- Heart Failure

Содержание
- 2. HEART FAILURE Randa Mahmoud Al-Harizy Prof. of Internal Medicine
- 3. HEART FAILURE Clinical syndrome that can result from any structural or functional cardiac disorder that impairs
- 4. Main causes Ischemic heart disease, Cardiomyopathy, Hypertension Other causes: Valvular heart disease, Congenital heart disease, Alcohol
- 5. Impaired cardiac contractility as in myocardial infarction and cardiomyopathy Ventricular outflow obstruction (pressure overload) as in
- 6. Infections Arrhythmias Physical, Dietary, Fluid, Environmental, and Emotional Excesses. Myocardial infarction Pulmonary embolism Anemia Thyrotoxicosis and
- 7. The heart depends on a number of adaptive mechanisms for maintenance of its pumping function: 1-
- 8. PATHOPHYSIOLOGICAL CHANGES Ventricular dilatation Myocyte hypertrophy Increased collagen synthesis Altered myosin gene expression Altered sarcoplasmic Ca2+-ATPase
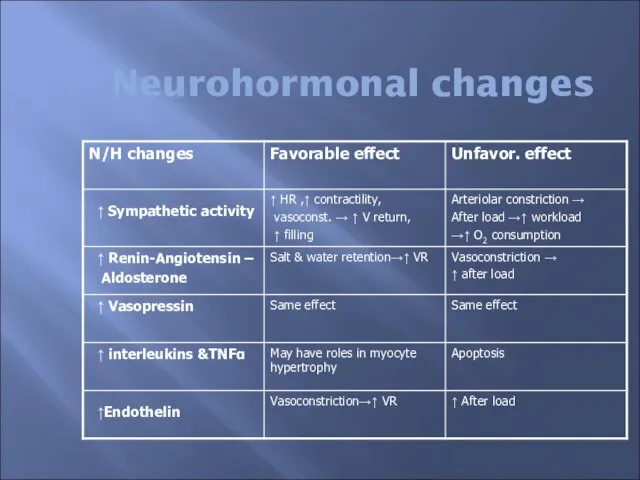
- 9. Neurohormonal changes
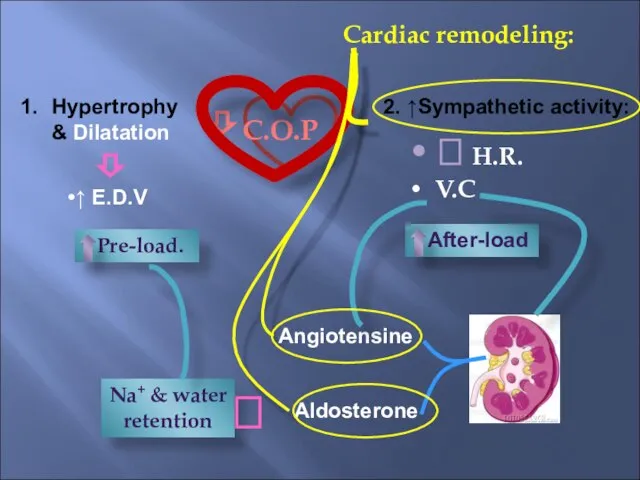
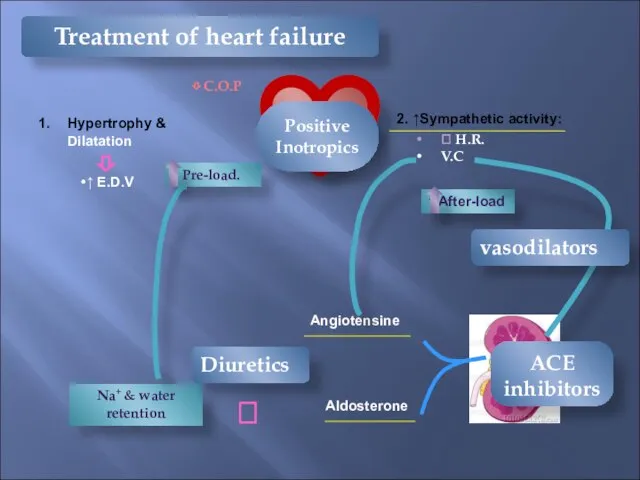
- 10. ⇩ C.O.P Cardiac remodeling: Hypertrophy & Dilatation ↑ E.D.V ⇩ 2. ↑Sympathetic activity: ⮥ H.R. V.C
- 11. CLINICAL SYNDROMES OF HEART FAILURE Left ventricular systolic dysfunction (LVSD) is commonly caused by ischaemic heart
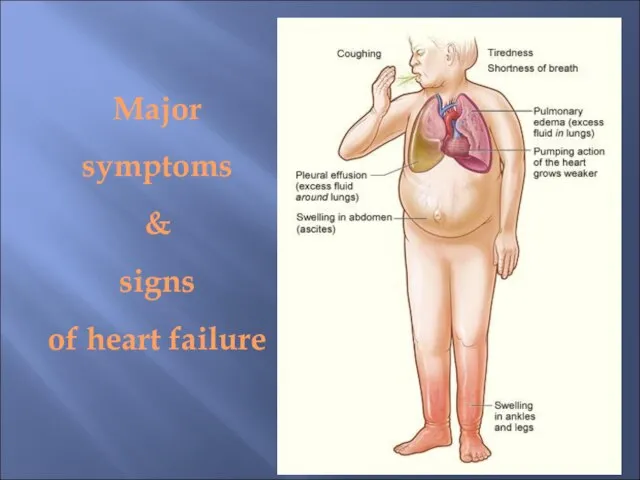
- 12. SYMPTOMS & SIGNS OF HEART FAILURE Left heart failure Symptoms are predominantly fatigue, exertional dyspnoea, orthopnoea
- 13. Right heart failure Symptoms (fatigue, breathlessness, anorexia and nausea) relate to distension and fluid accumulation in
- 14. Major symptoms & signs of heart failure
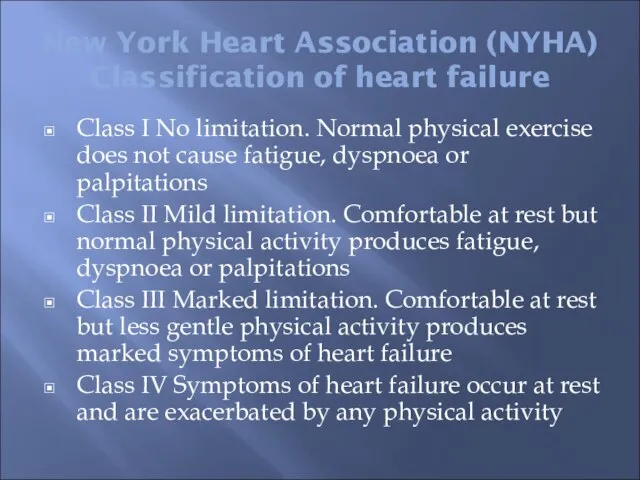
- 15. New York Heart Association (NYHA) Classification of heart failure Class I No limitation. Normal physical exercise
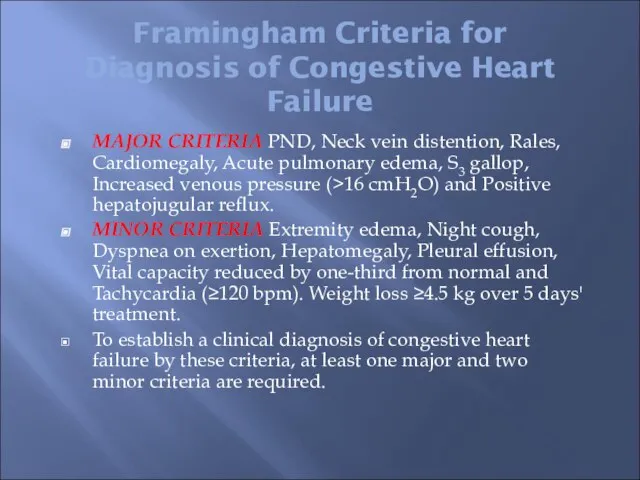
- 16. Framingham Criteria for Diagnosis of Congestive Heart Failure MAJOR CRITERIA PND, Neck vein distention, Rales, Cardiomegaly,
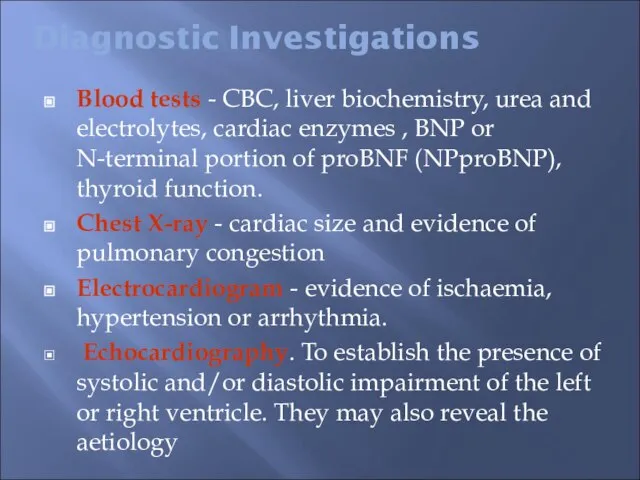
- 17. Diagnostic Investigations Blood tests - CBC, liver biochemistry, urea and electrolytes, cardiac enzymes , BNP or
- 18. BRAIN NATRIURETIC PEPTIDE (BNP) Pre pro-BNP is formed in the ventricles and, with myocyte stretch, is
- 19. Stress echocardiography. Exercise or pharmacological stress echocardiography has no radiation hazard and is a reliable technique
- 20. Treatment of Heart Failure The treatment of HF may be divided into five components: general measures.
- 21. Treatment of Heart Failure General measures: Rest, salt restriction, stop smoking Removal of the cause: This
- 22. ⇩ C.O.P Hypertrophy & Dilatation ↑ E.D.V ⇩ 2. ↑Sympathetic activity: ⮥ H.R. V.C ↑ After-load
- 24. Diuretics • Essential to control symptoms secondary to fluid retention • Prevent progression from HT to
- 25. Diuretics & ACEI reduces the number of sacks on the wagon
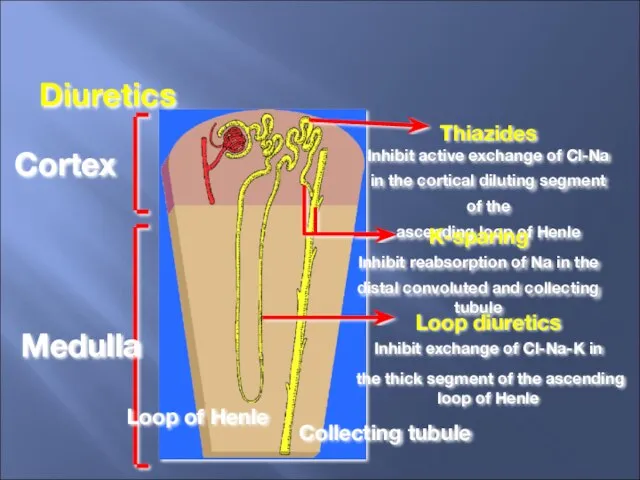
- 26. Cortex Medulla Thiazides Inhibit active exchange of Cl-Na in the cortical diluting segment of the ascending
- 27. Pharmacological Treatment Diuretics (loop diuretics, thiazide diuretics and potassium sparing diuretics) These act by promoting the
- 28. Diuretics (continue) Loop diuretics: such as furosemide and bumetanide Have a rapid onset of action (i.v.
- 29. Diuretics (continue) Thiazide diuretics: Thiazides are less effective in patients with reduced glomerular filtration rates. Thiazide
- 30. Diuretics (continue) Potassium-sparing diuretics: Spironolactone is a specific competitive antagonist to aldosterone, producing a weak diuresis
- 31. Vasodilator therapy Angiotensin-converting enzyme inhibitors ACEI: ACEI lower systemic vascular resistance and venous pressure, and reduce
- 32. Vasodilator therapy Angiotensin receptor antagonists: Angiotensin II receptor antagonists (ARA) (e.g. losartan, ibersartan, candesartan and valsartan)
- 33. Arteriolar vasodilators: Drugs such as α-adrenergic blockers (e.g. prazosin) and direct smooth-muscle relaxants (e.g. hydralazine) are
- 34. Venodilators: Short- and long-acting nitrates act by reducing preload and lowering venous pressure, with resulting reduction
- 35. β-Adrenoceptor blocking agents There is considerable evidence to support the use of beta-blockers in patients with
- 36. ß-Blockers Limit the donkey’s speed, thus saving energy
- 37. Inotropic Agents Intravenous inotropes are frequently used to support myocardial function in patients with acute left
- 38. Cardiac Glycosides Cardiac glycosides in clinical use are: Digoxin, Digitoxin Ouabain.
- 39. Digitalis Compounds Like the carrot placed in front of the donkey
- 40. Cardiac Glycosides Digitalis glycosides have been used for many years in patients with heart failure and
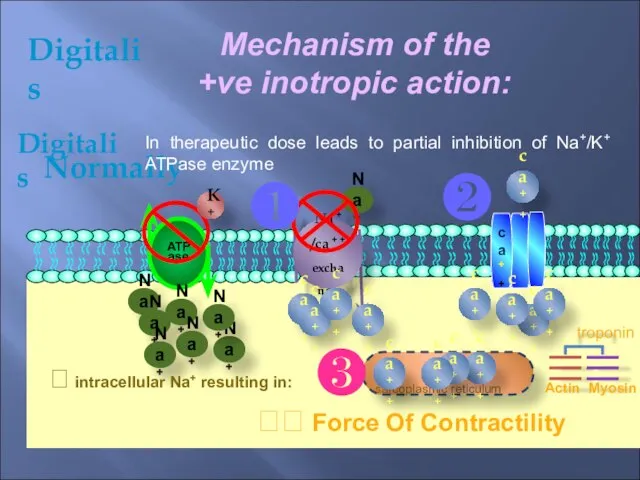
- 41. Digitalis Mechanism of the +ve inotropic action: ca++ ATPase ca++ Na+ Normally Digitalis In therapeutic dose
- 42. They have narrow safety margin GIT: Anorexia, nausea, vomiting (early toxicity) abdominal discomfort or pain and
- 43. C.V.S.: Any type of arrhythmia may be produced including: Bradycardia, Heart block, Ventricular extrasystole Ventricular fibrillation.
- 44. Gynecomastia: May be due to steroidal structure. Digitalis - Adverse (toxic) effects:
- 45. Treatment Of Digitalis Toxicitiy: 1) Stop the responsible drug. 2) KCl syrup or slow release or
- 46. ⮲Partial heart block is treated by atropine. ⮲ Ventricular arrhythmia without A-V block is treated by
- 47. OTHER MEDICATIONS Anticoagulants: Oral anticoagulants are recommended in patients with atrial fibrillation and in sinus rhythm
- 48. Antiarrhythmic agents: Precipitating factors should be treated, in particular electrolyte disturbance. Atrial fibrillation is common in
- 49. The administration of synthetic BNP (Nesritide) produces beneficial haemodynamic effects in acute heart failure (reducing pulmonary
- 50. NON-PHARMACOLOGICAL TREATMENT OF HEART FAILURE Revascularization Biventricular pacemaker or implantable cardioverter–defibrillator Cardiac transplantation
- 51. Cardiac Resynchronization Therapy Increase the donkey’s (heart) efficiency
- 52. Acute Heart FAILURE Acute heart failure (AHF) occurs with the rapid onset of symptoms and signs
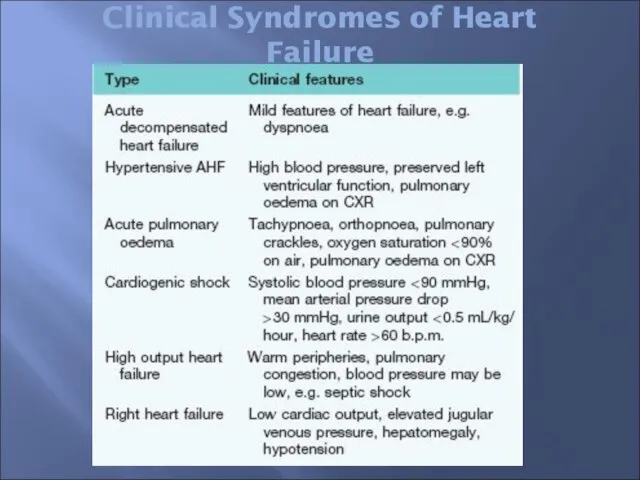
- 53. Clinical Syndromes of Heart Failure
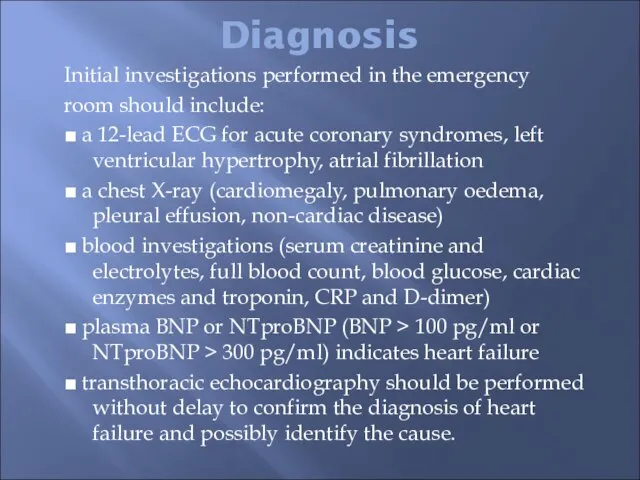
- 54. Diagnosis Initial investigations performed in the emergency room should include: ■ a 12-lead ECG for acute
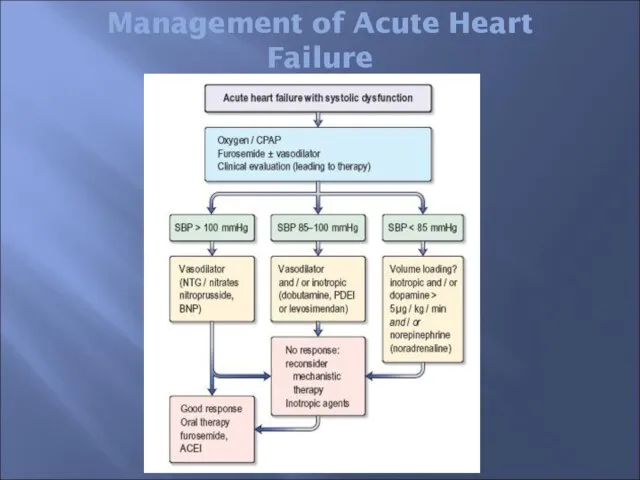
- 55. Management of Acute Heart Failure
- 56. Pulmonary Oedema PULMONARY OEDEMA This is a very frightening, life threatening emergency characterized by Extreme breathlessness.
- 57. TREATMENT - The patient must be placed in a sitting position. High-concentration oxygen is given. In
- 58. Cardiogenic Shock SHOCK is a severe failure of tissue perfusion, characterized by hypotension, a low cardiac
- 60. Скачать презентацию
Слайд 3HEART FAILURE
Clinical syndrome that can result from any structural or functional
HEART FAILURE
Clinical syndrome that can result from any structural or functional
Слайд 4Main causes
Ischemic heart disease, Cardiomyopathy, Hypertension
Other causes: Valvular heart disease, Congenital heart
disease,
Main causes
Ischemic heart disease, Cardiomyopathy, Hypertension
Other causes: Valvular heart disease, Congenital heart
disease,
Слайд 5Impaired cardiac contractility as in myocardial infarction and cardiomyopathy
Ventricular outflow obstruction (pressure
Impaired cardiac contractility as in myocardial infarction and cardiomyopathy
Ventricular outflow obstruction (pressure
Слайд 6Infections
Arrhythmias
Physical, Dietary, Fluid, Environmental, and Emotional Excesses.
Myocardial infarction
Pulmonary embolism
Anemia
Thyrotoxicosis and pregnancy
Aggravation of
Infections
Arrhythmias
Physical, Dietary, Fluid, Environmental, and Emotional Excesses.
Myocardial infarction
Pulmonary embolism
Anemia
Thyrotoxicosis and pregnancy
Aggravation of
Слайд 7The heart depends on a number of adaptive
mechanisms for maintenance of its
The heart depends on a number of adaptive
mechanisms for maintenance of its
Слайд 8PATHOPHYSIOLOGICAL CHANGES
Ventricular dilatation
Myocyte hypertrophy
Increased collagen synthesis
Altered myosin gene expression
Altered sarcoplasmic Ca2+-ATPase density
Increased
PATHOPHYSIOLOGICAL CHANGES
Ventricular dilatation
Myocyte hypertrophy
Increased collagen synthesis
Altered myosin gene expression
Altered sarcoplasmic Ca2+-ATPase density
Increased
Слайд 9Neurohormonal changes
Neurohormonal changes
Слайд 10⇩ C.O.P
Cardiac remodeling:
Hypertrophy & Dilatation
↑ E.D.V
⇩
2. ↑Sympathetic activity:
⮥ H.R.
V.C
↑ After-load
↑ Pre-load.
Angiotensine
Aldosterone
Na+
⇩ C.O.P
Cardiac remodeling:
Hypertrophy & Dilatation
↑ E.D.V
⇩
2. ↑Sympathetic activity:
⮥ H.R.
V.C
↑ After-load
↑ Pre-load.
Angiotensine
Aldosterone
Na+
Слайд 11CLINICAL SYNDROMES OF HEART FAILURE
Left ventricular systolic dysfunction (LVSD) is commonly caused
CLINICAL SYNDROMES OF HEART FAILURE
Left ventricular systolic dysfunction (LVSD) is commonly caused
Слайд 12SYMPTOMS & SIGNS OF HEART FAILURE
Left heart failure
Symptoms are predominantly fatigue,
exertional
SYMPTOMS & SIGNS OF HEART FAILURE
Left heart failure
Symptoms are predominantly fatigue,
exertional
Слайд 13Right heart failure
Symptoms (fatigue, breathlessness, anorexia and nausea) relate to distension and
Right heart failure
Symptoms (fatigue, breathlessness, anorexia and nausea) relate to distension and
Слайд 14Major symptoms
&
signs
of heart failure
Major symptoms
&
signs
of heart failure
Слайд 15New York Heart Association (NYHA)
Classification of heart failure
Class I No limitation. Normal
New York Heart Association (NYHA)
Classification of heart failure
Class I No limitation. Normal
Слайд 16Framingham Criteria for Diagnosis of Congestive Heart Failure
MAJOR CRITERIA PND, Neck vein
Framingham Criteria for Diagnosis of Congestive Heart Failure
MAJOR CRITERIA PND, Neck vein
Слайд 17Diagnostic Investigations
Blood tests - CBC, liver biochemistry, urea and electrolytes, cardiac enzymes
Diagnostic Investigations
Blood tests - CBC, liver biochemistry, urea and electrolytes, cardiac enzymes
Слайд 18BRAIN NATRIURETIC PEPTIDE (BNP)
Pre pro-BNP is formed in the ventricles and, with
BRAIN NATRIURETIC PEPTIDE (BNP)
Pre pro-BNP is formed in the ventricles and, with
Слайд 19Stress echocardiography. Exercise or pharmacological stress echocardiography has no radiation hazard and
Stress echocardiography. Exercise or pharmacological stress echocardiography has no radiation hazard and
Слайд 20Treatment of Heart Failure
The treatment of HF may be divided into five
components:
Treatment of Heart Failure
The treatment of HF may be divided into five
components:
Слайд 21Treatment of Heart Failure
General measures:
Rest, salt restriction, stop smoking
Removal of the
Treatment of Heart Failure
General measures:
Rest, salt restriction, stop smoking
Removal of the
Слайд 22⇩ C.O.P
Hypertrophy & Dilatation
↑ E.D.V
⇩
2. ↑Sympathetic activity:
⮥ H.R.
V.C
↑ After-load
↑ Pre-load.
Angiotensine
Aldosterone
Na+ &
⇩ C.O.P
Hypertrophy & Dilatation
↑ E.D.V
⇩
2. ↑Sympathetic activity:
⮥ H.R.
V.C
↑ After-load
↑ Pre-load.
Angiotensine
Aldosterone
Na+ &
Слайд 24Diuretics
• Essential to control symptoms
secondary to fluid retention
• Prevent progression from HT
Diuretics
• Essential to control symptoms
secondary to fluid retention
• Prevent progression from HT
Слайд 25Diuretics & ACEI reduces the number of sacks on the wagon
Diuretics & ACEI reduces the number of sacks on the wagon
Слайд 26Cortex
Medulla
Thiazides
Inhibit active exchange of Cl-Na
in the cortical diluting segment of the
Cortex
Medulla
Thiazides
Inhibit active exchange of Cl-Na
in the cortical diluting segment of the
Слайд 27Pharmacological Treatment
Diuretics
(loop diuretics, thiazide diuretics and potassium sparing diuretics)
These act by
Pharmacological Treatment
Diuretics
(loop diuretics, thiazide diuretics and potassium sparing diuretics)
These act by
Слайд 28Diuretics (continue)
Loop diuretics: such as furosemide and
bumetanide
Have a rapid onset
Diuretics (continue)
Loop diuretics: such as furosemide and
bumetanide
Have a rapid onset
Слайд 29Diuretics (continue)
Thiazide diuretics:
Thiazides are less effective in patients with reduced
Diuretics (continue)
Thiazide diuretics:
Thiazides are less effective in patients with reduced
Слайд 30Diuretics (continue)
Potassium-sparing diuretics:
Spironolactone is a specific competitive antagonist to aldosterone, producing
Diuretics (continue)
Potassium-sparing diuretics:
Spironolactone is a specific competitive antagonist to aldosterone, producing
Слайд 31Vasodilator therapy
Angiotensin-converting enzyme inhibitors ACEI:
ACEI lower systemic vascular resistance and venous
Vasodilator therapy
Angiotensin-converting enzyme inhibitors ACEI:
ACEI lower systemic vascular resistance and venous
Слайд 32Vasodilator therapy
Angiotensin receptor antagonists:
Angiotensin II receptor antagonists (ARA) (e.g. losartan, ibersartan,
Vasodilator therapy
Angiotensin receptor antagonists:
Angiotensin II receptor antagonists (ARA) (e.g. losartan, ibersartan,
Слайд 33Arteriolar vasodilators:
Drugs such as α-adrenergic blockers (e.g. prazosin) and direct smooth-muscle
Arteriolar vasodilators:
Drugs such as α-adrenergic blockers (e.g. prazosin) and direct smooth-muscle
Слайд 34Venodilators:
Short- and long-acting nitrates act by reducing preload and lowering venous
Short- and long-acting nitrates act by reducing preload and lowering venous
Слайд 35β-Adrenoceptor blocking agents
There is considerable evidence to support the use of
β-Adrenoceptor blocking agents
There is considerable evidence to support the use of
Слайд 36ß-Blockers
Limit the donkey’s speed, thus saving energy
ß-Blockers
Limit the donkey’s speed, thus saving energy
Слайд 37Inotropic Agents
Intravenous inotropes are frequently used to support myocardial function
Inotropic Agents
Intravenous inotropes are frequently used to support myocardial function
Слайд 38Cardiac Glycosides
Cardiac glycosides in clinical use are:
Digoxin,
Digitoxin
Ouabain.
Cardiac Glycosides
Cardiac glycosides in clinical use are:
Digoxin,
Digitoxin
Ouabain.
Слайд 39Digitalis Compounds
Like the carrot placed in front of the donkey
Digitalis Compounds
Like the carrot placed in front of the donkey

Слайд 40Cardiac Glycosides
Digitalis glycosides have been used for many years in patients with
Cardiac Glycosides
Digitalis glycosides have been used for many years in patients with
Слайд 41Digitalis
Mechanism of the +ve inotropic action:
ca++
ATPase
ca++
Na+
Normally
Digitalis
In therapeutic dose
Digitalis
Mechanism of the +ve inotropic action:
ca++
ATPase
ca++
Na+
Normally
Digitalis
In therapeutic dose
Слайд 42They have narrow safety margin
GIT:
Anorexia, nausea, vomiting (early toxicity)
abdominal discomfort
They have narrow safety margin
GIT:
Anorexia, nausea, vomiting (early toxicity)
abdominal discomfort
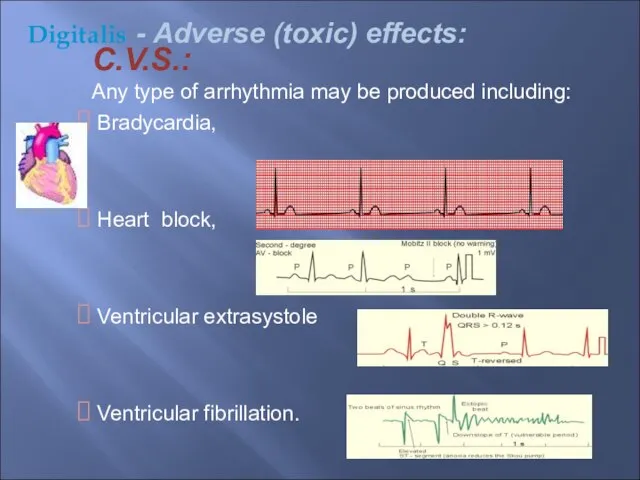
Слайд 43C.V.S.:
Any type of arrhythmia may be produced including:
Bradycardia,
Heart block,
C.V.S.:
Any type of arrhythmia may be produced including:
Bradycardia,
Heart block,
Слайд 44Gynecomastia:
May be due to steroidal structure.
Digitalis
- Adverse (toxic) effects:
Gynecomastia:
May be due to steroidal structure.
Digitalis
- Adverse (toxic) effects:
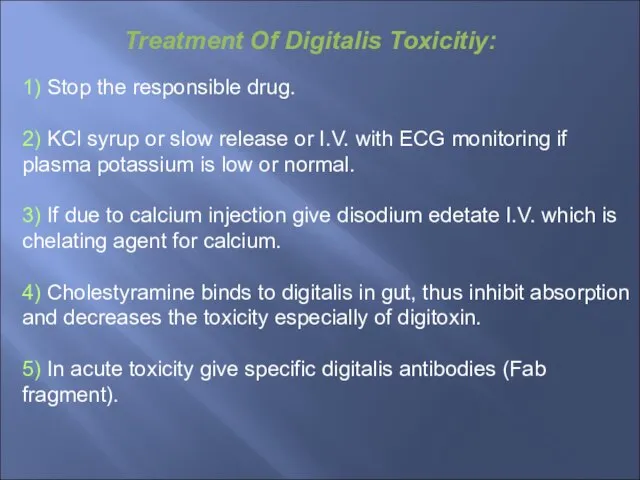
Слайд 45Treatment Of Digitalis Toxicitiy:
1) Stop the responsible drug.
2) KCl syrup or slow
Treatment Of Digitalis Toxicitiy:
1) Stop the responsible drug.
2) KCl syrup or slow
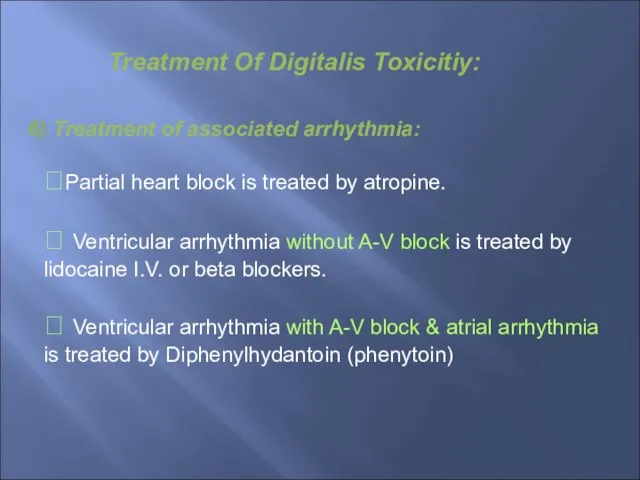
Слайд 46⮲Partial heart block is treated by atropine.
⮲ Ventricular arrhythmia without A-V block
⮲Partial heart block is treated by atropine.
⮲ Ventricular arrhythmia without A-V block
Слайд 47OTHER MEDICATIONS
Anticoagulants:
Oral anticoagulants are recommended in patients with atrial fibrillation and
OTHER MEDICATIONS
Anticoagulants:
Oral anticoagulants are recommended in patients with atrial fibrillation and
Слайд 48Antiarrhythmic agents:
Precipitating factors should be treated, in particular electrolyte disturbance.
Atrial
Antiarrhythmic agents:
Precipitating factors should be treated, in particular electrolyte disturbance.
Atrial
Слайд 49The administration of synthetic BNP (Nesritide) produces beneficial haemodynamic effects in acute
The administration of synthetic BNP (Nesritide) produces beneficial haemodynamic effects in acute
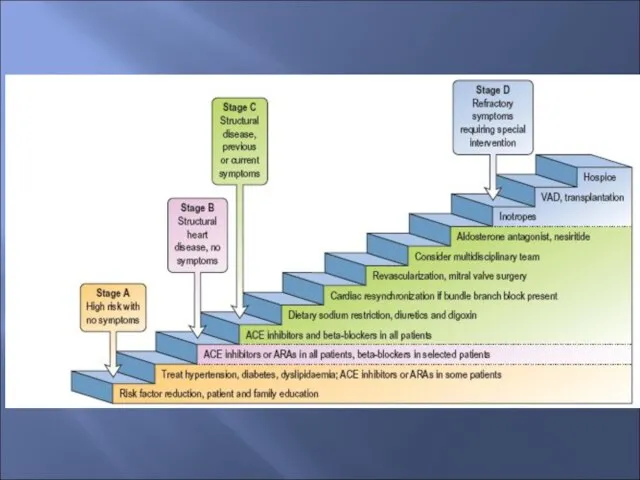
Слайд 50NON-PHARMACOLOGICAL TREATMENT OF HEART FAILURE
Revascularization
Biventricular pacemaker or implantable cardioverter–defibrillator
Cardiac transplantation
NON-PHARMACOLOGICAL TREATMENT OF HEART FAILURE
Revascularization
Biventricular pacemaker or implantable cardioverter–defibrillator
Cardiac transplantation
Слайд 51Cardiac Resynchronization Therapy
Increase the donkey’s (heart) efficiency
Cardiac Resynchronization Therapy
Increase the donkey’s (heart) efficiency
Слайд 52Acute Heart FAILURE
Acute heart failure (AHF) occurs with the rapid onset of
Acute Heart FAILURE
Acute heart failure (AHF) occurs with the rapid onset of
Слайд 53Clinical Syndromes of Heart Failure
Clinical Syndromes of Heart Failure
Слайд 54Diagnosis
Initial investigations performed in the emergency
room should include:
■ a 12-lead ECG for
Diagnosis
Initial investigations performed in the emergency
room should include:
■ a 12-lead ECG for
Слайд 55Management of Acute Heart Failure
Management of Acute Heart Failure
Слайд 56Pulmonary Oedema
PULMONARY OEDEMA
This is a very frightening, life threatening emergency characterized
Pulmonary Oedema
PULMONARY OEDEMA
This is a very frightening, life threatening emergency characterized
Слайд 57TREATMENT
- The patient must be placed in a sitting position.
- The patient must be placed in a sitting position.
Слайд 58Cardiogenic Shock
SHOCK is a severe failure of tissue perfusion, characterized by hypotension,
Cardiogenic Shock
SHOCK is a severe failure of tissue perfusion, characterized by hypotension,

 Тамчышоу. Тел дигән дәрья бар
Тамчышоу. Тел дигән дәрья бар Культурология как наука. Лекция 1
Культурология как наука. Лекция 1 Планирование и управление временем
Планирование и управление временем Объективы
Объективы 03_LOGITECH. B2B C&P Pres
03_LOGITECH. B2B C&P Pres Исследование фактов из жизни А. С. Пушкина, приведших к гибели поэта
Исследование фактов из жизни А. С. Пушкина, приведших к гибели поэта Презентация на тему Афиша
Презентация на тему Афиша Кафедра косметологии и массажа
Кафедра косметологии и массажа Plant tissue culture and applications
Plant tissue culture and applications Презентация по теме: «Личная гигиена больного»
Презентация по теме: «Личная гигиена больного» Great Britain
Great Britain www.sic-marking.ru ЗАО «ЮНИТ МАРК ПРО»
www.sic-marking.ru ЗАО «ЮНИТ МАРК ПРО» Улучшение качества мясных продуктов за последние 20 лет
Улучшение качества мясных продуктов за последние 20 лет Природа в лирике русских поэтов
Природа в лирике русских поэтов Основы здорового образа жизни
Основы здорового образа жизни Фармакокорректоры
Фармакокорректоры  Учебный проект «Станционный смотритель» или «История блудной дочери?…»
Учебный проект «Станционный смотритель» или «История блудной дочери?…» Легкая атлетика в системе физического воспитания
Легкая атлетика в системе физического воспитания 1-2 Software
1-2 Software Инженерно-экологические изыскания
Инженерно-экологические изыскания Элективный курс: Подросток и закон. Если тебя задержала милиция…
Элективный курс: Подросток и закон. Если тебя задержала милиция… Реформы Н.С. Хрущева
Реформы Н.С. Хрущева Финансирование и налогообложение в сфере образования
Финансирование и налогообложение в сфере образования СИСТЕМА МЕТОДИЧЕСКОЙ РАБОТЫ В ОБРАЗОВАТЕЛЬНЫХ УЧРЕЖДЕНИЯХ В УСЛОВИЯХ МОДЕРНИЗАЦИИ ОБРАЗОВАНИЯ
СИСТЕМА МЕТОДИЧЕСКОЙ РАБОТЫ В ОБРАЗОВАТЕЛЬНЫХ УЧРЕЖДЕНИЯХ В УСЛОВИЯХ МОДЕРНИЗАЦИИ ОБРАЗОВАНИЯ ПРЕЗЕНТАЦИЯ НА ТЕМУ ФИЛОСОФЫ ДРЕВНЕЙ ГРЕЦИИ
ПРЕЗЕНТАЦИЯ НА ТЕМУ ФИЛОСОФЫ ДРЕВНЕЙ ГРЕЦИИ  Strategic Marketing
Strategic Marketing  Законы России
Законы России Математика. Задачи
Математика. Задачи