- path anat

Содержание
- 2. INTRODUCTION PRIMARY CARCINOMA OF THE GALLBLADDER IS MORE PREVALENT THAN OTHER CANCERS OF THE EXTRAHEPATIC BILIARY
- 3. ETIOLOGY NUMBER OF ETIOLOGIC FACTORS HAVE BEEN IMPLICATED. 1. CHOLELITHIASIS AND CHOLECYSTITIS. THE MOST SIGNIFICANT ASSOCIATION
- 5. 2. CHEMICAL CARCINOGENS. A NUMBER OF CHEMICAL CARCINOGENS STRUCTURALLY SIMILAR TO NATURALLY-OCCURRING BILE ACIDS HAVE BEEN
- 6. 3. GENETIC FACTORS. THERE IS HIGHER INCIDENCE OF CANCER OF THE GALLBLADDER IN CERTAIN POPULATIONS LIVING
- 7. 4. MISCELLANEOUS. PATIENTS WHO HAVE UNDERGONE PREVIOUS SURGERY ON THE BILIARY TRACT HAVE HIGHER INCIDENCE OF
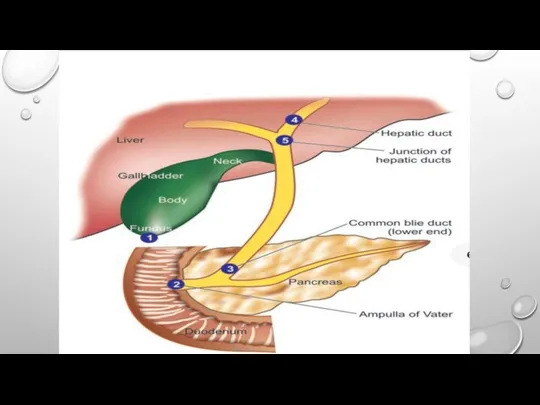
- 8. MORPHOLOGICAL FEATURES THE COMMONEST SITE IS THE FUNDUS, FOLLOWED NEXT IN FREQUENCY BY THE NECK OF
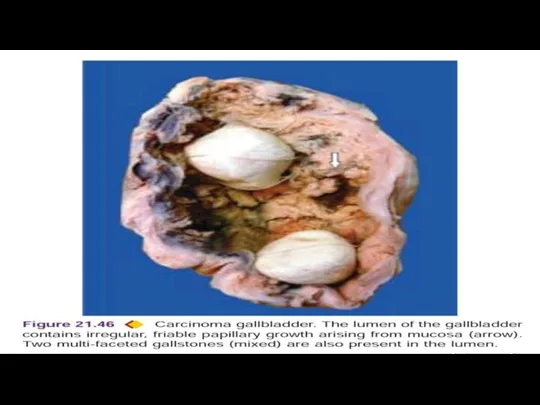
- 10. 2. FUNGATING TYPE GROWS LIKE AN IRREGULAR, FRIABLE, PAPILLARY OR CAULIFLOWER-LIKE GROWTH INTO THE LUMEN AS
- 11. HISTOLOGICAL FEATURES 1. MOST GALLBLADDER CANCERS ARE ADENOCARCINOMAS (90%). THEY MAY BE PAPILLARY OR INFILTRATIVE, WELL-DIFFERENTIATED
- 12. CLINICAL FEATURES CARCINOMA OF THE GALLBADDER IS SLOW-GROWING AND CAUSES SYMPTOMS LATE IN THE COURSE OF
- 13. DIAGNOSIS BLOOD TESTS. BLOOD TESTS TO EVALUATE YOUR LIVER FUNCTION MAY HELP YOUR DOCTOR DETERMINE WHAT’S
- 14. TREATMENT GALLBLADDER CANCER TREATMENT OPTIONS ARE AVAILABLE TO YOU WILL DEPEND ON THE STAGE OF YOUR
- 16. Скачать презентацию
Слайд 3ETIOLOGY
NUMBER OF ETIOLOGIC FACTORS HAVE BEEN IMPLICATED.
1. CHOLELITHIASIS AND CHOLECYSTITIS.
ETIOLOGY
NUMBER OF ETIOLOGIC FACTORS HAVE BEEN IMPLICATED.
1. CHOLELITHIASIS AND CHOLECYSTITIS.
Слайд 52. CHEMICAL CARCINOGENS.
A NUMBER OF CHEMICAL CARCINOGENS STRUCTURALLY SIMILAR TO NATURALLY-OCCURRING
2. CHEMICAL CARCINOGENS.
A NUMBER OF CHEMICAL CARCINOGENS STRUCTURALLY SIMILAR TO NATURALLY-OCCURRING
Слайд 63. GENETIC FACTORS.
THERE IS HIGHER INCIDENCE OF CANCER OF THE GALLBLADDER
3. GENETIC FACTORS.
THERE IS HIGHER INCIDENCE OF CANCER OF THE GALLBLADDER
Слайд 74. MISCELLANEOUS.
PATIENTS WHO HAVE UNDERGONE PREVIOUS SURGERY ON THE BILIARY TRACT
4. MISCELLANEOUS.
PATIENTS WHO HAVE UNDERGONE PREVIOUS SURGERY ON THE BILIARY TRACT
Слайд 8MORPHOLOGICAL FEATURES
THE COMMONEST SITE IS THE FUNDUS, FOLLOWED NEXT IN FREQUENCY
MORPHOLOGICAL FEATURES
THE COMMONEST SITE IS THE FUNDUS, FOLLOWED NEXT IN FREQUENCY
Слайд 102. FUNGATING TYPE
GROWS LIKE AN IRREGULAR, FRIABLE, PAPILLARY OR CAULIFLOWER-LIKE GROWTH
2. FUNGATING TYPE
GROWS LIKE AN IRREGULAR, FRIABLE, PAPILLARY OR CAULIFLOWER-LIKE GROWTH
Слайд 11HISTOLOGICAL FEATURES
1. MOST GALLBLADDER CANCERS ARE ADENOCARCINOMAS (90%). THEY MAY BE PAPILLARY
HISTOLOGICAL FEATURES
1. MOST GALLBLADDER CANCERS ARE ADENOCARCINOMAS (90%). THEY MAY BE PAPILLARY
Слайд 12CLINICAL FEATURES
CARCINOMA OF THE GALLBADDER IS SLOW-GROWING AND CAUSES SYMPTOMS LATE IN
CLINICAL FEATURES
CARCINOMA OF THE GALLBADDER IS SLOW-GROWING AND CAUSES SYMPTOMS LATE IN
Слайд 13DIAGNOSIS
BLOOD TESTS. BLOOD TESTS TO EVALUATE YOUR LIVER FUNCTION MAY HELP YOUR
DIAGNOSIS
BLOOD TESTS. BLOOD TESTS TO EVALUATE YOUR LIVER FUNCTION MAY HELP YOUR
Слайд 14TREATMENT
GALLBLADDER CANCER TREATMENT OPTIONS ARE AVAILABLE TO YOU WILL DEPEND ON THE
TREATMENT
GALLBLADDER CANCER TREATMENT OPTIONS ARE AVAILABLE TO YOU WILL DEPEND ON THE
 подготовке мероприятий, посвящённых празднованию Дня России в городе Ярославле
подготовке мероприятий, посвящённых празднованию Дня России в городе Ярославле Презентация на тему Параллельность прямых и плоскостей
Презентация на тему Параллельность прямых и плоскостей Виды сложноподчиненных предложений
Виды сложноподчиненных предложений Осанка - залог здоровья!
Осанка - залог здоровья! Нежилое помещение
Нежилое помещение Презентация на тему Курение или здоровье - выбирайте!
Презентация на тему Курение или здоровье - выбирайте! Present simple
Present simple  Презентация на тему Части речи 1 класс
Презентация на тему Части речи 1 класс Страницы памяти семейной... История швейной машинки в нашей семье
Страницы памяти семейной... История швейной машинки в нашей семье Презентация 4
Презентация 4 Выносные видоискатели разных типов студийных камер и их настройка
Выносные видоискатели разных типов студийных камер и их настройка Основания и этапы организации исследовательской деятельности при обучении английскому языку делового общения в Лингвистическом
Основания и этапы организации исследовательской деятельности при обучении английскому языку делового общения в Лингвистическом  Моё увлечение
Моё увлечение Формирование комфортной городской среды. Сквер в 5 микрорайоне, г. Югра
Формирование комфортной городской среды. Сквер в 5 микрорайоне, г. Югра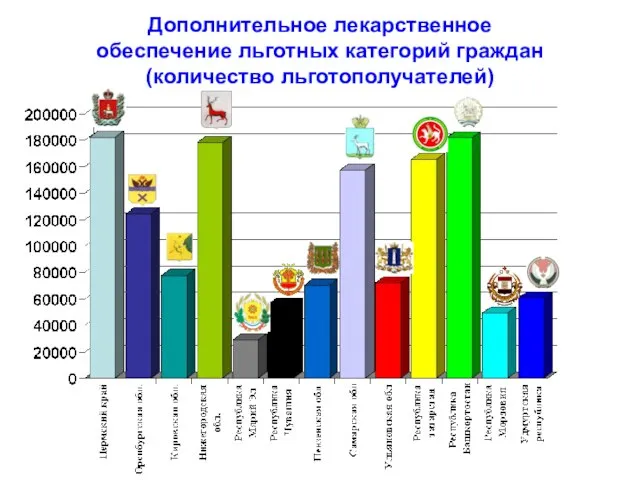 Дополнительное лекарственное обеспечение льготных категорий граждан (количество льготополучателей)
Дополнительное лекарственное обеспечение льготных категорий граждан (количество льготополучателей) Электронное правительство Тюменской области
Электронное правительство Тюменской области Презентация print GB 36 6
Презентация print GB 36 6 Культура Серебряного века
Культура Серебряного века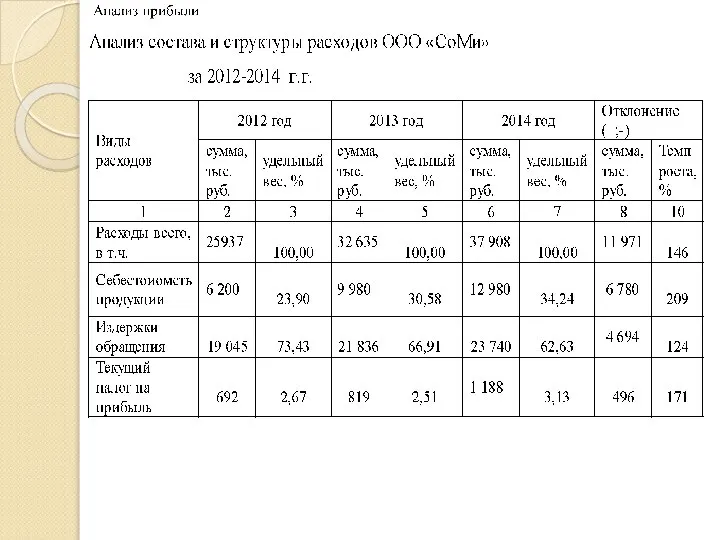 Корпоративные финансы. Анализ состава и структуры расходов ООО СоМи
Корпоративные финансы. Анализ состава и структуры расходов ООО СоМи О компании Компания «Форт» уже более 15 лет успешно работает на рынке Уральского региона в различных сферах деятельности. Благодар
О компании Компания «Форт» уже более 15 лет успешно работает на рынке Уральского региона в различных сферах деятельности. Благодар Муниципальное общеобразовательное учреждение начальная общеобразовательная школа № 12 «Гармония»
Муниципальное общеобразовательное учреждение начальная общеобразовательная школа № 12 «Гармония»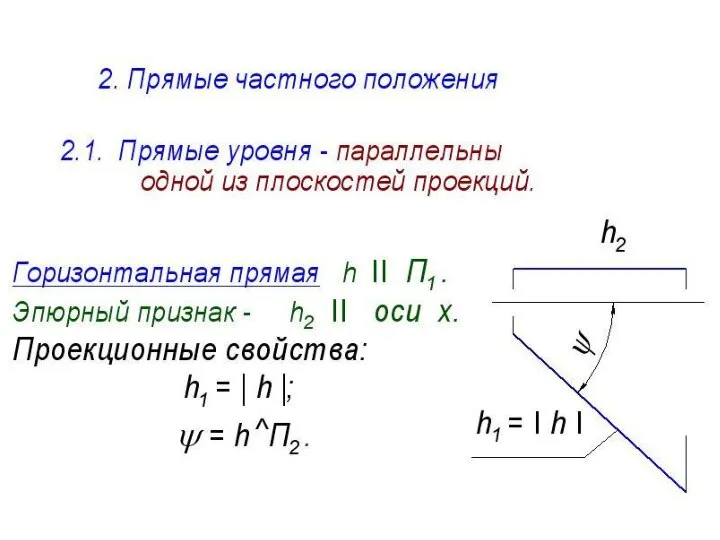 Прямые частного положения
Прямые частного положения СОХРАНЕНИЕ ЕЛОЧКИ – ЛЕСНОЙ КРАСАВИЦЫ
СОХРАНЕНИЕ ЕЛОЧКИ – ЛЕСНОЙ КРАСАВИЦЫ Проект
Проект Презентация
Презентация Повышение мотивации учебной деятельности учащихся на уроках географии
Повышение мотивации учебной деятельности учащихся на уроках географии Презентация на тему Молодежная субкультура
Презентация на тему Молодежная субкультура Электронное книгоиздание. Устройства для чтения и их применение в библиотеках Открытая практико-ориентированная лекция Москв
Электронное книгоиздание. Устройства для чтения и их применение в библиотеках Открытая практико-ориентированная лекция Москв