- Cervix and uteri cancer during pregnancy

Содержание
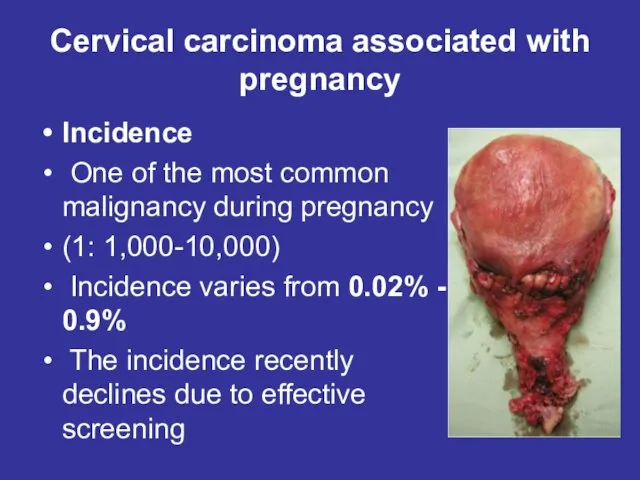
- 2. Cervical carcinoma associated with pregnancy Incidence One of the most common malignancy during pregnancy (1: 1,000-10,000)
- 3. Physiological changes during pregnancy in the mucous membrane of the cervix In the I trimester of
- 4. Symptoms and signs of cervical cancer during pregnancy Early cervical cancer often doesn’t have any noticeable
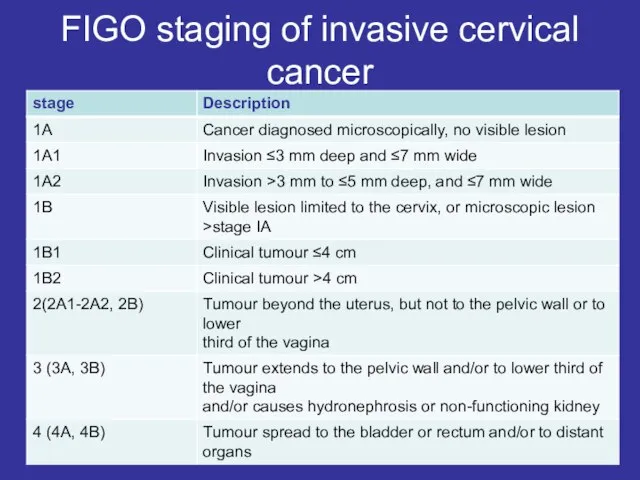
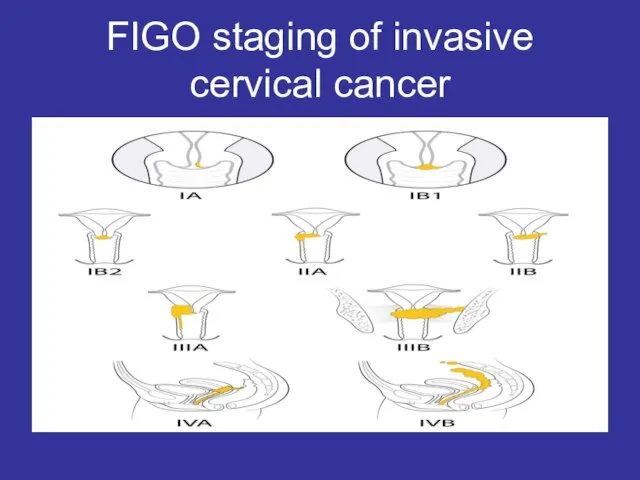
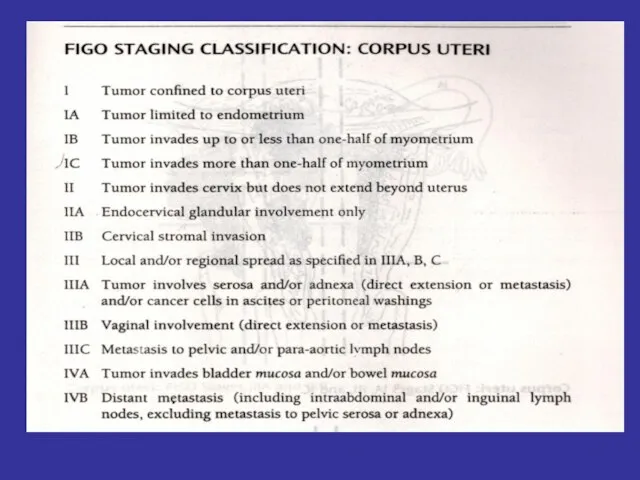
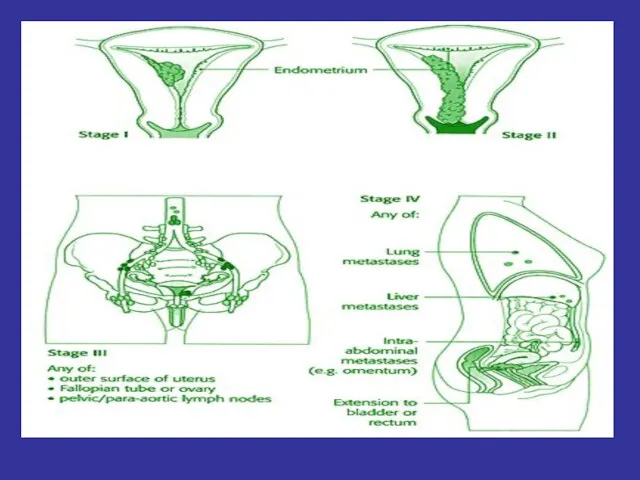
- 5. FIGO staging of invasive cervical cancer
- 6. FIGO staging of invasive cervical cancer
- 7. Treatment of cervical cancer during pregnancy The decision to continue the pregnancy should be based on
- 8. Treatment of intraepithelial cervical cancer (in situ) I trimester If patient don’t want to continue her
- 9. Treatment of microinvasive cervical cancer I trimester If patient wish to continue the pregnancy, but if
- 10. Treatment of cervical IA2, II stages In the case of diagnosis before 20 weeks of gestation,
- 11. Treatment of cervical IB, II stages I trimester The radical hysterectomy with iliac lymphadenectomy + 2-3
- 12. Treatment of cervical cancer III, IV stages: I trimester I. External irradiation, after spontaneous abortion (at
- 13. Endometrial carcinoma
- 17. Cancer During Pregnancy Cancer during pregnancy is uncommon. It occurs in only about one out of
- 18. Diagnosing cancer during pregnancy Being pregnant may delay a cancer diagnosis. This is because some cancer
- 19. Cancer treatment during pregnancy When making treatment decisions for cancer during pregnancy, it is important to
- 20. Treatment recommendations are based on many factors, including the following Stage of the pregnancy The type,
- 21. Treatment must be carefully planned to ensure the woman and unborn baby are safe. In general,
- 22. Treatments that may be used during pregnancy Surgery is the removal of the tumor and some
- 23. Chemotherapy. There is a risk of harm to the fetus if chemotherapy is given in the
- 24. During the second and third trimesters, doctors can give several types of chemotherapy without apparent risk
- 25. Radiation therapy. Radiation therapy is the use of high-energy x-rays to destroy cancer cells. Because radiation
- 26. Breastfeeding during treatment Doctors advise women who are receiving chemotherapy after a pregnancy not to breastfeed.
- 28. Скачать презентацию
Слайд 2Cervical carcinoma associated with
pregnancy
Incidence
One of the most common malignancy during
Cervical carcinoma associated with
pregnancy
Incidence
One of the most common malignancy during
Слайд 3Physiological changes during pregnancy in the mucous membrane of the cervix
In the
Physiological changes during pregnancy in the mucous membrane of the cervix
In the
Слайд 4Symptoms and signs of cervical cancer during pregnancy
Early cervical cancer often doesn’t
Symptoms and signs of cervical cancer during pregnancy
Early cervical cancer often doesn’t
Слайд 5FIGO staging of invasive cervical cancer
FIGO staging of invasive cervical cancer
Слайд 6FIGO staging of invasive cervical cancer
FIGO staging of invasive cervical cancer
Слайд 7Treatment of cervical cancer during pregnancy
The decision to continue the pregnancy should
Treatment of cervical cancer during pregnancy
The decision to continue the pregnancy should
Слайд 8Treatment of intraepithelial cervical cancer (in situ)
I trimester
If patient don’t want to
Treatment of intraepithelial cervical cancer (in situ)
I trimester
If patient don’t want to
Слайд 9Treatment of microinvasive cervical cancer
I trimester
If patient wish to continue the
Treatment of microinvasive cervical cancer
I trimester
If patient wish to continue the
Слайд 10Treatment of cervical IA2, II stages
In the case of diagnosis before 20
Treatment of cervical IA2, II stages
In the case of diagnosis before 20
Слайд 11Treatment of cervical IB, II stages
I trimester
The radical hysterectomy with
Treatment of cervical IB, II stages
I trimester
The radical hysterectomy with
Слайд 12Treatment of cervical cancer III, IV stages:
I trimester
I. External irradiation, after
Treatment of cervical cancer III, IV stages:
I trimester
I. External irradiation, after
Слайд 13Endometrial carcinoma
Endometrial carcinoma

Слайд 17Cancer During Pregnancy
Cancer during pregnancy is uncommon. It occurs in only about
Cancer During Pregnancy
Cancer during pregnancy is uncommon. It occurs in only about
Слайд 18Diagnosing cancer during pregnancy
Being pregnant may delay a cancer diagnosis. This is
Diagnosing cancer during pregnancy
Being pregnant may delay a cancer diagnosis. This is
Слайд 19Cancer treatment during pregnancy
When making treatment decisions for cancer during pregnancy, it
Cancer treatment during pregnancy
When making treatment decisions for cancer during pregnancy, it
Слайд 20Treatment recommendations are based on many factors, including the following
Stage of the
Treatment recommendations are based on many factors, including the following
Stage of the
Слайд 21Treatment must be carefully planned to ensure the woman and unborn baby
Treatment must be carefully planned to ensure the woman and unborn baby
Слайд 22Treatments that may be used during pregnancy
Surgery is the removal of the tumor
Treatments that may be used during pregnancy
Surgery is the removal of the tumor
Слайд 23Chemotherapy.
There is a risk of harm to the fetus if chemotherapy is
Chemotherapy.
There is a risk of harm to the fetus if chemotherapy is
Слайд 24During the second and third trimesters, doctors can give several types of
During the second and third trimesters, doctors can give several types of
Слайд 25Radiation therapy.
Radiation therapy is the use of high-energy x-rays to destroy cancer cells.
Radiation therapy.
Radiation therapy is the use of high-energy x-rays to destroy cancer cells.
Слайд 26Breastfeeding during treatment
Doctors advise women who are receiving chemotherapy after a pregnancy
Breastfeeding during treatment
Doctors advise women who are receiving chemotherapy after a pregnancy
 Идейно-художественное своеобразие произведения М.Ю. Лермонтова
Идейно-художественное своеобразие произведения М.Ю. Лермонтова Презентация на тему Гигиена органа слуха
Презентация на тему Гигиена органа слуха Площадь прямоугольного треугольника: алгоритм нахождения площади треугольника
Площадь прямоугольного треугольника: алгоритм нахождения площади треугольника Определение права, размера и сроков назначения трудовых пенсий
Определение права, размера и сроков назначения трудовых пенсий Коммерческое предложение от Laika Logistics
Коммерческое предложение от Laika Logistics СПИД Синдром приобретённого иммунного дефицита
СПИД Синдром приобретённого иммунного дефицита Статья 5. Никто не должен подвергаться пыткам или жестоким, бесчеловечным или унижающим достоинство обращению и наказанию
Статья 5. Никто не должен подвергаться пыткам или жестоким, бесчеловечным или унижающим достоинство обращению и наказанию Шрифтовая графика и типографика. Портфолио учебных работ
Шрифтовая графика и типографика. Портфолио учебных работ Марина Ивановна Цветаева. Биография поэта и поэтическое творчество
Марина Ивановна Цветаева. Биография поэта и поэтическое творчество Появился заказчик. Что делать?
Появился заказчик. Что делать? Причинно-следственный анализ
Причинно-следственный анализ Графическая работа. Проекции группы тел
Графическая работа. Проекции группы тел ФРАНЦИЯ
ФРАНЦИЯ People. Фотоальбом
People. Фотоальбом Сочинение по картине Ивана Ивановича Фирсова «Юный живописец»
Сочинение по картине Ивана Ивановича Фирсова «Юный живописец» powerpointstore.com_w57
powerpointstore.com_w57 Презентация на тему: «Похмелье»
Презентация на тему: «Похмелье» Государство, его признаки и формы
Государство, его признаки и формы Команда B2O
Команда B2O Бала құқықтары туралы
Бала құқықтары туралы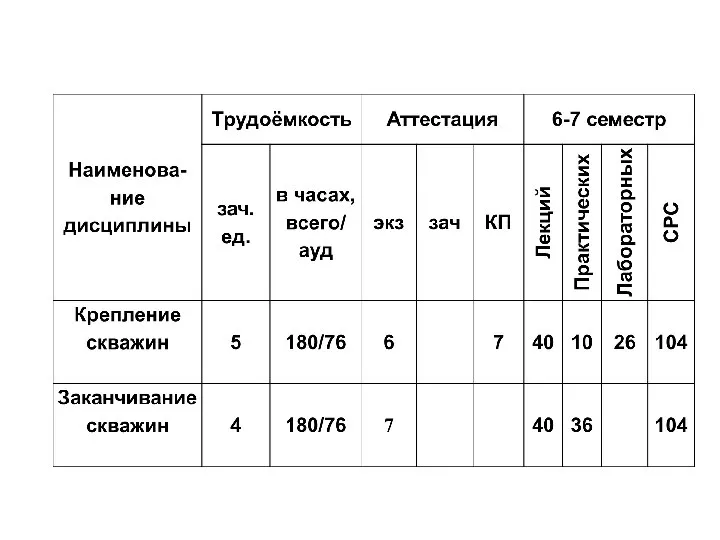 Крепление скважин
Крепление скважин Приложение №8 к административному регламенту
Приложение №8 к административному регламенту Команда Вознесенской школы впервые участвовавшая в краевых ( восточная зона) соревнованиях.
Команда Вознесенской школы впервые участвовавшая в краевых ( восточная зона) соревнованиях. «Опыт создания и деятельность Объединения РаЭл»
«Опыт создания и деятельность Объединения РаЭл» Школа панацея 17.09.2020
Школа панацея 17.09.2020 Тема проекта:«Как человек использует свойства воды?»
Тема проекта:«Как человек использует свойства воды?» Презентация на тему Насекомые рекордсмены
Презентация на тему Насекомые рекордсмены  Буквы Е и И в приставках НЕ - и НИ - отрицательных наречий
Буквы Е и И в приставках НЕ - и НИ - отрицательных наречий