- PATH%20ANT-1.. (1)

Содержание
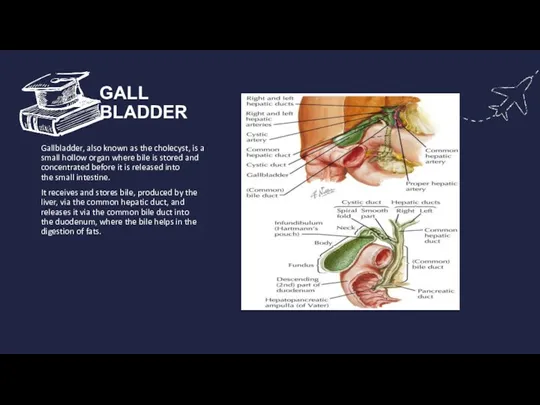
- 2. GALL BLADDER Gallbladder, also known as the cholecyst, is a small hollow organ where bile is
- 3. CHOLECYSTITIS Cholecystitis or infl ammation of the gallbladder may be acute, chronic, or acute superimposed on
- 4. CAUSES SEVERE ILLNESS BILE DUCT BLOCKAGE INFECTION TUMOR GALLSTONES
- 5. TYPES OF CHOLECYSTITIS CHRONIC ACUTE
- 6. CHRONIC CHOLECYSTITIS Chronic cholecystitis is the commonest type of clinical gallbladder disease. Th ere is almost
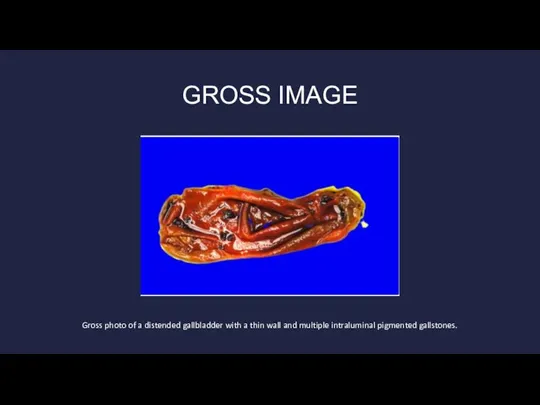
- 7. GROSS IMAGE Gross photo of a distended gallbladder with a thin wall and multiple intraluminal pigmented
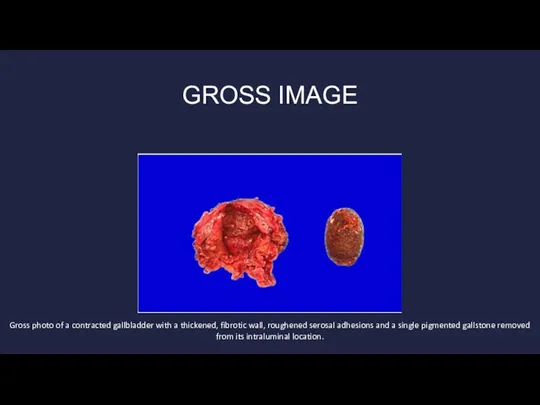
- 8. GROSS IMAGE Gross photo of a contracted gallbladder with a thickened, fibrotic wall, roughened serosal adhesions
- 9. MORPHOLOGIC FEATURES The gallbladder is generally contracted but may be normal or enlarged . The wall
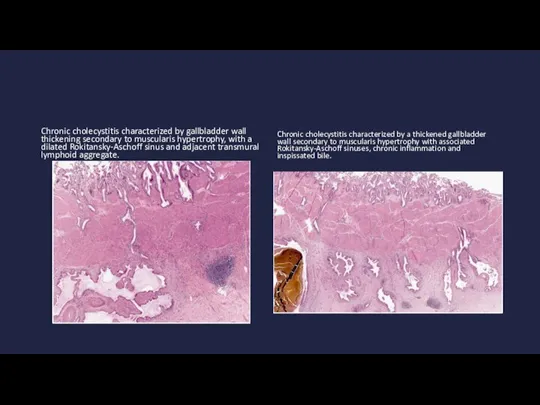
- 10. Chronic cholecystitis characterized by gallbladder wall thickening secondary to muscularis hypertrophy, with a dilated Rokitansky-Aschoff sinus
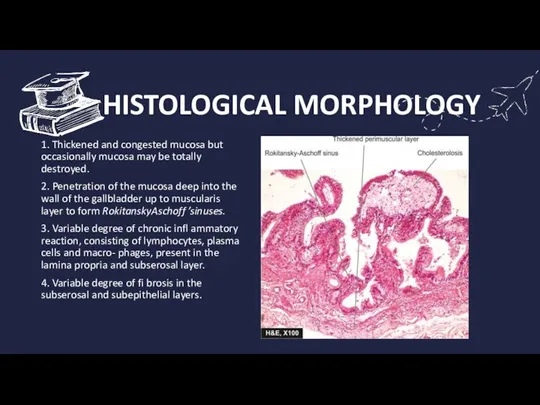
- 11. HISTOLOGICAL MORPHOLOGY 1. Thickened and congested mucosa but occasionally mucosa may be totally destroyed. 2. Penetration
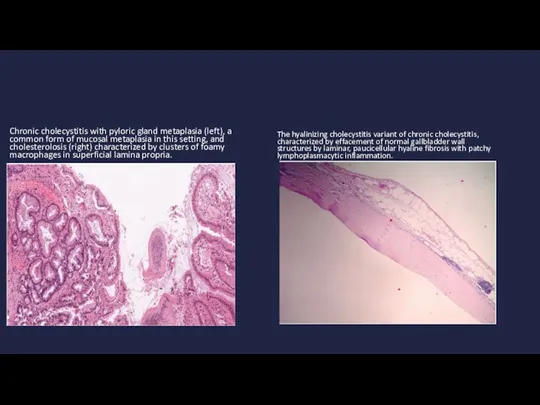
- 12. Chronic cholecystitis with pyloric gland metaplasia (left), a common form of mucosal metaplasia in this setting,
- 13. A few morphologic variants of chronic chole cystitis are considered below: Cholecystitis glandularis, when the mucosal
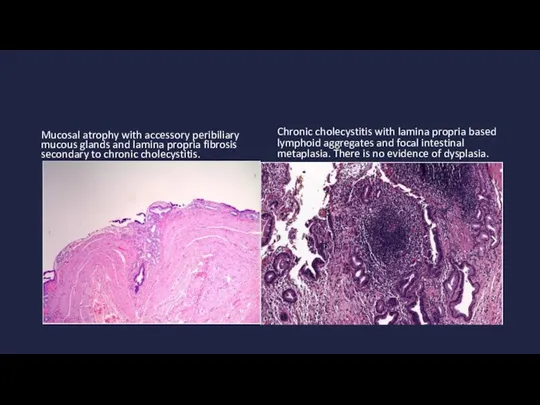
- 14. Mucosal atrophy with accessory peribiliary mucous glands and lamina propria fibrosis secondary to chronic cholecystitis. Chronic
- 15. Complications If untreated, cholecystitis can lead to a number of serious complications, including: Infection within the
- 16. PREVENTION You can reduce your risk of cholecystitis by taking the following steps to prevent gallstones:
- 17. DIAGONISTIC To diagnose cholecystis, your health care provider will likely do a physical exam and discuss
- 18. CLINICAL FEATURES Vomiting Tenderness over your abdomen when it's touched Nausea Pain that spreads to your
- 19. TREATMENT Treatment for cholecystitis usually involves a hospital stay to control the inflammation in your gallbladder.
- 20. TREATMENT Gallbladder drainage. In some cases, such as when surgery to remove the gallbladder is not
- 22. Скачать презентацию
Слайд 2GALL BLADDER
Gallbladder, also known as the cholecyst, is a small hollow organ where bile is stored
GALL BLADDER
Gallbladder, also known as the cholecyst, is a small hollow organ where bile is stored
Слайд 3CHOLECYSTITIS
Cholecystitis or infl ammation of the gallbladder may be acute, chronic, or
CHOLECYSTITIS
Cholecystitis or infl ammation of the gallbladder may be acute, chronic, or
Слайд 4CAUSES
SEVERE ILLNESS
BILE DUCT BLOCKAGE
INFECTION
TUMOR
GALLSTONES
CAUSES
SEVERE ILLNESS
BILE DUCT BLOCKAGE
INFECTION
TUMOR
GALLSTONES
Слайд 5 TYPES OF CHOLECYSTITIS
CHRONIC ACUTE
TYPES OF CHOLECYSTITIS
CHRONIC ACUTE
Слайд 6CHRONIC CHOLECYSTITIS
Chronic cholecystitis is the commonest type of clinical gallbladder disease. Th
CHRONIC CHOLECYSTITIS
Chronic cholecystitis is the commonest type of clinical gallbladder disease. Th
Слайд 7GROSS IMAGE
Gross photo of a distended gallbladder with a thin wall and
GROSS IMAGE
Gross photo of a distended gallbladder with a thin wall and
Слайд 8GROSS IMAGE
Gross photo of a contracted gallbladder with a thickened, fibrotic wall,
GROSS IMAGE
Gross photo of a contracted gallbladder with a thickened, fibrotic wall,
Слайд 9 MORPHOLOGIC FEATURES
The gallbladder is generally contracted but may be normal
MORPHOLOGIC FEATURES
The gallbladder is generally contracted but may be normal
Слайд 10Chronic cholecystitis characterized by gallbladder wall thickening secondary to muscularis hypertrophy, with
Chronic cholecystitis characterized by gallbladder wall thickening secondary to muscularis hypertrophy, with
Слайд 11 HISTOLOGICAL MORPHOLOGY
1. Thickened and congested mucosa but occasionally mucosa may be
HISTOLOGICAL MORPHOLOGY
1. Thickened and congested mucosa but occasionally mucosa may be
Слайд 12Chronic cholecystitis with pyloric gland metaplasia (left), a common form of mucosal
Chronic cholecystitis with pyloric gland metaplasia (left), a common form of mucosal
Слайд 13A few morphologic variants of chronic chole cystitis are
considered below:
Cholecystitis glandularis,
A few morphologic variants of chronic chole cystitis are
considered below:
Cholecystitis glandularis,
Слайд 14Mucosal atrophy with accessory peribiliary mucous glands and lamina propria fibrosis secondary
Mucosal atrophy with accessory peribiliary mucous glands and lamina propria fibrosis secondary
Слайд 15Complications
If untreated, cholecystitis can lead to a number of serious complications, including:
Infection
Complications
If untreated, cholecystitis can lead to a number of serious complications, including:
Infection

Слайд 16PREVENTION
You can reduce your risk of cholecystitis by taking the following steps
PREVENTION
You can reduce your risk of cholecystitis by taking the following steps
Слайд 17DIAGONISTIC
To diagnose cholecystis, your health care provider will likely do a physical
DIAGONISTIC
To diagnose cholecystis, your health care provider will likely do a physical
Слайд 18CLINICAL FEATURES
Vomiting
Tenderness over your abdomen when it's touched
Nausea
Pain that spreads to your
CLINICAL FEATURES
Vomiting
Tenderness over your abdomen when it's touched
Nausea
Pain that spreads to your
Слайд 19TREATMENT
Treatment for cholecystitis usually involves a hospital stay to control the inflammation
TREATMENT
Treatment for cholecystitis usually involves a hospital stay to control the inflammation
Слайд 20TREATMENT
Gallbladder drainage. In some cases, such as when surgery to remove the gallbladder
TREATMENT
Gallbladder drainage. In some cases, such as when surgery to remove the gallbladder
 IG_lektsia1
IG_lektsia1 «Решение систем уравнений второй степени»
«Решение систем уравнений второй степени»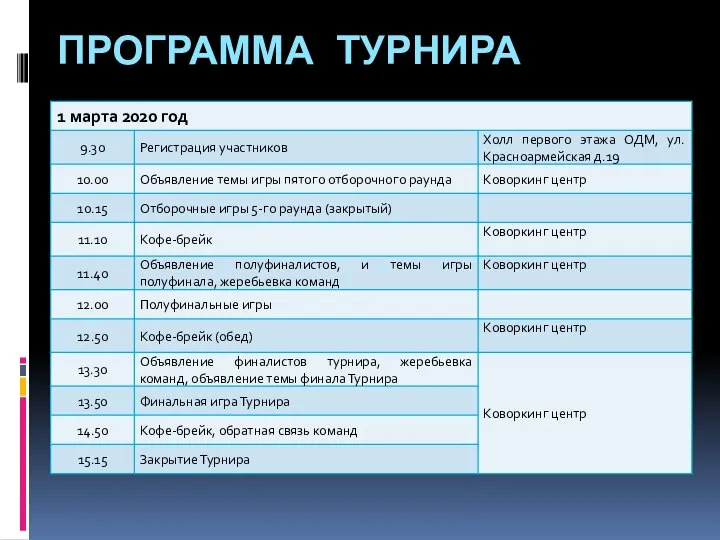 Программа турнира. Регистрация участников
Программа турнира. Регистрация участников Презентация на тему Хохлома
Презентация на тему Хохлома  Живая память
Живая память Стимулирование свободным временем
Стимулирование свободным временем Основные подходы к этиопатогенетической и симптомической терапии воспалительных заболеваний
Основные подходы к этиопатогенетической и симптомической терапии воспалительных заболеваний Как привлечь посетителей на сайт?
Как привлечь посетителей на сайт? Интерактивные технологии- как средство развития познавательных способностей младших школьников
Интерактивные технологии- как средство развития познавательных способностей младших школьников Когда формат важен. Новые формы событий в вузовской среде
Когда формат важен. Новые формы событий в вузовской среде Цветоведение
Цветоведение Штабные Учения
Штабные Учения Факультет прикладной математики и вычислительной техники (для абитуриентов)
Факультет прикладной математики и вычислительной техники (для абитуриентов) Предпосылки объединения русских земель. Усиление Московского княжества (§ 17)
Предпосылки объединения русских земель. Усиление Московского княжества (§ 17) Фьючерсные контракты
Фьючерсные контракты  Решение задач оптимизации, консолидации и масштабируемости Корпоративных территориально-распределенных сетей и приложений
Решение задач оптимизации, консолидации и масштабируемости Корпоративных территориально-распределенных сетей и приложений Причины сбоя работы ЭВМ
Причины сбоя работы ЭВМ Виды разборов по русскому языку
Виды разборов по русскому языку Representation of Functionns as Power Series
Representation of Functionns as Power Series Пациент и медицинский работник
Пациент и медицинский работник Профессиональное обучение (очная форма)
Профессиональное обучение (очная форма) Бизнес-план проекта “Маскарад мафии”
Бизнес-план проекта “Маскарад мафии” ПРИВИВКИ: КТО ПРОТИВ?
ПРИВИВКИ: КТО ПРОТИВ? Учет наличных денежных средств в кассе экваринг
Учет наличных денежных средств в кассе экваринг В лагерь с дневным пребыванием путёвки (от 6,6 лет до 17 лет) предоставляются
В лагерь с дневным пребыванием путёвки (от 6,6 лет до 17 лет) предоставляются Наставничество как условие организации работы студентов в малых учебных фирмах
Наставничество как условие организации работы студентов в малых учебных фирмах Orifleym. Менеджер 9%
Orifleym. Менеджер 9% Книга - главный герой или главная деталь произведения
Книга - главный герой или главная деталь произведения