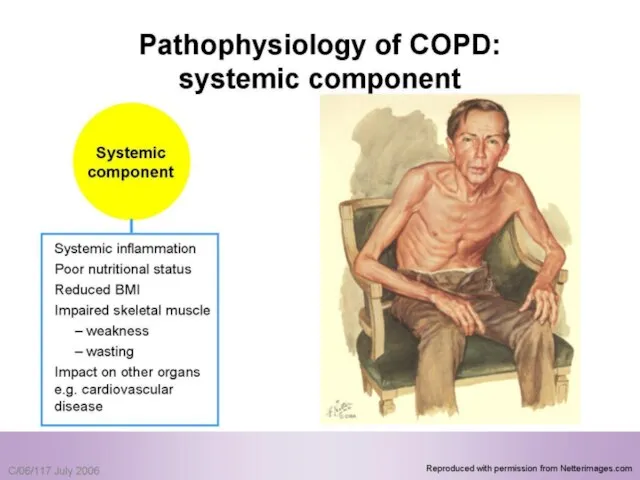
- 18. Systemic components: 1. Skeletal muscle weakness. 2. Increase circulating inflammatory markers. 3. Impaired salt and water
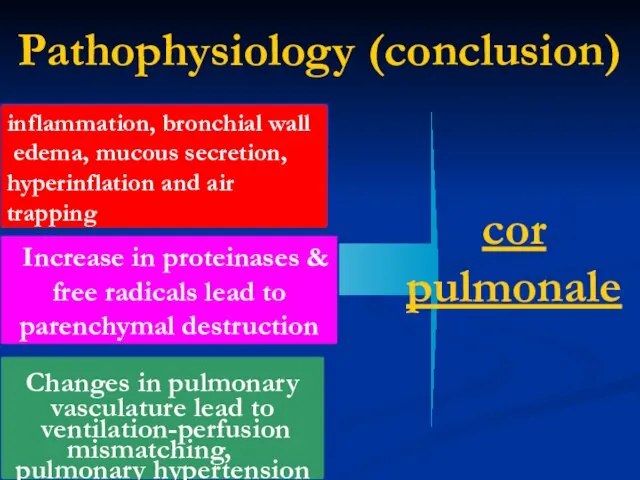
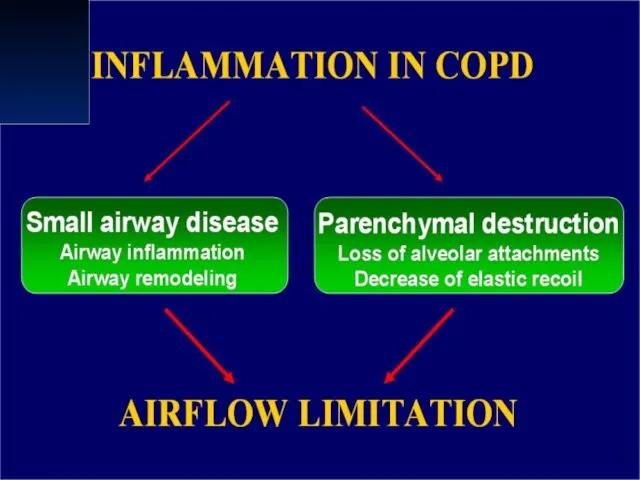
- 22. Pathophysiology (conclusion) inflammation, bronchial wall edema, mucous secretion, hyperinflation and air trapping Increase in proteinases &
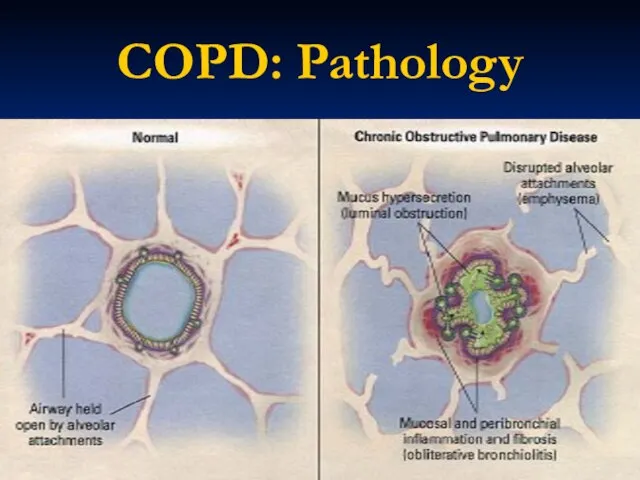
- 25. COPD: Pathology
- 29. Assess for COPD: Cough intermittent or daily present throughout day, seldom only nocturnal Sputum Any pattern
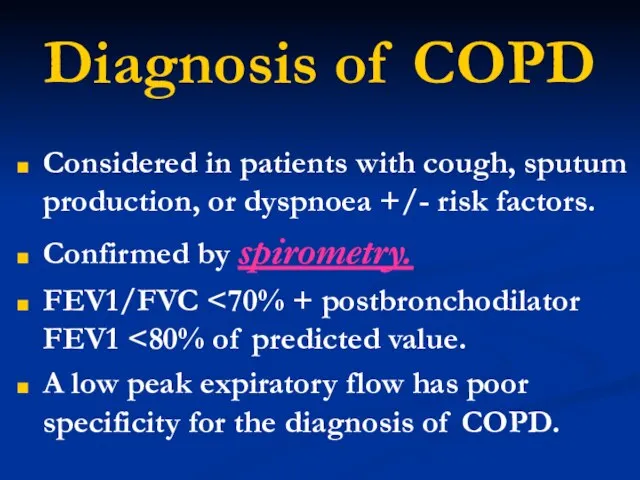
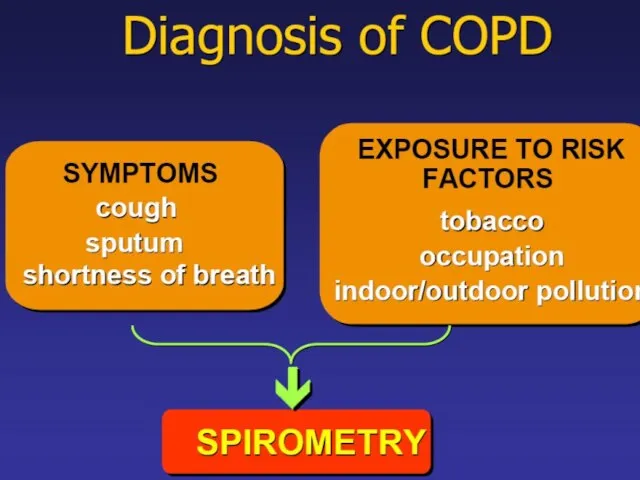
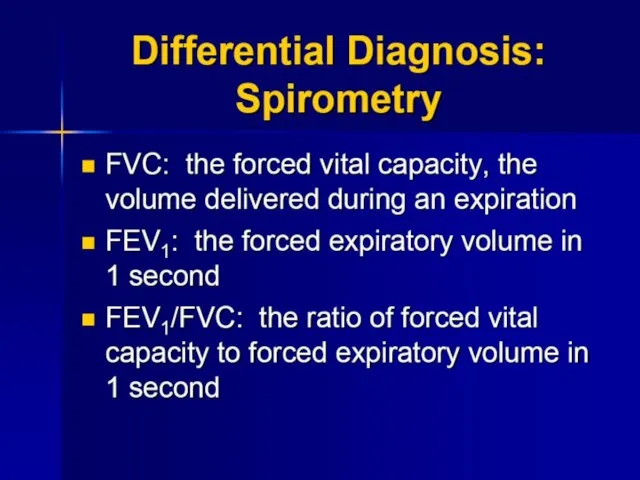
- 31. Diagnosis of COPD Considered in patients with cough, sputum production, or dyspnoea +/- risk factors. Confirmed
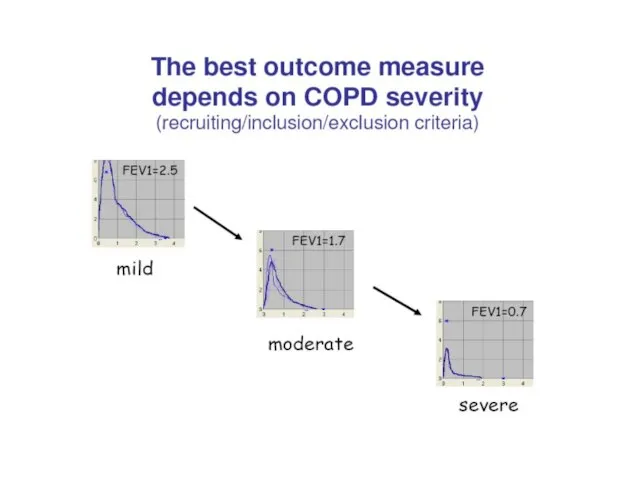
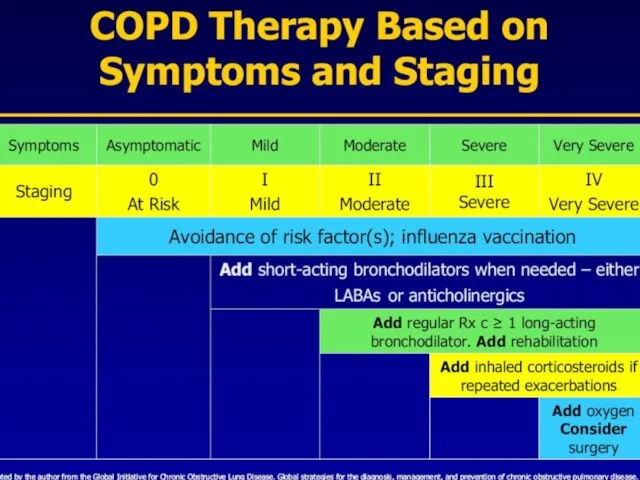
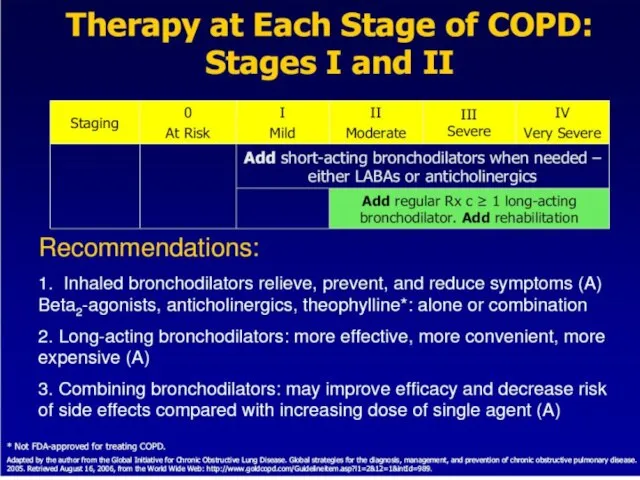
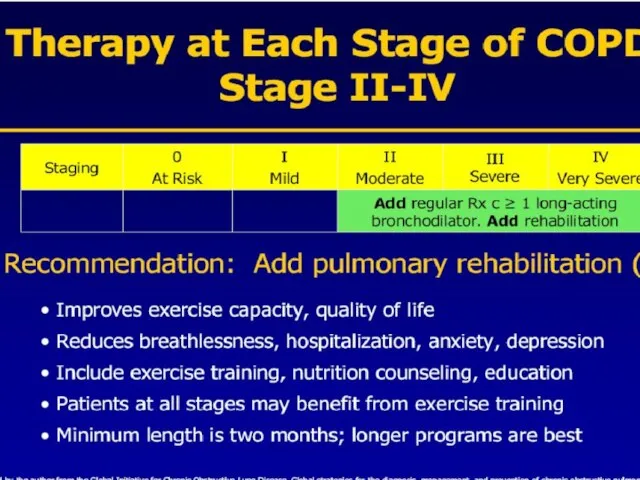
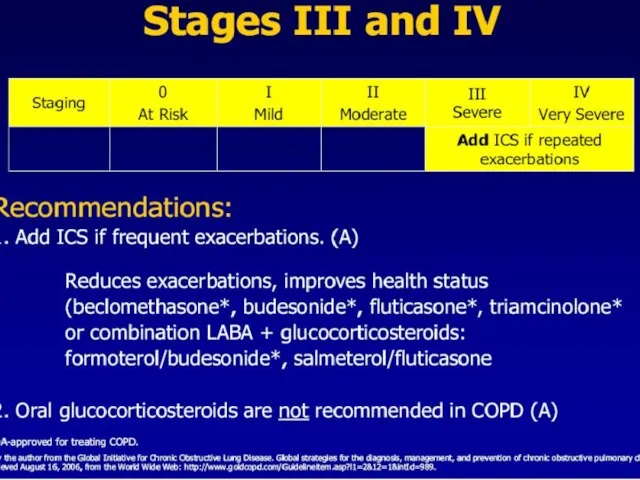
- 32. Classification of COPD Stage 0 At Risk Stage I Mild Stage II Moderate Stage III Severe
- 34. Stage 0 At Risk Normal spirometry +/- Chronic symptoms (cough, sputum, production)
- 35. Stage I Mild COPD FEV1/FVC FEV1 >80% predicted With or without chronic symptoms (cough, sputum production)
- 36. Stage II Moderate COPD FEV1/FVC 50% With or without chronic symptoms (cough, sputum production)
- 37. Stage III Severe COPD FEV1/FVC 30% With or without chronic symptoms (cough, sputum production)
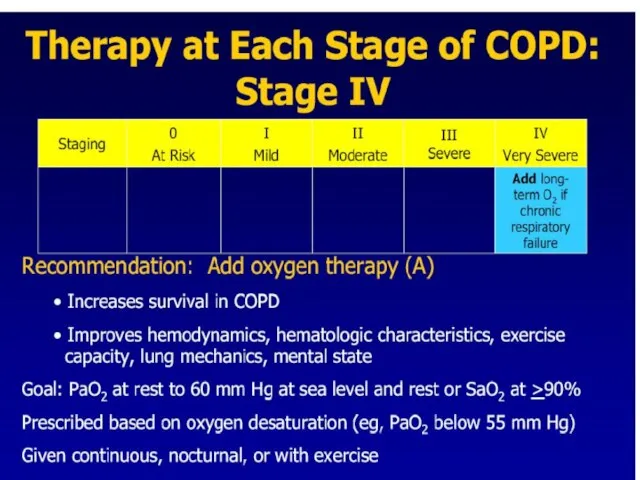
- 38. Stage IV Very Severe COPD FEV1/FVC FEV1 chronic respiratory failure
- 41. Diagnosis of COPD
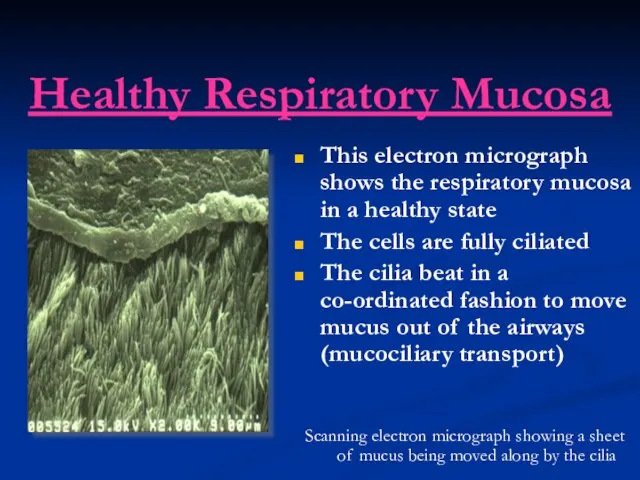
- 42. Healthy Respiratory Mucosa This electron micrograph shows the respiratory mucosa in a healthy state The cells
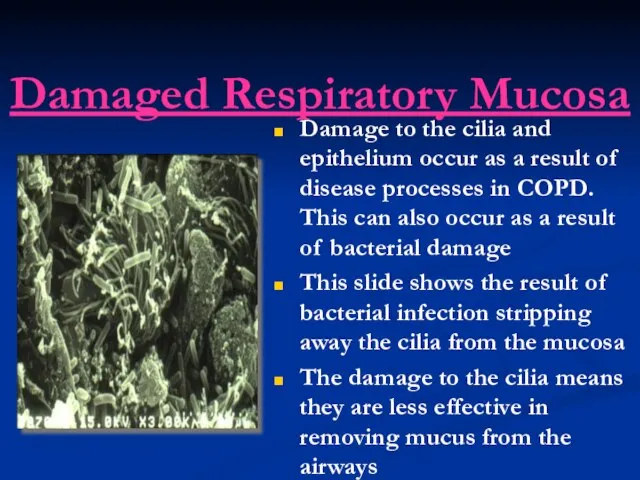
- 43. Damaged Respiratory Mucosa Damage to the cilia and epithelium occur as a result of disease processes
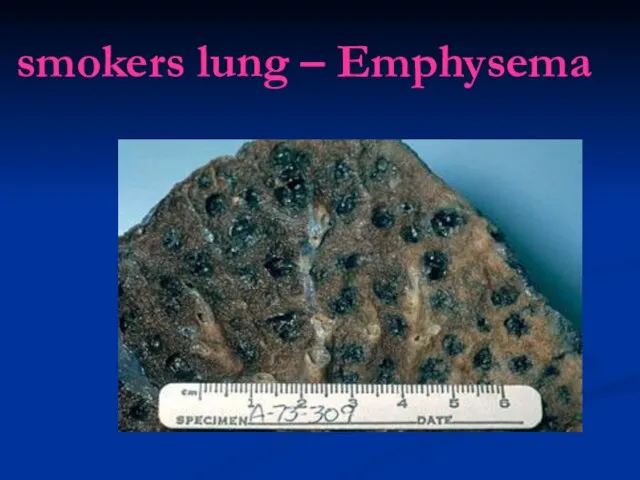
- 45. smokers lung – Emphysema
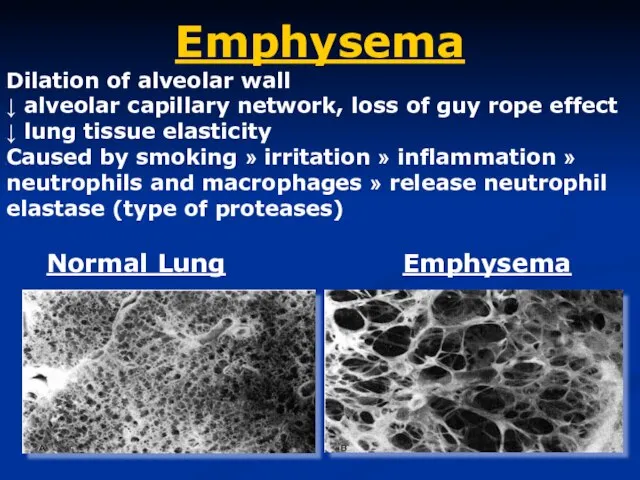
- 46. Emphysema Dilation of alveolar wall ↓ alveolar capillary network, loss of guy rope effect ↓ lung
- 47. Emphysema is defined pathologically as dilatation and destruction of the lung tissue distal to the terminal
- 48. classification Centri-acinar emphysema. Pan-acinar emphysema. Irregular emphysema.
- 49. Centri-acinar emphysema Distension and damage of lung tissue is concentrated around the respiratory bronchioles, whilst the
- 50. Pan-acinar emphysema Distension and destruction appear to involve the whole of the acinus, and in the
- 51. Irregular emphysema scarring and damage affect the lung parenchyma patchily without particular regard for acinar structure
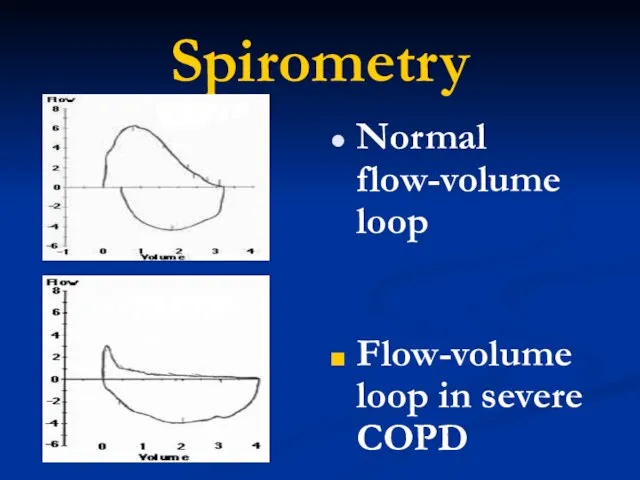
- 52. Spirometry Normal flow-volume loop Flow-volume loop in severe COPD
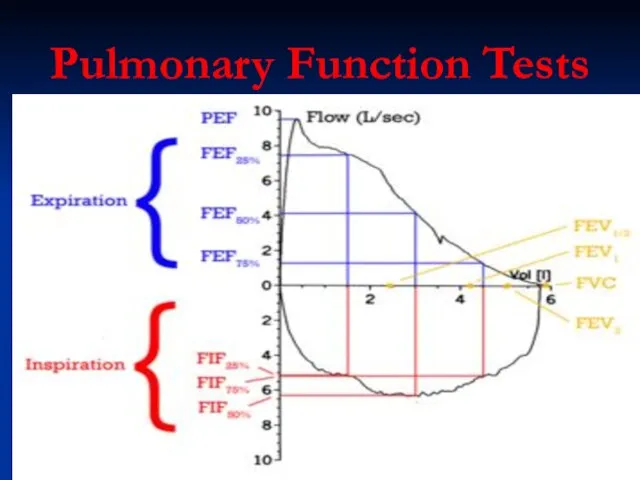
- 54. Pulmonary Function Tests
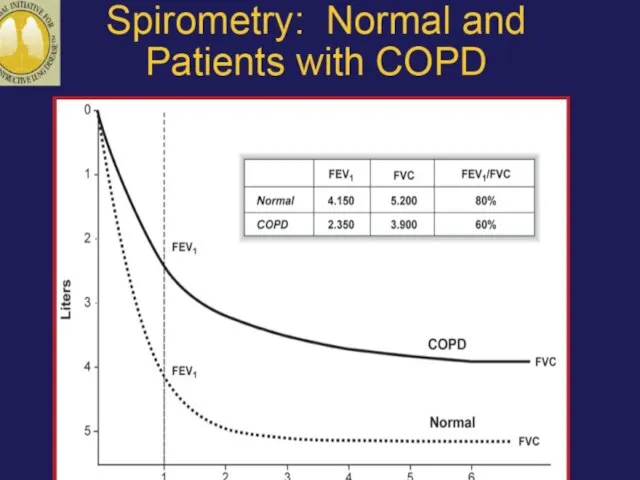
- 57. Assess: Measure Airflow Limitation Patients with COPD typically show a decrease in both FEV1 and FVC
- 60. GOALS of COPD MANAGEMENT Relieve symptoms Prevent disease progression Improve exercise tolerance Improve health status Prevent
- 62. General Points Only smoking cessation and O2 therapy have been shown to prolong survival Other therapies
- 63. Exacerbation management Chronic stable management Adjuvant therapy
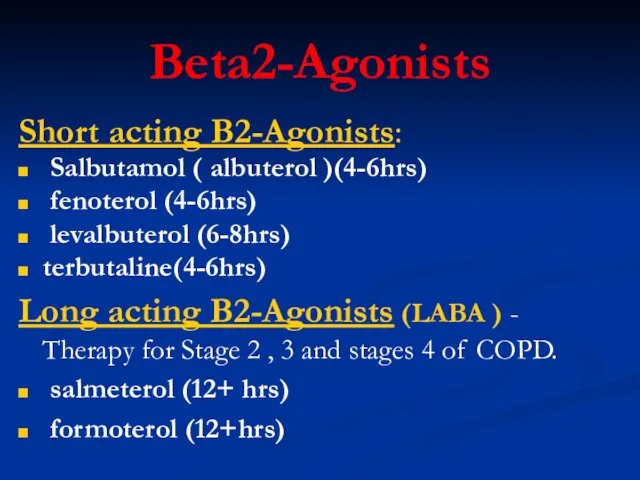
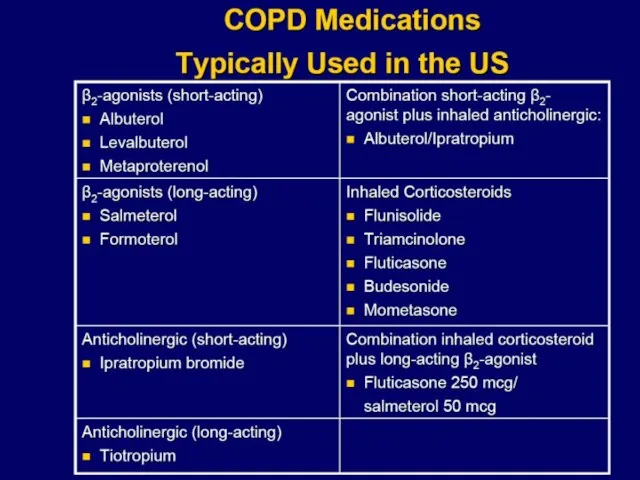
- 66. Beta2-Agonists Short acting B2-Agonists: Salbutamol ( albuterol )(4-6hrs) fenoterol (4-6hrs) levalbuterol (6-8hrs) terbutaline(4-6hrs) Long acting B2-Agonists
- 67. Beta2-Agonists Excellent bronchodilator and quick effect. Therapy for all stages, mostly rescue and as needed dosing
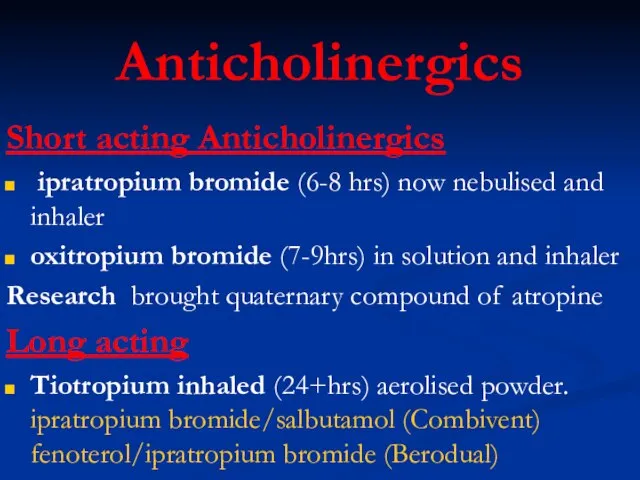
- 68. Anticholinergics Short acting Anticholinergics ipratropium bromide (6-8 hrs) now nebulised and inhaler oxitropium bromide (7-9hrs) in
- 69. Anticholinergics (Tiotropium) Block muscarinic receptors and prevent smooth muscle contraction while ↓ release of secretion from
- 70. Drug therapy for COPD begins with long acting anticholinergics and beta-2 agonist bronchodilators. These provide symptom
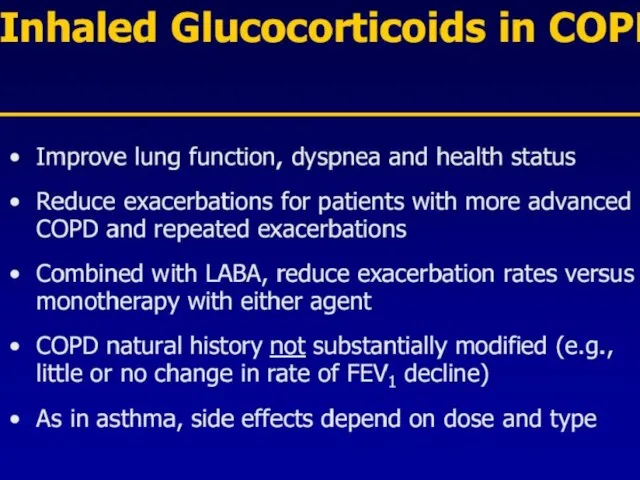
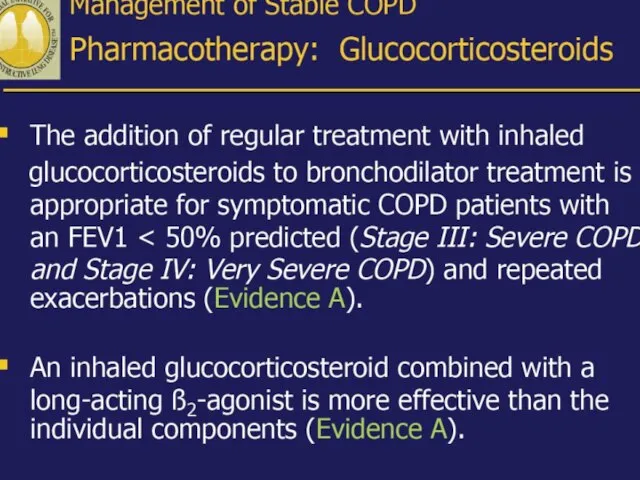
- 76. Inhaled Steroids Front line therapy for COPD stages 3 and 4 Budenoside Nebulizer Inhaled fluticasone Inhaled
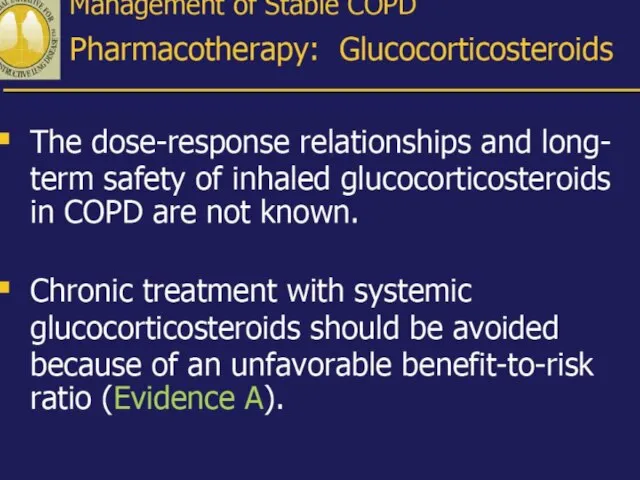
- 79. Treatment of Stable COPD Other Medications Chronic oral Prednisone Use in chronic COPD is controversial. No
- 80. Methylxanthines Multiple modes of action : bronchodilatation, ↑ dia-phragmatic contractility, stimulation of respiratory drive, inotropism, ↑
- 81. Mucokinetic Medications Nebulized water and saline and oral expectorants guaifenesin and saturated iodide are of no
- 82. Treatment of Stable COPD: Home Oxygen Therapy > 15 hours/day reduces mortality Criteria for O2 therapy
- 84. Exacerbations in COPD Etiology Primary – viral and bacterial infections – air pollution – discontinuation of
- 85. COPD Exacerbations Primary symptom— increased dyspnea —may be accompanied by wheezing and tightening of chest, increased
- 92. Antibiotics – Have proven beneficial in treating acute infective exacerbations of COPD – Should be used
- 93. Antibiotics in Acute Exacerbations of COPD Traditional regimen: three to 14 days of tetracycline, amoxicillin or
- 94. Inpatient Treatment of Acute Exacerbations Oxygen to keep O2 sat >90% Nebulizer treatments with bronchodilators Steroids
- 96. Oxygen therapy Generally only considered in severe (stage III) COPD patients with PaO2 • Goal: to
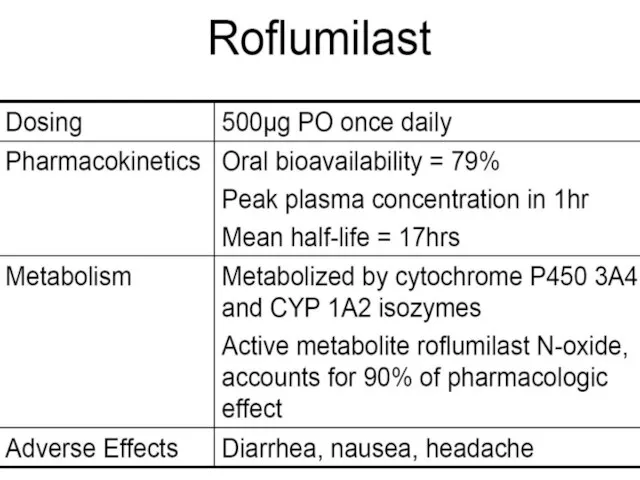
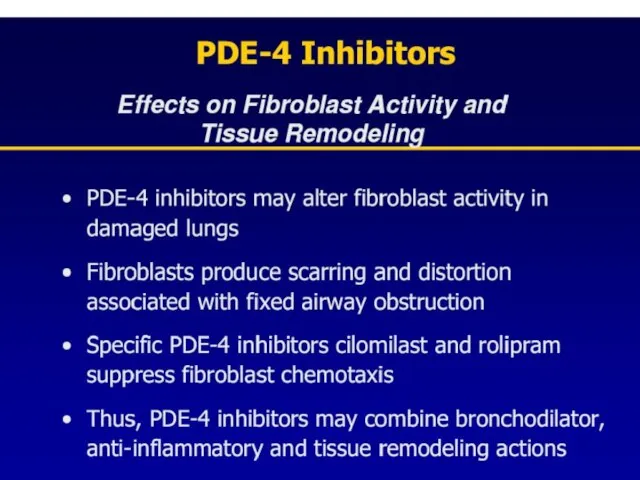
- 98. Phosphodiesterase-4 Inhibition (Roflumilast) Inhibition raises intracellular levels of cAMP resulting in downregulation of signaling pathways in
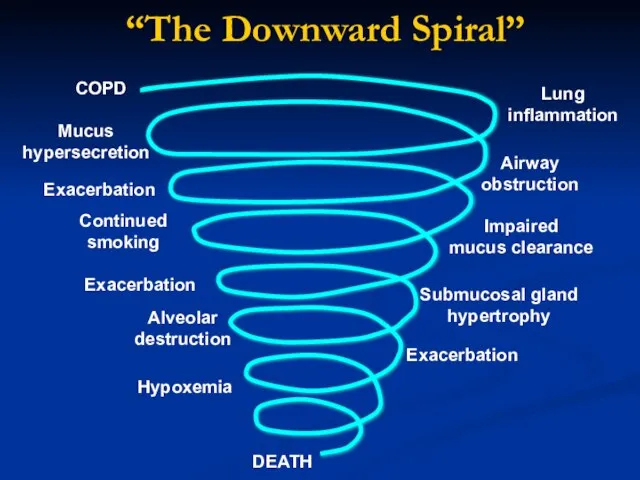
- 103. COPD Airway obstruction Exacerbation Mucus hypersecretion Continued smoking Lung inflammation Alveolar destruction Impaired mucus clearance Submucosal
- 104. SMOKERS “Hope and expect for the best. Prepare for the worst.” Back AL, Arnold RM, Quill
- 105. NEXT STAGE…
- 106. PREVENT COPD
- 107. PREVENT COPD
- 110. Скачать презентацию
Слайд 2THE Guideline
Global Initiative for Chronic Obstructive Lung Disease (GOLD), World Health Organization
THE Guideline
Global Initiative for Chronic Obstructive Lung Disease (GOLD), World Health Organization
Слайд 3Definition of COPD
COPD is a preventable and treatable chronic lung disease characterized
Definition of COPD
COPD is a preventable and treatable chronic lung disease characterized
Слайд 4Epidemiology of COPD
4th leading cause of death in world
4th leading cause of
Epidemiology of COPD
4th leading cause of death in world
4th leading cause of
Слайд 5
COPD includes:
chronic bronchitis
chronic bronchiolitis (small air way disease)
Emphysema
COPD includes:
chronic bronchitis
chronic bronchiolitis (small air way disease)
Emphysema
Слайд 8Risk Factors for COPD
Host factors
Alpha-1-antitrypsin deficiency
airway hyperrespon- siveness
Disordered lung development
Environmental factors
Tobacco smoke
Occupational
Risk Factors for COPD
Host factors
Alpha-1-antitrypsin deficiency
airway hyperrespon- siveness
Disordered lung development
Environmental factors
Tobacco smoke
Occupational

Слайд 10Risk factors
cigarette smoking remains
the most important.
Susceptibility to cigarette smoke varies
Risk factors
cigarette smoking remains
the most important.
Susceptibility to cigarette smoke varies
Слайд 11
Alpha-1-antitrypsin deficiency
α1-Antitrypsin is a proteinase inhibitor which is produced in the liver,
Alpha-1-antitrypsin deficiency
α1-Antitrypsin is a proteinase inhibitor which is produced in the liver,
Слайд 12Pathophysiology
COPD has both
Pulmonary components
Systemic components
Pathophysiology
COPD has both
Pulmonary components
Systemic components
Слайд 13Pulmonary components:
Mucus secretion An enlargement of mucous secreting glands and an increasing
Pulmonary components:
Mucus secretion An enlargement of mucous secreting glands and an increasing
Слайд 14Pulmonary components:
Premature airway closure leads to gas trapping and hyperinflation →
↓
Pulmonary components:
Premature airway closure leads to gas trapping and hyperinflation →
↓
Слайд 15Pulmonary components:
Flattening of the diaphragmatic muscles and increase horizontal alignment of
Pulmonary components:
Flattening of the diaphragmatic muscles and increase horizontal alignment of
Слайд 16Pulmonary components:
In the alveolar capillary units the unopposed action of proteases and
Pulmonary components:
In the alveolar capillary units the unopposed action of proteases and
Слайд 18Systemic components:
1. Skeletal muscle weakness.
2. Increase circulating inflammatory markers.
3. Impaired salt and
Systemic components:
1. Skeletal muscle weakness.
2. Increase circulating inflammatory markers.
3. Impaired salt and
Слайд 22Pathophysiology (conclusion)
inflammation, bronchial wall
edema, mucous secretion,
hyperinflation and air trapping
Increase
Pathophysiology (conclusion)
inflammation, bronchial wall
edema, mucous secretion,
hyperinflation and air trapping
Increase
Слайд 25COPD: Pathology
COPD: Pathology

Слайд 29Assess for COPD:
Cough
intermittent or daily
present throughout day, seldom only nocturnal
Sputum
Any pattern
Assess for COPD:
Cough
intermittent or daily
present throughout day, seldom only nocturnal
Sputum
Any pattern
Слайд 31Diagnosis of COPD
Considered in patients with cough, sputum production, or dyspnoea +/-
Diagnosis of COPD
Considered in patients with cough, sputum production, or dyspnoea +/-
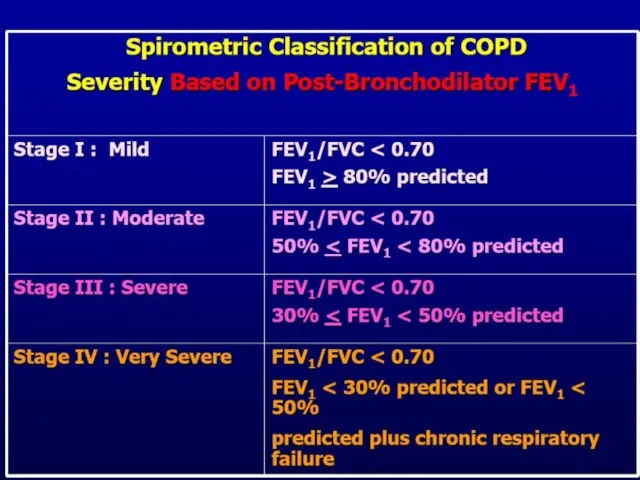
Слайд 32Classification of COPD
Stage 0 At Risk
Stage I Mild
Stage II Moderate
Stage
Classification of COPD
Stage 0 At Risk
Stage I Mild
Stage II Moderate
Stage
Слайд 34Stage 0 At Risk
Normal spirometry
+/- Chronic symptoms (cough, sputum, production)
Stage 0 At Risk
Normal spirometry
+/- Chronic symptoms (cough, sputum, production)
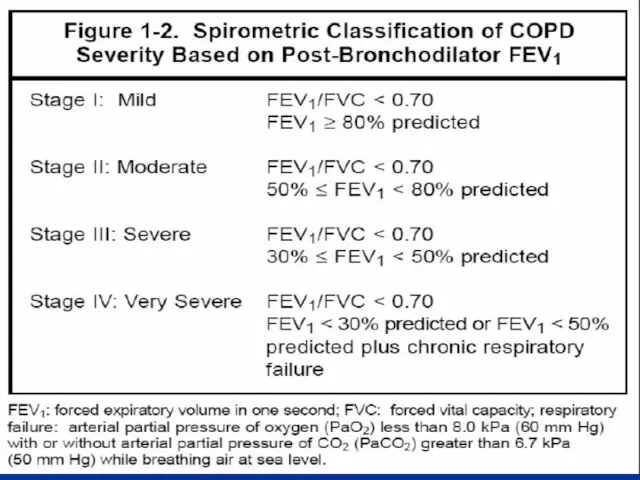
Слайд 35Stage I Mild COPD
FEV1/FVC <70%
FEV1 >80% predicted
With or without chronic
Stage I Mild COPD
FEV1/FVC <70%
FEV1 >80% predicted
With or without chronic
Слайд 36Stage II Moderate COPD
FEV1/FVC <70%
50% With or without
Stage II Moderate COPD
FEV1/FVC <70%
50%
Слайд 37Stage III Severe COPD
FEV1/FVC <70%
30% With or without
Stage III Severe COPD
FEV1/FVC <70%
30%
Слайд 38Stage IV Very Severe COPD
FEV1/FVC <70%
FEV1 <30% predicted or FEV1 <50%
Stage IV Very Severe COPD
FEV1/FVC <70%
FEV1 <30% predicted or FEV1 <50%
Слайд 41Diagnosis of COPD
Diagnosis of COPD
Слайд 42Healthy Respiratory Mucosa
This electron micrograph shows the respiratory mucosa in a healthy
Healthy Respiratory Mucosa
This electron micrograph shows the respiratory mucosa in a healthy
Слайд 43Damaged Respiratory Mucosa
Damage to the cilia and epithelium occur as a result
Damaged Respiratory Mucosa
Damage to the cilia and epithelium occur as a result
Слайд 45smokers lung – Emphysema
smokers lung – Emphysema
Слайд 46Emphysema
Dilation of alveolar wall
↓ alveolar capillary network, loss of guy rope effect
↓
Emphysema
Dilation of alveolar wall
↓ alveolar capillary network, loss of guy rope effect
↓
Слайд 47
Emphysema
is defined pathologically as dilatation and destruction of the lung tissue
Emphysema
is defined pathologically as dilatation and destruction of the lung tissue
Слайд 48classification
Centri-acinar emphysema.
Pan-acinar emphysema.
Irregular emphysema.
classification
Centri-acinar emphysema.
Pan-acinar emphysema.
Irregular emphysema.
Слайд 49Centri-acinar emphysema
Distension and damage of lung tissue is concentrated around the
Centri-acinar emphysema
Distension and damage of lung tissue is concentrated around the
Слайд 50Pan-acinar emphysema
Distension and destruction appear to involve the whole of the acinus,
Pan-acinar emphysema
Distension and destruction appear to involve the whole of the acinus,
Слайд 51Irregular emphysema
scarring and damage affect the lung parenchyma patchily without particular
Irregular emphysema
scarring and damage affect the lung parenchyma patchily without particular
Слайд 52Spirometry
Normal flow-volume loop
Flow-volume loop in severe COPD
Spirometry
Normal flow-volume loop
Flow-volume loop in severe COPD
Слайд 54Pulmonary Function Tests
Pulmonary Function Tests
Слайд 57Assess:
Measure Airflow Limitation
Patients with COPD typically show a decrease in
Assess:
Measure Airflow Limitation
Patients with COPD typically show a decrease in
Слайд 60GOALS of COPD MANAGEMENT
Relieve symptoms
Prevent disease progression
Improve exercise tolerance
GOALS of COPD MANAGEMENT
Relieve symptoms
Prevent disease progression
Improve exercise tolerance
Слайд 62General Points
Only smoking cessation and O2 therapy have been shown to prolong
General Points
Only smoking cessation and O2 therapy have been shown to prolong
Слайд 63Exacerbation management
Chronic stable management
Adjuvant therapy
Exacerbation management
Chronic stable management
Adjuvant therapy
Слайд 66Beta2-Agonists
Short acting B2-Agonists:
Salbutamol ( albuterol )(4-6hrs)
fenoterol (4-6hrs)
levalbuterol
Beta2-Agonists
Short acting B2-Agonists:
Salbutamol ( albuterol )(4-6hrs)
fenoterol (4-6hrs)
levalbuterol
Слайд 67Beta2-Agonists
Excellent bronchodilator and quick effect. Therapy for all stages, mostly rescue and
Beta2-Agonists
Excellent bronchodilator and quick effect. Therapy for all stages, mostly rescue and
Слайд 68Anticholinergics
Short acting Anticholinergics
ipratropium bromide (6-8 hrs) now nebulised and inhaler
Anticholinergics
Short acting Anticholinergics
ipratropium bromide (6-8 hrs) now nebulised and inhaler
Слайд 69Anticholinergics (Tiotropium)
Block muscarinic receptors and prevent smooth muscle contraction while ↓ release
Anticholinergics (Tiotropium)
Block muscarinic receptors and prevent smooth muscle contraction while ↓ release
Слайд 70Drug therapy for COPD begins with long acting anticholinergics and beta-2 agonist
Drug therapy for COPD begins with long acting anticholinergics and beta-2 agonist
Слайд 76Inhaled Steroids
Front line therapy for COPD stages 3 and 4
Budenoside Nebulizer
Inhaled
Inhaled Steroids
Front line therapy for COPD stages 3 and 4
Budenoside Nebulizer
Inhaled
Слайд 79Treatment of Stable COPD
Other Medications
Chronic oral Prednisone
Use in chronic COPD is controversial.
Treatment of Stable COPD
Other Medications
Chronic oral Prednisone
Use in chronic COPD is controversial.
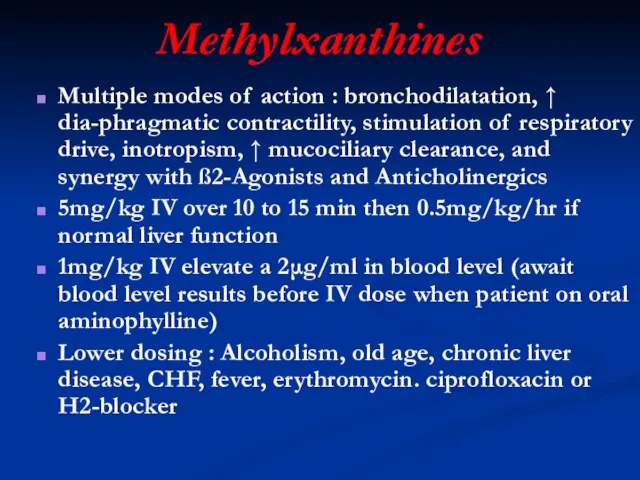
Слайд 80Methylxanthines
Multiple modes of action : bronchodilatation, ↑ dia-phragmatic contractility, stimulation of respiratory
Methylxanthines
Multiple modes of action : bronchodilatation, ↑ dia-phragmatic contractility, stimulation of respiratory
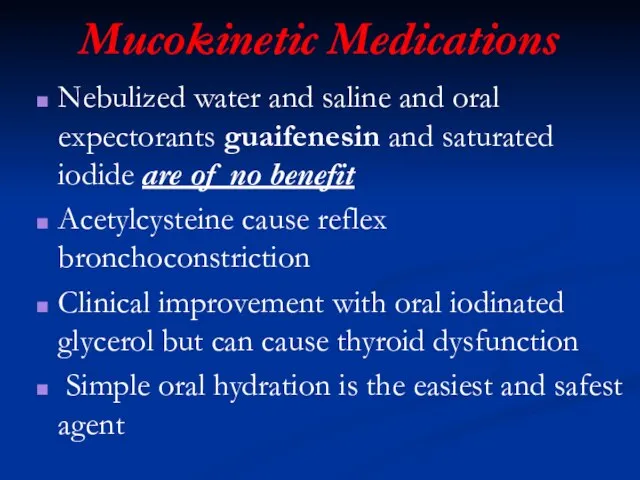
Слайд 81Mucokinetic Medications
Nebulized water and saline and oral expectorants guaifenesin and saturated iodide
Mucokinetic Medications
Nebulized water and saline and oral expectorants guaifenesin and saturated iodide
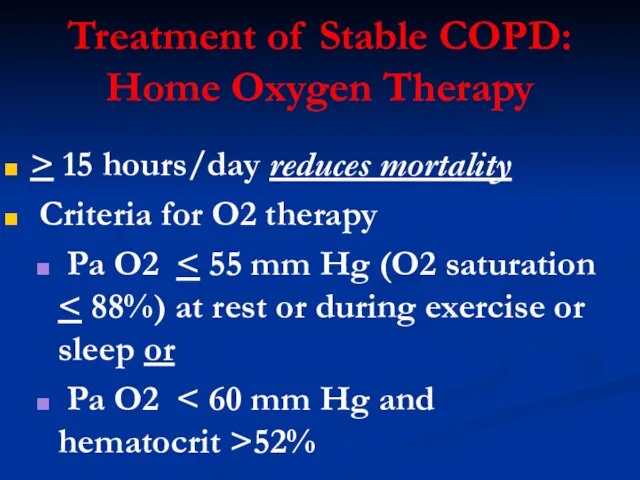
Слайд 82Treatment of Stable COPD:
Home Oxygen Therapy
> 15 hours/day reduces mortality
Treatment of Stable COPD:
Home Oxygen Therapy
> 15 hours/day reduces mortality
Слайд 84Exacerbations in COPD
Etiology
Primary
– viral and bacterial infections
– air pollution
– discontinuation of
Exacerbations in COPD
Etiology
Primary
– viral and bacterial infections
– air pollution
– discontinuation of
Слайд 85COPD Exacerbations
Primary symptom— increased dyspnea —may be accompanied by wheezing and tightening
COPD Exacerbations
Primary symptom— increased dyspnea —may be accompanied by wheezing and tightening


Слайд 92Antibiotics
– Have proven beneficial in treating acute infective exacerbations of COPD
– Should
Antibiotics
– Have proven beneficial in treating acute infective exacerbations of COPD
– Should
Слайд 93
Antibiotics in Acute
Exacerbations of COPD
Traditional regimen: three to 14 days of
Antibiotics in Acute
Exacerbations of COPD
Traditional regimen: three to 14 days of
Слайд 94Inpatient Treatment of Acute Exacerbations
Oxygen to keep O2 sat >90%
Nebulizer treatments
Inpatient Treatment of Acute Exacerbations
Oxygen to keep O2 sat >90%
Nebulizer treatments
Слайд 96Oxygen therapy
Generally only considered in severe (stage III) COPD patients with PaO2
Oxygen therapy
Generally only considered in severe (stage III) COPD patients with PaO2

Слайд 98Phosphodiesterase-4 Inhibition
(Roflumilast)
Inhibition raises intracellular levels of cAMP resulting in downregulation of
Phosphodiesterase-4 Inhibition
(Roflumilast)
Inhibition raises intracellular levels of cAMP resulting in downregulation of

Слайд 103COPD
Airway
obstruction
Exacerbation
Mucus
hypersecretion
Continued
smoking
Lung
inflammation
Alveolar
destruction
Impaired
mucus clearance
Submucosal gland
hypertrophy
Exacerbation
Exacerbation
Hypoxemia
DEATH
“The Downward Spiral”
COPD
Airway
obstruction
Exacerbation
Mucus
hypersecretion
Continued
smoking
Lung
inflammation
Alveolar
destruction
Impaired
mucus clearance
Submucosal gland
hypertrophy
Exacerbation
Exacerbation
Hypoxemia
DEATH
“The Downward Spiral”
Слайд 104SMOKERS
“Hope and expect for the best.
Prepare for the worst.”
Back AL, Arnold RM,
SMOKERS
“Hope and expect for the best.
Prepare for the worst.”
Back AL, Arnold RM,
Слайд 105NEXT STAGE…
NEXT STAGE…

Слайд 106PREVENT COPD
PREVENT COPD
Слайд 107PREVENT COPD
PREVENT COPD

 Презентация на тему Чем опасно селфи
Презентация на тему Чем опасно селфи Организация и технология торговли в специализированных продовольственных магазинах. Продажа спортивных товаров
Организация и технология торговли в специализированных продовольственных магазинах. Продажа спортивных товаров Мировые финансовые рынки
Мировые финансовые рынки ООО Мелон
ООО Мелон Право природопользования
Право природопользования Презентация на тему Сергей Васильевич Рахманинов
Презентация на тему Сергей Васильевич Рахманинов Косплей. Фарфоровая кожа
Косплей. Фарфоровая кожа Презентация на тему Информация ее хранение и способы передачи
Презентация на тему Информация ее хранение и способы передачи Информацияо результатах деятельности за 2010 годотдела управления предприятиями и организациями
Информацияо результатах деятельности за 2010 годотдела управления предприятиями и организациями Кодирование информации. Двоичное кодирование информации
Кодирование информации. Двоичное кодирование информации Методы обнаружения фальсификации рыбной муки
Методы обнаружения фальсификации рыбной муки Презентация на тему Политическая система и политический режим
Презентация на тему Политическая система и политический режим  Кодекс профессиональной этики проводника пассажирского вагона
Кодекс профессиональной этики проводника пассажирского вагона Традесканция
Традесканция Дом как отражение личности
Дом как отражение личности 663980 Красноярский край, г.Бородино, мкрн. Победы, 4. Тел. 8-391-68-3-32-27
663980 Красноярский край, г.Бородино, мкрн. Победы, 4. Тел. 8-391-68-3-32-27 Оптимизация конверсии
Оптимизация конверсии Эпидемиологический надзор за ВИЧ-инфекцией Киев, 1 июня 2010 г.
Эпидемиологический надзор за ВИЧ-инфекцией Киев, 1 июня 2010 г. Это презентационный материал концепции развития Сергиева Посада как столицы Православия был подготовлен в 2007 году. Заказчиками и
Это презентационный материал концепции развития Сергиева Посада как столицы Православия был подготовлен в 2007 году. Заказчиками и  8 шагов на пути успешного решения проблем
8 шагов на пути успешного решения проблем Скифы 11 класс
Скифы 11 класс Преимущества программы «1С:Зарплата и Управление Персоналом 8» при переходе с «1С:Зарплата и Кадры 7.7»
Преимущества программы «1С:Зарплата и Управление Персоналом 8» при переходе с «1С:Зарплата и Кадры 7.7» Устройство освещения пешеходного перехода.
Устройство освещения пешеходного перехода. Отчёт директора МБУ ДО ДШИ №1
Отчёт директора МБУ ДО ДШИ №1 Производительность МП и ее тестирование
Производительность МП и ее тестирование Как продавать продукты Embarcadero
Как продавать продукты Embarcadero Универсальные учебные действия в реализации системно – деятельностного подхода
Универсальные учебные действия в реализации системно – деятельностного подхода Презентация на тему Сергей Павлович Королев
Презентация на тему Сергей Павлович Королев