- VALVULAR HEART DISEASE

Содержание
- 2. Overview Aortic Stenosis Mitral Stenosis Aortic Regurgitation Acute and Chronic Mitral Regurgitation Acute and Chronic
- 3. Etiology Pathophysiology Physical Exam Natural History Testing Treatment
- 4. Aortic Stenosis
- 6. Aortic Stenosis Overview: Normal Aortic Valve Area: 3-4 cm2 Symptoms: Occur when valve area is 1/4th
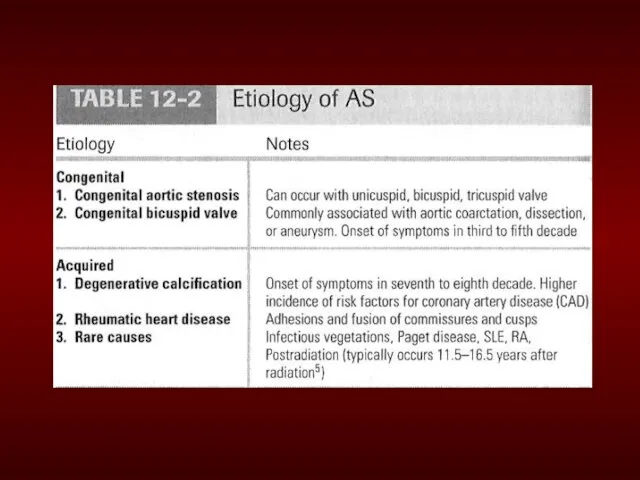
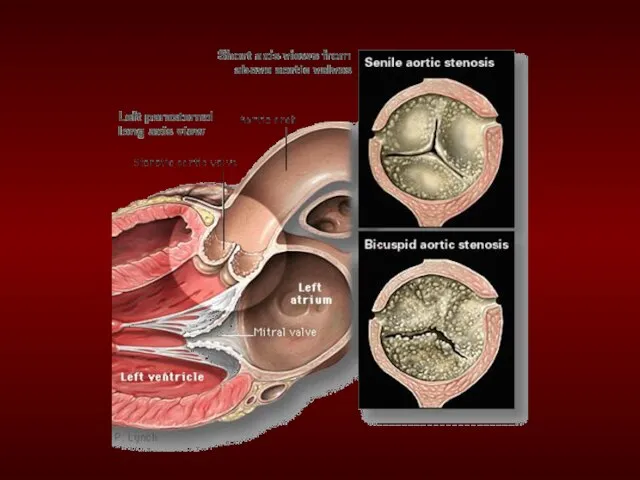
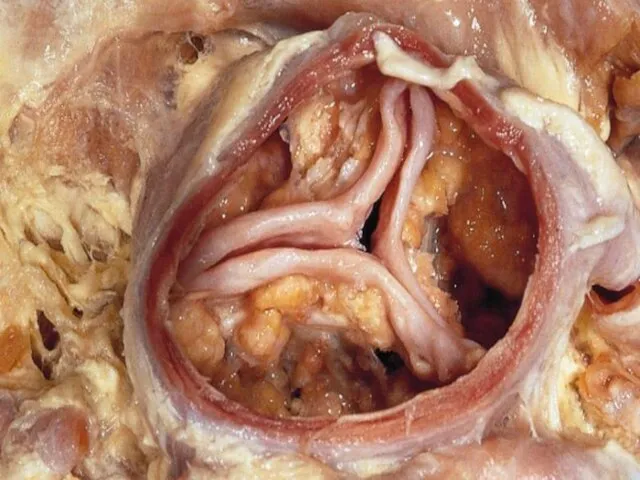
- 7. Etiology of Aortic Stenosis Congenital Rheumatic Degenerative/Calcific Patients under 70: >50% have a congenital cause Patients
- 12. Pathophysiology of Aortic Stenosis A pressure gradient develops between the left ventricle and the aorta. (increased
- 13. Presentation of Aortic Stenosis Syncope: (exertional) Angina: (increased myocardial oxygen demand; demand/supply mismatch) Dyspnea: on exertion
- 14. Physical Findings in Aortic Stenosis Slow rising carotid pulse (pulsus tardus) & decreased pulse amplitude (pulsus
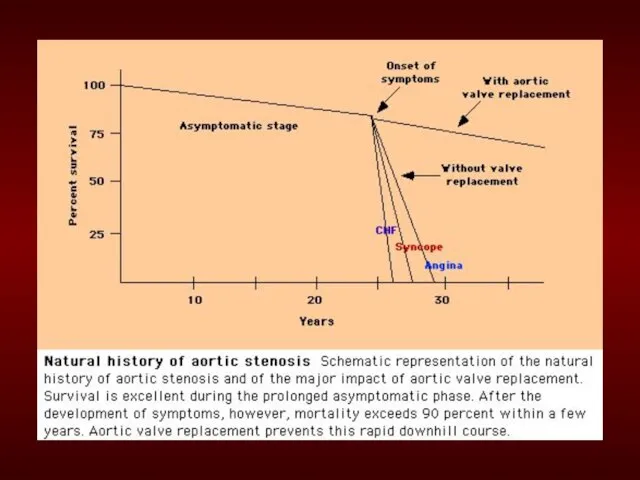
- 15. Natural History Mild AS to Severe AS: 8% in 10 years 22% in 22 years 38%
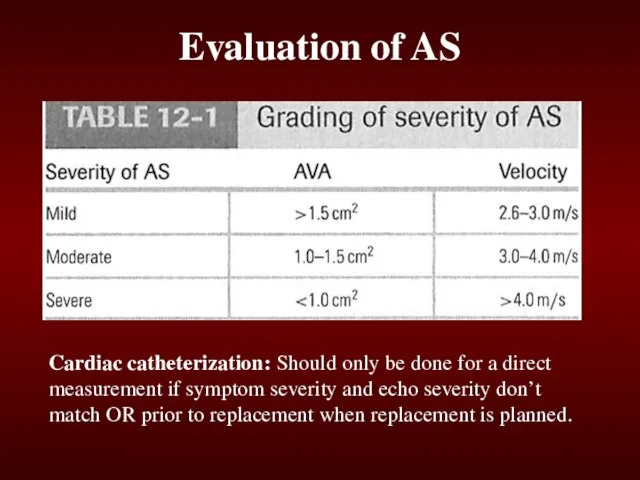
- 17. Evaluation of AS Echocardiography is the most valuable test for diagnosis, quantification and follow-up of patients
- 18. Evaluation of AS Cardiac catheterization: Should only be done for a direct measurement if symptom severity
- 19. Management of AS General- IE prophylaxis in dental procedures with a prosthetic AV or history of
- 20. Echo Surveillance Mild: Every 5 years Moderate: Every 2 years Severe: Every 6 months to 1
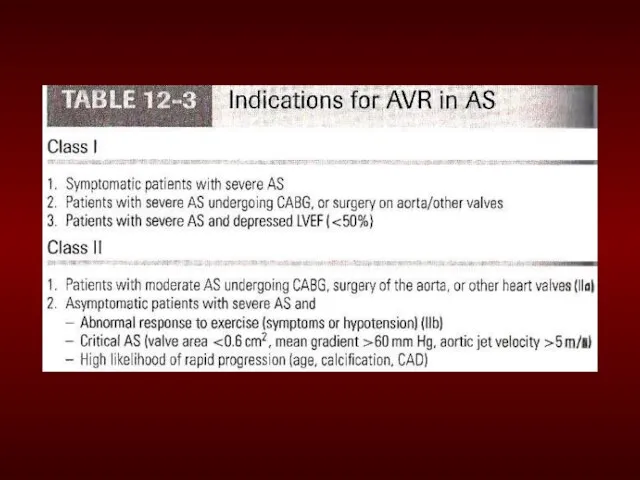
- 22. Simplified Indications for Surgery in Aortic Stenosis Any SYMPTOMATIC patient with severe AS (includes symptoms with
- 23. Summary Disease of aging Look for the signs on physical exam Echocardiogram to assess severity Asymptomatic:
- 24. Mitral Stenosis
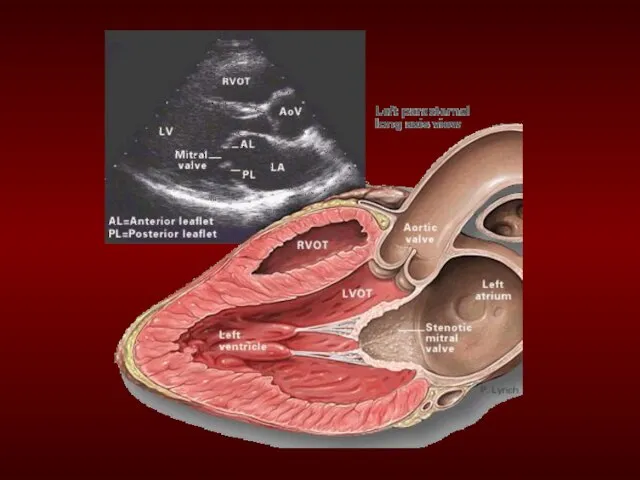
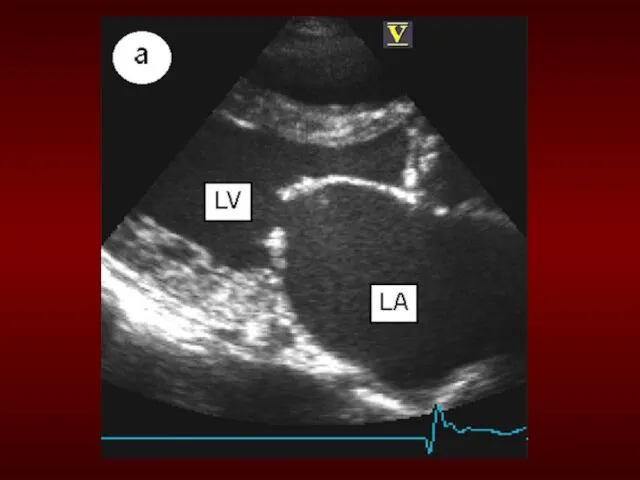
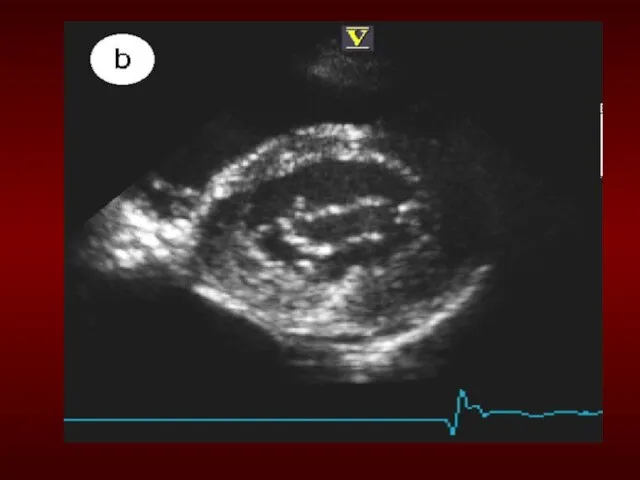
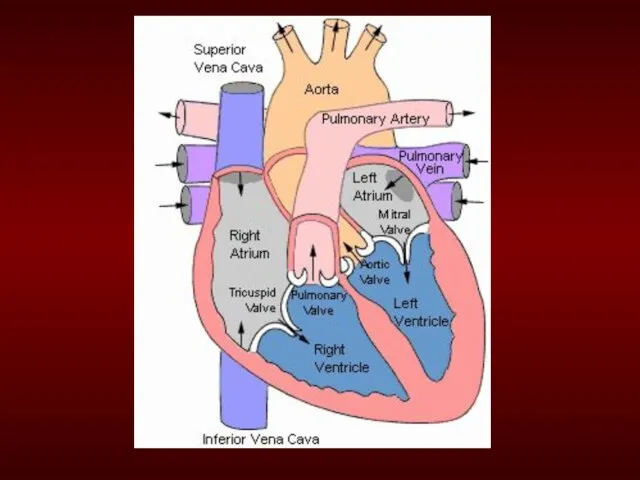
- 25. Mitral Stenosis Overview Definition: Obstruction of LV inflow that prevents proper filling during diastole Normal MV
- 26. Etiology of Mitral Stenosis Rheumatic heart disease: 77-99% of all cases Infective endocarditis: 3.3% Mitral annular
- 31. MS Pathophysiology Progressive Dyspnea (70%): LA dilation ? pulmonary congestion (reduced emptying) worse with exercise, fever,
- 32. Natural History of MS Disease of plateaus: Mild MS: 10 years after initial RHD insult Moderate:
- 33. Physical Exam Findings of MS prominent "a" wave in jugular venous pulsations: Due to pulmonary hypertension
- 34. Diastolic murmur: Low-pitched diastolic rumble most prominent at the apex. Heard best with the patient lying
- 35. Loud Opening S1 snap: heard at the apex when leaflets are still mobile Due to the
- 36. Evaluation of MS ECG: may show atrial fibrillation and LA enlargement CXR: LA enlargement and pulmonary
- 38. Management of MS Serial echocardiography: Mild: 3-5 years Moderate:1-2 years Severe: yearly Medications: MS like AS
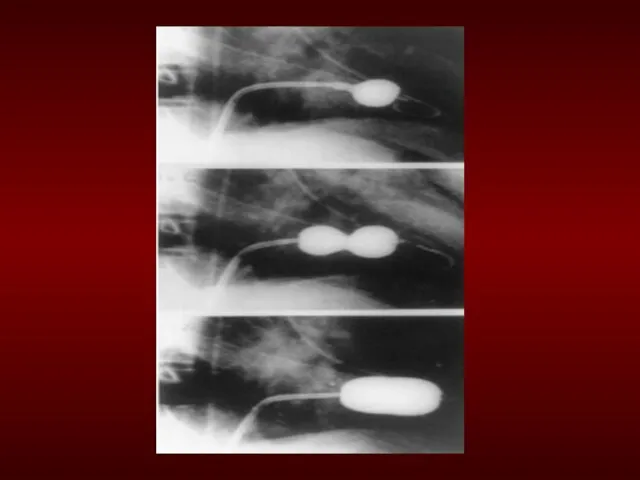
- 39. Management of MS Identify patient early who might benefit from percutaneous mitral balloon valvotomy. IE prophylaxis:
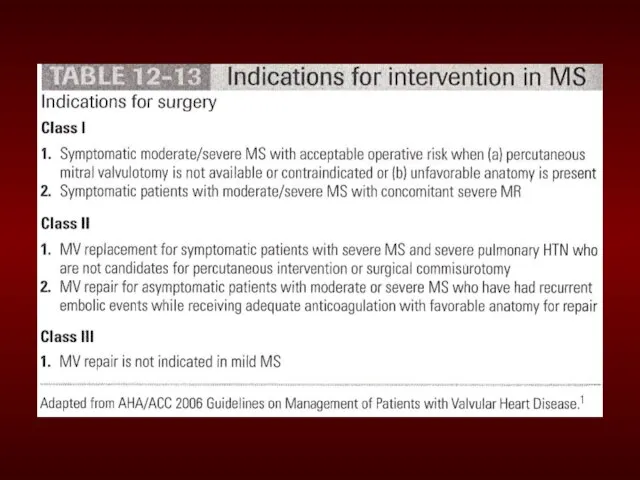
- 44. Simplified Indications for Mitral valve replacement ANY SYMPTOMATIC Patient with NYHA Class III or IV Symptoms
- 45. Aortic Regurgitation
- 47. Aortic Regurgitation Overview Definition: Leakage of blood into LV during diastole due to ineffective coaptation of
- 48. Etiology of Acute AR Endocarditis Aortic Dissection Physical Findings: Wide pulse pressure Diastolic murmur Florid pulmonary
- 49. Treatment of Acute AR True Surgical Emergency: Positive inotrope: (eg, dopamine, dobutamine) Vasodilators: (eg, nitroprusside) Avoid
- 51. Etiology of Chronic AR Bicuspid aortic valve Rheumatic Infective endocarditis
- 52. Pathophysiology of AR Combined pressure AND volume overload Compensatory Mechanisms: LV dilation, LVH. Progressive dilation leads
- 53. Natural History of AR Asymptomatic until 4th or 5th decade Rate of Progression: 4-6% per year
- 54. Physical Exam findings of AR Wide pulse pressure: most sensitive Hyperdynamic and displaced apical impulse Auscultation-
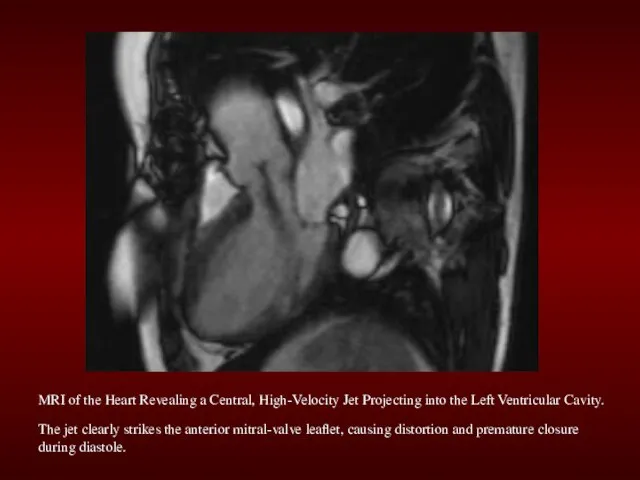
- 56. MRI of the Heart Revealing a Central, High-Velocity Jet Projecting into the Left Ventricular Cavity. The
- 57. The Evaluation of AR CXR: enlarged cardiac silhouette and aortic root enlargement ECHO: Evaluation of the
- 59. Management of AR General: IE prophylaxis in dental procedures with a prosthetic AV or history of
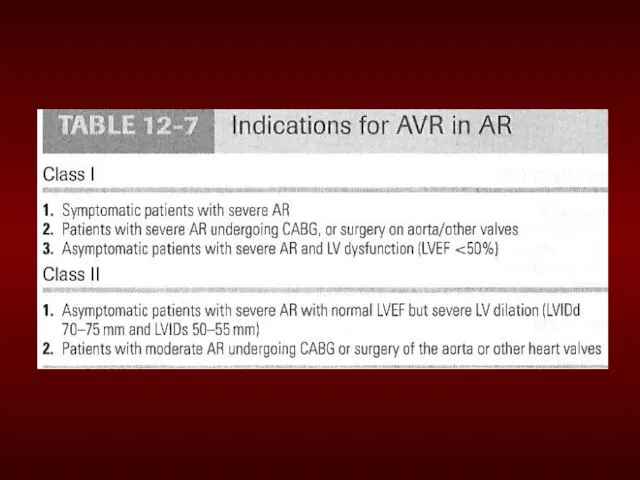
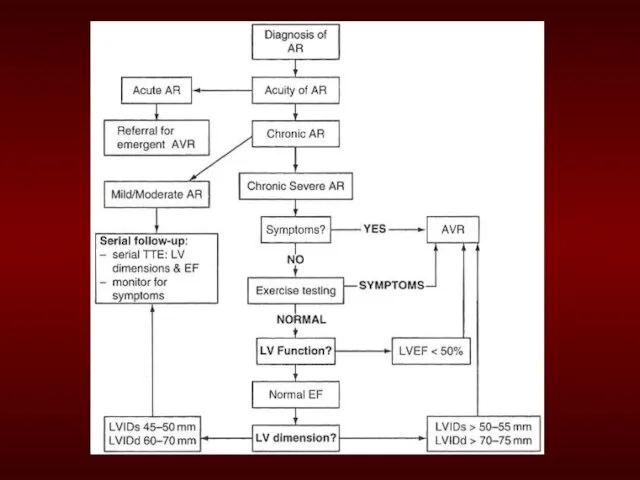
- 62. Simplified Indications for Surgical Treatment of AR ANY Symptoms at rest or exercise Asymptomatic treatment if:
- 63. Mitral Regurgitation
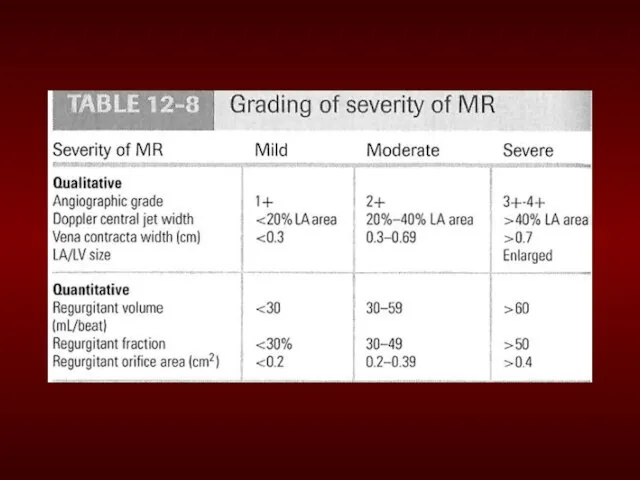
- 64. Definition: Backflow of blood from the LV to the LA during systole Mild (physiological) MR is
- 65. Acute MR Endocarditis Acute MI: Malfunction or disruption of prosthetic valve
- 66. Management of Acute MR Myocardial infarction: Cardiac cath or thrombolytics Most other cases of mitral regurgitation
- 67. Management of Acute MR Do not attempt to alleviate tachycardia with beta-blockers. Mild-to-moderate tachycardia is beneficial
- 68. Treatment of Acute MR Balloon Pump Nitroprusside even if hypotensive Emergent Surgery
- 69. Myxomatous degeneration (MVP) Ischemic MR Rheumatic heart disease Infective Endocarditis Etiologies of Chronic Mitral Regurgitation
- 70. Pathophysiology of MR Pure Volume Overload Compensatory Mechanisms: Left atrial enlargement, LVH and increased contractility Progressive
- 71. Physical Exam findings in MR Auscultation: soft S1 and a holosystolic murmur at the apex radiating
- 72. The Natural History of MR Compensatory phase: 10-15 years Patients with asymptomatic severe MR have a
- 73. Imaging studies in MR ECG: May show, LA enlargement, atrial fibrillation and LV hypertrophy with severe
- 75. Management of MR Medications Vasodilator such as hydralazine Rate control for atrial fibrillation with β-blockers, CCB,
- 76. Management of MR Serial Echocardiography: Mild: 2-3 years Moderate: 1-2 years Severe: 6-12 months IE prophylaxis:
- 79. Simplified Indications for MV Replacement in Severe MR ANY Symptoms at rest or exercise with (repair
- 81. Скачать презентацию
Слайд 2Overview
Aortic Stenosis
Mitral Stenosis
Aortic Regurgitation
Acute and Chronic
Mitral Regurgitation
Acute and Chronic
Overview
Aortic Stenosis
Mitral Stenosis
Aortic Regurgitation
Acute and Chronic
Mitral Regurgitation
Acute and Chronic
Слайд 3Etiology
Pathophysiology
Physical Exam
Natural History
Testing
Treatment
Etiology
Pathophysiology
Physical Exam
Natural History
Testing
Treatment
Слайд 4Aortic Stenosis
Aortic Stenosis
Слайд 6Aortic Stenosis Overview:
Normal Aortic Valve Area: 3-4 cm2
Symptoms: Occur when valve area
Aortic Stenosis Overview:
Normal Aortic Valve Area: 3-4 cm2
Symptoms: Occur when valve area
Слайд 7Etiology of Aortic Stenosis
Congenital
Rheumatic
Degenerative/Calcific
Patients under 70: >50% have a congenital cause
Patients over
Etiology of Aortic Stenosis
Congenital
Rheumatic
Degenerative/Calcific
Patients under 70: >50% have a congenital cause
Patients over
Слайд 12Pathophysiology of Aortic Stenosis
A pressure gradient develops between the left ventricle and
Pathophysiology of Aortic Stenosis
A pressure gradient develops between the left ventricle and
Слайд 13Presentation of Aortic Stenosis
Syncope: (exertional)
Angina: (increased myocardial oxygen demand; demand/supply mismatch)
Dyspnea: on
Presentation of Aortic Stenosis
Syncope: (exertional)
Angina: (increased myocardial oxygen demand; demand/supply mismatch)
Dyspnea: on
Слайд 14Physical Findings in Aortic Stenosis
Slow rising carotid pulse (pulsus tardus) & decreased
Physical Findings in Aortic Stenosis
Slow rising carotid pulse (pulsus tardus) & decreased
Слайд 15Natural History
Mild AS to Severe AS:
8% in 10 years
22% in 22 years
38%
Natural History
Mild AS to Severe AS:
8% in 10 years
22% in 22 years
38%
Слайд 17Evaluation of AS
Echocardiography is the most valuable test for diagnosis, quantification and
Evaluation of AS
Echocardiography is the most valuable test for diagnosis, quantification and
Слайд 18Evaluation of AS
Cardiac catheterization: Should only be done for a direct measurement
Evaluation of AS
Cardiac catheterization: Should only be done for a direct measurement
Слайд 19Management of AS
General- IE prophylaxis in dental procedures with a prosthetic AV
Management of AS
General- IE prophylaxis in dental procedures with a prosthetic AV
Слайд 20Echo Surveillance
Mild: Every 5 years
Moderate: Every 2 years
Severe: Every 6 months to
Echo Surveillance
Mild: Every 5 years
Moderate: Every 2 years
Severe: Every 6 months to

Слайд 22Simplified Indications for Surgery in Aortic Stenosis
Any SYMPTOMATIC patient with severe AS
Simplified Indications for Surgery in Aortic Stenosis
Any SYMPTOMATIC patient with severe AS
Слайд 23Summary
Disease of aging
Look for the signs on physical exam
Echocardiogram to assess severity
Asymptomatic:
Summary
Disease of aging
Look for the signs on physical exam
Echocardiogram to assess severity
Asymptomatic:
Слайд 24Mitral Stenosis
Mitral Stenosis
Слайд 25Mitral Stenosis Overview
Definition: Obstruction of LV inflow that prevents proper filling during
Mitral Stenosis Overview
Definition: Obstruction of LV inflow that prevents proper filling during
Слайд 26Etiology of Mitral Stenosis
Rheumatic heart disease: 77-99% of all cases
Infective endocarditis: 3.3%
Mitral
Etiology of Mitral Stenosis
Rheumatic heart disease: 77-99% of all cases
Infective endocarditis: 3.3%
Mitral

Слайд 31MS Pathophysiology
Progressive Dyspnea (70%): LA dilation ? pulmonary congestion (reduced emptying)
worse with
MS Pathophysiology
Progressive Dyspnea (70%): LA dilation ? pulmonary congestion (reduced emptying)
worse with
Слайд 32Natural History of MS
Disease of plateaus:
Mild MS: 10 years after initial
Natural History of MS
Disease of plateaus:
Mild MS: 10 years after initial
Слайд 33Physical Exam Findings of MS
prominent "a" wave in jugular venous pulsations: Due
Physical Exam Findings of MS
prominent "a" wave in jugular venous pulsations: Due
Слайд 34Diastolic murmur:
Low-pitched diastolic rumble most prominent at the apex.
Heard best
Diastolic murmur:
Low-pitched diastolic rumble most prominent at the apex.
Heard best
Слайд 35Loud Opening S1 snap: heard at the apex when leaflets are still
Loud Opening S1 snap: heard at the apex when leaflets are still
Слайд 36Evaluation of MS
ECG: may show atrial fibrillation and LA enlargement
CXR: LA enlargement
Evaluation of MS
ECG: may show atrial fibrillation and LA enlargement
CXR: LA enlargement
Слайд 38Management of MS
Serial echocardiography:
Mild: 3-5 years
Moderate:1-2 years
Severe: yearly
Medications: MS like AS
Management of MS
Serial echocardiography:
Mild: 3-5 years
Moderate:1-2 years
Severe: yearly
Medications: MS like AS
Слайд 39Management of MS
Identify patient early who might benefit from percutaneous mitral balloon
Management of MS
Identify patient early who might benefit from percutaneous mitral balloon
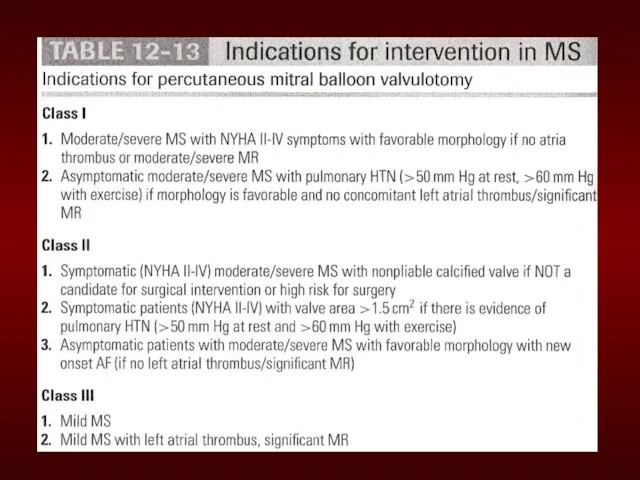
Слайд 44Simplified Indications for Mitral valve replacement
ANY SYMPTOMATIC Patient with NYHA Class III
Simplified Indications for Mitral valve replacement
ANY SYMPTOMATIC Patient with NYHA Class III
Слайд 45Aortic Regurgitation
Aortic Regurgitation
Слайд 47Aortic Regurgitation Overview
Definition: Leakage of blood into LV during diastole due to
Aortic Regurgitation Overview
Definition: Leakage of blood into LV during diastole due to
Слайд 48Etiology of Acute AR
Endocarditis
Aortic Dissection
Physical Findings:
Wide pulse pressure
Diastolic murmur
Florid pulmonary edema
Etiology of Acute AR
Endocarditis
Aortic Dissection
Physical Findings:
Wide pulse pressure
Diastolic murmur
Florid pulmonary edema
Слайд 49Treatment of Acute AR
True Surgical Emergency:
Positive inotrope: (eg, dopamine, dobutamine)
Vasodilators: (eg,
Treatment of Acute AR
True Surgical Emergency:
Positive inotrope: (eg, dopamine, dobutamine)
Vasodilators: (eg,

Слайд 51Etiology of Chronic AR
Bicuspid aortic valve
Rheumatic
Infective endocarditis
Etiology of Chronic AR
Bicuspid aortic valve
Rheumatic
Infective endocarditis
Слайд 52Pathophysiology of AR
Combined pressure AND volume overload
Compensatory Mechanisms: LV dilation, LVH. Progressive
Pathophysiology of AR
Combined pressure AND volume overload
Compensatory Mechanisms: LV dilation, LVH. Progressive
Слайд 53Natural History of AR
Asymptomatic until 4th or 5th decade
Rate of Progression: 4-6%
Natural History of AR
Asymptomatic until 4th or 5th decade
Rate of Progression: 4-6%
Слайд 54Physical Exam findings of AR
Wide pulse pressure: most sensitive
Hyperdynamic and displaced apical
Physical Exam findings of AR
Wide pulse pressure: most sensitive
Hyperdynamic and displaced apical
Слайд 56MRI of the Heart Revealing a Central, High-Velocity Jet Projecting into the
MRI of the Heart Revealing a Central, High-Velocity Jet Projecting into the
Слайд 57The Evaluation of AR
CXR: enlarged cardiac silhouette and aortic root enlargement
ECHO: Evaluation
The Evaluation of AR
CXR: enlarged cardiac silhouette and aortic root enlargement
ECHO: Evaluation
Слайд 59Management of AR
General: IE prophylaxis in dental procedures with a prosthetic AV
Management of AR
General: IE prophylaxis in dental procedures with a prosthetic AV
Слайд 62Simplified Indications for Surgical Treatment of AR
ANY Symptoms at rest or exercise
Asymptomatic
Simplified Indications for Surgical Treatment of AR
ANY Symptoms at rest or exercise
Asymptomatic
Слайд 63Mitral Regurgitation
Mitral Regurgitation

Слайд 64Definition: Backflow of blood from the LV to the LA during systole
Mild
Definition: Backflow of blood from the LV to the LA during systole
Mild
Слайд 65Acute MR
Endocarditis
Acute MI:
Malfunction or disruption of prosthetic valve
Acute MR
Endocarditis
Acute MI:
Malfunction or disruption of prosthetic valve
Слайд 66Management of Acute MR
Myocardial infarction: Cardiac cath or thrombolytics
Most other cases of
Management of Acute MR
Myocardial infarction: Cardiac cath or thrombolytics
Most other cases of
Слайд 67Management of Acute MR
Do not attempt to alleviate tachycardia with beta-blockers. Mild-to-moderate
Management of Acute MR
Do not attempt to alleviate tachycardia with beta-blockers. Mild-to-moderate
Слайд 68Treatment of Acute MR
Balloon Pump
Nitroprusside even if hypotensive
Emergent Surgery
Treatment of Acute MR
Balloon Pump
Nitroprusside even if hypotensive
Emergent Surgery
Слайд 69Myxomatous degeneration (MVP)
Ischemic MR
Rheumatic heart disease
Infective Endocarditis
Etiologies of Chronic Mitral Regurgitation
Myxomatous degeneration (MVP)
Ischemic MR
Rheumatic heart disease
Infective Endocarditis
Etiologies of Chronic Mitral Regurgitation
Слайд 70Pathophysiology of MR
Pure Volume Overload
Compensatory Mechanisms: Left atrial enlargement, LVH and increased
Pathophysiology of MR
Pure Volume Overload
Compensatory Mechanisms: Left atrial enlargement, LVH and increased
Слайд 71Physical Exam findings in MR
Auscultation: soft S1 and a holosystolic murmur at
Physical Exam findings in MR
Auscultation: soft S1 and a holosystolic murmur at
Слайд 72The Natural History of MR
Compensatory phase: 10-15 years
Patients with asymptomatic severe MR
The Natural History of MR
Compensatory phase: 10-15 years
Patients with asymptomatic severe MR
Слайд 73Imaging studies in MR
ECG: May show, LA enlargement, atrial fibrillation and LV
Imaging studies in MR
ECG: May show, LA enlargement, atrial fibrillation and LV
Слайд 75Management of MR
Medications
Vasodilator such as hydralazine
Rate control for atrial fibrillation with β-blockers,
Management of MR
Medications
Vasodilator such as hydralazine
Rate control for atrial fibrillation with β-blockers,
Слайд 76Management of MR
Serial Echocardiography:
Mild: 2-3 years
Moderate: 1-2 years
Severe: 6-12 months
IE prophylaxis:
Management of MR
Serial Echocardiography:
Mild: 2-3 years
Moderate: 1-2 years
Severe: 6-12 months
IE prophylaxis:
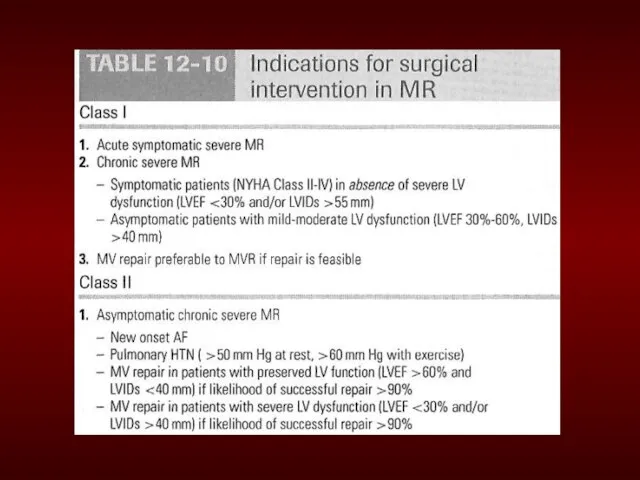
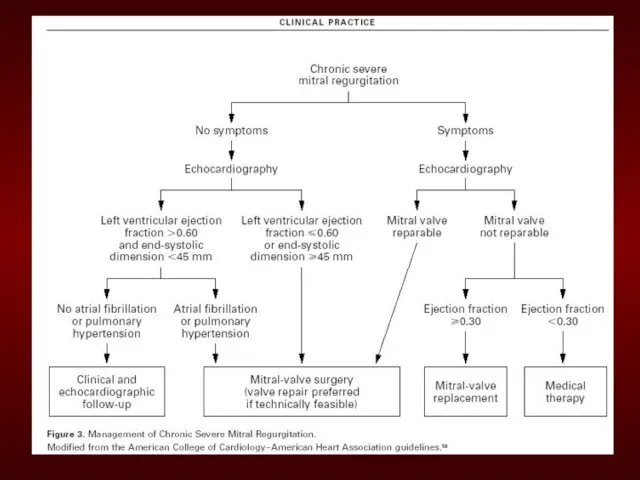
Слайд 79Simplified Indications for MV Replacement in Severe MR
ANY Symptoms at rest or
Simplified Indications for MV Replacement in Severe MR
ANY Symptoms at rest or
 Реформа армии и военного управления Петра I
Реформа армии и военного управления Петра I Художественная гимнастика с лентой
Художественная гимнастика с лентой Способы оформления блюд из овощей
Способы оформления блюд из овощей Вирусный маркетинг: российские уроки
Вирусный маркетинг: российские уроки Famous people of the USA
Famous people of the USA Рабочая программа по учебному предмету
Рабочая программа по учебному предмету Права и обязанности лицеистов
Права и обязанности лицеистов Презентация 1
Презентация 1 Смутное время 1598-1613
Смутное время 1598-1613 Покорение Сибирского ханства
Покорение Сибирского ханства Советы развития творческого мышления от Михай Чиксентмихайи
Советы развития творческого мышления от Михай Чиксентмихайи Правописание безударных гласных в корне слова
Правописание безударных гласных в корне слова Экономика потребителя §11
Экономика потребителя §11 Стабилизаторы напряжения
Стабилизаторы напряжения Работа с особыми группами пользователей
Работа с особыми группами пользователей Презентация на тему Шедевры архитектуры Индии
Презентация на тему Шедевры архитектуры Индии Альфред Адлер. Комплекс неполноценности
Альфред Адлер. Комплекс неполноценности Английские традиции общения
Английские традиции общения Проект по химии : «Керамика»
Проект по химии : «Керамика» Общие требования технических условий размещения и крепления грузов в вагонах и контейнерах
Общие требования технических условий размещения и крепления грузов в вагонах и контейнерах Визуальные детерминанты формирования образа семьи у детей
Визуальные детерминанты формирования образа семьи у детей Congratulate him to Christmas and New Year
Congratulate him to Christmas and New Year Story Book InColor
Story Book InColor Презентация на тему Базисные условия поставки Инкотермс - 2000
Презентация на тему Базисные условия поставки Инкотермс - 2000  Дорожные знаки 5 класс
Дорожные знаки 5 класс задачи по теме прямоугольный параллелепипед 9а
задачи по теме прямоугольный параллелепипед 9а Презентация на тему город Курск
Презентация на тему город Курск  Рождение театра
Рождение театра