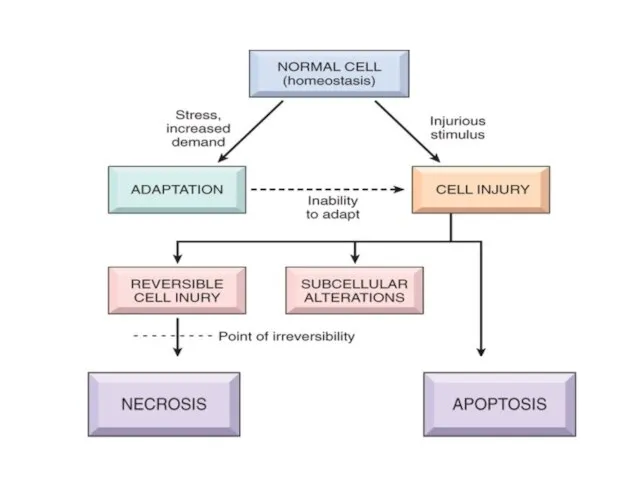
- Cell Injury, Cell Death, and Adaptations

Содержание
- 2. Cells Cells are active participants in their environment, constantly adjusting their structure and function to accommodate
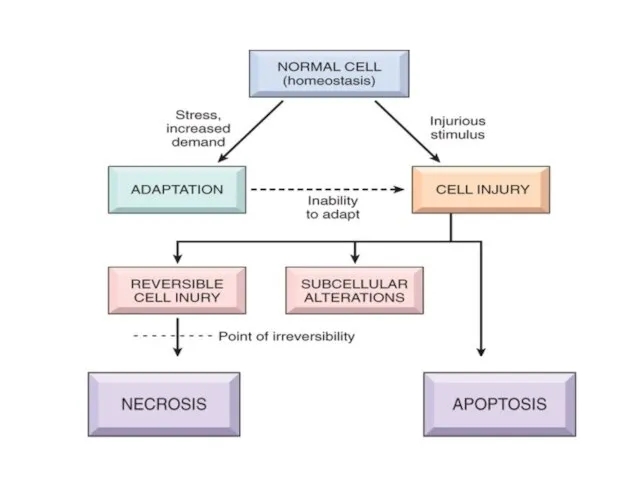
- 3. CELLULAR ADAPTATIONS As cells encounter physiologic stresses or pathologic stimuli, they can undergo: adaptation achieving a
- 4. CELLULAR ADAPTATIONS Broadly speaking, such physiologic and pathologic adaptations occur by Decreasing or increasing their size
- 5. Cells may adapt to a pathological (disease) stimulus by extending the three normal physiological adaptive responses:
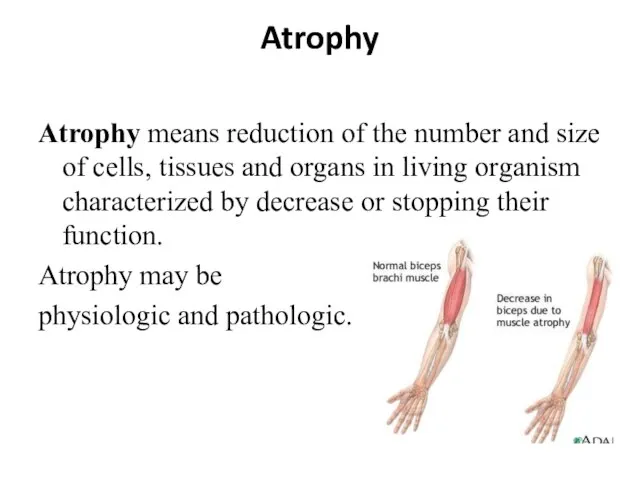
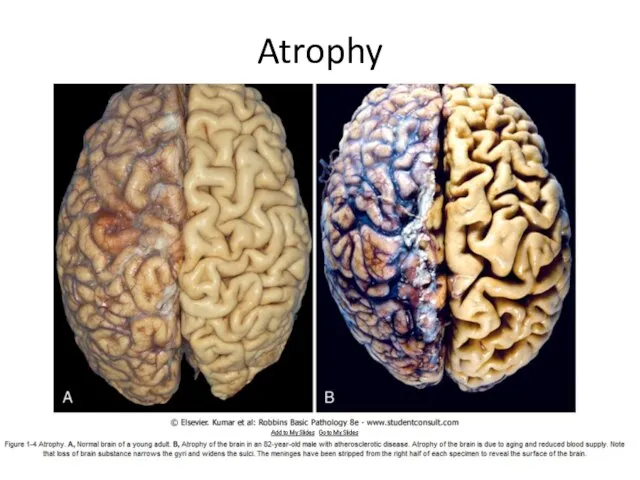
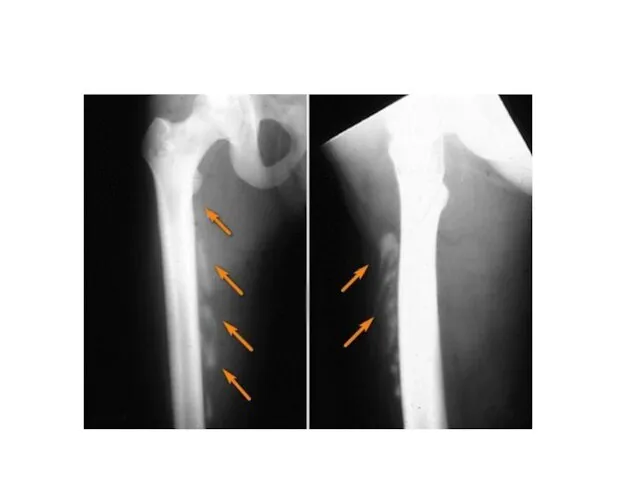
- 7. Atrophy Atrophy means reduction of the number and size of cells, tissues and organs in living
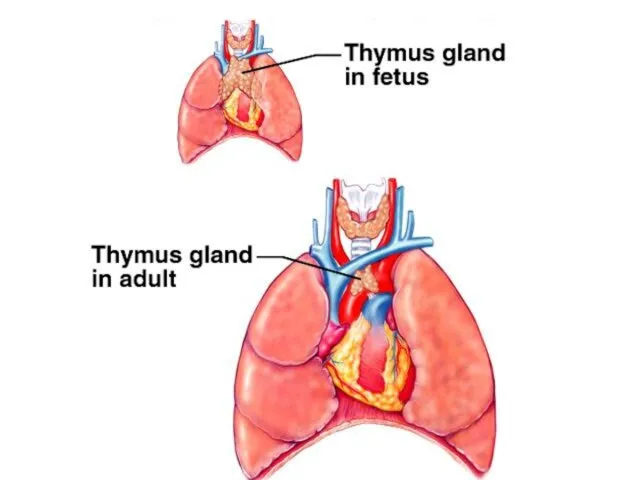
- 8. A. Physiologic atrophy. It is a normal process of aging in some tissues: 1. Atrophy of
- 10. Atrophy
- 12. B. Pathologic atrophy may be general and local. General atrophy is observed in cachexia due to
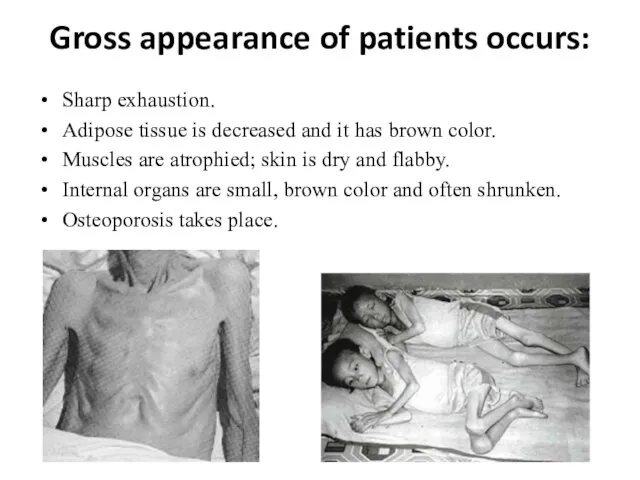
- 13. Gross appearance of patients occurs: Sharp exhaustion. Adipose tissue is decreased and it has brown color.
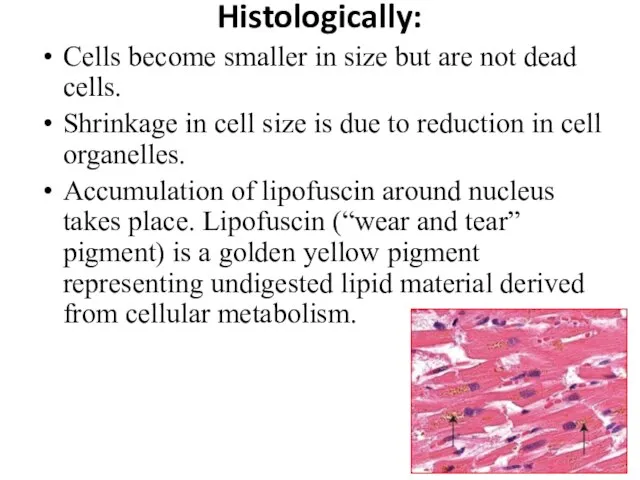
- 14. Histologically: Cells become smaller in size but are not dead cells. Shrinkage in cell size is
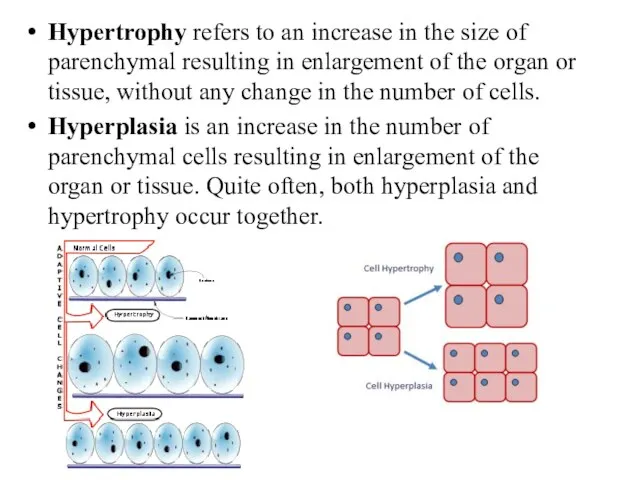
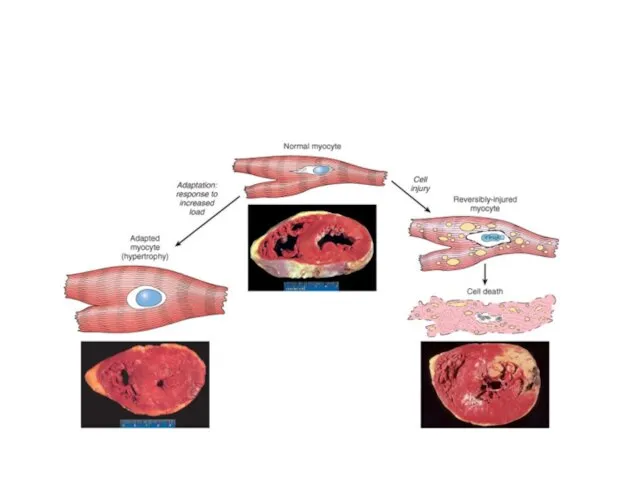
- 15. Hypertrophy refers to an increase in the size of parenchymal resulting in enlargement of the organ
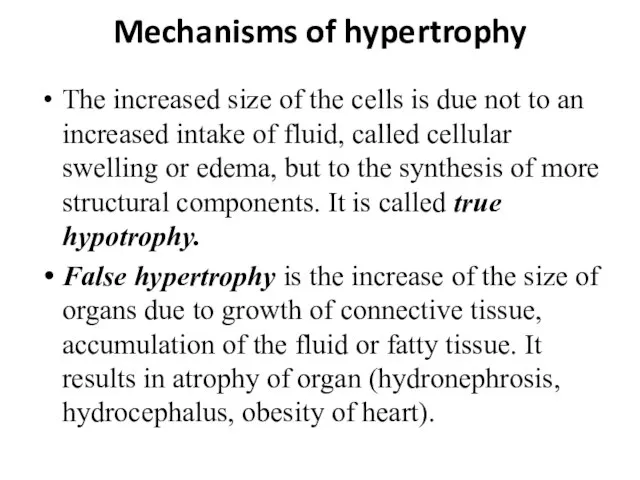
- 16. Mechanisms of hypertrophy The increased size of the cells is due not to an increased intake
- 17. True hypertrophy (hyperplasia) has adaptative and compensative characteristics and may be: physiologic pathologic
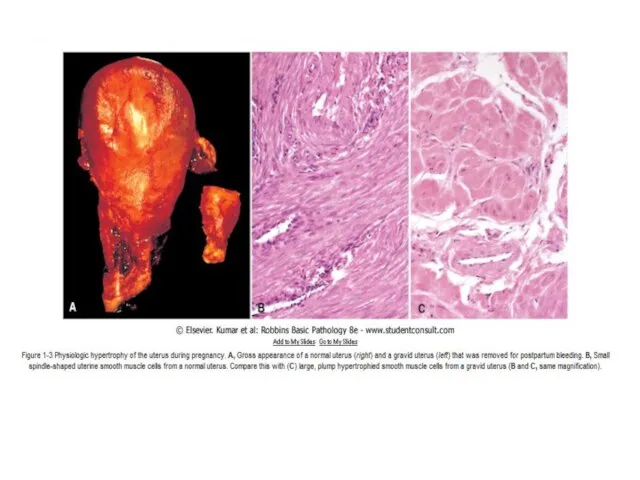
- 18. A. Physiologic hypertrophy (hyperplasia). 1. Neurogumoral (hormonal) hypertrophy: hypertrophy of female breast at puberty, during pregnancy
- 21. B. Pathologic hypertrophy (hyperplasia). Neurogumoral hypertrophy develops due to impairment of endocrine functions. Endometrial glandular hyperplasia
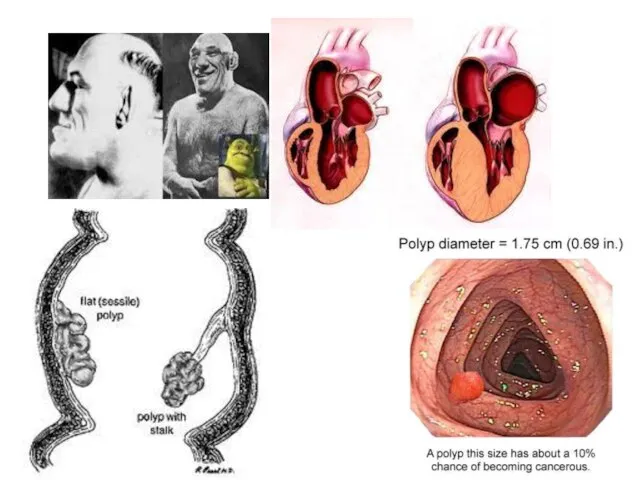
- 22. 3. Compensatory reparative hypertrophy: regeneration of the liver following partial hepatectomy, regeneration of epidermis after skin
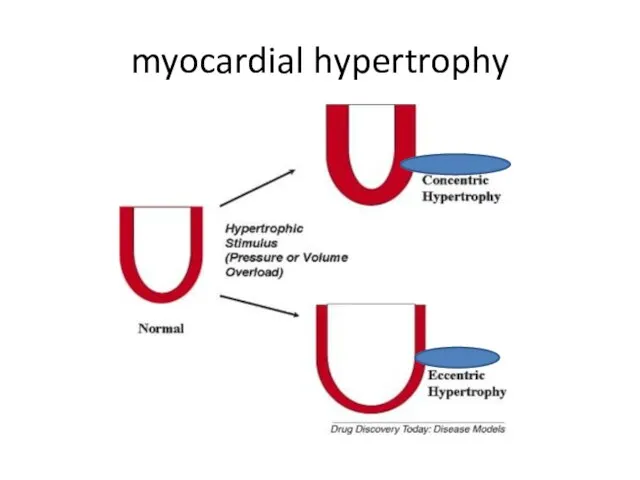
- 24. According to stage of adaptation two types of myocardial hypertrophy have been described: Concentric. In concentric
- 25. myocardial hypertrophy
- 26. Metaplasia Metaplasia is defined as a reversible change of one type to another type of adult
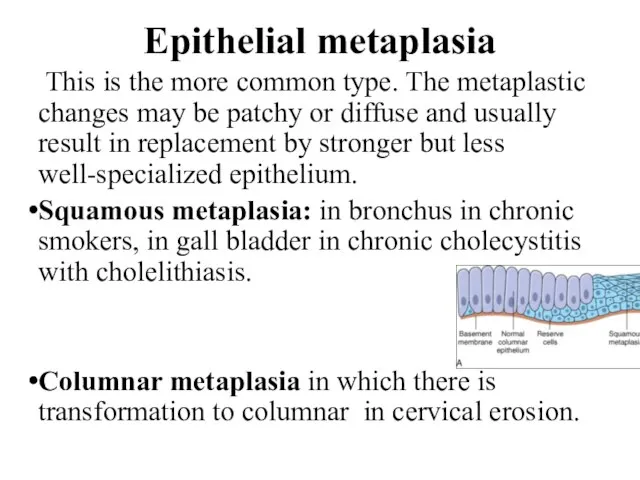
- 27. Epithelial metaplasia This is the more common type. The metaplastic changes may be patchy or diffuse
- 29. Mezenhymal metaplasia. Transformation of one adult type of mesenchymal tissue to another. Osseous metaplasia. Osseous metaplasia
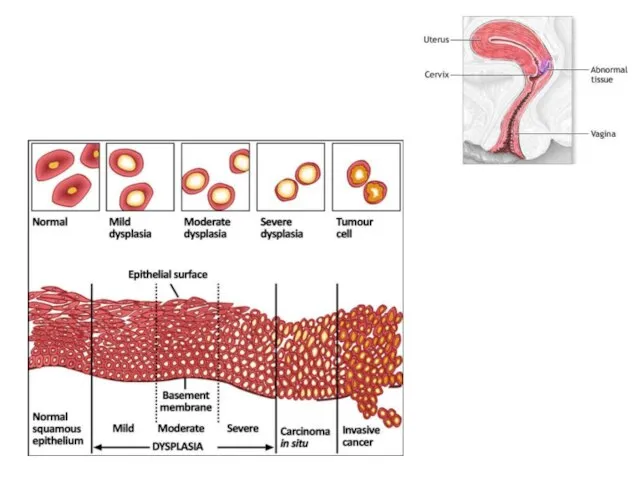
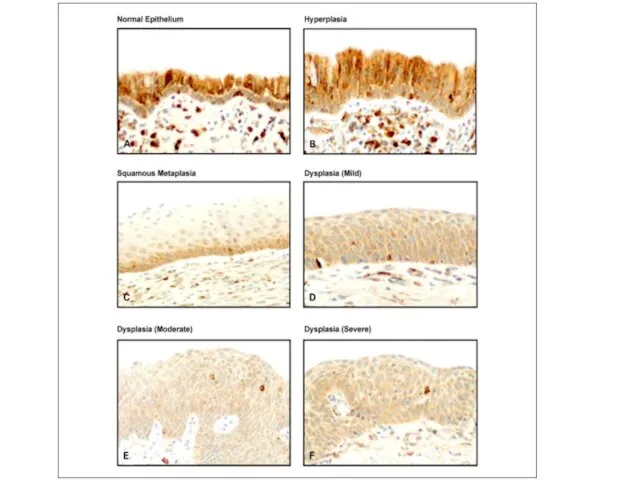
- 31. Dysplasia Dysplasia means “disordered cellular development”, often accompanied with metaplasia and hyperplasia, it is therefore also
- 36. If the adaptive capability is exceeded or if the external stress is inherently harmful, cell injury
- 37. IRREVERSIBLE CELLULAR INJURY: Cell death is a state of irreversible injury. It may occur in the
- 38. Cell death is One of the most crucial events in the evolution of disease in any
- 39. Autolysis (“self-digestion”) Is disintegration of the cell by its own hydrolytic enzymes liberated from lysosomes. Autolysis
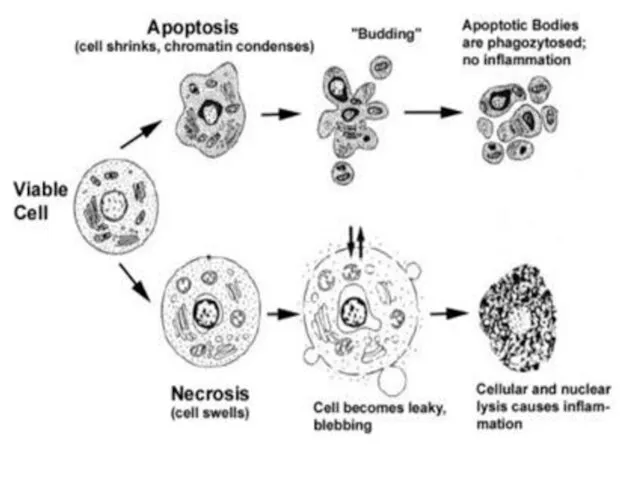
- 40. Necrosis Is celullar death in the living body in the disease. Necrosis is defined as focal
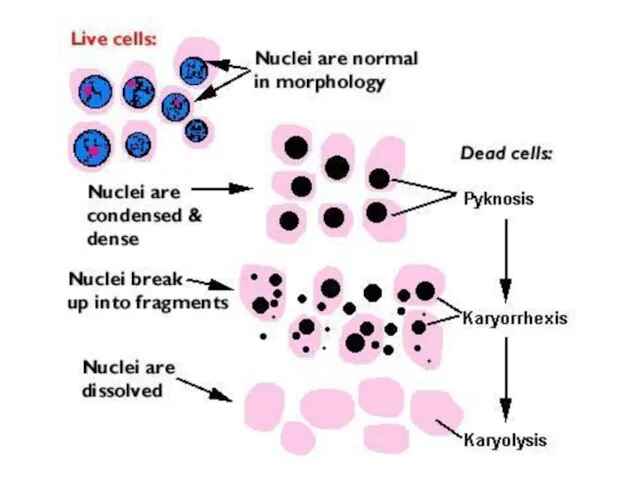
- 41. Nuclear changes. The irreversibly damaged nuclei are characterized by one of the following three features: Karyopicnosis
- 43. At electron microscopic level In addition to the above nuclear changes, disorganization and disintegration of the
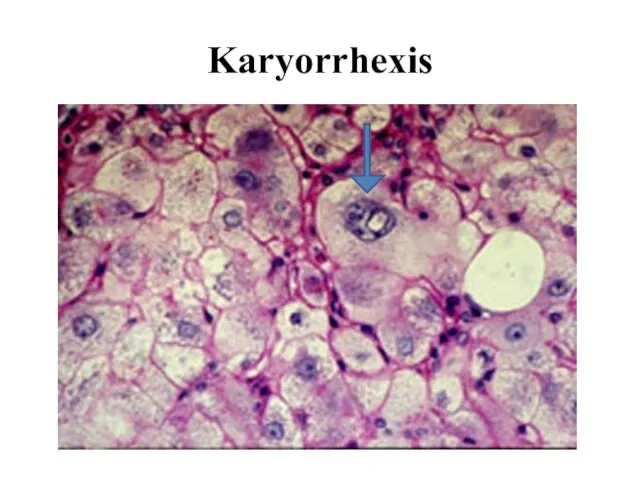
- 44. Karyorrhexis
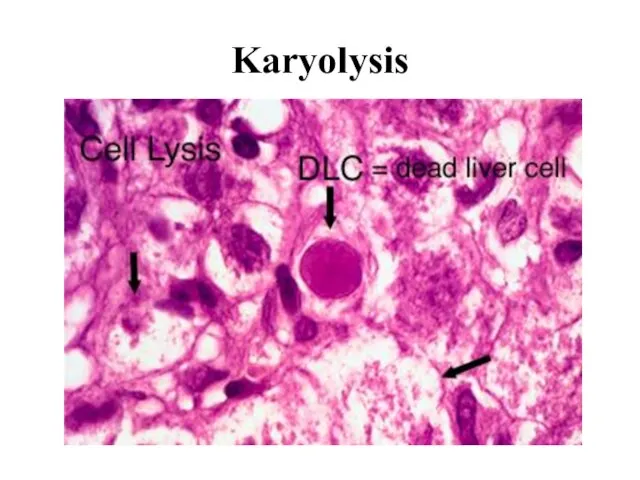
- 45. Karyolysis
- 46. The presence of the grains of chromatin in a focus of caseous necrosis is a manifestation
- 47. Stages of necrosis (or morphogenesis): 1. Paranecrosis - reversible changes; as a rule, reversible degeneration. 2.
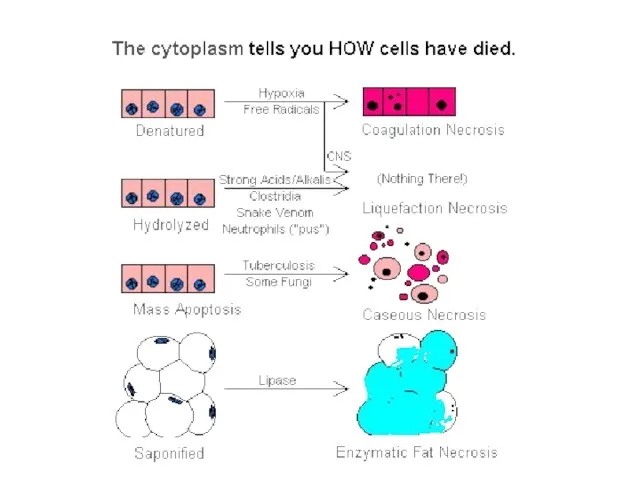
- 48. Types of necrosis According to the mechanisms of development: 1. Direct (from influence of mechanical, physical,
- 49. Types of necrosis According to the cause: 1. Traumatic. 2. Toxic. 3. Trophoneurotic. 4. Allergic. 5.
- 50. Coagulative necrosis Is associated with inhibition of lytic enzymes. Foci of coagulative necrosis in the early
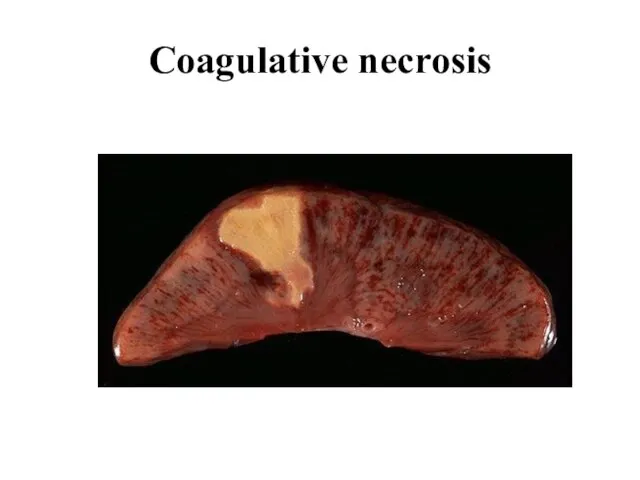
- 51. Coagulative necrosis
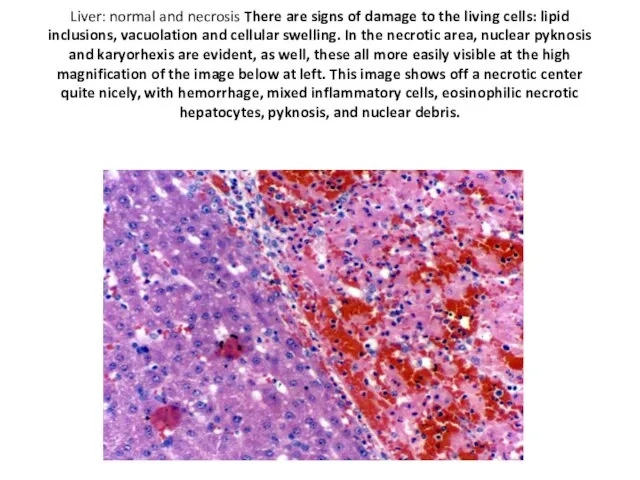
- 52. Liver: normal and necrosis There are signs of damage to the living cells: lipid inclusions, vacuolation
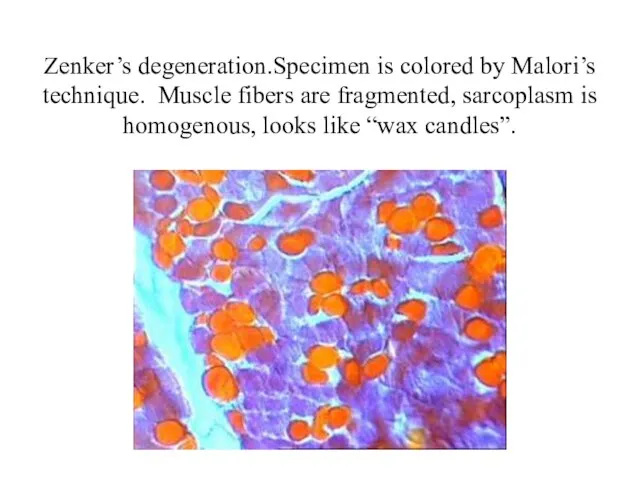
- 53. Zenker’s degeneration.Specimen is colored by Malori’s technique. Muscle fibers are fragmented, sarcoplasm is homogenous, looks like
- 54. Liquefactive (colliquative) necrosis Is marked by dissolution of tissue due to enzymatic lysis of dead cells.
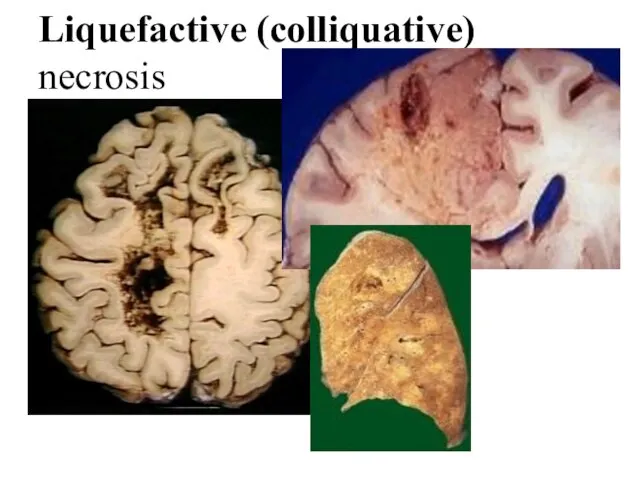
- 55. Liquefactive (colliquative) necrosis
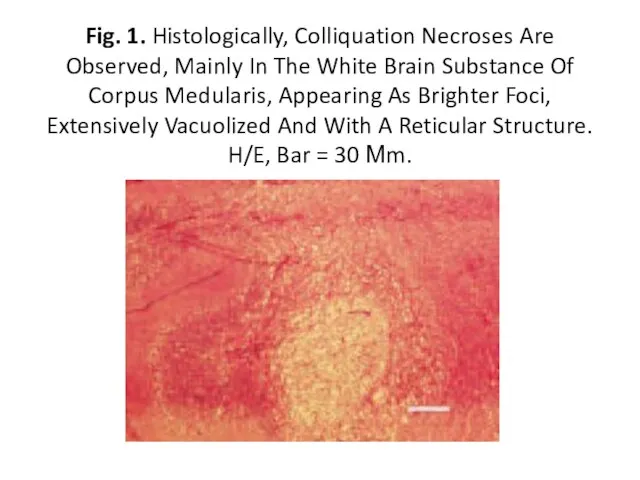
- 56. Fig. 1. Histologically, Colliquation Necroses Are Observed, Mainly In The White Brain Substance Of Corpus Medularis,
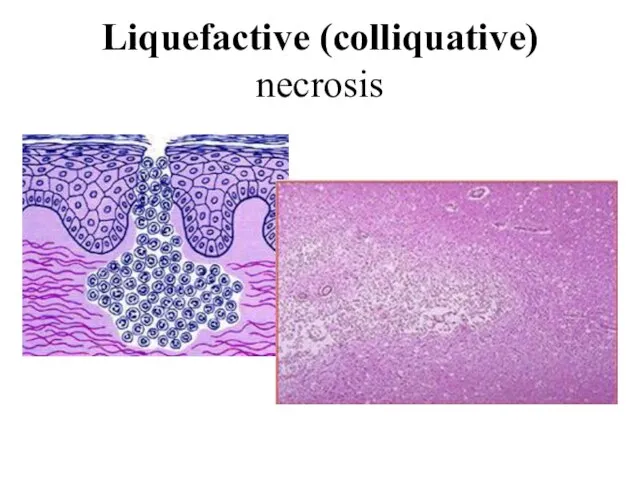
- 57. Liquefactive (colliquative) necrosis
- 58. Gangrene develops in organs and tissues having contact with environment. The most often examples of gangrene
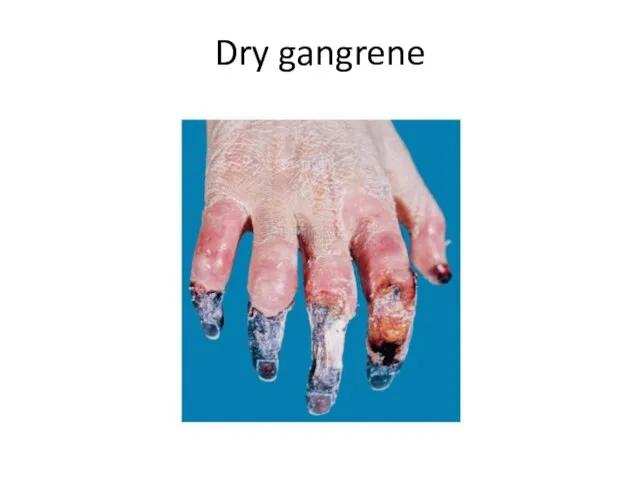
- 59. Dry gangrene
- 60. Wet gangrene
- 61. Gas gangrene
- 62. Gangrene does not appear in… Skin Kidney Lungs Uterus Intestine (bowel)
- 63. On autopsy it is revealed enlarged dense right lung, fibrin layers on the pleura. Lung tissue
- 64. A patient with diabetes mellitus suddenly began having sharp pain in his right foot. The examination
- 65. In 77-year-old patient suffered with atherosclerosis the pain has appeared in the right foot. The foot
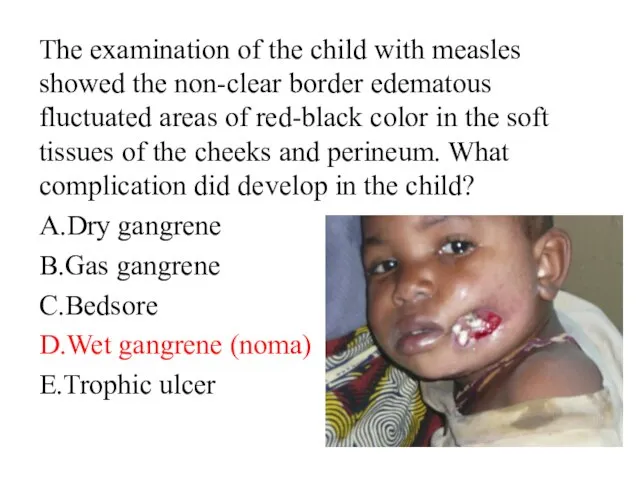
- 66. The examination of the child with measles showed the non-clear border edematous fluctuated areas of red-black
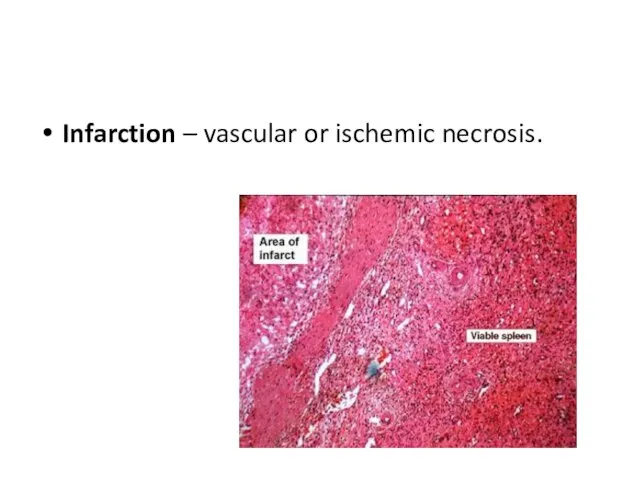
- 67. Infarction – vascular or ischemic necrosis.
- 68. A patient died from acute cardiac insufficiency. The histological examination of his heart revealed in myocardium
- 69. Infarction is… Hyperemia Stasis Ichemical necrosis Secquestrum Degeneration
- 70. A 65-year-old patient, who suffered from arteriosclerosis, has been hospitalized in surgical department because he had
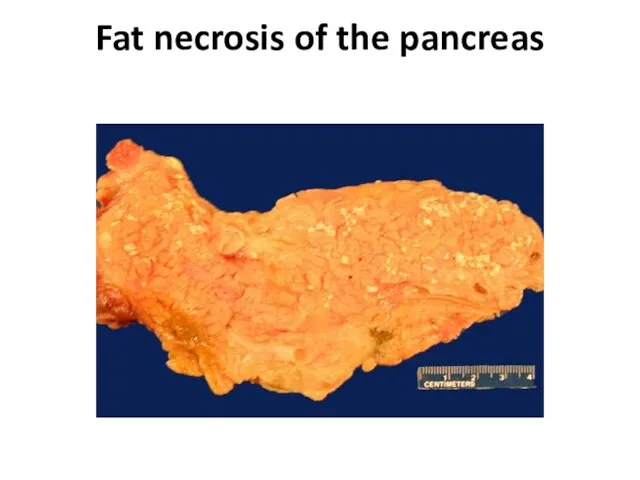
- 71. Fat necrosis is encountered in adipose tissue contiguous to the pancreas and more rarely at distant
- 72. Fat necrosis of the pancreas
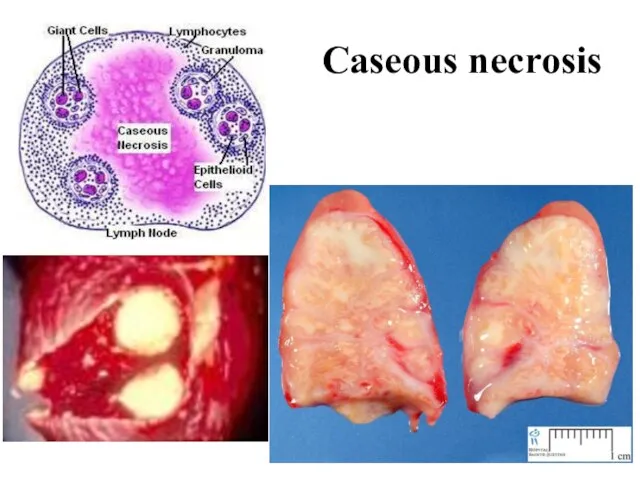
- 73. Caseous necrosis Has features of both coagulative and liquefactive necrosis. Typically, it occurs in the center
- 74. Caseous necrosis
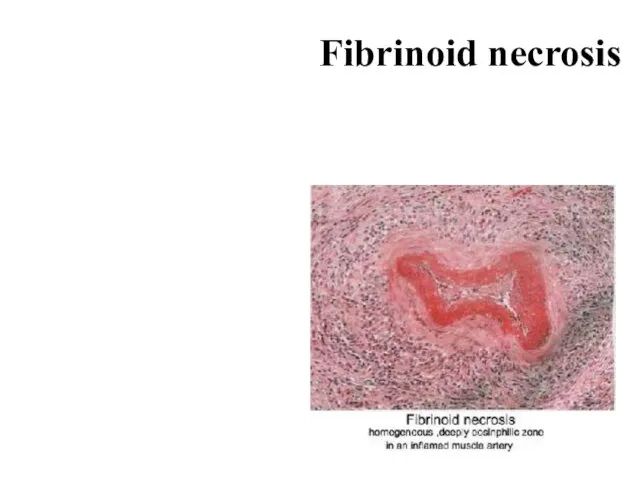
- 75. Fibrinoid necrosis Is characterised by deposition of fibrin-like material, which has the staining properties of fibrin.
- 76. Fibrinoid necrosis
- 78. Outcomes of necrosis Regeneration of tissues – replacement of the dead tissue with a new one.
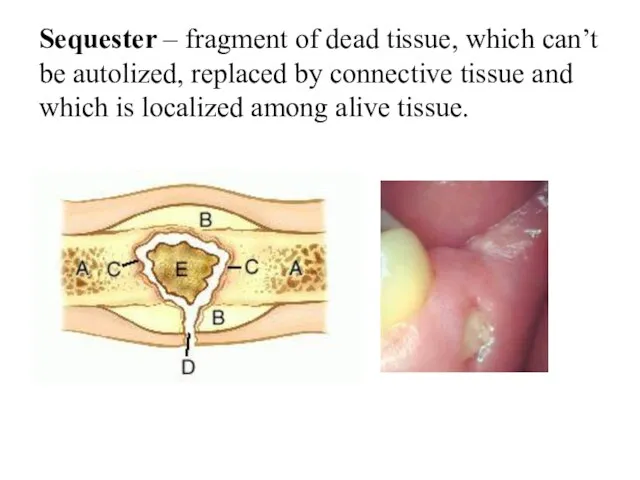
- 79. Sequester – fragment of dead tissue, which can’t be autolized, replaced by connective tissue and which
- 80. Apoptosis Is a programmed (physiological) death of the cell in the living body. Morphologic features of
- 81. Histologically In tissues stained with hematoxylin and eosin, apoptotic involves single cells or small clusters of
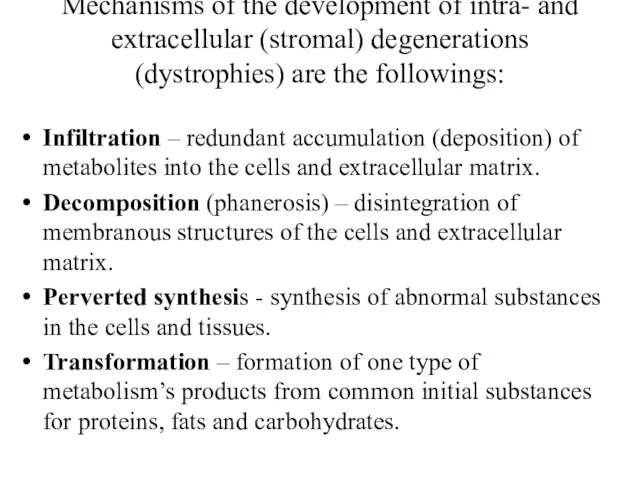
- 83. Mechanisms of the development of intra- and extracellular (stromal) degenerations (dystrophies) are the followings: Infiltration –
- 84. Intracellular fatty degenerations For identification of different kind of fats we usually use special reactions (staining):
- 85. Disturbance of fat metabolism may manifest as: appearance in the place where it does not appear
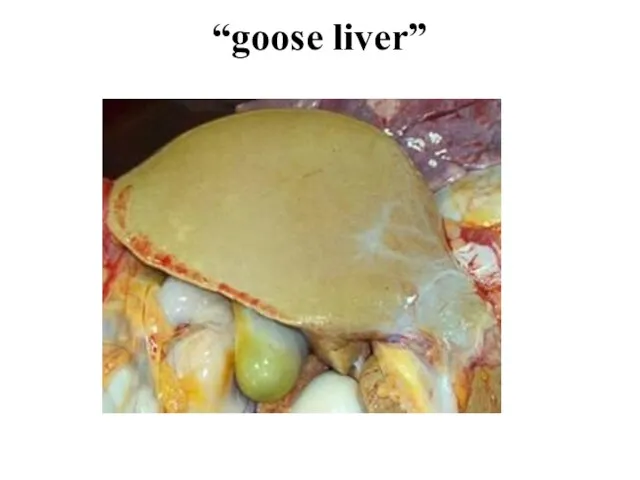
- 86. Fatty degeneration of the liver Macroscopically the fatty liver is enlarged with rounded margins. The cut
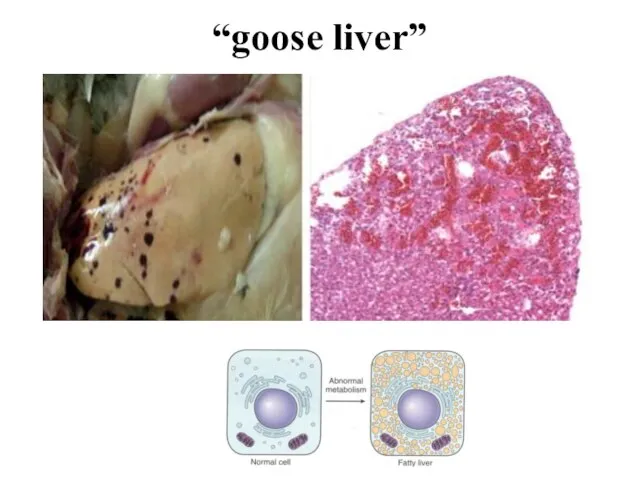
- 87. “goose liver”
- 88. “goose liver”
- 89. Autopsy of the patient who had suffered from tuberculosis demonstrated that the liver weighed 1600 g,
- 90. Fatty degeneration of the heart It is also called “Tiger’s” heart. Macroscopically the heart is enlarged,
- 91. External examination of a newborn revealed dry dull pale skin Autopsy of the patient who had
- 92. Autopsy of the patient who had suffered from hypertension disease revealed considerable enlarged flabby heart with
- 93. The kidneys look like “large white kidney”. They are enlarged, flabby. The cortical substance is gray
- 94. Stromal fatty infiltration is the deposition of mature adipose cells in the stromal connective tissue. The
- 95. Depending on the excess of the patient mass compared to the norm, 4 degrees of obesity
- 96. The two commonly affected organs are the heart and the pancreas. Subepicardial fat covers the heart
- 97. According to the etiology the following types of obesity are defined: 1. Primary (idiopathic); 2. Secondary.
- 98. According to the patient's appearance, obesity may be 1. Symmetrical 2. Upper 3. Medial 4. Lower.
- 99. In hypertrophic type adipose tissue enlarges due to increased volume of fatty cells, in hyperplastic due
- 100. A 45-year old man died of sudden cardiac arrest. Symmetrical stage III obesity, rupture of the
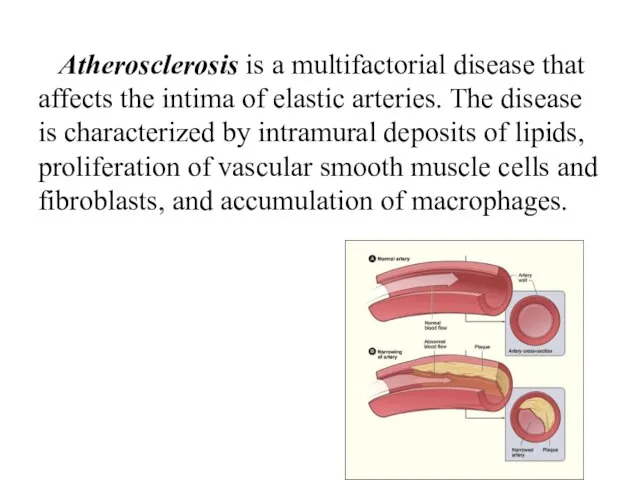
- 102. Atherosclerosis is a multifactorial disease that affects the intima of elastic arteries. The disease is characterized
- 103. Accumulations of proteins
- 104. A granular degeneration (dystrophy). Macroscopical kind of organs at this dystrophy it is determined as “muddy
- 105. Hyaline-drop degeneration is characterized by the aggregation of small proteins granules into cytoplasm of cells. It
- 106. Hydropic (cloudy, vacuolar, balloon) Is characterized by accumulation of water within the cell due to cytoplasmic
- 107. These vacuoles represent distended cisternas of the endoplasmic reticulum. Ultrastructural changes in hydropic swelling include the
- 108. Microscopy of the kidneys from the dead patient who had suffered from chronic glomerulonephritis showed enlarged
- 109. Keratoid (horney) degeneration Is characterized by increase production of keratin substance. This process may be local
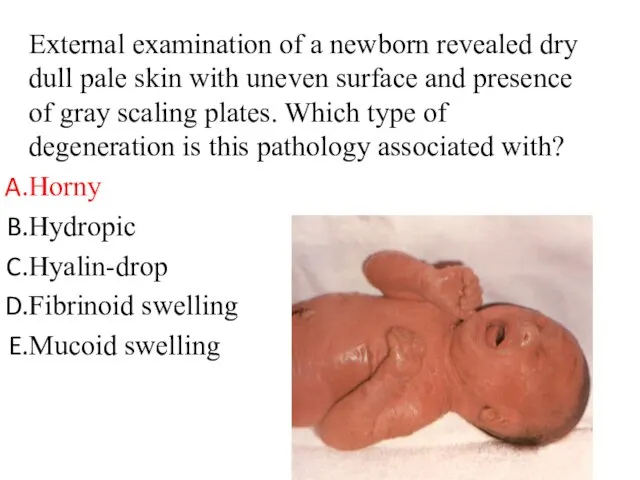
- 110. External examination of a newborn revealed dry dull pale skin with uneven surface and presence of
- 111. Mescnchymal (stromal vascular) degenerations develop in the connective tissue as a result of metabolic disturbances in
- 112. 1. Mucoid swelling Mucoid swelling is superficial reversible disorganization of the connective tissue. These processes are
- 113. Histology of the deformed mitral valve revealed marked basophilic reaction at staining with hematoxylin-eosin of the
- 114. 2. Fibrinoid changes Fibrinoid swelling is deep irreversible connective tissue disorganization. Fibrinoid is formed as a
- 115. Skin biopsy of the patient with allergic vasculitis demonstrated a thickened homogenic, pyroninophilic vascular walls at
- 116. 3. Hyaline changes (hyalinosis) Hyaline changes (hyalinosis) - (greek “hyalos” - transparent, glass-like) usually refers to
- 117. Autopsy of the man revealed the signs of rheumatic heart defect, i.e. thickened deformed cartilage-like valves
- 118. Amyloidosis is the term used for a group of diseases characterised by extracellular deposition of fibrillar
- 119. A patient ages 42 had suffered from bronchiectasis and died of renal failure. Autopsy revealed enlarged
- 120. Autopsy of a man aged 56 who had suffered from fibrous-cavernous pulmonary tuberculosis revealed enlarged dense
- 122. Скачать презентацию
Слайд 2Cells
Cells are active participants in their environment, constantly adjusting their structure
Cells
Cells are active participants in their environment, constantly adjusting their structure
Слайд 3CELLULAR ADAPTATIONS
As cells encounter physiologic stresses or pathologic stimuli, they can
CELLULAR ADAPTATIONS
As cells encounter physiologic stresses or pathologic stimuli, they can
Слайд 4CELLULAR ADAPTATIONS
Broadly speaking, such physiologic and pathologic adaptations occur by
Decreasing or
CELLULAR ADAPTATIONS
Broadly speaking, such physiologic and pathologic adaptations occur by
Decreasing or
Слайд 5Cells may adapt to a pathological (disease) stimulus by extending the three
Cells may adapt to a pathological (disease) stimulus by extending the three
Слайд 7Atrophy
Atrophy means reduction of the number and size of cells, tissues and
Atrophy
Atrophy means reduction of the number and size of cells, tissues and
Слайд 8A. Physiologic atrophy. It is a normal process of aging in some
A. Physiologic atrophy. It is a normal process of aging in some
Слайд 10Atrophy
Atrophy
Слайд 12B. Pathologic atrophy may be general and local.
General atrophy is observed in
B. Pathologic atrophy may be general and local.
General atrophy is observed in
Слайд 13Gross appearance of patients occurs:
Sharp exhaustion.
Adipose tissue is decreased and it has
Gross appearance of patients occurs:
Sharp exhaustion.
Adipose tissue is decreased and it has
Слайд 14Histologically:
Cells become smaller in size but are not dead cells.
Shrinkage in cell
Histologically:
Cells become smaller in size but are not dead cells.
Shrinkage in cell
Слайд 15Hypertrophy refers to an increase in the size of parenchymal resulting in
Hypertrophy refers to an increase in the size of parenchymal resulting in
Слайд 16Mechanisms of hypertrophy
The increased size of the cells is due not to
Mechanisms of hypertrophy
The increased size of the cells is due not to
Слайд 17 True hypertrophy (hyperplasia)
has adaptative and compensative characteristics and may be:
physiologic
pathologic
True hypertrophy (hyperplasia)
has adaptative and compensative characteristics and may be:
physiologic
pathologic
Слайд 18A. Physiologic hypertrophy (hyperplasia).
1. Neurogumoral (hormonal) hypertrophy: hypertrophy of female breast at
A. Physiologic hypertrophy (hyperplasia).
1. Neurogumoral (hormonal) hypertrophy: hypertrophy of female breast at
Слайд 21B. Pathologic hypertrophy (hyperplasia).
Neurogumoral hypertrophy develops due to impairment of
endocrine functions.
B. Pathologic hypertrophy (hyperplasia).
Neurogumoral hypertrophy develops due to impairment of
endocrine functions.
Слайд 223. Compensatory reparative hypertrophy: regeneration of the liver following partial hepatectomy, regeneration
3. Compensatory reparative hypertrophy: regeneration of the liver following partial hepatectomy, regeneration
Слайд 24 According to stage of adaptation two types of myocardial hypertrophy have
According to stage of adaptation two types of myocardial hypertrophy have
Слайд 25myocardial hypertrophy
myocardial hypertrophy
Слайд 26Metaplasia
Metaplasia is defined as a reversible change of one type to
Metaplasia
Metaplasia is defined as a reversible change of one type to
Слайд 27Epithelial metaplasia
This is the more common type. The metaplastic changes may
Epithelial metaplasia
This is the more common type. The metaplastic changes may
Слайд 29
Mezenhymal metaplasia.
Transformation of one adult type of mesenchymal tissue to another.
Osseous
Mezenhymal metaplasia.
Transformation of one adult type of mesenchymal tissue to another.
Osseous
Слайд 31Dysplasia
Dysplasia means “disordered cellular development”, often accompanied with metaplasia and hyperplasia, it
Dysplasia
Dysplasia means “disordered cellular development”, often accompanied with metaplasia and hyperplasia, it
Слайд 36 If the adaptive capability is exceeded or if the external stress
If the adaptive capability is exceeded or if the external stress
Слайд 37IRREVERSIBLE CELLULAR INJURY:
Cell death is a state of irreversible injury. It may
IRREVERSIBLE CELLULAR INJURY:
Cell death is a state of irreversible injury. It may
Слайд 38Cell death is
One of the most crucial events in the
Cell death is
One of the most crucial events in the
Слайд 39Autolysis (“self-digestion”)
Is disintegration of the cell by its own hydrolytic enzymes
Autolysis (“self-digestion”)
Is disintegration of the cell by its own hydrolytic enzymes
Слайд 40Necrosis
Is celullar death in the living body in the disease. Necrosis is
Necrosis
Is celullar death in the living body in the disease. Necrosis is
Слайд 41Nuclear changes. The irreversibly damaged nuclei are characterized by one of the
Nuclear changes. The irreversibly damaged nuclei are characterized by one of the
Слайд 43At electron microscopic level
In addition to the above nuclear changes, disorganization and
At electron microscopic level
In addition to the above nuclear changes, disorganization and
Слайд 44Karyorrhexis
Karyorrhexis
Слайд 45Karyolysis
Karyolysis
Слайд 46The presence of the grains of chromatin in a focus of caseous
The presence of the grains of chromatin in a focus of caseous
Слайд 47Stages of necrosis (or morphogenesis):
1. Paranecrosis - reversible changes; as a rule,
Stages of necrosis (or morphogenesis):
1. Paranecrosis - reversible changes; as a rule,
Слайд 48Types of necrosis
According to the mechanisms of development:
1. Direct (from influence of
Types of necrosis
According to the mechanisms of development:
1. Direct (from influence of
Слайд 49Types of necrosis
According to the cause:
1. Traumatic.
2. Toxic.
3. Trophoneurotic.
4. Allergic.
5. Vascular or
Types of necrosis
According to the cause:
1. Traumatic.
2. Toxic.
3. Trophoneurotic.
4. Allergic.
5. Vascular or
Слайд 50
Coagulative necrosis
Is associated with inhibition of lytic enzymes. Foci
Coagulative necrosis
Is associated with inhibition of lytic enzymes. Foci
Слайд 51Coagulative necrosis
Coagulative necrosis
Слайд 52Liver: normal and necrosis There are signs of damage to the living
Liver: normal and necrosis There are signs of damage to the living
Слайд 53Zenker’s degeneration.Specimen is colored by Malori’s technique. Muscle fibers are fragmented, sarcoplasm is homogenous, looks
Zenker’s degeneration.Specimen is colored by Malori’s technique. Muscle fibers are fragmented, sarcoplasm is homogenous, looks
Слайд 54Liquefactive (colliquative) necrosis
Is marked by dissolution of tissue due to
Liquefactive (colliquative) necrosis
Is marked by dissolution of tissue due to
Слайд 55Liquefactive (colliquative) necrosis
Liquefactive (colliquative) necrosis
Слайд 56Fig. 1. Histologically, Colliquation Necroses Are Observed, Mainly In The White Brain Substance
Fig. 1. Histologically, Colliquation Necroses Are Observed, Mainly In The White Brain Substance
Слайд 57Liquefactive (colliquative) necrosis
Liquefactive (colliquative) necrosis
Слайд 58Gangrene
develops in organs and tissues having contact with environment. The most
Gangrene
develops in organs and tissues having contact with environment. The most
Слайд 59Dry gangrene
Dry gangrene
Слайд 60Wet gangrene
Wet gangrene

Слайд 61Gas gangrene
Gas gangrene

Слайд 62Gangrene does not appear in…
Skin
Kidney
Lungs
Uterus
Intestine (bowel)
Gangrene does not appear in…
Skin
Kidney
Lungs
Uterus
Intestine (bowel)
Слайд 63On autopsy it is revealed enlarged dense right lung, fibrin layers on
On autopsy it is revealed enlarged dense right lung, fibrin layers on
Слайд 64A patient with diabetes mellitus suddenly began having sharp pain in his
A patient with diabetes mellitus suddenly began having sharp pain in his
Слайд 65In 77-year-old patient suffered with atherosclerosis the pain has appeared in the
In 77-year-old patient suffered with atherosclerosis the pain has appeared in the
Слайд 66The examination of the child with measles showed the non-clear border edematous
The examination of the child with measles showed the non-clear border edematous
Слайд 67Infarction – vascular or ischemic necrosis.
Infarction – vascular or ischemic necrosis.
Слайд 68A patient died from acute cardiac insufficiency. The histological examination of his
A patient died from acute cardiac insufficiency. The histological examination of his
Слайд 69Infarction is…
Hyperemia
Stasis
Ichemical necrosis
Secquestrum
Degeneration
Infarction is…
Hyperemia
Stasis
Ichemical necrosis
Secquestrum
Degeneration
Слайд 70A 65-year-old patient, who suffered from arteriosclerosis, has been hospitalized in surgical
A 65-year-old patient, who suffered from arteriosclerosis, has been hospitalized in surgical
Слайд 71Fat necrosis
is encountered in adipose tissue contiguous to the pancreas and
Fat necrosis
is encountered in adipose tissue contiguous to the pancreas and
Слайд 72Fat necrosis of the pancreas
Fat necrosis of the pancreas
Слайд 73Caseous necrosis
Has features of both coagulative and liquefactive necrosis. Typically, it
Caseous necrosis
Has features of both coagulative and liquefactive necrosis. Typically, it
Слайд 74Caseous necrosis
Caseous necrosis
Слайд 75Fibrinoid necrosis
Is characterised by deposition of fibrin-like material, which has
Fibrinoid necrosis
Is characterised by deposition of fibrin-like material, which has
Слайд 76Fibrinoid necrosis
Fibrinoid necrosis
Слайд 78Outcomes of necrosis
Regeneration of tissues – replacement of the dead tissue with
Outcomes of necrosis
Regeneration of tissues – replacement of the dead tissue with
Слайд 79Sequester – fragment of dead tissue, which can’t be autolized, replaced by
Sequester – fragment of dead tissue, which can’t be autolized, replaced by
Слайд 80Apoptosis
Is a programmed (physiological) death of the cell in the living body.
Morphologic
Apoptosis
Is a programmed (physiological) death of the cell in the living body.
Morphologic
Слайд 81Histologically
In tissues stained with hematoxylin and eosin, apoptotic involves single cells or
Histologically
In tissues stained with hematoxylin and eosin, apoptotic involves single cells or
Слайд 83Mechanisms of the development of intra- and extracellular (stromal) degenerations (dystrophies) are
Mechanisms of the development of intra- and extracellular (stromal) degenerations (dystrophies) are
Слайд 84Intracellular fatty degenerations
For identification of different kind of fats we usually use
Intracellular fatty degenerations
For identification of different kind of fats we usually use
Слайд 85Disturbance of fat metabolism may manifest as:
appearance in the place where it
Disturbance of fat metabolism may manifest as:
appearance in the place where it
Слайд 86Fatty degeneration of the liver
Macroscopically the fatty liver is enlarged with rounded
Fatty degeneration of the liver
Macroscopically the fatty liver is enlarged with rounded
Слайд 87“goose liver”
“goose liver”
Слайд 88“goose liver”
“goose liver”
Слайд 89Autopsy of the patient who had suffered from tuberculosis demonstrated that the
Autopsy of the patient who had suffered from tuberculosis demonstrated that the
Слайд 90Fatty degeneration of the heart
It is also called “Tiger’s” heart.
Macroscopically the heart
Fatty degeneration of the heart
It is also called “Tiger’s” heart.
Macroscopically the heart
Слайд 91External examination of a newborn revealed dry dull pale skin Autopsy of
External examination of a newborn revealed dry dull pale skin Autopsy of
Слайд 92Autopsy of the patient who had suffered from hypertension disease revealed considerable
Autopsy of the patient who had suffered from hypertension disease revealed considerable
Слайд 93The kidneys look like “large white kidney”. They are enlarged, flabby. The
The kidneys look like “large white kidney”. They are enlarged, flabby. The
Слайд 94Stromal fatty infiltration is the deposition of mature adipose cells in the
Stromal fatty infiltration is the deposition of mature adipose cells in the
Слайд 95Depending on the excess of the patient mass compared to the norm,
Depending on the excess of the patient mass compared to the norm,
Слайд 96The two commonly affected organs are the heart and the pancreas.
Subepicardial fat
The two commonly affected organs are the heart and the pancreas.
Subepicardial fat
Слайд 97According to the etiology the following types of obesity are defined:
1. Primary
According to the etiology the following types of obesity are defined:
1. Primary
Слайд 98According to the patient's appearance, obesity may be
1. Symmetrical
2. Upper
3.
According to the patient's appearance, obesity may be
1. Symmetrical
2. Upper
3.
Слайд 99In hypertrophic type adipose tissue enlarges due to increased volume of fatty
In hypertrophic type adipose tissue enlarges due to increased volume of fatty
Слайд 100A 45-year old man died of sudden cardiac arrest. Symmetrical stage III
A 45-year old man died of sudden cardiac arrest. Symmetrical stage III

Слайд 102 Atherosclerosis is a multifactorial disease that affects the intima of elastic
Atherosclerosis is a multifactorial disease that affects the intima of elastic
Слайд 103Accumulations of proteins
Accumulations of proteins
Слайд 104A granular degeneration (dystrophy).
Macroscopical kind of organs at this dystrophy it is
A granular degeneration (dystrophy).
Macroscopical kind of organs at this dystrophy it is
Слайд 105Hyaline-drop degeneration
is characterized by the aggregation of small proteins granules
Hyaline-drop degeneration
is characterized by the aggregation of small proteins granules
Слайд 106Hydropic (cloudy, vacuolar, balloon)
Is characterized by accumulation of water within the cell
Hydropic (cloudy, vacuolar, balloon)
Is characterized by accumulation of water within the cell
Слайд 107These vacuoles represent distended cisternas of the endoplasmic reticulum. Ultrastructural changes in
These vacuoles represent distended cisternas of the endoplasmic reticulum. Ultrastructural changes in
Слайд 108Microscopy of the kidneys from the dead patient who had suffered from
Microscopy of the kidneys from the dead patient who had suffered from
Слайд 109Keratoid (horney) degeneration
Is characterized by increase production of keratin substance. This
Keratoid (horney) degeneration
Is characterized by increase production of keratin substance. This
Слайд 110External examination of a newborn revealed dry dull pale skin with uneven
External examination of a newborn revealed dry dull pale skin with uneven
Слайд 111Mescnchymal (stromal vascular) degenerations develop in the connective tissue as a result
Mescnchymal (stromal vascular) degenerations develop in the connective tissue as a result
Слайд 1121. Mucoid swelling
Mucoid swelling is superficial reversible disorganization of the connective tissue.
These
1. Mucoid swelling
Mucoid swelling is superficial reversible disorganization of the connective tissue.
These
Слайд 113Histology of the deformed mitral valve revealed marked basophilic reaction at staining
Histology of the deformed mitral valve revealed marked basophilic reaction at staining
Слайд 1142. Fibrinoid changes
Fibrinoid swelling is deep irreversible connective tissue disorganization.
Fibrinoid is formed
2. Fibrinoid changes
Fibrinoid swelling is deep irreversible connective tissue disorganization.
Fibrinoid is formed
Слайд 115Skin biopsy of the patient with allergic vasculitis demonstrated a thickened homogenic,
Skin biopsy of the patient with allergic vasculitis demonstrated a thickened homogenic,
Слайд 1163. Hyaline changes (hyalinosis)
Hyaline changes (hyalinosis) - (greek “hyalos” - transparent, glass-like)
3. Hyaline changes (hyalinosis)
Hyaline changes (hyalinosis) - (greek “hyalos” - transparent, glass-like)
Слайд 117Autopsy of the man revealed the signs of rheumatic heart defect, i.e.
Autopsy of the man revealed the signs of rheumatic heart defect, i.e.
Слайд 118Amyloidosis is the term used for a group of diseases characterised by
Amyloidosis is the term used for a group of diseases characterised by
Слайд 119A patient ages 42 had suffered from bronchiectasis and died of renal
A patient ages 42 had suffered from bronchiectasis and died of renal
Слайд 120Autopsy of a man aged 56 who had suffered from fibrous-cavernous pulmonary
Autopsy of a man aged 56 who had suffered from fibrous-cavernous pulmonary
 organizatsionaya_struktura1
organizatsionaya_struktura1 Деление на двузначное число
Деление на двузначное число Презентация на тему Подготовка к сочинению. Описание местности
Презентация на тему Подготовка к сочинению. Описание местности Маслий Варвара
Маслий Варвара Муниципальный опорный центр дополнительного образования детей Новоселовского района (МОЦ)
Муниципальный опорный центр дополнительного образования детей Новоселовского района (МОЦ) Акции как объект инвестирования средств. Роль и значение для российских компаний
Акции как объект инвестирования средств. Роль и значение для российских компаний Механическая обработка овощей
Механическая обработка овощей Моя комната My room
Моя комната My room 3 день презентация
3 день презентация М.Ю. Лермонтов Герои нашего времени
М.Ю. Лермонтов Герои нашего времени Информационные
Информационные Портфолио рерайтера
Портфолио рерайтера Министерство сельского хозяйства Ульяновской области МЯСНЫЕ ПОРОДЫКРУПНОГО РОГАТОГО СКОТА
Министерство сельского хозяйства Ульяновской области МЯСНЫЕ ПОРОДЫКРУПНОГО РОГАТОГО СКОТА Якопо Робусти, более известный как Тинторе́тто (1518 или 1519 — 1594)
Якопо Робусти, более известный как Тинторе́тто (1518 или 1519 — 1594) Тренинговое занятие по профилактике наркомании
Тренинговое занятие по профилактике наркомании Модель Вертолёт(1)
Модель Вертолёт(1) Старт инициативной программы ИГУПИТна «площадке» г. Твери
Старт инициативной программы ИГУПИТна «площадке» г. Твери Тренинг_2016_DY
Тренинг_2016_DY Внешняя политика СССР и международные отношения в 30-е годы.
Внешняя политика СССР и международные отношения в 30-е годы. История коньков
История коньков МАРИНА ЦВЕТАЕВА. ОЧЕРКИ ЖИЗНИ.
МАРИНА ЦВЕТАЕВА. ОЧЕРКИ ЖИЗНИ. Сказка мудростью богата
Сказка мудростью богата РЛизингПрезентация компании
РЛизингПрезентация компании Разметка заготовок из древесины
Разметка заготовок из древесины Презентация на тему Самые большие птицы
Презентация на тему Самые большие птицы ИТ-инфраструктура предприятия. Процессы управление конфигурациями и управление изменениями
ИТ-инфраструктура предприятия. Процессы управление конфигурациями и управление изменениями Презентация на тему Метод координат
Презентация на тему Метод координат  Анатомия и морфология растений
Анатомия и морфология растений