- Auscultation heart

Содержание
- 2. Auscultation was inculcated by French physitian Rene Laennec Рис. 10. Стетоскопи тверд!.
- 3. First device for auscultation was a stetoscope
- 4. First binaural stetoscope
- 5. First phonendoscope
- 6. Modern stetophonendoscope
- 7. The heart is usually auscultated by a stethoscope or a phonendoscope, but direct (immediate) auscultation is
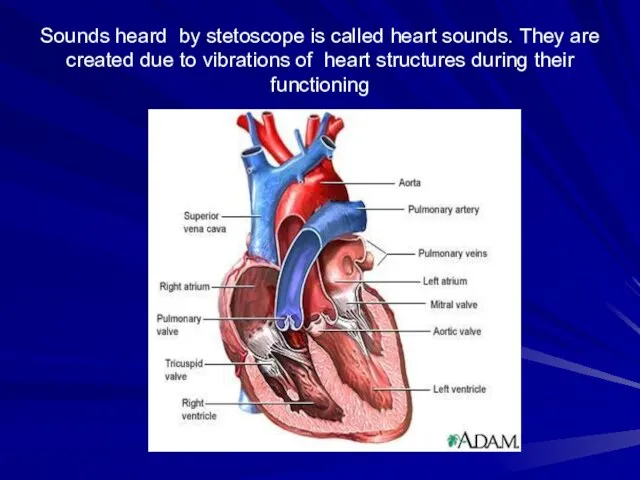
- 9. Sounds heard by stetoscope is called heart sounds. They are created due to vibrations of heart
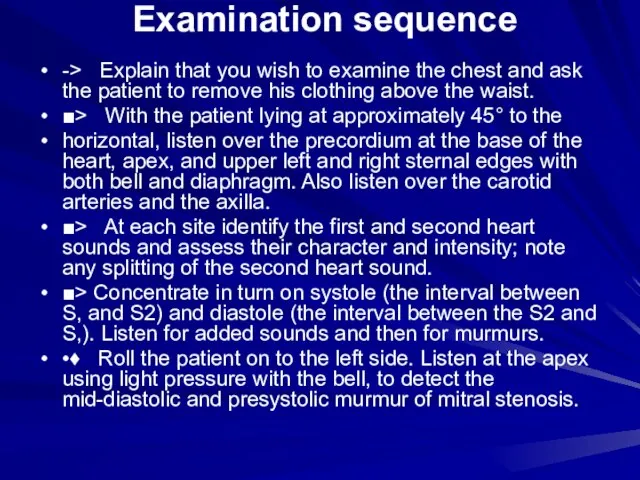
- 10. Examination sequence -> Explain that you wish to examine the chest and ask the patient to
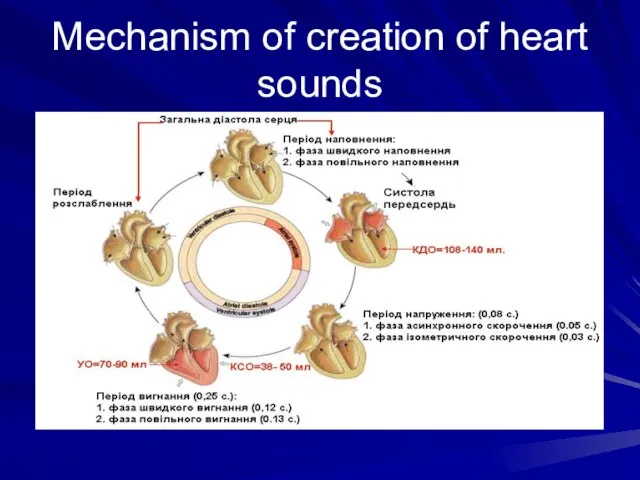
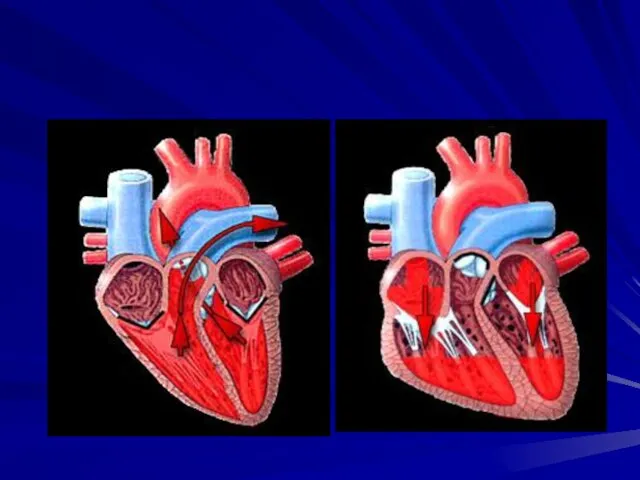
- 13. Mechanism of creation of heart sounds
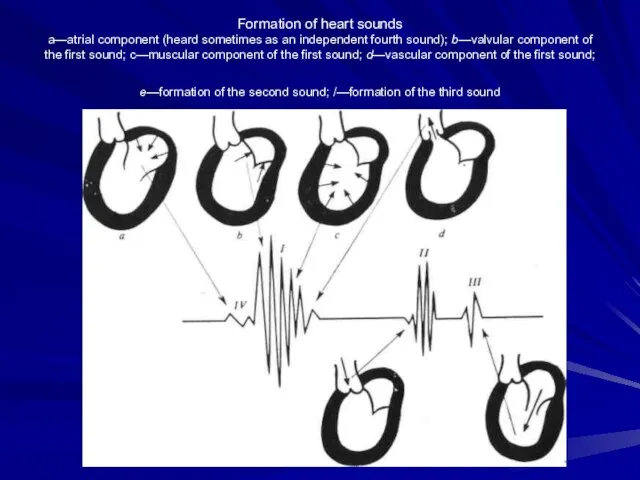
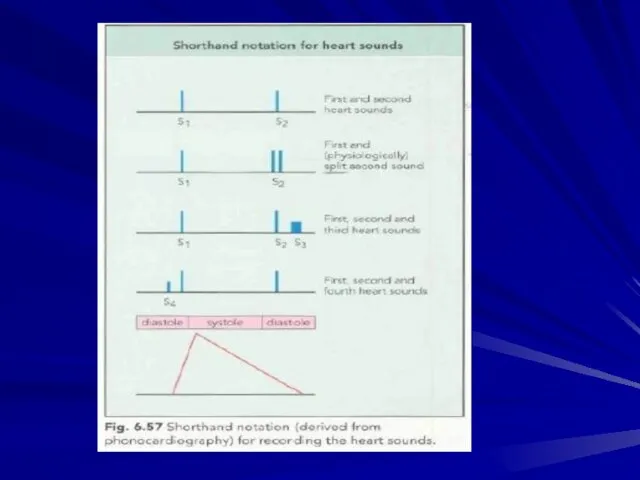
- 15. Formation of heart sounds a—atrial component (heard sometimes as an independent fourth sound); b—valvular component of
- 16. Auscultation involves listening for heart sounds with the stethoscope, similar to the procedure used in assessing
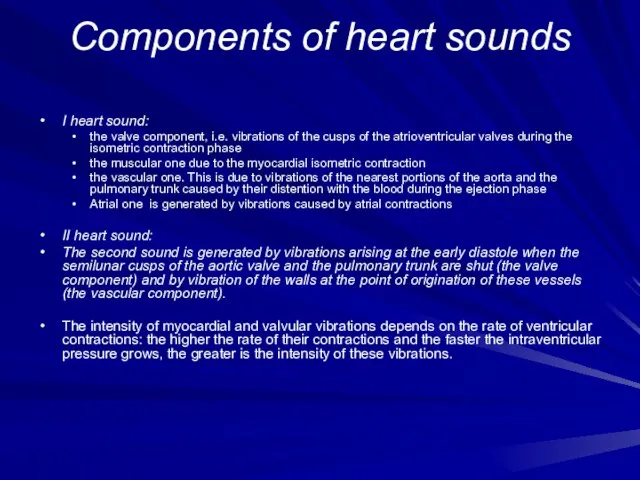
- 17. Сomponents of heart sounds I heart sound: the valve component, i.e. vibrations of the cusps of
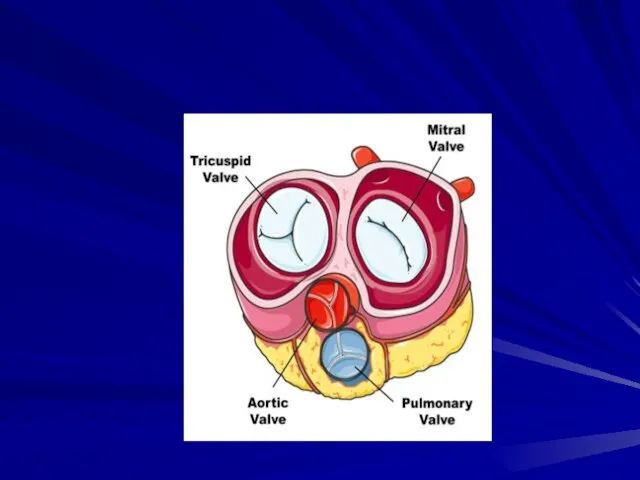
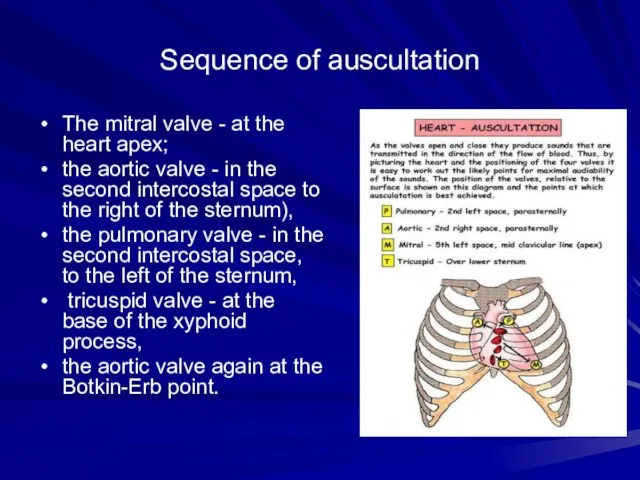
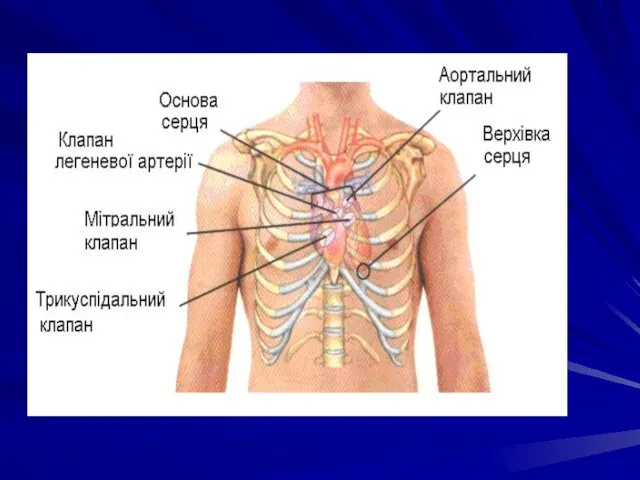
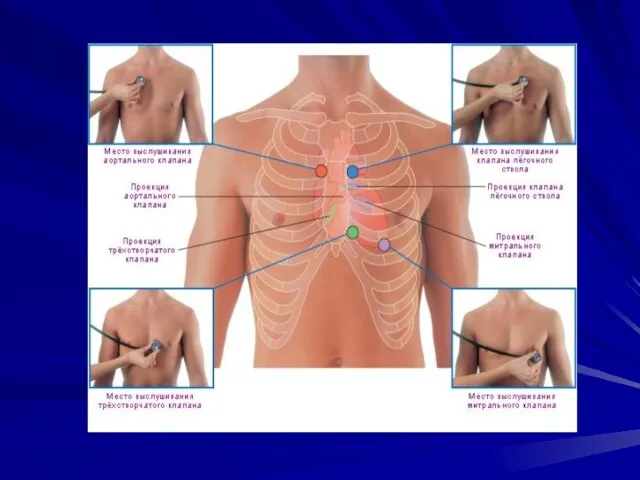
- 18. Sequence of auscultation The mitral valve - at the heart apex; the aortic valve - in
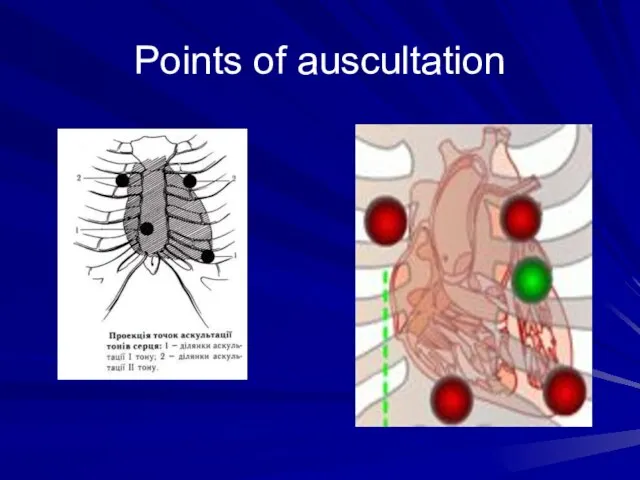
- 23. Points of auscultation
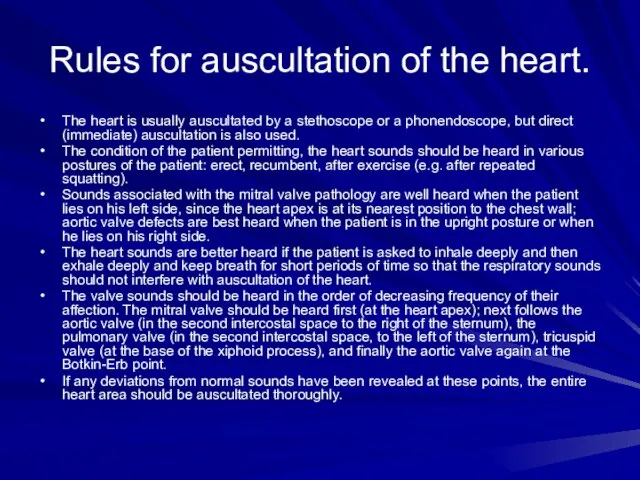
- 24. Rules for auscultation of the heart. The heart is usually auscultated by a stethoscope or a
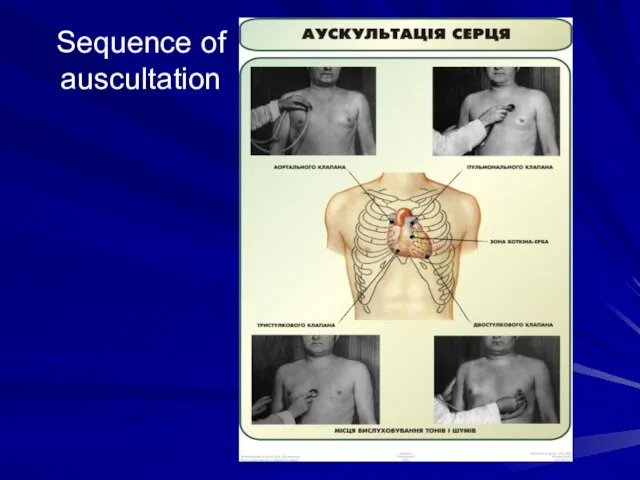
- 25. Sequence of auscultation
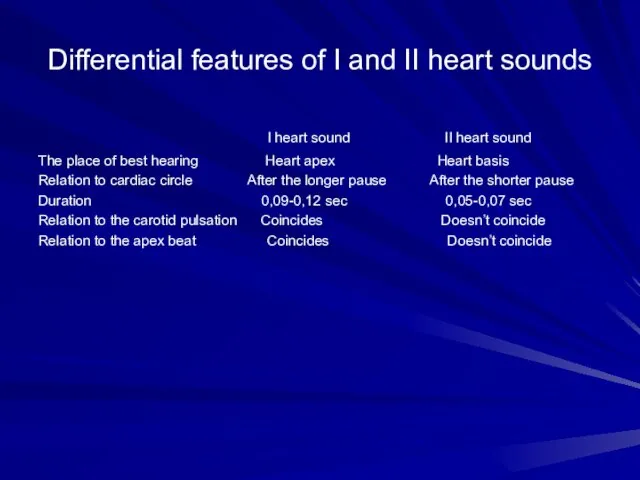
- 27. Differential features of I and II heart sounds I heart sound II heart sound The place
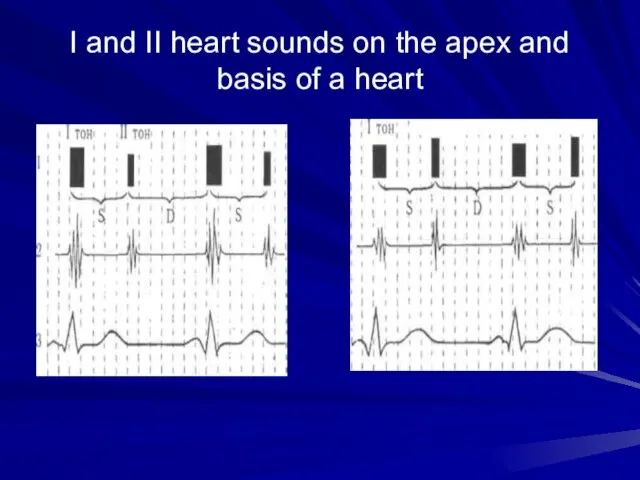
- 29. I and II heart sounds on the apex and basis of a heart
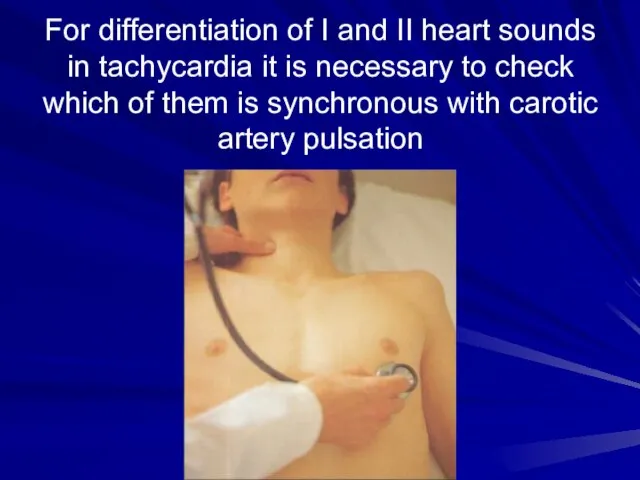
- 30. For differentiation of I and II heart sounds in tachycardia it is necessary to check which
- 31. Intensity of the heart sounds may depend on conditions of the sound wave transmission The intensity
- 32. The intensity of the heart sounds increases if their transmission to the chest becomes better: thin
- 33. Scheme of weakening and intensification of both heart sounds
- 34. Separate changes of one heart sound (I or II): First heart sound diminishes: in the mitral
- 35. Splitting or reduplication of the sounds occurs in asynchronous work and right chambers of the heart
- 36. The second sound is reduplicated more frequently Reduplication occurs due to asynchronous closure of the valve
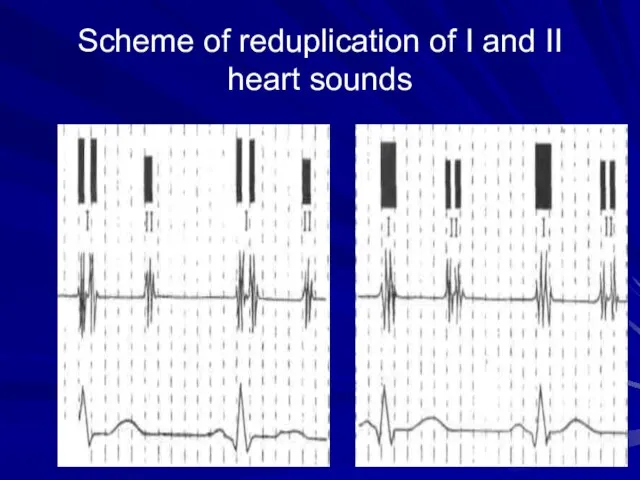
- 37. Scheme of reduplication of I and II heart sounds
- 38. Adventitious heart sounds The third heart sound (S3) is the result of vibrations produced during ventricular
- 40. Heart melodies Intensification of S3 or S4 sounds gives a three-sound or even four- three-sound rhythm,
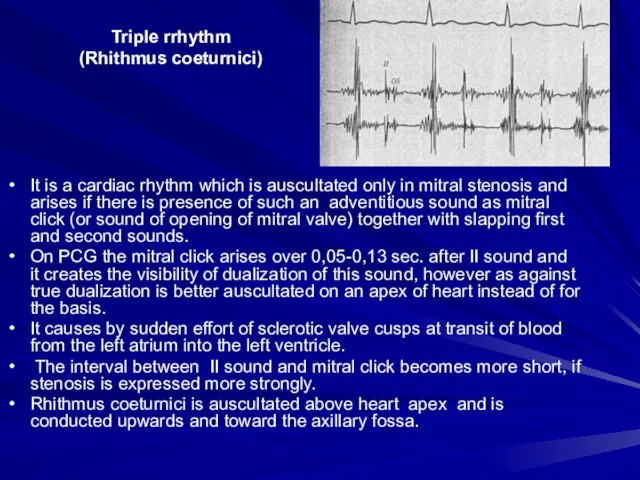
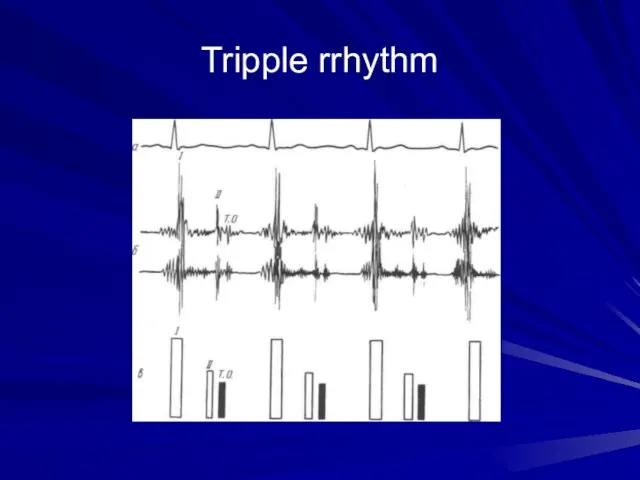
- 41. Triple rrhythm (Rhithmus coeturnici) It is a cardiac rhythm which is auscultated only in mitral stenosis
- 43. Tripple rrhythm
- 44. Pendulum rhythm In the case of pendulum rhythm the large (diastolic) heart pause is so shortened,
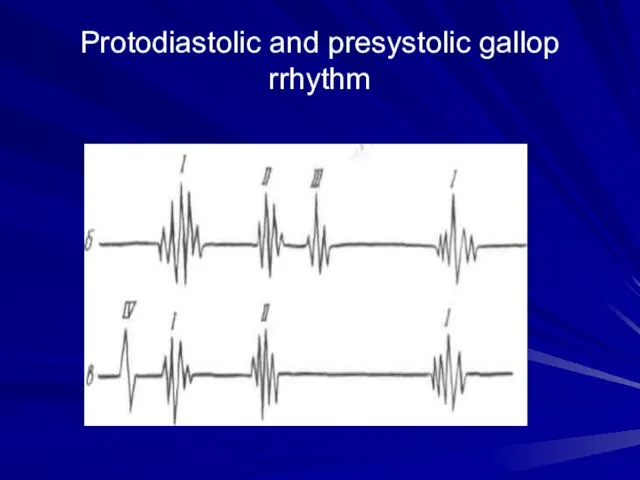
- 45. Protodiastolic and presystolic gallop rrhythm
- 46. Cardiac murmurs- phenpmena which arise due to pathological blood flow in the heart Intracardial murmurs: Organic
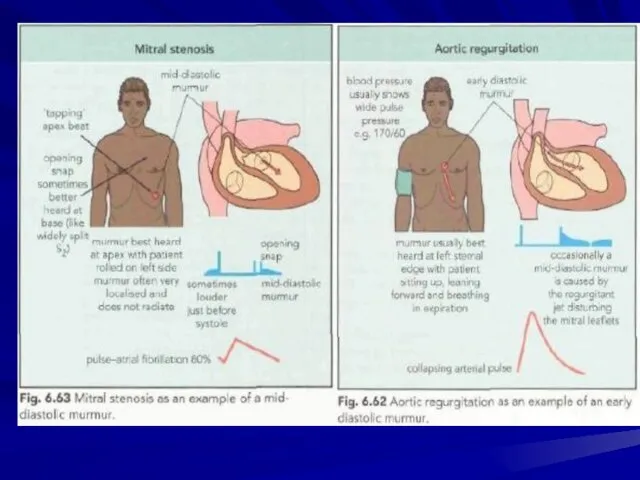
- 47. Properties of murmurs Duration The murmurs of mitral (and tricuspid) regurgitation start simultaneously with the first
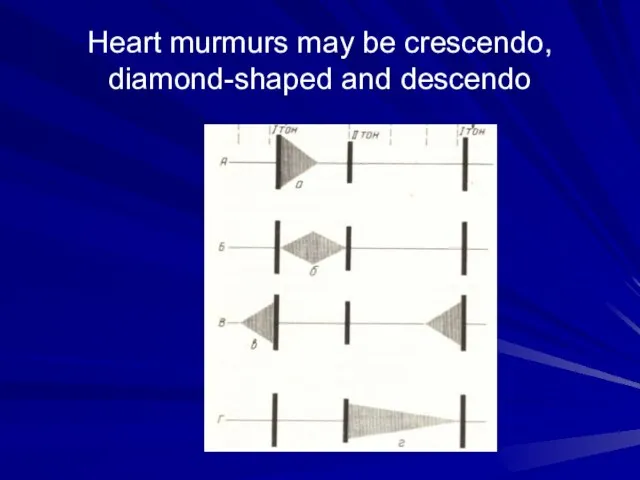
- 48. Heart murmurs may be crescendo, diamond-shaped and descendo
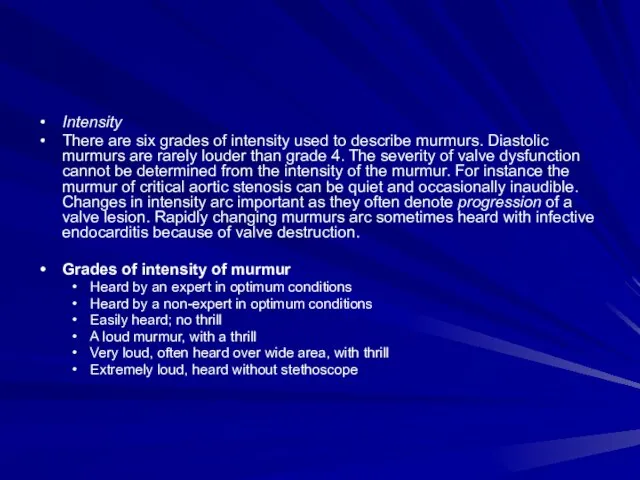
- 49. Intensity There are six grades of intensity used to describe murmurs. Diastolic murmurs are rarely louder
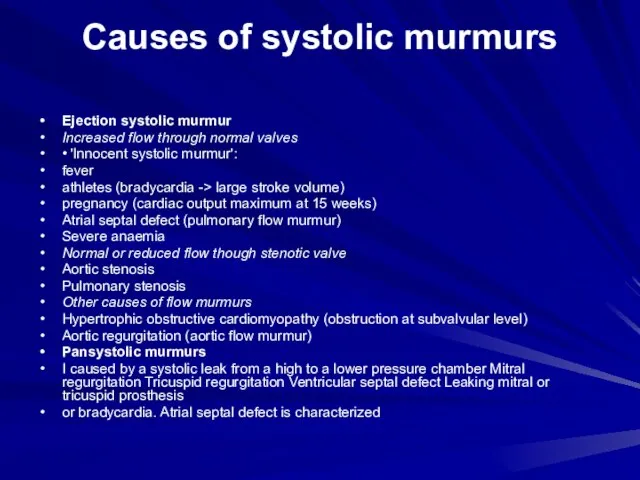
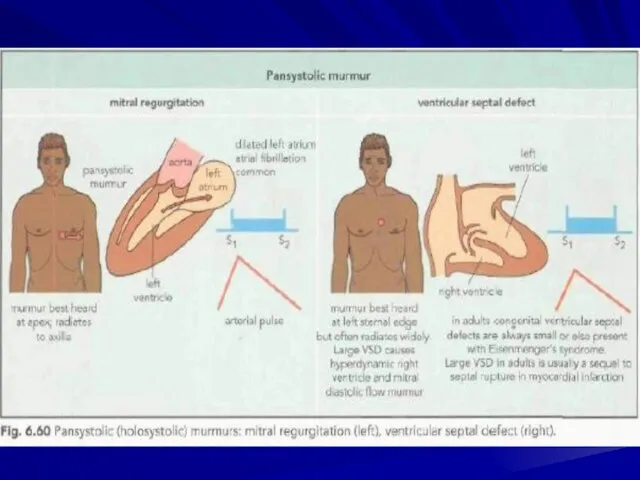
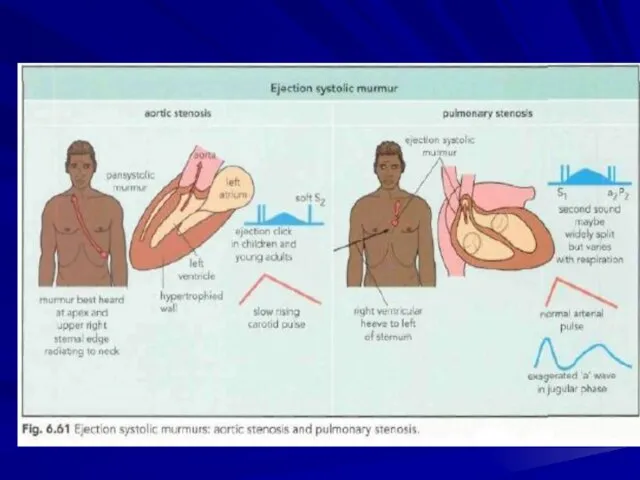
- 50. Causes of systolic murmurs Ejection systolic murmur Increased flow through normal valves • 'Innocent systolic murmur':
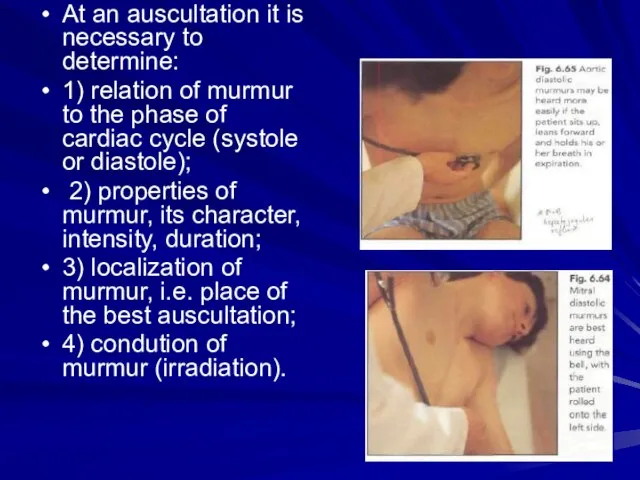
- 54. At an auscultation it is necessary to determine: 1) relation of murmur to the phase of
- 55. Murmurs are auscultated better at points of auscultation of those valves, in which they were formed.
- 56. Differentiation of functional and organic murmurs in the most cases functional murmurs are systolic; the murmurs
- 57. The pericardial friction It is develops in change of visceral and parietal pericardiac layers, when the
- 58. The pleuropericardial friction murmur It arises in inflammation of pleura, immediately accumbent to heart, owing to
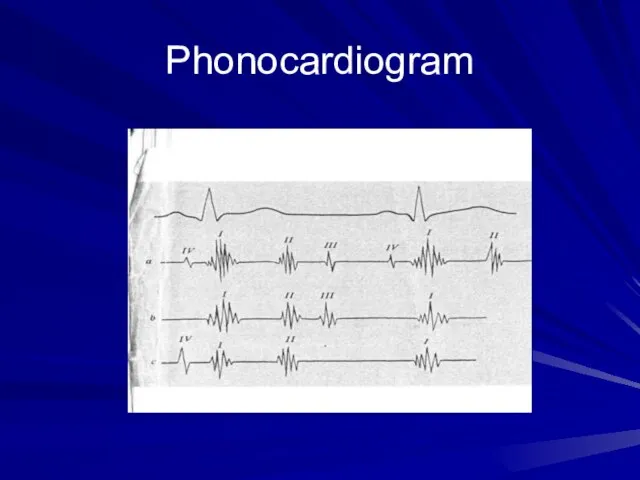
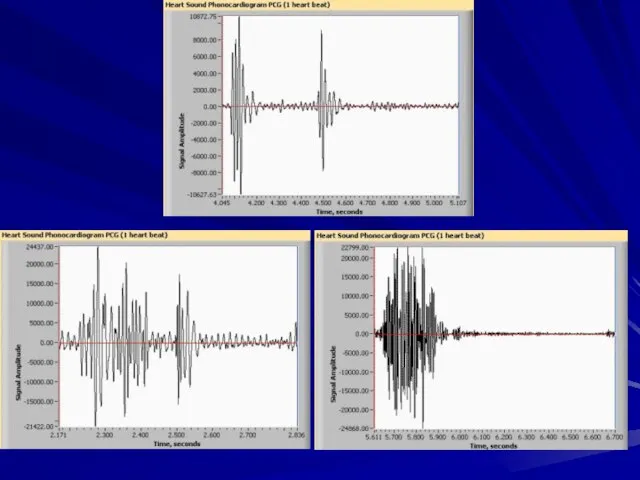
- 59. Phonocardiogram
- 61. AUSCULTATION OF VESSELS Auscultation of arteries. Arteries of medium calibre, such as the carotid, subclavian, or
- 62. In norm: Two sounds can be heard on the carotid and subclavian arteries in healthy persons.
- 63. Systolic sound produced by the stenosed aortal orifice is usually well transmitted onto the carotid and
- 64. Auscultation of veins Neither sounds nor murmurs are normally heard over veins. Auscultation of the jugular
- 66. Скачать презентацию
Слайд 3First device for auscultation was a stetoscope
First device for auscultation was a stetoscope
Слайд 4First binaural stetoscope
First binaural stetoscope

Слайд 5First phonendoscope
First phonendoscope
Слайд 6Modern stetophonendoscope
Modern stetophonendoscope

Слайд 7The heart is usually auscultated by a stethoscope or a phonendoscope, but
The heart is usually auscultated by a stethoscope or a phonendoscope, but

Слайд 9Sounds heard by stetoscope is called heart sounds. They are created due
Sounds heard by stetoscope is called heart sounds. They are created due
Слайд 10 Examination sequence
-> Explain that you wish to examine the chest and
Examination sequence
-> Explain that you wish to examine the chest and
Слайд 13Mechanism of creation of heart sounds
Mechanism of creation of heart sounds
Слайд 15Formation of heart sounds
a—atrial component (heard sometimes as an independent fourth sound);
Formation of heart sounds a—atrial component (heard sometimes as an independent fourth sound);
Слайд 16Auscultation involves listening for heart sounds with the stethoscope, similar to the
Auscultation involves listening for heart sounds with the stethoscope, similar to the
Слайд 17Сomponents of heart sounds
I heart sound:
the valve component, i.e. vibrations of the
Сomponents of heart sounds
I heart sound:
the valve component, i.e. vibrations of the
Слайд 18Sequence of auscultation
The mitral valve - at the heart apex;
the aortic valve
Sequence of auscultation
The mitral valve - at the heart apex;
the aortic valve
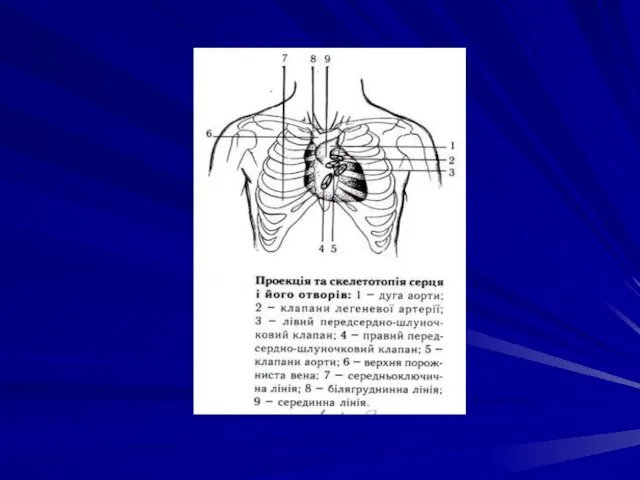
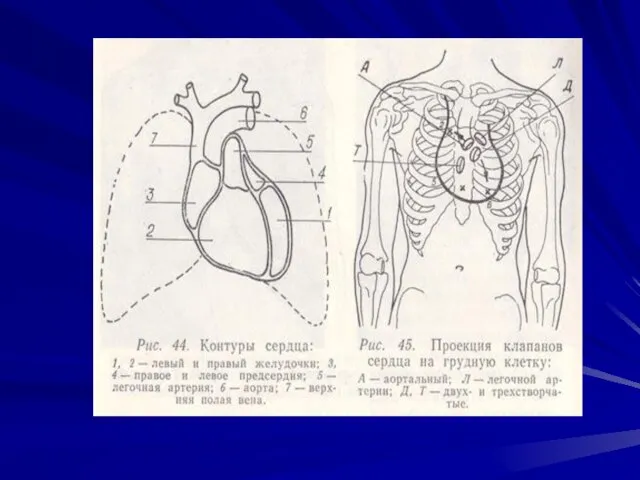

Слайд 23Points of auscultation
Points of auscultation
Слайд 24Rules for auscultation of the heart.
The heart is usually auscultated by a
Rules for auscultation of the heart.
The heart is usually auscultated by a
Слайд 25Sequence of auscultation
Sequence of auscultation
Слайд 27Differential features of I and II heart sounds
I heart sound II
Differential features of I and II heart sounds
I heart sound II

Слайд 29I and II heart sounds on the apex and basis of a
I and II heart sounds on the apex and basis of a
Слайд 30For differentiation of I and II heart sounds in tachycardia it is
For differentiation of I and II heart sounds in tachycardia it is
Слайд 31Intensity of the heart sounds may depend on conditions of the sound
Intensity of the heart sounds may depend on conditions of the sound
Слайд 32The intensity of the heart sounds increases if their transmission to the
The intensity of the heart sounds increases if their transmission to the
Слайд 33Scheme of weakening and intensification of both heart sounds
Scheme of weakening and intensification of both heart sounds
Слайд 34Separate changes of one heart sound (I or II):
First heart sound diminishes:
Separate changes of one heart sound (I or II):
First heart sound diminishes:
Слайд 35Splitting or reduplication of the sounds occurs in asynchronous work
and right chambers
Splitting or reduplication of the sounds occurs in asynchronous work and right chambers
Слайд 36The second sound is reduplicated more frequently
Reduplication occurs due to asynchronous closure
The second sound is reduplicated more frequently
Reduplication occurs due to asynchronous closure
Слайд 37Scheme of reduplication of I and II heart sounds
Scheme of reduplication of I and II heart sounds
Слайд 38Adventitious heart sounds
The third heart sound (S3) is the result of vibrations
Adventitious heart sounds
The third heart sound (S3) is the result of vibrations
Слайд 40Heart melodies
Intensification of S3 or S4 sounds gives a three-sound or even
Heart melodies
Intensification of S3 or S4 sounds gives a three-sound or even
Слайд 41Triple rrhythm
(Rhithmus coeturnici)
It is a cardiac rhythm which is auscultated only
Triple rrhythm
(Rhithmus coeturnici)
It is a cardiac rhythm which is auscultated only

Слайд 43Tripple rrhythm
Tripple rrhythm
Слайд 44Pendulum rhythm
In the case of pendulum rhythm the large (diastolic) heart pause
Pendulum rhythm
In the case of pendulum rhythm the large (diastolic) heart pause
Слайд 45Protodiastolic and presystolic gallop rrhythm
Protodiastolic and presystolic gallop rrhythm
Слайд 46Cardiac murmurs-
phenpmena which arise due to pathological blood flow in the heart
Intracardial
Cardiac murmurs-
phenpmena which arise due to pathological blood flow in the heart
Intracardial
Слайд 47Properties of murmurs
Duration
The murmurs of mitral (and tricuspid) regurgitation start simultaneously with
Properties of murmurs
Duration
The murmurs of mitral (and tricuspid) regurgitation start simultaneously with
Слайд 48Heart murmurs may be crescendo, diamond-shaped and descendo
Heart murmurs may be crescendo, diamond-shaped and descendo
Слайд 49Intensity
There are six grades of intensity used to describe murmurs. Diastolic murmurs
Intensity
There are six grades of intensity used to describe murmurs. Diastolic murmurs
Слайд 50Causes of systolic murmurs
Ejection systolic murmur
Increased flow through normal valves
• 'Innocent systolic murmur':
fever
athletes
Causes of systolic murmurs
Ejection systolic murmur
Increased flow through normal valves
• 'Innocent systolic murmur':
fever
athletes
Слайд 54At an auscultation it is necessary to determine:
1) relation of murmur
At an auscultation it is necessary to determine:
1) relation of murmur
Слайд 55 Murmurs are auscultated better at points of auscultation of those valves,
Murmurs are auscultated better at points of auscultation of those valves,
Слайд 56Differentiation of functional and organic murmurs
in the most cases functional murmurs are
Differentiation of functional and organic murmurs
in the most cases functional murmurs are
Слайд 57The pericardial friction
It is develops in change of visceral and parietal pericardiac
The pericardial friction
It is develops in change of visceral and parietal pericardiac
Слайд 58The pleuropericardial friction murmur
It arises in inflammation of pleura, immediately accumbent to
The pleuropericardial friction murmur
It arises in inflammation of pleura, immediately accumbent to
Слайд 59Phonocardiogram
Phonocardiogram
Слайд 61AUSCULTATION OF VESSELS
Auscultation of arteries. Arteries of medium calibre, such as the
AUSCULTATION OF VESSELS
Auscultation of arteries. Arteries of medium calibre, such as the
Слайд 62In norm:
Two sounds can be heard on the carotid and subclavian arteries
Two sounds can be heard on the carotid and subclavian arteries
Слайд 63Systolic sound produced by the stenosed aortal orifice is usually well transmitted
Systolic sound produced by the stenosed aortal orifice is usually well transmitted
Слайд 64Auscultation of veins
Neither sounds nor murmurs are normally heard over veins.
Auscultation
Auscultation of veins
Neither sounds nor murmurs are normally heard over veins.
Auscultation
 Consumer buyer behavior
Consumer buyer behavior Реки
Реки Сопротивление движению поезда
Сопротивление движению поезда Загрязнение озера Байкал
Загрязнение озера Байкал Абсолютные и сравнительные преимущества. Условия взаимовыгодной торговли
Абсолютные и сравнительные преимущества. Условия взаимовыгодной торговли Петербург Достоевского – «город, в котором невозможно быть»
Петербург Достоевского – «город, в котором невозможно быть» Презентация на тему Политическое развитие: понятие и критерии
Презентация на тему Политическое развитие: понятие и критерии  решение
решение Реализация требований федерального государственного образовательного стандарта средствами системы Л.В.Занкова
Реализация требований федерального государственного образовательного стандарта средствами системы Л.В.Занкова Модель семьи
Модель семьи ТРУДОВІ РЕСУРСИ І ЗАЙНЯТІСТЬ НАСЕЛЕННЯ
ТРУДОВІ РЕСУРСИ І ЗАЙНЯТІСТЬ НАСЕЛЕННЯ  Айсинг
Айсинг Презентация на тему Князь Олег
Презентация на тему Князь Олег Движение - жизнь
Движение - жизнь От инфраструктуры к бизнесу: трансформация сознания Денис Кириенко
От инфраструктуры к бизнесу: трансформация сознания Денис Кириенко Аттестация руководящих и педагогических кадров
Аттестация руководящих и педагогических кадров Конституционно - правовой статус Президента РФ
Конституционно - правовой статус Президента РФ Портрет. Картины
Портрет. Картины Инструменты развития туризма
Инструменты развития туризма  Обеспечение качества изготовления детали сателлит
Обеспечение качества изготовления детали сателлит Сүзлекләр һәм алардан файдалану күнегүләре
Сүзлекләр һәм алардан файдалану күнегүләре Формирование УУД у обучающихся основной ступени образования
Формирование УУД у обучающихся основной ступени образования Поэзия периода великой отечественной войны
Поэзия периода великой отечественной войны Педагогическая диагностика как условие дифференциации в начальной школе
Педагогическая диагностика как условие дифференциации в начальной школе Муниципальное автономное образовательное учреждение дополнительного образования детей «Детско-юношеский центр» г. Нытва
Муниципальное автономное образовательное учреждение дополнительного образования детей «Детско-юношеский центр» г. Нытва Право в системе социальных норм
Право в системе социальных норм CROWDFUNDING AS AN IDEA FOR A BUSINESS
CROWDFUNDING AS AN IDEA FOR A BUSINESS Характеристика этапов инновационного процесса
Характеристика этапов инновационного процесса