- VASCULITIS

Содержание
- 2. Definition Blood vessels inflammation and damage Tissue ischemia Primary vasculitis Secondary vasculitis (infections, viruses, tumors, collagen
- 3. VASCULITIS CLASSIFICATION LARGE-MEDIUM-SIZED VESSELS Takayasu’s arteritis Temporal arteritis MEDIUM-SMALL-SIZED VESSELS Polyarteritis nodosa Kawasaki’s disease Churg-Strauss syndrome
- 4. VASCULITIS CLASSIFICATION MISCELLANEOUS SYNDROMES Behcet’s syndrome Pyoderma gangrenosum
- 5. VASCULITIS Pathogenesis - Immune complexes formation Ag Ab WBC Ag+Ab=IC C B-cell activation RBC
- 6. Vasculitis with IC Serum sickness CTD SLE PAN Virus hepatitis B in IC Cryoglobulinemic vasculitis Hepatitis
- 7. Vasculitis with IC Antigen excess IC formation Increased permeability of blood vessels PLT & MC: histamine,
- 8. Vasculitis with IC depositions Henoch-Schonlein purpura CVD Serum sickness HCV related mixed cryoglobulinemia HBV related PAN
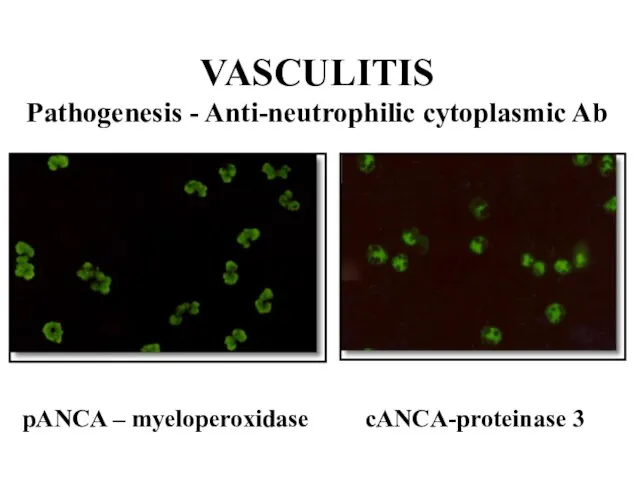
- 9. VASCULITIS Pathogenesis - Anti-neutrophilic cytoplasmic Ab pANCA – myeloperoxidase cANCA-proteinase 3
- 10. ANCA related Wegener’s granulomatosis Churg-Strauss syndrome Microscopic polyangiitis Necrotizing & crescentic GN Goodpasture’s syndrome Crohn’s disease
- 11. ANCA associated vasculitis TNFα, IL-1 induce translocation of azurophilic granules to membrane of monocytes and PMNC
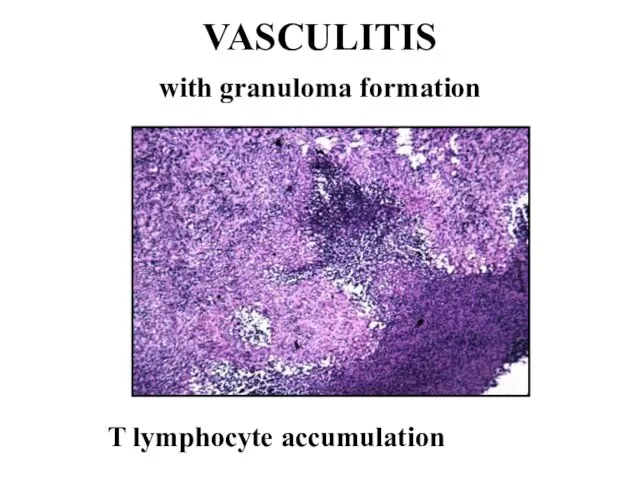
- 12. VASCULITIS with granuloma formation T lymphocyte accumulation
- 13. VASCULITIS with granuloma formation Ag or IC induce delayed hypersensitivity and cell mediated injury EC activation
- 14. T-ly response and granuloma formation GCA Takayasu-s Wegener’s granulomatosis Churg-Strauss syndrome
- 15. Suspicion of vasculitis Systemic ilness Purpura Pulmonary infiltrates Microhematuria Chronic sinusitis Mononeuritis multiplex Unexplaned ischemia GN
- 16. DD vasculitis Infection Neoplasia Lymphoma Coagulopathy Drugs/toxins Others
- 17. Takayasu’s Arteritis Pulse-less disease Incidence: 1-3/1 000 000/year. Epidemiology: girls+young women Japan, India, Africa, Asia, South
- 18. Takayasu’s Arteritis General: malaise, fever, night sweats, weight loss, arthralgia/arthritis Vascular: Arm claudication/numbness Pulses changes/discrepancy Hypertension
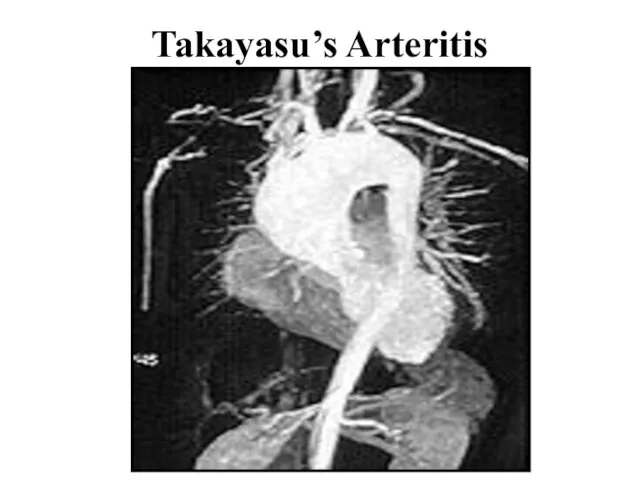
- 19. Takayasu’s Arteritis
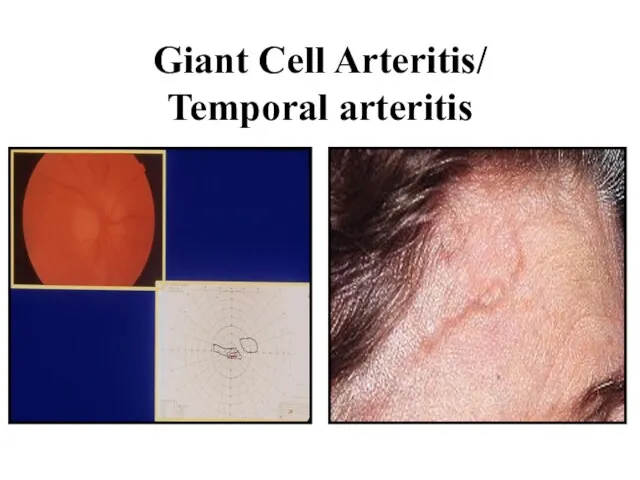
- 20. Giant Cell Arteritis/ Temporal arteritis
- 21. GCA Medial and large vessels vasculitis Branches of carotid artery Temporal arteries Strong association with PMR
- 22. GCA/PMR Age >50 F>>M Rare in blacks 6-30/100000 HLA DR4, HLA DRB1 IL-2, INF CD4+ Panarteritis
- 23. GCA Fever Headache General signs PMR Scalp tenderness Jaw claudication Ischemic optic neuropathy, visual loss Visceral
- 24. GCA Diagnosis US Doppler TA biopsy 14 days Treatment Cs (40-60 mg/d ~1 months) Aspirin MTX
- 25. PMR Diagnosis Shoulder and hip pain Stiffness High ESR Absence of signs GCA Treatment Cs (20mg/d)
- 26. Polyarteritis Nodosa (PAN) Incidence: 5-9 to 80/1 000 000 Epidemiology: M:F=2-3:1, young patients Pathology: fibrinoid necrosis
- 27. Polyarteritis Nodosa Clinical features: General: severe disease, weight loss, mild to high fever, malaise Musculo-skeletal (64%):
- 28. Polyarteritis Nodosa GIT: abdominal pain, mesenteric thrombosis, peritonitis, bleeding Kidney (60%): hypertension, renal failure, proteinuria, hematuria
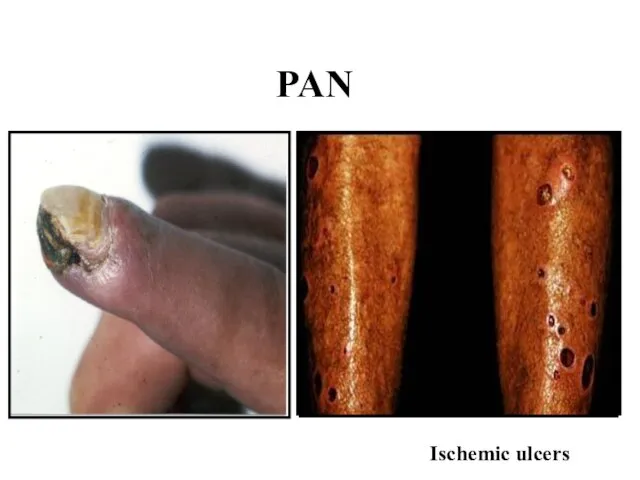
- 29. PAN Ischemic ulcers
- 30. PAN Laboratory data: ESR↑, anemia, globulins↑, 30% HBS Ag+, aHCV+, 20-30% pANCA+ , abnormal urine Diagnosis:
- 31. PAN Prognosis: 5 year survival 15%-80% Treatment: Hepatitis neg: Steroids, Cyclophosphamide, Imuran, Methotrexate Hepatitis pos: Antiviral
- 32. Microscopic polyangiitis Necrotizing vasculitis of small vessels M>F, >55y GN (80%) Pulmonary capillaritis (12%) – hemorrhage
- 33. Churg-Strauss Syndrome Incidence: 1-2/1 000 000 Epidemiology: M:F=2:1 Pathology: allergic necrotizing angiitis, eosinophils infiltration, extra-vascular granuloma
- 34. Churg-Strauss Syndrome Prodromal period: bronchial asthma Second phase: eosinophilia Lóffler s-me - eosinophilic pneumonia eosinophilic gastroenteritis
- 35. Churg-Strauss Syndrome Clinical features: General signs: fever, malaise, weight loss Lung involvement: asthma, lung infiltrates, allergic
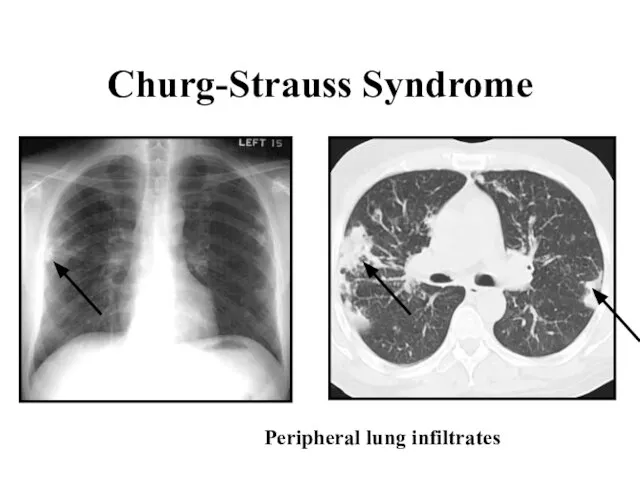
- 36. Churg-Strauss Syndrome Peripheral lung infiltrates
- 37. Churg-Strauss Syndrome Laboratory data: anemia, ESR ↑, 5 000-10 000 eosinophils/mm3, IgE ↑, pANCA + (70%)
- 38. Wegener’s Granulomatosis Incidence: 3/1 000 000 Epidemiology: M:F=1,2:1 Rare in blacks Age >40 y Pathology: necrotizing
- 39. Wegener’s Granulomatosis General signs: fever, malaise, weight loss Upper Respiratory Tract (95%): sinusitis, otitis media, nasal
- 40. Wegener’s Granulomatosis Purpura (45%)→Necrotic ulcers Arthritis (50-70%) Eyes (52%): orbital/periorbital mass and damage, scleritis, vasculitis, NS:
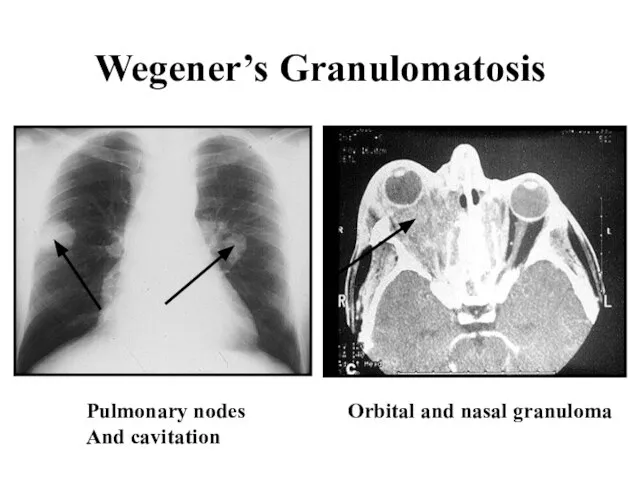
- 41. Wegener’s Granulomatosis Orbital and nasal granuloma Pulmonary nodes And cavitation
- 42. Wegener’s Granulomatosis Laboratory data: leukocytosis, anemia, ESR↑, cANCA + (90%), abnormal urine, RF+, thrombocytosis Diagnosis: nasal
- 43. Wegener’s Granulomatosis Prognosis: 5 years survival - 50-75% Progressive renal failure Late organ damage Co-morbidities Cancer
- 44. Henoch-Schőnlein Purpura Incidence: 4-10/100 000 Epidemiology: M:F=1,2:1, age 4-14 years Pathogenesis: IC vasculitis (Drugs? Infections?) Pathology:
- 45. Henoch-Schőnlein Purpura Clinical features: General signs Skin: palpable purpura (100%), ulceration (rare) Arthritis, arthralgia (60%) GIT
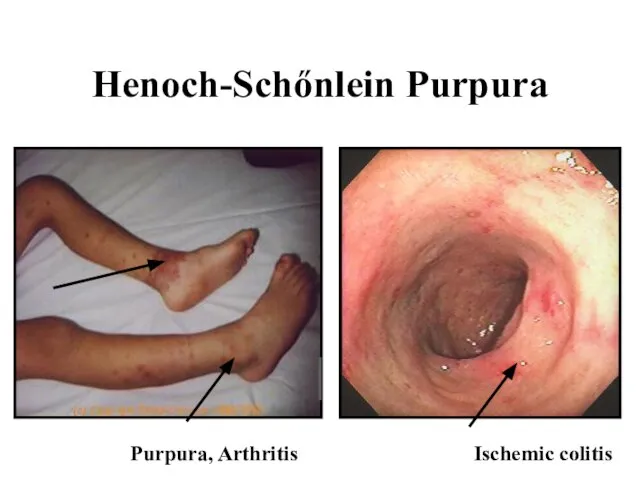
- 46. Henoch-Schőnlein Purpura Purpura, Arthritis Ischemic colitis
- 47. Henoch-Schőnlein Purpura Laboratory data: elevated ESR/CRP, leukocytosis, mild anemia, hematuria, high IgA Diagnosis: clinical +/- biopsy
- 48. Essential Mixed Cryoglobulinemia Cryo – cold-precipitable Ig (mono/polyclonal) Systemic signs Primary - rare Secondary in most
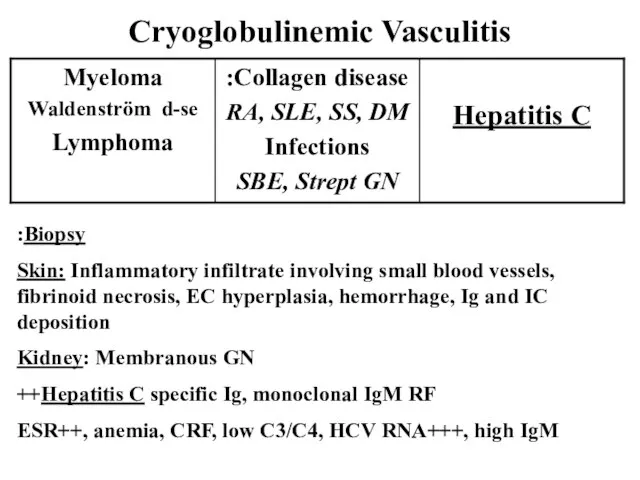
- 49. Cryoglobulinemic Vasculitis Biopsy: Skin: Inflammatory infiltrate involving small blood vessels, fibrinoid necrosis, EC hyperplasia, hemorrhage, Ig
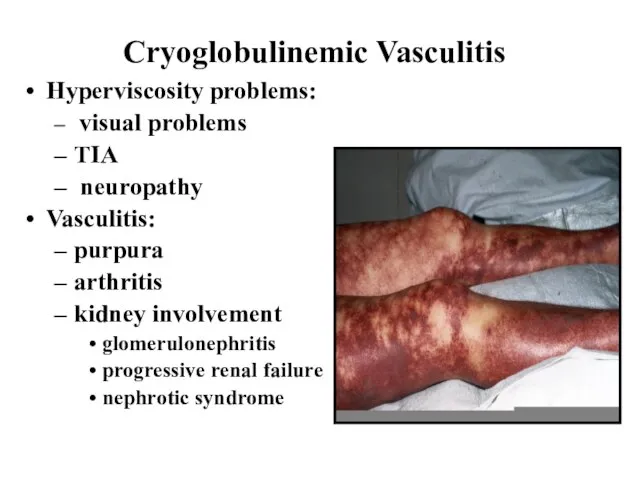
- 50. Cryoglobulinemic Vasculitis Hyperviscosity problems: visual problems TIA neuropathy Vasculitis: purpura arthritis kidney involvement glomerulonephritis progressive renal
- 51. Cryoglobulinemic Vasculitis Prognosis: poor, depends on viremia Treatment: plasmapheresis, antiviral therapy (Ribaverin + Interferon α) Cs
- 52. Behcet’s Disease Epidemiology: Japan, Meddle East (Silk rood) Family penetration Clinical feature: Oral aphthous ulcers (100%)
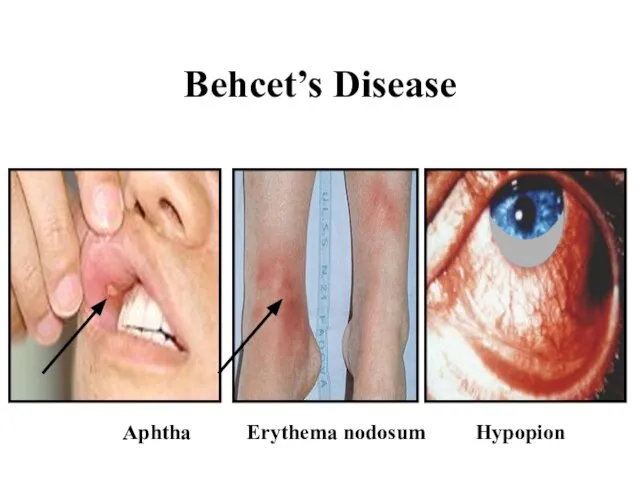
- 53. Behcet’s Disease Aphtha Erythema nodosum Hypopion
- 54. Behcet’s Disease Laboratory data: HLA B51 pos. Pathergy skin test Prognosis: serious in uveitis - blindness,
- 56. Скачать презентацию
Слайд 2Definition
Blood vessels inflammation and damage
Tissue ischemia
Primary vasculitis
Secondary vasculitis
(infections, viruses, tumors, collagen diseases:
RA,
Definition
Blood vessels inflammation and damage
Tissue ischemia
Primary vasculitis
Secondary vasculitis
(infections, viruses, tumors, collagen diseases:
RA,
Слайд 3VASCULITIS
CLASSIFICATION
LARGE-MEDIUM-SIZED VESSELS
Takayasu’s arteritis
Temporal arteritis
MEDIUM-SMALL-SIZED VESSELS
Polyarteritis nodosa
Kawasaki’s disease
Churg-Strauss syndrome
Wegener’s granulematosis
SMALL-SIZED VESSELS
Schonlein-Henoch syndrome
Cryoglobulinemia
Goodpasture’s
VASCULITIS
CLASSIFICATION
LARGE-MEDIUM-SIZED VESSELS
Takayasu’s arteritis
Temporal arteritis
MEDIUM-SMALL-SIZED VESSELS
Polyarteritis nodosa
Kawasaki’s disease
Churg-Strauss syndrome
Wegener’s granulematosis
SMALL-SIZED VESSELS
Schonlein-Henoch syndrome
Cryoglobulinemia
Goodpasture’s
Слайд 4VASCULITIS
CLASSIFICATION
MISCELLANEOUS SYNDROMES
Behcet’s syndrome
Pyoderma gangrenosum
VASCULITIS
CLASSIFICATION
MISCELLANEOUS SYNDROMES
Behcet’s syndrome
Pyoderma gangrenosum
Слайд 5VASCULITIS
Pathogenesis - Immune complexes formation
Ag
Ab
WBC
Ag+Ab=IC
C
B-cell activation
RBC
VASCULITIS
Pathogenesis - Immune complexes formation
Ag
Ab
WBC
Ag+Ab=IC
C
B-cell activation
RBC
Слайд 6Vasculitis with IC
Serum sickness
CTD
SLE
PAN
Virus hepatitis B in IC
Cryoglobulinemic vasculitis
Hepatitis C related IC
Vasculitis with IC
Serum sickness
CTD
SLE
PAN
Virus hepatitis B in IC
Cryoglobulinemic vasculitis
Hepatitis C related IC
Слайд 7Vasculitis with IC
Antigen excess
IC formation
Increased permeability of blood vessels
PLT & MC: histamine,
Vasculitis with IC
Antigen excess
IC formation
Increased permeability of blood vessels
PLT & MC: histamine,
Слайд 8Vasculitis with IC depositions
Henoch-Schonlein purpura
CVD
Serum sickness
HCV related mixed cryoglobulinemia
HBV related PAN
Vasculitis with IC depositions
Henoch-Schonlein purpura
CVD
Serum sickness
HCV related mixed cryoglobulinemia
HBV related PAN
Слайд 9VASCULITIS
Pathogenesis - Anti-neutrophilic cytoplasmic Ab
pANCA – myeloperoxidase cANCA-proteinase 3
VASCULITIS
Pathogenesis - Anti-neutrophilic cytoplasmic Ab
pANCA – myeloperoxidase cANCA-proteinase 3
Слайд 10ANCA related
Wegener’s granulomatosis
Churg-Strauss syndrome
Microscopic polyangiitis
Necrotizing & crescentic GN
Goodpasture’s syndrome
Crohn’s disease , others
ANCA related
Wegener’s granulomatosis
Churg-Strauss syndrome
Microscopic polyangiitis
Necrotizing & crescentic GN
Goodpasture’s syndrome
Crohn’s disease , others
Слайд 11ANCA associated vasculitis
TNFα, IL-1 induce translocation of azurophilic granules to membrane of
ANCA associated vasculitis
TNFα, IL-1 induce translocation of azurophilic granules to membrane of
Слайд 12VASCULITIS
with granuloma formation
T lymphocyte accumulation
VASCULITIS
with granuloma formation
T lymphocyte accumulation
Слайд 13VASCULITIS
with granuloma formation
Ag or IC induce delayed hypersensitivity and cell mediated
VASCULITIS
with granuloma formation
Ag or IC induce delayed hypersensitivity and cell mediated
Слайд 14T-ly response and granuloma formation
GCA
Takayasu-s
Wegener’s granulomatosis
Churg-Strauss syndrome
T-ly response and granuloma formation
GCA
Takayasu-s
Wegener’s granulomatosis
Churg-Strauss syndrome
Слайд 15Suspicion of vasculitis
Systemic ilness
Purpura
Pulmonary infiltrates
Microhematuria
Chronic sinusitis
Mononeuritis multiplex
Unexplaned ischemia
GN
Suspicion of vasculitis
Systemic ilness
Purpura
Pulmonary infiltrates
Microhematuria
Chronic sinusitis
Mononeuritis multiplex
Unexplaned ischemia
GN
Слайд 16DD vasculitis
Infection
Neoplasia
Lymphoma
Coagulopathy
Drugs/toxins
Others
DD vasculitis
Infection
Neoplasia
Lymphoma
Coagulopathy
Drugs/toxins
Others
Слайд 17Takayasu’s Arteritis
Pulse-less disease
Incidence: 1-3/1 000 000/year.
Epidemiology: girls+young women
Japan, India, Africa, Asia,
Takayasu’s Arteritis
Pulse-less disease
Incidence: 1-3/1 000 000/year.
Epidemiology: girls+young women
Japan, India, Africa, Asia,
Слайд 18Takayasu’s Arteritis
General: malaise, fever, night sweats, weight loss, arthralgia/arthritis
Vascular:
Arm claudication/numbness
Pulses
Takayasu’s Arteritis
General: malaise, fever, night sweats, weight loss, arthralgia/arthritis
Vascular:
Arm claudication/numbness
Pulses
Слайд 19Takayasu’s Arteritis
Takayasu’s Arteritis
Слайд 20Giant Cell Arteritis/
Temporal arteritis
Giant Cell Arteritis/
Temporal arteritis
Слайд 21GCA
Medial and large vessels vasculitis
Branches of carotid artery
Temporal arteries
Strong association with PMR
GCA
Medial and large vessels vasculitis
Branches of carotid artery
Temporal arteries
Strong association with PMR
Слайд 22GCA/PMR
Age >50
F>>M
Rare in blacks
6-30/100000
HLA DR4, HLA DRB1
IL-2, INF
CD4+
Panarteritis with mononuclear cells accumulation
GCA/PMR
Age >50
F>>M
Rare in blacks
6-30/100000
HLA DR4, HLA DRB1
IL-2, INF
CD4+
Panarteritis with mononuclear cells accumulation
Слайд 23GCA
Fever
Headache
General signs
PMR
Scalp tenderness
Jaw claudication
Ischemic optic neuropathy, visual loss
Visceral ischemia, strokes
Aortic aneurisms,
GCA
Fever
Headache
General signs
PMR
Scalp tenderness
Jaw claudication
Ischemic optic neuropathy, visual loss
Visceral ischemia, strokes
Aortic aneurisms,
Слайд 24GCA
Diagnosis
US Doppler
TA biopsy
14 days
Treatment
Cs (40-60 mg/d ~1 months)
Aspirin
MTX
Follow up: ESR
GCA
Diagnosis
US Doppler
TA biopsy
14 days
Treatment
Cs (40-60 mg/d ~1 months)
Aspirin
MTX
Follow up: ESR
Слайд 25PMR
Diagnosis
Shoulder and hip pain
Stiffness
High ESR
Absence of signs GCA
Treatment
Cs (20mg/d)
PMR
Diagnosis
Shoulder and hip pain
Stiffness
High ESR
Absence of signs GCA
Treatment
Cs (20mg/d)
Слайд 26Polyarteritis Nodosa (PAN)
Incidence: 5-9 to 80/1 000 000
Epidemiology: M:F=2-3:1, young patients
Pathology: fibrinoid
Polyarteritis Nodosa (PAN)
Incidence: 5-9 to 80/1 000 000
Epidemiology: M:F=2-3:1, young patients
Pathology: fibrinoid
Слайд 27Polyarteritis Nodosa
Clinical features:
General: severe disease, weight loss, mild to high fever, malaise
Polyarteritis Nodosa
Clinical features:
General: severe disease, weight loss, mild to high fever, malaise
Слайд 28Polyarteritis Nodosa
GIT: abdominal pain, mesenteric thrombosis, peritonitis, bleeding
Kidney (60%): hypertension, renal failure,
Polyarteritis Nodosa
GIT: abdominal pain, mesenteric thrombosis, peritonitis, bleeding
Kidney (60%): hypertension, renal failure,
Слайд 29PAN
Ischemic ulcers
PAN
Ischemic ulcers
Слайд 30PAN
Laboratory data: ESR↑, anemia, globulins↑,
30% HBS Ag+, aHCV+, 20-30% pANCA+
PAN
Laboratory data: ESR↑, anemia, globulins↑,
30% HBS Ag+, aHCV+, 20-30% pANCA+

Слайд 31PAN
Prognosis: 5 year survival 15%-80%
Treatment:
Hepatitis neg: Steroids, Cyclophosphamide, Imuran, Methotrexate
Hepatitis pos:
PAN
Prognosis: 5 year survival 15%-80%
Treatment:
Hepatitis neg: Steroids, Cyclophosphamide, Imuran, Methotrexate
Hepatitis pos:
Слайд 32Microscopic polyangiitis
Necrotizing vasculitis of small vessels
M>F, >55y
GN (80%)
Pulmonary capillaritis (12%) – hemorrhage
Cardiac
Microscopic polyangiitis
Necrotizing vasculitis of small vessels
M>F, >55y
GN (80%)
Pulmonary capillaritis (12%) – hemorrhage
Cardiac
Слайд 33Churg-Strauss Syndrome
Incidence: 1-2/1 000 000
Epidemiology: M:F=2:1
Pathology:
allergic necrotizing angiitis, eosinophils infiltration, extra-vascular
Churg-Strauss Syndrome
Incidence: 1-2/1 000 000
Epidemiology: M:F=2:1
Pathology:
allergic necrotizing angiitis, eosinophils infiltration, extra-vascular
Слайд 34Churg-Strauss Syndrome
Prodromal period: bronchial asthma
Second phase:
eosinophilia
Lóffler s-me - eosinophilic pneumonia
Churg-Strauss Syndrome
Prodromal period: bronchial asthma
Second phase:
eosinophilia
Lóffler s-me - eosinophilic pneumonia
Слайд 35Churg-Strauss Syndrome
Clinical features:
General signs: fever, malaise, weight loss
Lung involvement: asthma, lung infiltrates,
Churg-Strauss Syndrome
Clinical features:
General signs: fever, malaise, weight loss
Lung involvement: asthma, lung infiltrates,
Слайд 36Churg-Strauss Syndrome
Peripheral lung infiltrates
Churg-Strauss Syndrome
Peripheral lung infiltrates
Слайд 37Churg-Strauss Syndrome
Laboratory data: anemia, ESR ↑,
5 000-10 000 eosinophils/mm3, IgE ↑,
Churg-Strauss Syndrome
Laboratory data: anemia, ESR ↑,
5 000-10 000 eosinophils/mm3, IgE ↑,
Слайд 38Wegener’s Granulomatosis
Incidence: 3/1 000 000
Epidemiology: M:F=1,2:1
Rare in blacks
Age >40 y
Pathology: necrotizing vasculitis
Wegener’s Granulomatosis
Incidence: 3/1 000 000
Epidemiology: M:F=1,2:1
Rare in blacks
Age >40 y
Pathology: necrotizing vasculitis
Слайд 39Wegener’s Granulomatosis
General signs: fever, malaise, weight loss
Upper Respiratory Tract (95%): sinusitis, otitis
Wegener’s Granulomatosis
General signs: fever, malaise, weight loss
Upper Respiratory Tract (95%): sinusitis, otitis
Слайд 40Wegener’s Granulomatosis
Purpura (45%)→Necrotic ulcers
Arthritis (50-70%)
Eyes (52%): orbital/periorbital mass and damage, scleritis, vasculitis,
Wegener’s Granulomatosis
Purpura (45%)→Necrotic ulcers
Arthritis (50-70%)
Eyes (52%): orbital/periorbital mass and damage, scleritis, vasculitis,
Слайд 41Wegener’s Granulomatosis
Orbital and nasal granuloma
Pulmonary nodes
And cavitation
Wegener’s Granulomatosis
Orbital and nasal granuloma
Pulmonary nodes
And cavitation
Слайд 42Wegener’s Granulomatosis
Laboratory data: leukocytosis, anemia, ESR↑, cANCA + (90%), abnormal urine, RF+,
Wegener’s Granulomatosis
Laboratory data: leukocytosis, anemia, ESR↑, cANCA + (90%), abnormal urine, RF+,
Слайд 43Wegener’s Granulomatosis
Prognosis: 5 years survival - 50-75%
Progressive renal failure
Late organ damage
Co-morbidities
Cancer (bladder)
Follow
Wegener’s Granulomatosis
Prognosis: 5 years survival - 50-75%
Progressive renal failure
Late organ damage
Co-morbidities
Cancer (bladder)
Follow
Слайд 44Henoch-Schőnlein Purpura
Incidence: 4-10/100 000
Epidemiology: M:F=1,2:1, age 4-14 years
Pathogenesis: IC vasculitis (Drugs? Infections?)
Pathology:
Henoch-Schőnlein Purpura
Incidence: 4-10/100 000
Epidemiology: M:F=1,2:1, age 4-14 years
Pathogenesis: IC vasculitis (Drugs? Infections?)
Pathology:
Слайд 45Henoch-Schőnlein Purpura
Clinical features:
General signs
Skin: palpable purpura (100%), ulceration (rare)
Arthritis, arthralgia (60%)
GIT vasculitis
Henoch-Schőnlein Purpura
Clinical features:
General signs
Skin: palpable purpura (100%), ulceration (rare)
Arthritis, arthralgia (60%)
GIT vasculitis
Слайд 46Henoch-Schőnlein Purpura
Purpura, Arthritis
Ischemic colitis
Henoch-Schőnlein Purpura
Purpura, Arthritis
Ischemic colitis
Слайд 47Henoch-Schőnlein Purpura
Laboratory data: elevated ESR/CRP, leukocytosis, mild anemia, hematuria, high IgA
Diagnosis: clinical
Henoch-Schőnlein Purpura
Laboratory data: elevated ESR/CRP, leukocytosis, mild anemia, hematuria, high IgA
Diagnosis: clinical
Слайд 48Essential Mixed Cryoglobulinemia
Cryo – cold-precipitable Ig (mono/polyclonal)
Systemic signs
Primary - rare
Secondary in most
Essential Mixed Cryoglobulinemia
Cryo – cold-precipitable Ig (mono/polyclonal)
Systemic signs
Primary - rare
Secondary in most
Слайд 49Cryoglobulinemic Vasculitis
Biopsy:
Skin: Inflammatory infiltrate involving small blood vessels, fibrinoid necrosis, EC
Cryoglobulinemic Vasculitis
Biopsy:
Skin: Inflammatory infiltrate involving small blood vessels, fibrinoid necrosis, EC
Слайд 50Cryoglobulinemic Vasculitis
Hyperviscosity problems:
visual problems
TIA
neuropathy
Vasculitis:
purpura
arthritis
kidney involvement
glomerulonephritis
progressive renal
Cryoglobulinemic Vasculitis
Hyperviscosity problems:
visual problems
TIA
neuropathy
Vasculitis:
purpura
arthritis
kidney involvement
glomerulonephritis
progressive renal
Слайд 51Cryoglobulinemic Vasculitis
Prognosis: poor, depends on viremia
Treatment:
plasmapheresis,
antiviral therapy (Ribaverin + Interferon
Cryoglobulinemic Vasculitis
Prognosis: poor, depends on viremia
Treatment:
plasmapheresis,
antiviral therapy (Ribaverin + Interferon
Слайд 52Behcet’s Disease
Epidemiology: Japan, Meddle East (Silk rood)
Family penetration
Clinical feature:
Oral aphthous ulcers (100%)
Behcet’s Disease
Epidemiology: Japan, Meddle East (Silk rood)
Family penetration
Clinical feature:
Oral aphthous ulcers (100%)
Слайд 53Behcet’s Disease
Aphtha
Erythema nodosum
Hypopion
Behcet’s Disease
Aphtha
Erythema nodosum
Hypopion
Слайд 54Behcet’s Disease
Laboratory data: HLA B51 pos.
Pathergy skin test
Prognosis: serious in uveitis
Behcet’s Disease
Laboratory data: HLA B51 pos.
Pathergy skin test
Prognosis: serious in uveitis
 СОБРАНИЕ ВОЕННОСЛУЖАЩИХ, НУЖДАЮЩИХСЯ В УЛУЧШЕНИИ ЖИЛИЩНЫХ УСЛОВИЙ
СОБРАНИЕ ВОЕННОСЛУЖАЩИХ, НУЖДАЮЩИХСЯ В УЛУЧШЕНИИ ЖИЛИЩНЫХ УСЛОВИЙ Корто Мальтезе. Французский комикс
Корто Мальтезе. Французский комикс «Шаровые молнии» - презентация ученика 8б класса МОУ СОШ №2 п.Энергетик Зайнутдинова Ильи
«Шаровые молнии» - презентация ученика 8б класса МОУ СОШ №2 п.Энергетик Зайнутдинова Ильи Максим Кузнецов, Тотемская СОШ №2
Максим Кузнецов, Тотемская СОШ №2 Саранча
Саранча Гражданство Доминиканской Республики
Гражданство Доминиканской Республики как обеспечить ситуацию успеха на уроке
как обеспечить ситуацию успеха на уроке Юридическая ответственность и ее виды
Юридическая ответственность и ее виды AGRANCO CORPORATION USA
AGRANCO CORPORATION USA Трудовые правоотношения
Трудовые правоотношения ШКОЛЕ БУДУЩЕГО
ШКОЛЕ БУДУЩЕГО Презентация на тему Крещение Господне
Презентация на тему Крещение Господне Занятия с гороховым конструктором, или От проб и ошибок к системности мышления
Занятия с гороховым конструктором, или От проб и ошибок к системности мышления Презентация на тему Магазины. Покупки
Презентация на тему Магазины. Покупки Программа тренинга «Управление временем» Тренинг-менеджер Тренинг-Центр «Прорыв» Ганджа Людмила.
Программа тренинга «Управление временем» Тренинг-менеджер Тренинг-Центр «Прорыв» Ганджа Людмила. Менеджмент. Модели менеджмента
Менеджмент. Модели менеджмента Дистанцирование
Дистанцирование Соотношение национального и мирового правового развития. Общеправовые тенденции развития
Соотношение национального и мирового правового развития. Общеправовые тенденции развития 60-летию разгрома немецко – фашистских войск в Заполярьепосвящается …
60-летию разгрома немецко – фашистских войск в Заполярьепосвящается … БЕБРА1
БЕБРА1 Презентация на тему Развитие эмоционально-волевой сферы детей старшего дошкольного возраста посредством специальных игр, упражн
Презентация на тему Развитие эмоционально-волевой сферы детей старшего дошкольного возраста посредством специальных игр, упражн Презентация на тему Дает силы нам всегда витаминная еда!
Презентация на тему Дает силы нам всегда витаминная еда! По страницам повести И.С.Тургенева «Ася»
По страницам повести И.С.Тургенева «Ася» Маяковский Владимир Владимирович 1893 - 1930
Маяковский Владимир Владимирович 1893 - 1930 Геодезические работы при строительстве СПГ Портовая в Ленинградской области
Геодезические работы при строительстве СПГ Портовая в Ленинградской области Образы мира и человека в античности
Образы мира и человека в античности Психологиялық сынақтар
Психологиялық сынақтар Праздник преподобного Сергия
Праздник преподобного Сергия