- Pulmonary tuberculosis

Содержание
- 2. Pulmonary Tuberculosis Tuberculosis (abbreviated as TB for tubercle bacillus or Tuberculosis) is a common and often
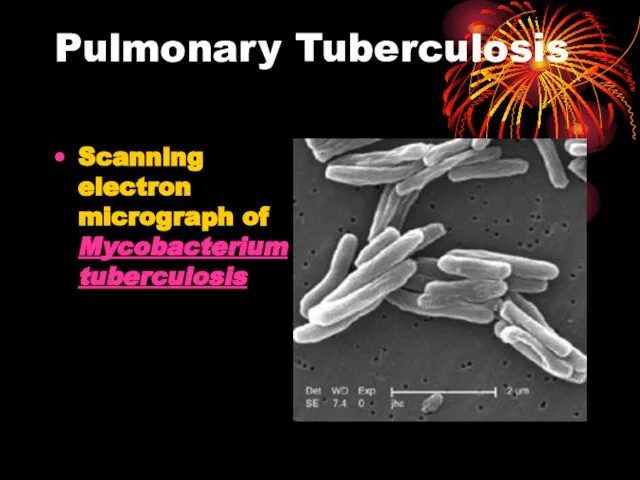
- 3. Pulmonary Tuberculosis Scanning electron micrograph of Mycobacterium tuberculosis
- 4. Epidemiology According to the World Health Organization (WHO), nearly 2 billion people—one third of the world's
- 5. Epidemiology Most common infectious cause of death worldwide Latent phase of TB enabled it to spread
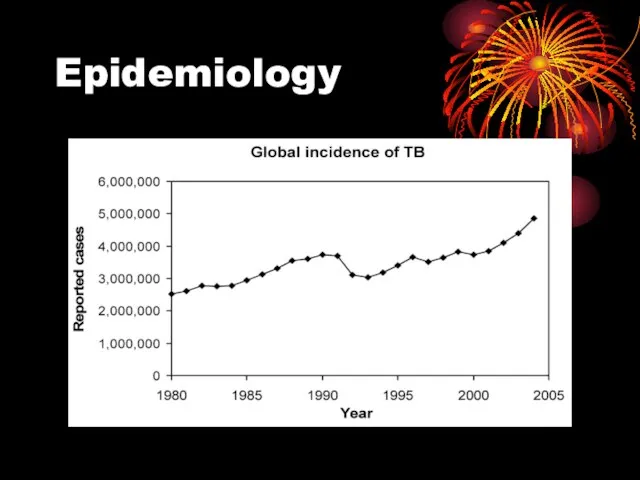
- 6. Epidemiology
- 7. Epidemiology Major changes in trends secondary to HIV - 1953-1985 cases decreased from 84,304 to 22,201
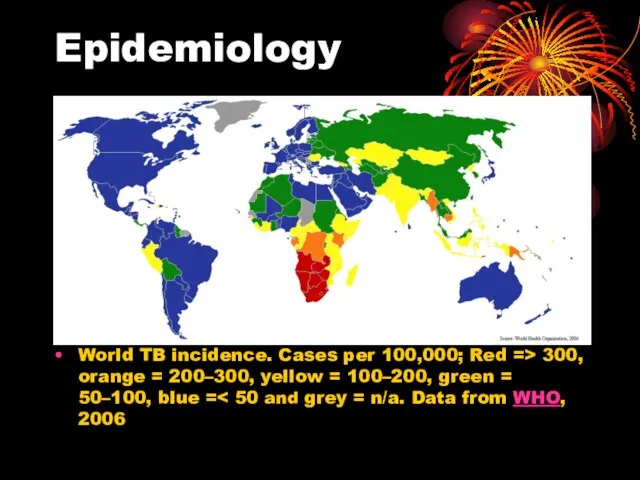
- 8. Epidemiology World TB incidence. Cases per 100,000; Red => 300, orange = 200–300, yellow = 100–200,
- 9. Incidence 1985-1990 TB cases increased 55% in Hispanics and 27% in African Americans Populations at risk
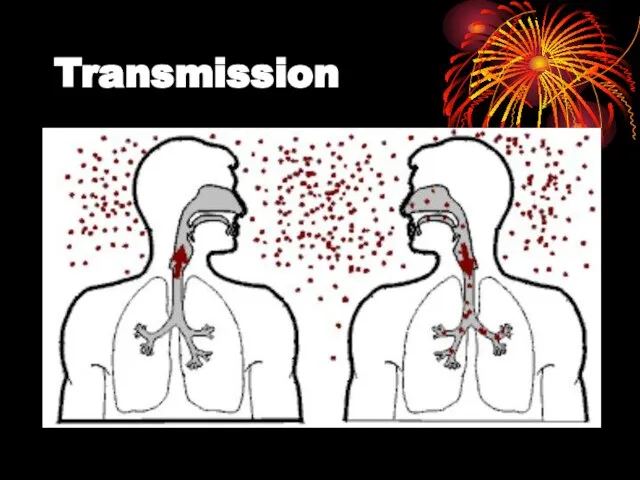
- 10. Transmission When people suffering from active pulmonary TB cough, sneeze, speak, or spit, they expel infectious
- 11. Transmission
- 12. Transmission people who inject drugs using unsanitary needles, residents and employees of high-risk congregate settings, medically
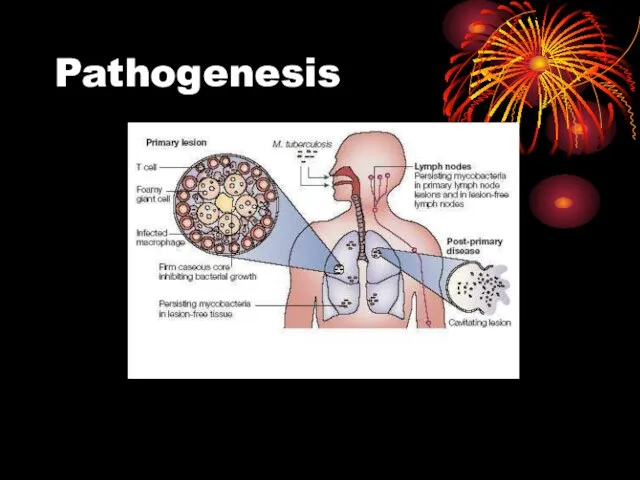
- 13. Pathogenesis
- 14. Pathogenesis Hyperlink to Microsoft Word Pathophysiology of Pulmonary Tuberculosis.doc Pathogenesis of TB infection and disease.doc
- 15. Diagnostics Inject intradermally 0.1 ml of 5TU PPD tuberculin Produce wheal 6 mm to 10 mm
- 16. Reading of Mantoux test Read reaction 48-72 hours after injection Measure only induration Record reaction in
- 17. Classifying the Tuberculin Reaction >5 mm is classified as positive in HIV-positive persons Recent contacts of
- 18. Classifying the tuberculin reaction >10 mm is classified as positive in Recent arrivals from high-prevalence countries
- 19. Classifying the tuberculin reaction >15 mm is classified as positive in Persons with no known risk
- 20. Factors may affect TST False negative Faulty application Anergy Acute TB (2-10 wks to convert) Very
- 21. Chest Radiography Abnormalities often seen in apical or posterior segments of upper lobe or superior segments
- 22. Chest radiography No chest X-ray pattern is absolutely typical of TB 10-15% of culture-positive TB patients
- 23. Specimen Collection Obtain 3 sputum specimens for smear examination and culture Persons unable to cough up
- 24. Number of sputum samples required overall diagnostic yield for sputum examination related to the quantity of
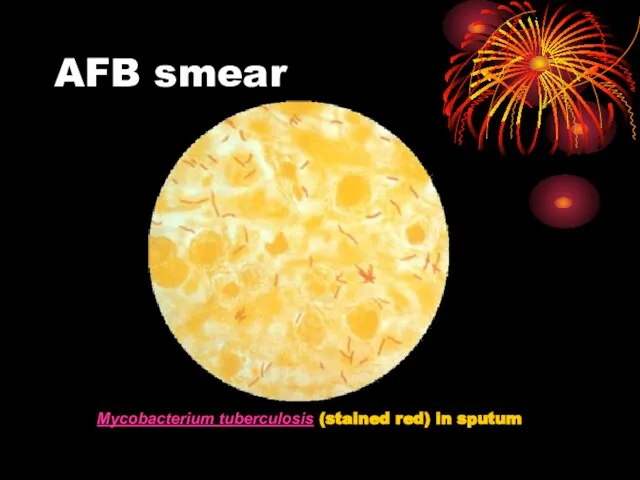
- 25. Smear Examination Strongly consider TB in patients with smears containing acid-fast bacilli (AFB) Results should be
- 26. AFB smear Mycobacterium tuberculosis (stained red) in sputum
- 27. Cultures
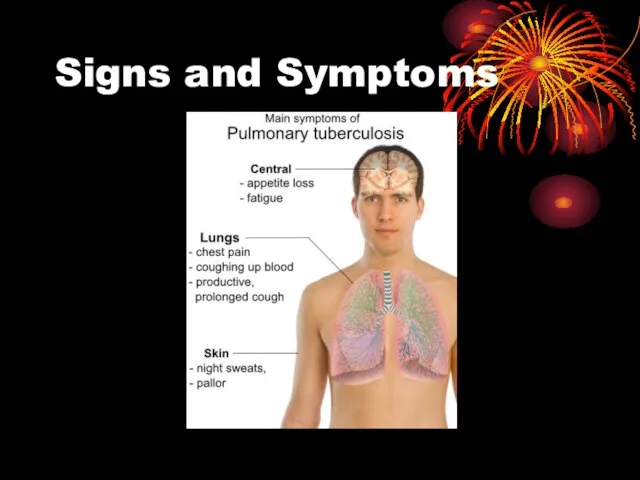
- 28. Signs and Symptoms
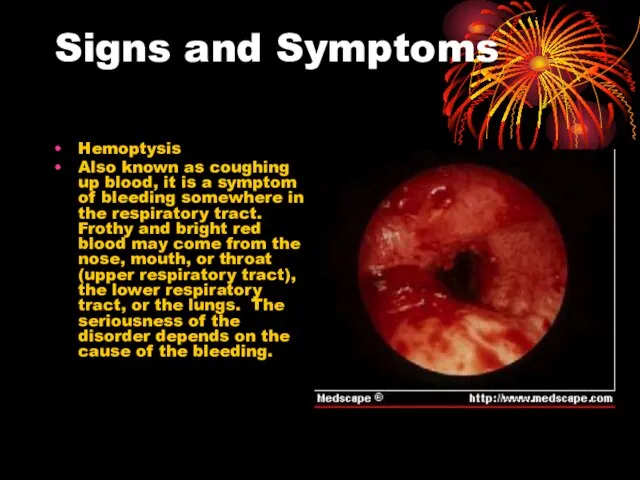
- 29. Signs and Symptoms Hemoptysis Also known as coughing up blood, it is a symptom of bleeding
- 30. Signs and Symptoms Anorexia The sysmptom of poor appetite whatever the cause
- 31. Treatment
- 32. Tuberculosis treatment The standard "short" course treatment for tuberculosis (TB), is isoniazid (TB), is isoniazid, rifampicin
- 33. Drugs All first-line anti-tuberculous drug names have a standard three-letter and a single-letter abbreviation: ethambutol is
- 34. Drugs There are six classes of second-line drugs (SLDs) used for the treatment of TB. A
- 35. Drugs considered "third-line drugs" not very effective or because their efficacy has not been proven .
- 36. Drugs Daily Dose of TB Drugs
- 37. Drugs Multi-drug resistant TB (MDR-TB) is defined as resistance to the two most effective first-line TB
- 38. Monitoring and DOTS DOTSDOTS stands for "Directly Observed Therapy, Short-course" and is a major plan in
- 39. Prevention TB prevention and control takes two parallel approaches. In the first, people with TB and
- 40. Vaccines Many countries use Bacillus Calmette-Guérin (BCG) vaccine as part of their TB control programs, especially
- 41. Current Surgical Intervention Patients with hemoptysis first received Bronchial Artery Embolization because of the recurrent hemoptysis.
- 43. Скачать презентацию
Слайд 2Pulmonary Tuberculosis
Tuberculosis (abbreviated as TB for tubercle bacillus or Tuberculosis) is a
Pulmonary Tuberculosis
Tuberculosis (abbreviated as TB for tubercle bacillus or Tuberculosis) is a
Слайд 3Pulmonary Tuberculosis
Scanning electron micrograph of Mycobacterium tuberculosis
Pulmonary Tuberculosis
Scanning electron micrograph of Mycobacterium tuberculosis
Слайд 4Epidemiology
According to the World Health Organization (WHO), nearly 2 billion people—one third
Epidemiology
According to the World Health Organization (WHO), nearly 2 billion people—one third
Слайд 5Epidemiology
Most common infectious cause of death worldwide
Latent phase of TB enabled
Epidemiology
Most common infectious cause of death worldwide
Latent phase of TB enabled
Слайд 6Epidemiology
Epidemiology
Слайд 7Epidemiology
Major changes in trends secondary to HIV
- 1953-1985 cases decreased from 84,304
Epidemiology
Major changes in trends secondary to HIV
- 1953-1985 cases decreased from 84,304
Слайд 8Epidemiology
World TB incidence. Cases per 100,000; Red => 300, orange = 200–300,
Epidemiology
World TB incidence. Cases per 100,000; Red => 300, orange = 200–300,
Слайд 9Incidence
1985-1990 TB cases increased 55% in Hispanics and 27% in African Americans
Populations
Incidence
1985-1990 TB cases increased 55% in Hispanics and 27% in African Americans
Populations
Слайд 10Transmission
When people suffering from active pulmonary TB cough, sneeze, speak, or spit,
Transmission
When people suffering from active pulmonary TB cough, sneeze, speak, or spit,
Слайд 11Transmission
Transmission
Слайд 12Transmission
people who inject drugs using unsanitary needles,
residents and employees of high-risk
Transmission
people who inject drugs using unsanitary needles,
residents and employees of high-risk
Слайд 13Pathogenesis
Pathogenesis
Слайд 14Pathogenesis
Hyperlink to Microsoft Word
Pathophysiology of Pulmonary Tuberculosis.doc
Pathogenesis of TB infection and
Pathogenesis
Hyperlink to Microsoft Word
Pathophysiology of Pulmonary Tuberculosis.doc
Pathogenesis of TB infection and
Слайд 15Diagnostics
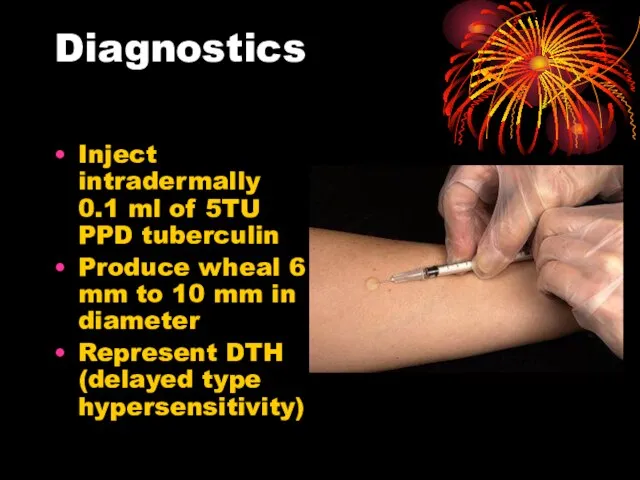
Inject intradermally 0.1 ml of 5TU PPD tuberculin
Produce wheal 6 mm to
Diagnostics
Inject intradermally 0.1 ml of 5TU PPD tuberculin
Produce wheal 6 mm to
Слайд 16Reading of Mantoux test
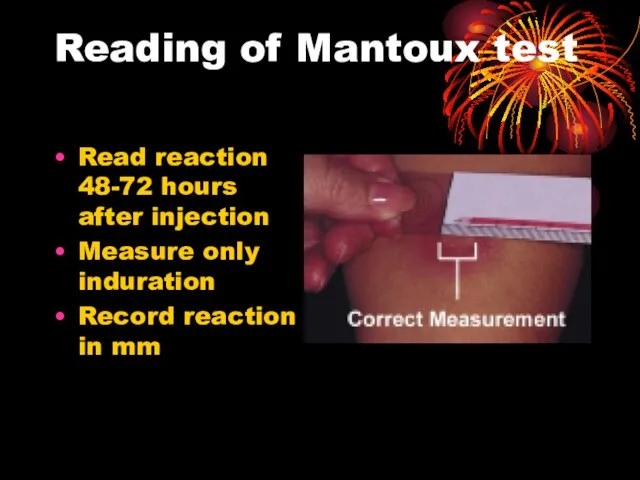
Read reaction 48-72 hours after injection
Measure only induration
Record reaction
Reading of Mantoux test
Read reaction 48-72 hours after injection
Measure only induration
Record reaction
Слайд 17Classifying the Tuberculin Reaction
>5 mm is classified as positive in
HIV-positive persons
Recent contacts
Classifying the Tuberculin Reaction
>5 mm is classified as positive in
HIV-positive persons
Recent contacts
Слайд 18Classifying the tuberculin reaction
>10 mm is classified as positive in
Recent arrivals from
Classifying the tuberculin reaction
>10 mm is classified as positive in
Recent arrivals from
Слайд 19Classifying the tuberculin reaction
>15 mm is classified as positive in
Persons with no
Classifying the tuberculin reaction
>15 mm is classified as positive in
Persons with no
Слайд 20Factors may affect TST
False negative
Faulty application
Anergy
Acute TB (2-10 wks to convert)
Very young
Factors may affect TST
False negative
Faulty application
Anergy
Acute TB (2-10 wks to convert)
Very young
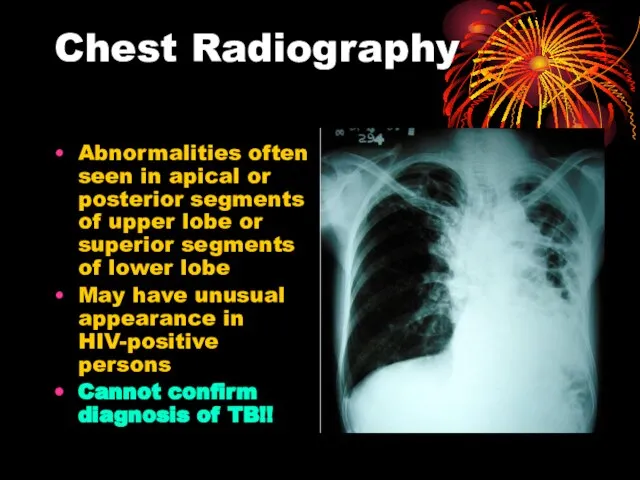
Слайд 21Chest Radiography
Abnormalities often seen in apical or posterior segments of upper lobe
Chest Radiography
Abnormalities often seen in apical or posterior segments of upper lobe
Слайд 22Chest radiography
No chest X-ray pattern is absolutely typical of TB
10-15% of culture-positive
Chest radiography
No chest X-ray pattern is absolutely typical of TB
10-15% of culture-positive
Слайд 23Specimen Collection
Obtain 3 sputum specimens for smear examination and culture
Persons unable to
Specimen Collection
Obtain 3 sputum specimens for smear examination and culture
Persons unable to
Слайд 24Number of sputum samples required
overall diagnostic yield for sputum examination related to
Number of sputum samples required
overall diagnostic yield for sputum examination related to
Слайд 25Smear Examination
Strongly consider TB in patients with smears containing acid-fast bacilli (AFB)
Results
Smear Examination
Strongly consider TB in patients with smears containing acid-fast bacilli (AFB)
Results
Слайд 26AFB smear
Mycobacterium tuberculosis (stained red) in sputum
AFB smear
Mycobacterium tuberculosis (stained red) in sputum
Слайд 27Cultures
Cultures

Слайд 28Signs and Symptoms
Signs and Symptoms
Слайд 29Signs and Symptoms
Hemoptysis
Also known as coughing up blood, it is a symptom
Signs and Symptoms
Hemoptysis
Also known as coughing up blood, it is a symptom
Слайд 30Signs and Symptoms
Anorexia
The sysmptom of poor appetite whatever the cause
Signs and Symptoms
Anorexia
The sysmptom of poor appetite whatever the cause
Слайд 31Treatment
Treatment

Слайд 32Tuberculosis treatment
The standard "short" course treatment for tuberculosis (TB), is isoniazid (TB),
Tuberculosis treatment
The standard "short" course treatment for tuberculosis (TB), is isoniazid (TB),
Слайд 33Drugs
All first-line anti-tuberculous drug names have a standard three-letter and a single-letter
Drugs
All first-line anti-tuberculous drug names have a standard three-letter and a single-letter
Слайд 34Drugs
There are six classes of second-line drugs (SLDs) used for the treatment
Drugs
There are six classes of second-line drugs (SLDs) used for the treatment
Слайд 35Drugs
considered "third-line drugs"
not very effective or because their efficacy has not
Drugs
considered "third-line drugs"
not very effective or because their efficacy has not
Слайд 36Drugs
Daily Dose of TB Drugs
Drugs
Daily Dose of TB Drugs

Слайд 37Drugs
Multi-drug resistant TB (MDR-TB) is defined as resistance to the two most
Drugs
Multi-drug resistant TB (MDR-TB) is defined as resistance to the two most
Слайд 38Monitoring and DOTS
DOTSDOTS stands for "Directly Observed Therapy, Short-course" and is a
Monitoring and DOTS
DOTSDOTS stands for "Directly Observed Therapy, Short-course" and is a
Слайд 39Prevention
TB prevention and control takes two parallel approaches.
In the first, people
Prevention
TB prevention and control takes two parallel approaches.
In the first, people

Слайд 40Vaccines
Many countries use Bacillus Calmette-Guérin (BCG) vaccine as part of their TB
Vaccines
Many countries use Bacillus Calmette-Guérin (BCG) vaccine as part of their TB
Слайд 41
Current Surgical Intervention
Patients with hemoptysis first received Bronchial Artery Embolization because
Current Surgical Intervention
Patients with hemoptysis first received Bronchial Artery Embolization because
 Political systems of the world and the Nenets autonomous okrug
Political systems of the world and the Nenets autonomous okrug АРЕНДА БЕТОНОНАСОСОВ
АРЕНДА БЕТОНОНАСОСОВ Презентация на тему В экваториальном лесу Южной Америки
Презентация на тему В экваториальном лесу Южной Америки Работа с бумагой
Работа с бумагой Большая китайская панда
Большая китайская панда Совещание с Дистрибьюторами г.Москва в рамках регионального совещания в г.Москва
Совещание с Дистрибьюторами г.Москва в рамках регионального совещания в г.Москва Крестики – нолики
Крестики – нолики Реконструкция Политехнического музея
Реконструкция Политехнического музея Блюдо из птицы
Блюдо из птицы Е.Л. Николаева Президент НАМИКС
Е.Л. Николаева Президент НАМИКС Казачество
Казачество 3. Types of Computer
3. Types of Computer Курс «Взаимодействие с заинтересованными сторонами и планирование деятельности в соответствии со стандартом AA1000 SES»
Курс «Взаимодействие с заинтересованными сторонами и планирование деятельности в соответствии со стандартом AA1000 SES» Эскиз
Эскиз «Оценивание программ и политик: методология и применение» - от межфакультетского семинара (2004-2005) к общегородскому коллоквиуму И
«Оценивание программ и политик: методология и применение» - от межфакультетского семинара (2004-2005) к общегородскому коллоквиуму И Мастер-класс Рисование пластилином картин
Мастер-класс Рисование пластилином картин Комплекс по сжижению, хранению и отгрузке СПГ в районе КС Портовая (Ленинградская область)
Комплекс по сжижению, хранению и отгрузке СПГ в районе КС Портовая (Ленинградская область) Новое похождения выпускников, или удивительное путешествие по океану знаний
Новое похождения выпускников, или удивительное путешествие по океану знаний Режимы электроэнергетических систем
Режимы электроэнергетических систем ратцель
ратцель Сравнительный анализ стандартов по географии 8-9 классы
Сравнительный анализ стандартов по географии 8-9 классы Зачем нам нужны растения?
Зачем нам нужны растения? Автоматическое повторное включение
Автоматическое повторное включение ИССЛЕДОВАНИЕ ТЕКСТОВ, ВЫПОЛНЕННЫХ «ПЕЧАТНЫМ» ПОЧЕРКОМ
ИССЛЕДОВАНИЕ ТЕКСТОВ, ВЫПОЛНЕННЫХ «ПЕЧАТНЫМ» ПОЧЕРКОМ МАОУ СОШ №91
МАОУ СОШ №91 Р-даы олданыстаы мырышты-орасынды байыту
Р-даы олданыстаы мырышты-орасынды байыту Детство без границ. Юбилею школы Горького посвящается
Детство без границ. Юбилею школы Горького посвящается Паремии
Паремии