- Physiological Changes in Pregnancy

Содержание
- 2. Introductory Comments This lecture/presentation is a “work in progress” Not possible to cover “all” the changes
- 3. Physiological Adaptations to Pregnancy Numerous normal changes in response to pregnancy It is important to have
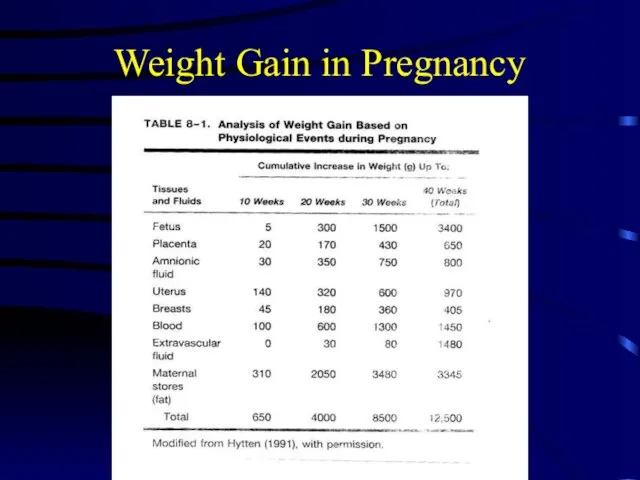
- 4. Weight Gain in Pregnancy Normal weight gain can be 30-35 lbs in average patient and 50-70
- 5. Weight Gain in Pregnancy
- 6. Weight Gain in Pregnancy
- 7. Breast Changes Increased blood flow to breasts Increased size Increased ductal growth, alveolar enlargement Colustrum production
- 8. Musculoskeletal Changes in Pregnancy Ligament laxity throughout Progressively more bothersome backpain not uncommon “Pride of pregnancy”
- 9. Skin Changes Vascular spiders Palmar erythema Striae gravidarum Hyperpigmentation effects Linea nigra Mask of pregnancy Increased
- 10. Gastrointestinal Changes Key Changes Appetite Usually increased, with cravings Gastric Reflux Sphincter relaxation GI Motility Decreased
- 11. Common GI Changes in Pregnancy Nausea and vomiting of pregnancy or “morning sickness” Exact etiology is
- 12. Physiological GI Changes. The hormonal effects on the gastrointestinal tract are an issue of debate among
- 13. Physiological GI Changes Recent studies, however, have shed a different light on the subject. Measuring peak
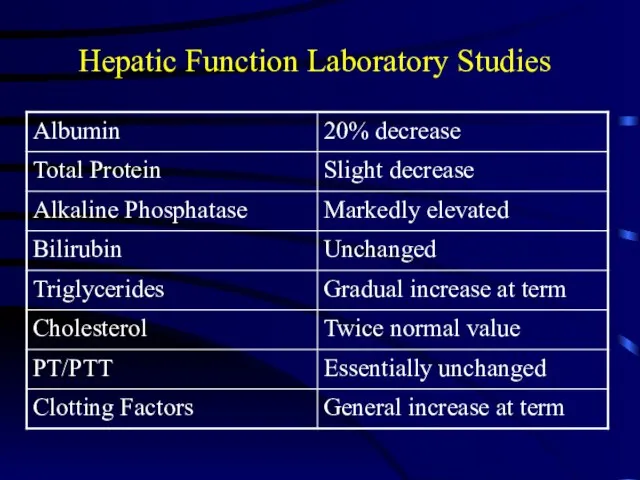
- 14. Hepatic Function Laboratory Studies
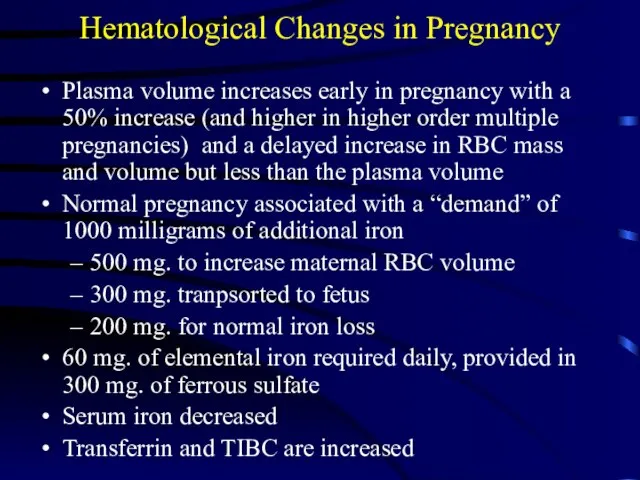
- 15. Hematological Changes in Pregnancy Plasma volume increases early in pregnancy with a 50% increase (and higher
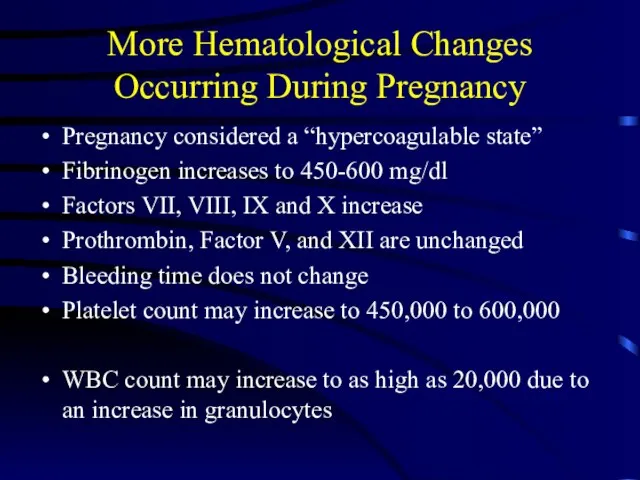
- 16. More Hematological Changes Occurring During Pregnancy Pregnancy considered a “hypercoagulable state” Fibrinogen increases to 450-600 mg/dl
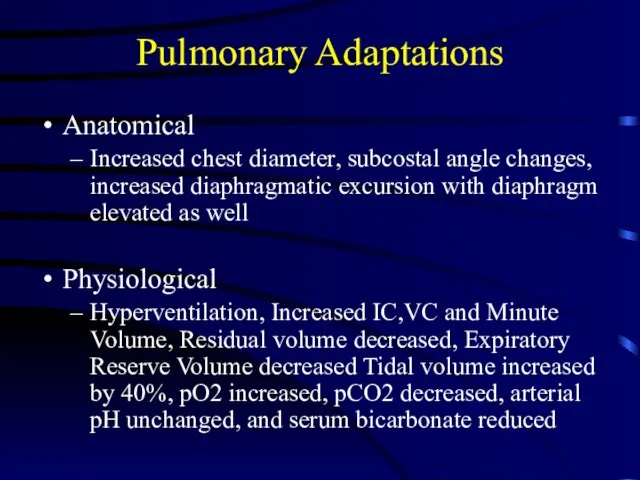
- 17. Pulmonary Adaptations Anatomical Increased chest diameter, subcostal angle changes, increased diaphragmatic excursion with diaphragm elevated as
- 18. Ventilation and Respiratory Gases. A progressive increase in minute ventilation starts soon after conception and peaks
- 19. Ventilation and Respiratory Gases. Arterial and alveolar carbon dioxide tensions are decreased by the increased ventilation.
- 20. Ventilation and Respiratory Gases Oxygen consumption increases gradually in response to the needs of the growing
- 21. Cardiac Changes in Pregnancy Cardiac output increases around 50% from an increase in HR and SV
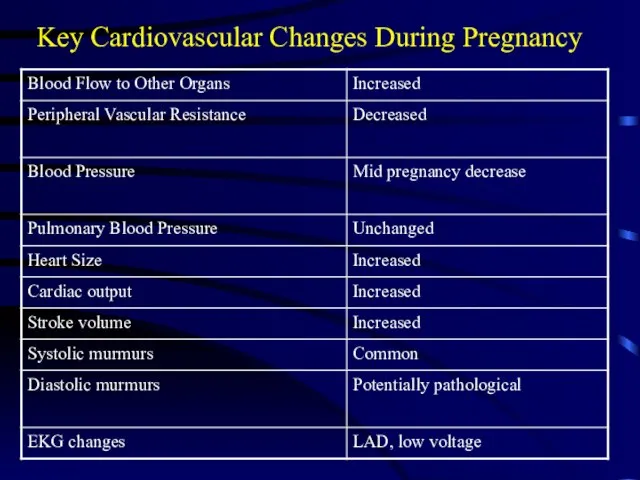
- 22. Key Cardiovascular Changes During Pregnancy
- 23. Blood Volume Blood Volume increases progressively from 6-8 weeks gestation (pregnancy) and reaches a maximum at
- 24. Blood Volume The increased blood volume serves two purposes. First, it facilitates maternal and fetal exchanges
- 25. Blood Constituents. As mentioned above, red cell mass is increased 20-30%. Leukocyte counts are variable during
- 26. Cardiac Output Cardiac Output increases to a similar degree as the blood volume. During the first
- 27. Cardiac Output During labor, further increases are seen with pain in response to increased catecholamine secretion;
- 28. Cardiac Size/Position/ECG. There are both size and position changes which can lead to changes in ECG
- 29. Blood Pressure . Systemic arterial pressure is never increased during normal gestation. In fact, by midpregnancy,
- 30. Renal Changes in Pregnancy Minimal renal enlargement, bilaterally Both renal pelvises and ureters are dilated (“hydronephrosis
- 31. More Renal Changes in Pregnancy GFR increases 50% over on-pregnant state Creatinine clearance increases to 150-200
- 32. Endocrine Changes with Pregnancy Carbohydrate Metabolism Overall effect is that pregnancy is diabetogenic First half: tendency
- 33. Metabolism All metabolic functions are increased during pregnancy to provide for the demands of fetus, placenta
- 34. Metabolism Carbohydrate metabolism, however, demonstrates the most dramatic changes. Metabolically speaking, pregnant women live in a
- 35. Hypoglycaemia. Optimal blood glucose levels in pregnant women range between 4.4 to 5.5 mmol/1. In healthy
- 36. Hypoglycaemia. Hypoglycaemia initiates the release of glucagon, cortisol and, importantly, catecholamines. In the anaesthetised state, however,
- 37. Endocrine Changes in Pregnancy Thyroid Function in Pregnancy The normal pregnant woman remains euthyroid while pregnant
- 38. Endocrine Changes in Pregnancy GnRH concentration increases during pregnancy, but the physiological significance of this change
- 39. Endocrinology Changes in Pregnancy
- 40. Endocrine Changes in Pregnancy The placenta produces a hormone (similar to thyroid-stimulating hormone) that stimulates the
- 41. Endocrine Changes in Pregnancy The placenta produces corticotropin-releasing hormone (CRH), which stimulates maternal ACTH production. Increased
- 42. Endocrine Changes in Pregnancy The placenta produces melanocyte-stimulating hormone (MSH), which increases skin pigmentation late in
- 43. Endocrine Changes in Pregnancy Effects of thyroid hormone tend to increase and may resemble hyperthyroidism, with
- 45. Скачать презентацию
Слайд 2Introductory Comments
This lecture/presentation is a “work in progress”
Not possible to cover “all”
Introductory Comments
This lecture/presentation is a “work in progress”
Not possible to cover “all”
Слайд 3Physiological Adaptations to Pregnancy
Numerous normal changes in response to pregnancy
It is important
Physiological Adaptations to Pregnancy
Numerous normal changes in response to pregnancy
It is important
Слайд 4Weight Gain in Pregnancy
Normal weight gain can be 30-35 lbs in average
Weight Gain in Pregnancy
Normal weight gain can be 30-35 lbs in average
Слайд 5Weight Gain in Pregnancy
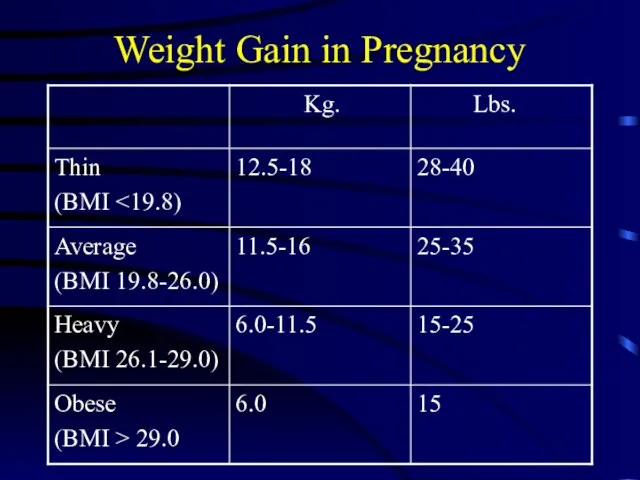
Weight Gain in Pregnancy
Слайд 6Weight Gain in Pregnancy
Weight Gain in Pregnancy
Слайд 7Breast Changes
Increased blood flow to breasts
Increased size
Increased ductal growth, alveolar enlargement
Colustrum production
Lactation
Breast Changes
Increased blood flow to breasts
Increased size
Increased ductal growth, alveolar enlargement
Colustrum production
Lactation
Слайд 8Musculoskeletal Changes in Pregnancy
Ligament laxity throughout
Progressively more bothersome backpain not uncommon
“Pride of
Musculoskeletal Changes in Pregnancy
Ligament laxity throughout
Progressively more bothersome backpain not uncommon
“Pride of
Слайд 9Skin Changes
Vascular spiders
Palmar erythema
Striae gravidarum
Hyperpigmentation effects
Linea nigra
Mask of pregnancy
Increased fine hair growth
Skin Changes
Vascular spiders
Palmar erythema
Striae gravidarum
Hyperpigmentation effects
Linea nigra
Mask of pregnancy
Increased fine hair growth
Слайд 10 Gastrointestinal Changes
Key Changes
Appetite Usually increased, with cravings
Gastric Reflux Sphincter relaxation
GI
Gastrointestinal Changes
Key Changes
Appetite Usually increased, with cravings
Gastric Reflux Sphincter relaxation
GI
Слайд 11Common GI Changes in Pregnancy
Nausea and vomiting of pregnancy or “morning sickness”
Exact
Common GI Changes in Pregnancy
Nausea and vomiting of pregnancy or “morning sickness”
Exact
Слайд 12Physiological GI Changes.
The hormonal effects on the gastrointestinal tract are an issue
Physiological GI Changes.
The hormonal effects on the gastrointestinal tract are an issue
Слайд 13Physiological GI Changes
Recent studies, however, have shed a different light on the
Physiological GI Changes
Recent studies, however, have shed a different light on the
Слайд 14Hepatic Function Laboratory Studies
Hepatic Function Laboratory Studies
Слайд 15Hematological Changes in Pregnancy
Plasma volume increases early in pregnancy with a 50%
Hematological Changes in Pregnancy
Plasma volume increases early in pregnancy with a 50%
Слайд 16More Hematological Changes Occurring During Pregnancy
Pregnancy considered a “hypercoagulable state”
Fibrinogen increases to
More Hematological Changes Occurring During Pregnancy
Pregnancy considered a “hypercoagulable state”
Fibrinogen increases to
Слайд 17Pulmonary Adaptations
Anatomical
Increased chest diameter, subcostal angle changes, increased diaphragmatic excursion with diaphragm
Pulmonary Adaptations
Anatomical
Increased chest diameter, subcostal angle changes, increased diaphragmatic excursion with diaphragm
Слайд 18Ventilation and Respiratory Gases.
A progressive increase in minute ventilation starts soon after
Ventilation and Respiratory Gases.
A progressive increase in minute ventilation starts soon after
Слайд 19Ventilation and Respiratory Gases.
Arterial and alveolar carbon dioxide tensions are decreased by
Ventilation and Respiratory Gases.
Arterial and alveolar carbon dioxide tensions are decreased by
Слайд 20Ventilation and Respiratory Gases
Oxygen consumption increases gradually in response to the needs
Ventilation and Respiratory Gases
Oxygen consumption increases gradually in response to the needs
Слайд 21Cardiac Changes in Pregnancy
Cardiac output increases around 50% from an increase in
Cardiac Changes in Pregnancy
Cardiac output increases around 50% from an increase in
Слайд 22Key Cardiovascular Changes During Pregnancy
Key Cardiovascular Changes During Pregnancy
Слайд 23Blood Volume
Blood Volume increases progressively from 6-8 weeks gestation (pregnancy) and reaches
Blood Volume
Blood Volume increases progressively from 6-8 weeks gestation (pregnancy) and reaches
Слайд 24Blood Volume
The increased blood volume serves two purposes. First, it facilitates maternal
Blood Volume
The increased blood volume serves two purposes. First, it facilitates maternal
Слайд 25Blood Constituents.
As mentioned above, red cell mass is increased 20-30%. Leukocyte counts
Blood Constituents.
As mentioned above, red cell mass is increased 20-30%. Leukocyte counts
Слайд 26Cardiac Output
Cardiac Output increases to a similar degree as the blood volume.
Cardiac Output
Cardiac Output increases to a similar degree as the blood volume.
Слайд 27Cardiac Output
During labor, further increases are seen with pain in response to
Cardiac Output
During labor, further increases are seen with pain in response to
Слайд 28Cardiac Size/Position/ECG.
There are both size and position changes which can lead to
Cardiac Size/Position/ECG.
There are both size and position changes which can lead to
Слайд 29Blood Pressure
. Systemic arterial pressure is never increased during normal gestation. In
Blood Pressure
. Systemic arterial pressure is never increased during normal gestation. In
Слайд 30Renal Changes in Pregnancy
Minimal renal enlargement, bilaterally
Both renal pelvises and ureters are
Renal Changes in Pregnancy
Minimal renal enlargement, bilaterally
Both renal pelvises and ureters are
Слайд 31More Renal Changes in Pregnancy
GFR increases 50% over on-pregnant state
Creatinine clearance increases
More Renal Changes in Pregnancy
GFR increases 50% over on-pregnant state
Creatinine clearance increases
Слайд 32Endocrine Changes with Pregnancy
Carbohydrate Metabolism
Overall effect is that pregnancy is diabetogenic
First half:
Endocrine Changes with Pregnancy
Carbohydrate Metabolism
Overall effect is that pregnancy is diabetogenic
First half:
Слайд 33Metabolism
All metabolic functions are increased during pregnancy to provide for the demands
Metabolism
All metabolic functions are increased during pregnancy to provide for the demands
Слайд 34Metabolism
Carbohydrate metabolism, however, demonstrates the most dramatic changes. Metabolically speaking, pregnant women
Metabolism
Carbohydrate metabolism, however, demonstrates the most dramatic changes. Metabolically speaking, pregnant women
Слайд 35Hypoglycaemia.
Optimal blood glucose levels in pregnant women range between 4.4 to 5.5 mmol/1.
Hypoglycaemia.
Optimal blood glucose levels in pregnant women range between 4.4 to 5.5 mmol/1.
Слайд 36Hypoglycaemia.
Hypoglycaemia initiates the release of glucagon, cortisol and, importantly, catecholamines. In the
Hypoglycaemia.
Hypoglycaemia initiates the release of glucagon, cortisol and, importantly, catecholamines. In the
Слайд 37Endocrine Changes in Pregnancy
Thyroid Function in Pregnancy
The normal pregnant woman remains
Endocrine Changes in Pregnancy
Thyroid Function in Pregnancy
The normal pregnant woman remains
Слайд 38 Endocrine Changes in Pregnancy
GnRH concentration increases during pregnancy, but the physiological
Endocrine Changes in Pregnancy
GnRH concentration increases during pregnancy, but the physiological
Слайд 39Endocrinology Changes in Pregnancy
Endocrinology Changes in Pregnancy
Слайд 40Endocrine Changes in Pregnancy
The placenta produces a hormone (similar to thyroid-stimulating hormone)
Endocrine Changes in Pregnancy
The placenta produces a hormone (similar to thyroid-stimulating hormone)
Слайд 41Endocrine Changes in Pregnancy
The placenta produces corticotropin-releasing hormone (CRH), which stimulates maternal
Endocrine Changes in Pregnancy
The placenta produces corticotropin-releasing hormone (CRH), which stimulates maternal
Слайд 42Endocrine Changes in Pregnancy
The placenta produces melanocyte-stimulating hormone (MSH), which increases skin
Endocrine Changes in Pregnancy
The placenta produces melanocyte-stimulating hormone (MSH), which increases skin
Слайд 43Endocrine Changes in Pregnancy
Effects of thyroid hormone tend to increase and may
Endocrine Changes in Pregnancy
Effects of thyroid hormone tend to increase and may
 Выбор поставщика для регулярных поставок керамогранита в открываемын магазины Zolla в СФО и ближайших регионах
Выбор поставщика для регулярных поставок керамогранита в открываемын магазины Zolla в СФО и ближайших регионах Глаголы 3 группы
Глаголы 3 группы Презентация на тему ПРЕИМУЩЕСТВА И НЕДОСТАТКИ РЫНОЧНОЙ ЭКОНОМИКИ
Презентация на тему ПРЕИМУЩЕСТВА И НЕДОСТАТКИ РЫНОЧНОЙ ЭКОНОМИКИ  Интернет-Центр «Cafemax» Пятницкая
Интернет-Центр «Cafemax» Пятницкая Активность участников рынка в продвижении лекарственных средств: Основные тенденции и перспективы развития
Активность участников рынка в продвижении лекарственных средств: Основные тенденции и перспективы развития Финансовое обеспечение инвестиций в РБ
Финансовое обеспечение инвестиций в РБ Минералы. Сокровища Земли
Минералы. Сокровища Земли Реформы_в_сфере_образования_в_Республике_Узбекистан
Реформы_в_сфере_образования_в_Республике_Узбекистан Раскрась флажки красным цветом. После этого измени только:
Раскрась флажки красным цветом. После этого измени только: Ароматизаторы
Ароматизаторы Загадки о полезных ископаемых
Загадки о полезных ископаемых Условный алгоритм
Условный алгоритм Михаил Евграфович Салтыков-Щедрин
Михаил Евграфович Салтыков-Щедрин Что это такое?
Что это такое? Презентация на тему Автотуризм
Презентация на тему Автотуризм Выборочное изложение по тексту Е.В. Мурашовой
Выборочное изложение по тексту Е.В. Мурашовой Презентация на тему Венеция
Презентация на тему Венеция  Метод контроля качества сварных соединений полимерно-армированных труб (ПАТ)
Метод контроля качества сварных соединений полимерно-армированных труб (ПАТ) Грани личности
Грани личности Дизайнер в отечественном ИТ бизнесе: многообразие деятельности, недооцененные компоненты профессионализма, стратегия роста Сер
Дизайнер в отечественном ИТ бизнесе: многообразие деятельности, недооцененные компоненты профессионализма, стратегия роста Сер ВРОЖДЕННЫЕ ПОРОКИ СЕРДЦА ДонГМУ, кафедра госпитальной хирургии им. В.М. Богославского
ВРОЖДЕННЫЕ ПОРОКИ СЕРДЦА ДонГМУ, кафедра госпитальной хирургии им. В.М. Богославского Эффективность деятельности фирмы
Эффективность деятельности фирмы  Покажи красный цвет
Покажи красный цвет Юлия Друнина: Я родом не из детства – Нет, это не заслуга, а удача — из войны
Юлия Друнина: Я родом не из детства – Нет, это не заслуга, а удача — из войны Презентация на тему Хеллоуин
Презентация на тему Хеллоуин  А. С. Пушкин «Эхо»
А. С. Пушкин «Эхо» Фёдор Иванович Тютчев (1803г.-1873г.)
Фёдор Иванович Тютчев (1803г.-1873г.) Конституционное право – ведущая отрасль права Беларуси
Конституционное право – ведущая отрасль права Беларуси