- Clinical Case Conference

Содержание
- 2. HPI 17 year old female presents with a 6 day history of increasing fatigue and diffuse
- 3. PMHx Epilepsy (GTC) since 8 years old Medications: Zonisamide, Trileptal Allergies: Tegretol (rash) Family Hx Non-contributory
- 4. Laboratory Total bilirubin 25.2, conjugated 13 Total protein 5.1, albumin 2.8 Amylase 53, Lipase 45 Ammonia
- 5. Physical Exam General: tired, easily aroused HEENT: PERRLA, NCAT, icteric sclera CV: I/VI SEM at LSB,
- 6. Viral, bacterial and stool cultures sent Started Vitamin K and Ursodiol Repeat abdominal ultrasound Hepatosplenomegaly Normal
- 7. DIFFERENTIAL DIAGNOSIS
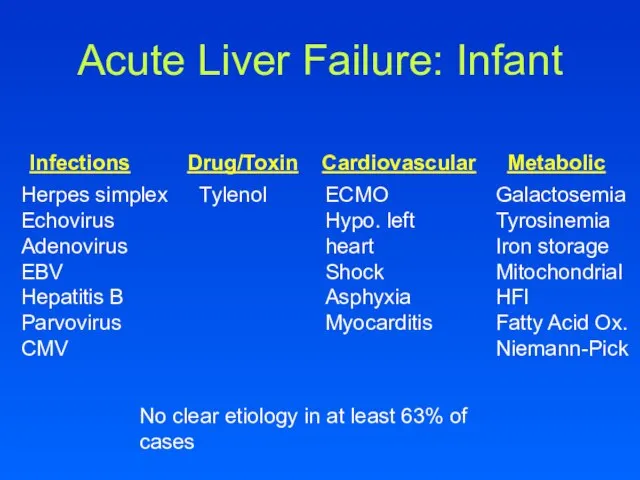
- 8. Acute Liver Failure: Infant Infections Drug/Toxin Cardiovascular Metabolic Herpes simplex Echovirus Adenovirus EBV Hepatitis B Parvovirus
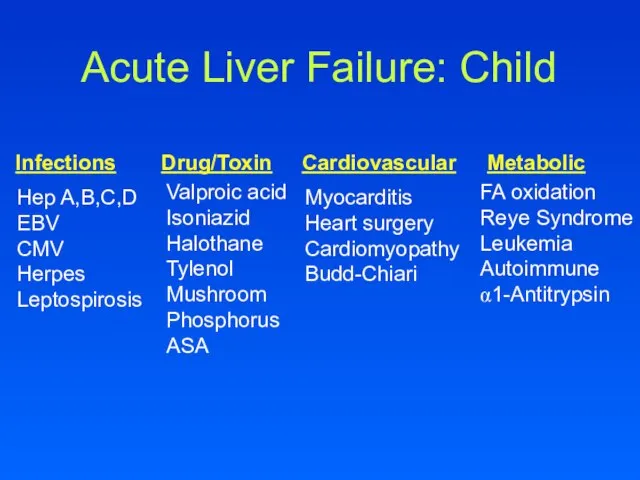
- 9. Acute Liver Failure: Child Infections Drug/Toxin Cardiovascular Metabolic Hep A,B,C,D EBV CMV Herpes Leptospirosis Valproic acid
- 10. Acute Liver Failure: The Adult Infections Drug/Toxin Cardiovascular Metabolic Hep A,B,C,D,E Yellow fever Dengue Fever Lassa
- 11. Hospital Course Hemoglobin steadily falling 11.7 to 8.8 Reticulocyte count 6.6% Increasing total bilirubin, peak 43.7
- 12. What would you do?
- 13. CMV, EBV negative Hepatitis A,B,C negative Autoimmune markers negative Copper 120 (nl) Ceruloplasmin 18 (low) Low
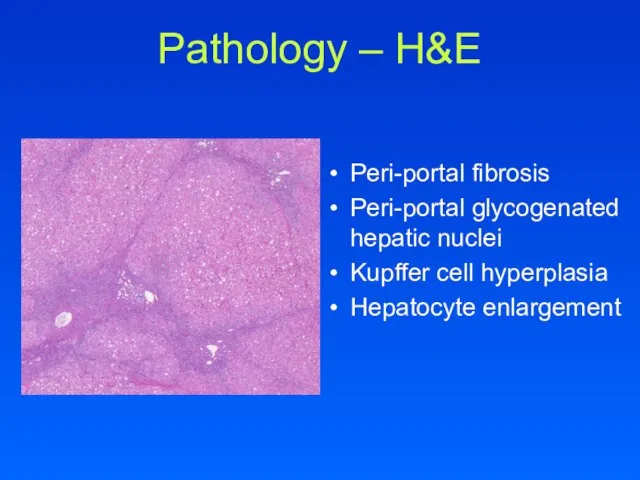
- 14. Pathology – H&E Peri-portal fibrosis Peri-portal glycogenated hepatic nuclei Kupffer cell hyperplasia Hepatocyte enlargement
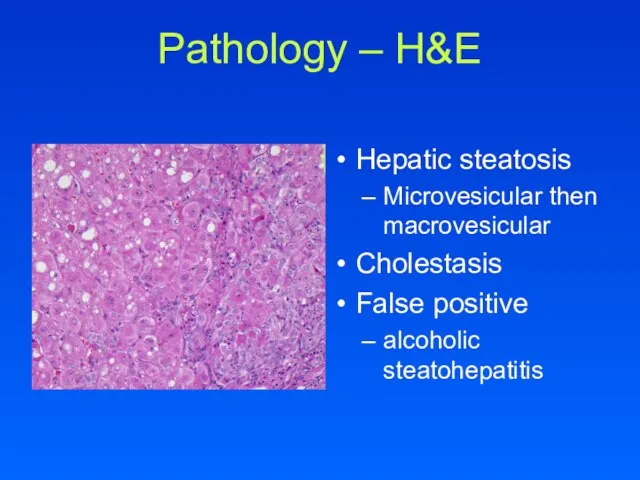
- 15. Pathology – H&E Hepatic steatosis Microvesicular then macrovesicular Cholestasis False positive alcoholic steatohepatitis
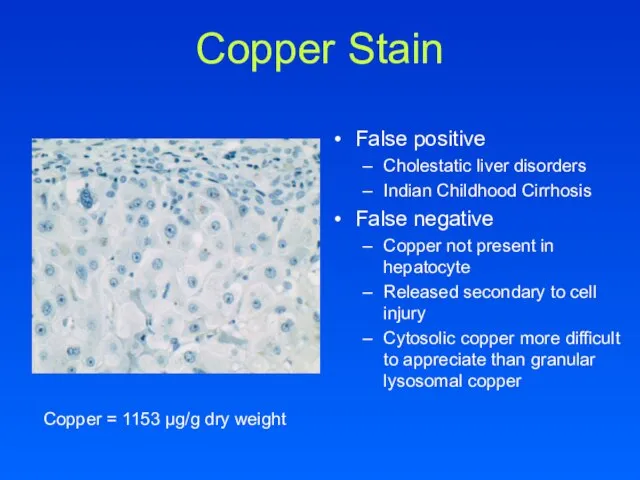
- 16. Copper Stain False positive Cholestatic liver disorders Indian Childhood Cirrhosis False negative Copper not present in
- 17. WILSON’S DISEASE
- 18. Copper Physiology Most abundant in unprocessed wheat, dried beans, peas, shellfish, chocolate, liver, kidney Impair copper
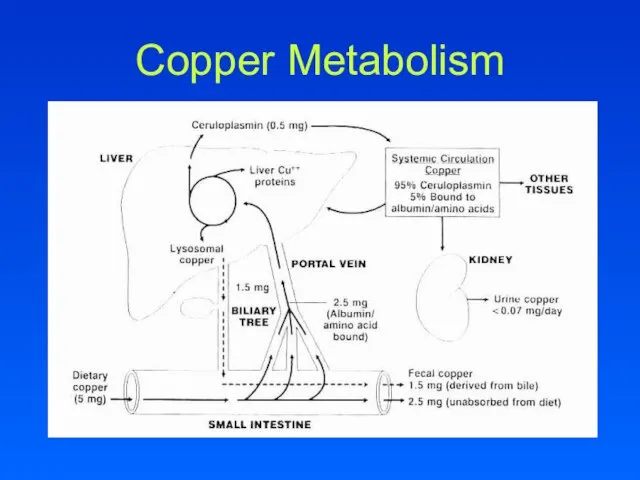
- 19. Copper Metabolism
- 20. Copper Metabolism Copper is transported into hepatocytes by the human copper transporter (hCTR) In hepatocyte, copper
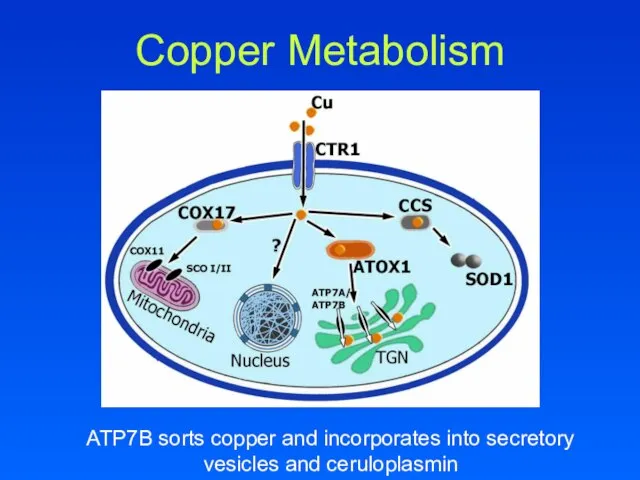
- 21. Copper Metabolism ATP7B sorts copper and incorporates into secretory vesicles and ceruloplasmin
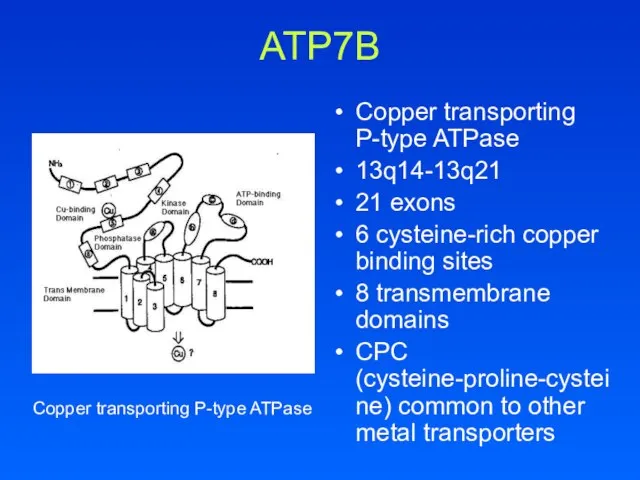
- 22. ATP7B Copper transporting P-type ATPase 13q14-13q21 21 exons 6 cysteine-rich copper binding sites 8 transmembrane domains
- 23. ATP7B >200 mutations identified Most small deletions or missense mutations Missense: neurologic and later presentation Deletions:
- 24. ATP7B Makes copper available for ceruloplasmin synthesis and transport of copper into vesicles Long-Evans Cinnamon (LEC)
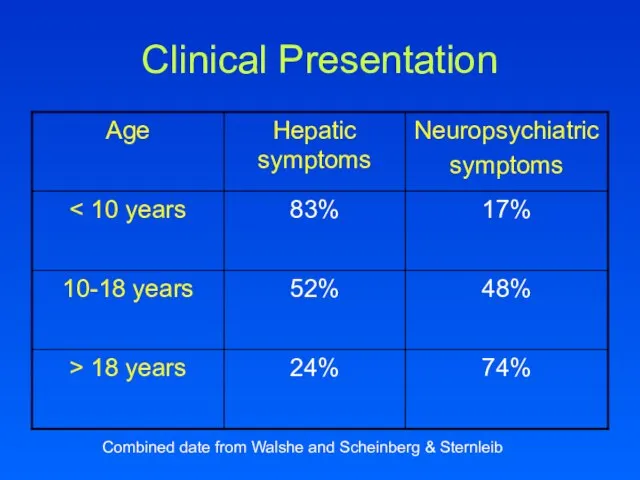
- 25. Clinical Presentation Combined date from Walshe and Scheinberg & Sternleib
- 26. Hepatic Acute hepatitis 25% Fulminant hepatic failure Liver transplant May also present after discontinuing copper chelation
- 27. Laboratory Mildly elevated serum aminotransferase levels Low alkaline phosphatase Serum alkaline phosphatase to total bilirubin ratio
- 28. Neuropsychiatric 40-45% as presentation Most common 2nd to 3rd decades of life Extrapyramidal and cerebrellar dysfunction
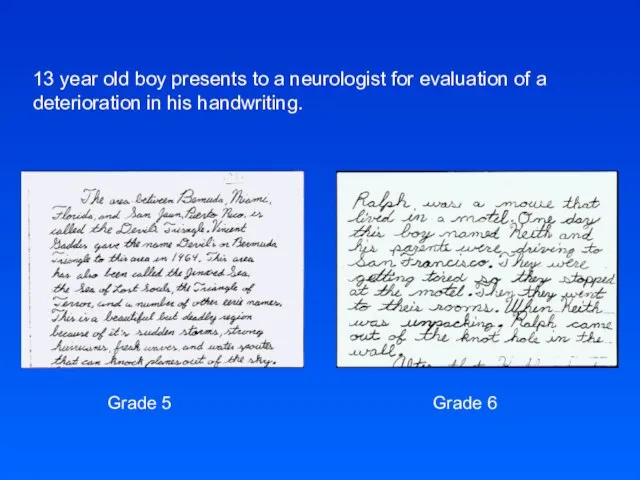
- 29. 13 year old boy presents to a neurologist for evaluation of a deterioration in his handwriting.
- 30. Imaging CT abnormalities 73% ventricular dilation 63% cortical atrophy 55% brainstem atrophy 45% hypodensity in basal
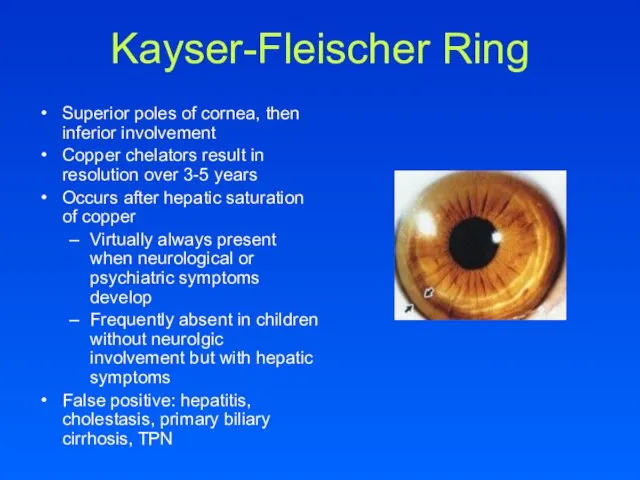
- 31. Kayser-Fleischer Ring Superior poles of cornea, then inferior involvement Copper chelators result in resolution over 3-5
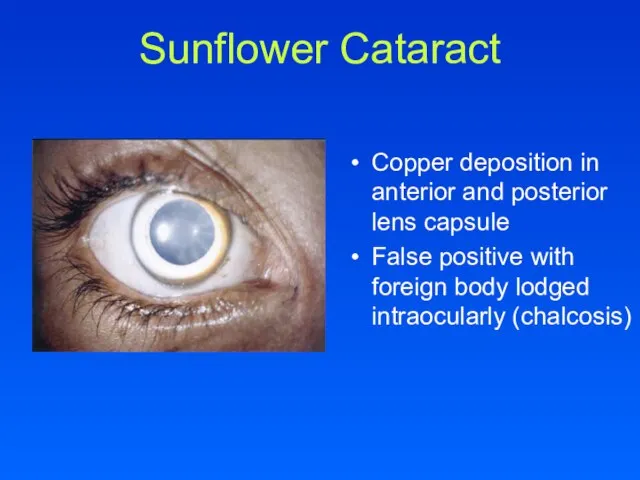
- 32. Sunflower Cataract Copper deposition in anterior and posterior lens capsule False positive with foreign body lodged
- 33. Other Renal Proximal renal tubular dysfunction (Fanconi’s syndrome) Renal insufficiency Nephrocalcinosis Hematologic Coombs negative hemolytic anemia
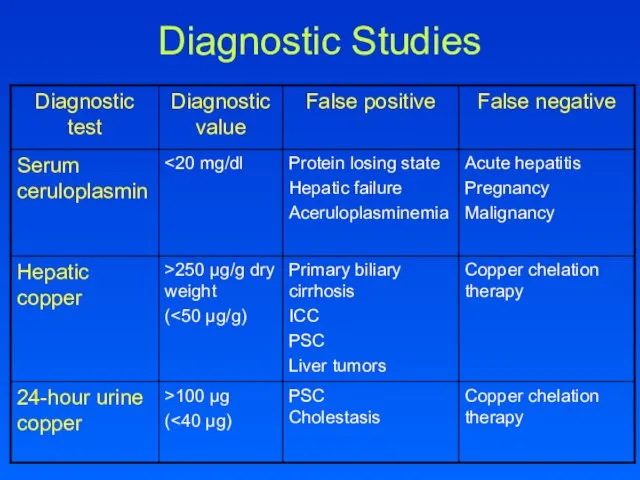
- 34. Diagnostic Studies
- 35. Genetic Analysis Genetic studies are becoming more available but limited Kumar et al characterized ATP7B mutations
- 36. Treatment Goals Reduce copper accumulation by Enhancing urinary excretion Decreasing intestinal absorption
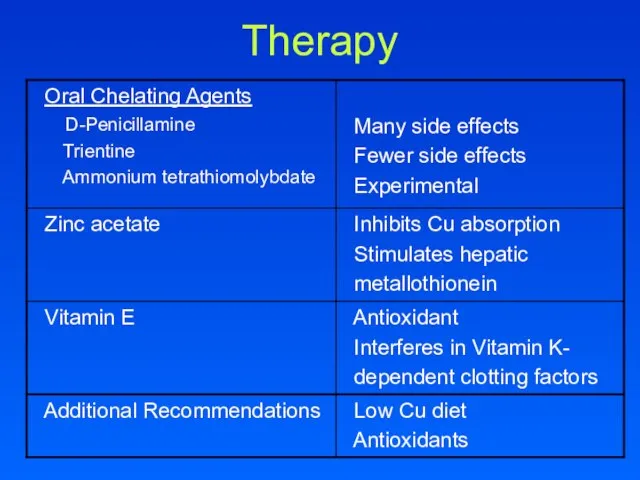
- 37. Therapy
- 38. Liver Transplant Life-saving Acute fulminant hepatic failure Decompensated cirrhosis with progressive end stage liver disease
- 39. Long-Evans Cinnamon Rats A deletion of 900 base pairs at the 3’ end of ATP7B gene,
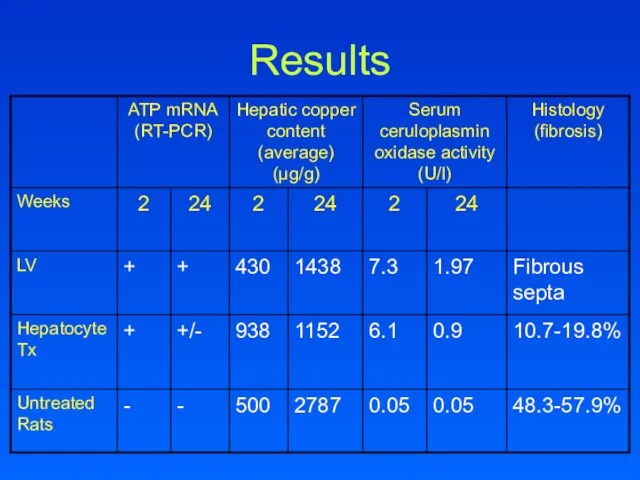
- 40. Results
- 41. Conclusions Liver copper levels were lowered in all treatment groups compared to untreated LEC rats Histological
- 42. Wilson’s Disease Wilson disease is a disorder of copper transport resulting in copper deposition in multiple
- 44. Bibliography Kumar et al. Familial gene analysis for Wilson disease from north-west Indian patients. Annals of
- 46. Скачать презентацию
Слайд 3PMHx
Epilepsy (GTC) since 8 years old
Medications: Zonisamide, Trileptal
Allergies: Tegretol (rash)
Family Hx
Non-contributory
Social
PMHx
Epilepsy (GTC) since 8 years old
Medications: Zonisamide, Trileptal
Allergies: Tegretol (rash)
Family Hx
Non-contributory
Social
Слайд 4Laboratory
Total bilirubin 25.2, conjugated 13
Total protein 5.1, albumin 2.8
Amylase 53, Lipase 45
Ammonia
Laboratory
Total bilirubin 25.2, conjugated 13
Total protein 5.1, albumin 2.8
Amylase 53, Lipase 45
Ammonia
Слайд 5Physical Exam
General: tired, easily aroused
HEENT: PERRLA, NCAT, icteric sclera
CV: I/VI SEM at
Physical Exam
General: tired, easily aroused
HEENT: PERRLA, NCAT, icteric sclera
CV: I/VI SEM at
Слайд 6Viral, bacterial and stool cultures sent
Started Vitamin K and Ursodiol
Repeat abdominal ultrasound
Hepatosplenomegaly
Normal
Viral, bacterial and stool cultures sent
Started Vitamin K and Ursodiol
Repeat abdominal ultrasound
Hepatosplenomegaly
Normal
Слайд 7DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
Слайд 8Acute Liver Failure: Infant
Infections Drug/Toxin Cardiovascular Metabolic
Herpes simplex
Echovirus
Adenovirus
EBV
Hepatitis B
Parvovirus
CMV
ECMO
Hypo. left heart
Shock
Asphyxia
Myocarditis
Galactosemia
Tyrosinemia
Iron storage
Mitochondrial
HFI
Fatty
Acute Liver Failure: Infant
Infections Drug/Toxin Cardiovascular Metabolic
Herpes simplex
Echovirus
Adenovirus
EBV
Hepatitis B
Parvovirus
CMV
ECMO
Hypo. left heart
Shock
Asphyxia
Myocarditis
Galactosemia
Tyrosinemia
Iron storage
Mitochondrial
HFI
Fatty
Слайд 9Acute Liver Failure: Child
Infections Drug/Toxin Cardiovascular Metabolic
Hep A,B,C,D
EBV
CMV
Herpes
Leptospirosis
Valproic acid
Isoniazid
Halothane
Tylenol
Mushroom
Phosphorus
ASA
Myocarditis
Heart surgery
Cardiomyopathy
Budd-Chiari
FA oxidation
Reye
Acute Liver Failure: Child
Infections Drug/Toxin Cardiovascular Metabolic
Hep A,B,C,D
EBV
CMV
Herpes
Leptospirosis
Valproic acid
Isoniazid
Halothane
Tylenol
Mushroom
Phosphorus
ASA
Myocarditis
Heart surgery
Cardiomyopathy
Budd-Chiari
FA oxidation
Reye
Слайд 10Acute Liver Failure: The Adult
Infections Drug/Toxin Cardiovascular Metabolic
Hep A,B,C,D,E
Yellow fever
Dengue Fever
Lassa Fever
Tylenol
Tetracycline
Halothane
Valproic
Acute Liver Failure: The Adult
Infections Drug/Toxin Cardiovascular Metabolic
Hep A,B,C,D,E
Yellow fever
Dengue Fever
Lassa Fever
Tylenol
Tetracycline
Halothane
Valproic
Слайд 11Hospital Course
Hemoglobin steadily falling 11.7 to 8.8
Reticulocyte count 6.6%
Increasing total bilirubin, peak
Hospital Course
Hemoglobin steadily falling 11.7 to 8.8
Reticulocyte count 6.6%
Increasing total bilirubin, peak
Слайд 12What would you do?
What would you do?
Слайд 13CMV, EBV negative
Hepatitis A,B,C negative
Autoimmune markers negative
Copper 120 (nl)
Ceruloplasmin 18 (low)
Low factor
CMV, EBV negative
Hepatitis A,B,C negative
Autoimmune markers negative
Copper 120 (nl)
Ceruloplasmin 18 (low)
Low factor
Слайд 14Pathology – H&E
Peri-portal fibrosis
Peri-portal glycogenated hepatic nuclei
Kupffer cell hyperplasia
Hepatocyte enlargement
Pathology – H&E
Peri-portal fibrosis
Peri-portal glycogenated hepatic nuclei
Kupffer cell hyperplasia
Hepatocyte enlargement
Слайд 15Pathology – H&E
Hepatic steatosis
Microvesicular then macrovesicular
Cholestasis
False positive
alcoholic steatohepatitis
Pathology – H&E
Hepatic steatosis
Microvesicular then macrovesicular
Cholestasis
False positive
alcoholic steatohepatitis
Слайд 16Copper Stain
False positive
Cholestatic liver disorders
Indian Childhood Cirrhosis
False negative
Copper not present in
Copper Stain
False positive
Cholestatic liver disorders
Indian Childhood Cirrhosis
False negative
Copper not present in
Слайд 17WILSON’S DISEASE
WILSON’S DISEASE
Слайд 18Copper Physiology
Most abundant in unprocessed wheat, dried beans, peas, shellfish, chocolate, liver,
Copper Physiology
Most abundant in unprocessed wheat, dried beans, peas, shellfish, chocolate, liver,
Слайд 19Copper Metabolism
Copper Metabolism
Слайд 20Copper Metabolism
Copper is transported into hepatocytes by the human copper transporter (hCTR)
In
Copper Metabolism
Copper is transported into hepatocytes by the human copper transporter (hCTR)
In
Слайд 21Copper Metabolism
ATP7B sorts copper and incorporates into secretory vesicles and ceruloplasmin
Copper Metabolism
ATP7B sorts copper and incorporates into secretory vesicles and ceruloplasmin
Слайд 22ATP7B
Copper transporting P-type ATPase
13q14-13q21
21 exons
6 cysteine-rich copper binding sites
8 transmembrane domains
CPC (cysteine-proline-cysteine)
ATP7B
Copper transporting P-type ATPase
13q14-13q21
21 exons
6 cysteine-rich copper binding sites
8 transmembrane domains
CPC (cysteine-proline-cysteine)
Слайд 23ATP7B
>200 mutations identified
Most small deletions or missense mutations
Missense: neurologic and later
ATP7B
>200 mutations identified
Most small deletions or missense mutations
Missense: neurologic and later
Слайд 24ATP7B
Makes copper available for ceruloplasmin synthesis and transport of copper into vesicles
Long-Evans
ATP7B
Makes copper available for ceruloplasmin synthesis and transport of copper into vesicles
Long-Evans
Слайд 25Clinical Presentation
Combined date from Walshe and Scheinberg & Sternleib
Clinical Presentation
Combined date from Walshe and Scheinberg & Sternleib
Слайд 26Hepatic
Acute hepatitis
25%
Fulminant hepatic failure
Liver transplant
May also present after discontinuing copper chelation
Chronic active
Hepatic
Acute hepatitis
25%
Fulminant hepatic failure
Liver transplant
May also present after discontinuing copper chelation
Chronic active
Слайд 27Laboratory
Mildly elevated serum aminotransferase levels
Low alkaline phosphatase
Serum alkaline phosphatase to total
Laboratory
Mildly elevated serum aminotransferase levels
Low alkaline phosphatase
Serum alkaline phosphatase to total
Слайд 28Neuropsychiatric
40-45% as presentation
Most common 2nd to 3rd decades of life
Extrapyramidal and cerebrellar
Neuropsychiatric
40-45% as presentation
Most common 2nd to 3rd decades of life
Extrapyramidal and cerebrellar
Слайд 2913 year old boy presents to a neurologist for evaluation of a
deterioration
13 year old boy presents to a neurologist for evaluation of a deterioration
Слайд 30Imaging
CT abnormalities
73% ventricular dilation
63% cortical atrophy
55% brainstem atrophy
45% hypodensity in basal ganglia
10%
Imaging
CT abnormalities
73% ventricular dilation
63% cortical atrophy
55% brainstem atrophy
45% hypodensity in basal ganglia
10%
Слайд 31Kayser-Fleischer Ring
Superior poles of cornea, then inferior involvement
Copper chelators result in
Kayser-Fleischer Ring
Superior poles of cornea, then inferior involvement
Copper chelators result in
Слайд 32Sunflower Cataract
Copper deposition in anterior and posterior lens capsule
False positive with foreign
Sunflower Cataract
Copper deposition in anterior and posterior lens capsule
False positive with foreign
Слайд 33Other
Renal
Proximal renal tubular dysfunction (Fanconi’s syndrome)
Renal insufficiency
Nephrocalcinosis
Hematologic
Coombs negative hemolytic anemia
Cardiac
Autonomic dysfunction
Cardiomyopathy
Skeletal
Bone
Other
Renal
Proximal renal tubular dysfunction (Fanconi’s syndrome)
Renal insufficiency
Nephrocalcinosis
Hematologic
Coombs negative hemolytic anemia
Cardiac
Autonomic dysfunction
Cardiomyopathy
Skeletal
Bone
Слайд 34Diagnostic Studies
Diagnostic Studies
Слайд 35Genetic Analysis
Genetic studies are becoming more available but limited
Kumar et al
Genetic Analysis
Genetic studies are becoming more available but limited
Kumar et al
Слайд 36Treatment Goals
Reduce copper accumulation by
Enhancing urinary excretion
Decreasing intestinal absorption
Treatment Goals
Reduce copper accumulation by
Enhancing urinary excretion
Decreasing intestinal absorption
Слайд 37Therapy
Therapy
Слайд 38Liver Transplant
Life-saving
Acute fulminant hepatic failure
Decompensated cirrhosis with progressive end stage liver
Liver Transplant
Life-saving
Acute fulminant hepatic failure
Decompensated cirrhosis with progressive end stage liver
Слайд 39Long-Evans Cinnamon Rats
A deletion of 900 base pairs at the 3’ end
Long-Evans Cinnamon Rats
A deletion of 900 base pairs at the 3’ end
Слайд 40Results
Results
Слайд 41Conclusions
Liver copper levels were lowered in all treatment groups compared to untreated
Conclusions
Liver copper levels were lowered in all treatment groups compared to untreated
Слайд 42Wilson’s Disease
Wilson disease is a disorder of copper transport resulting in copper
Wilson’s Disease
Wilson disease is a disorder of copper transport resulting in copper
Слайд 44Bibliography
Kumar et al. Familial gene analysis for Wilson disease from north-west Indian
Bibliography
Kumar et al. Familial gene analysis for Wilson disease from north-west Indian
 Структурное и бесструктурное управление. Тема 2.5
Структурное и бесструктурное управление. Тема 2.5 Современные барьеры пространственной мобильности в России
Современные барьеры пространственной мобильности в России «Император – Освободитель»
«Император – Освободитель» Дизайн кухни
Дизайн кухни Объекты культурного наследия
Объекты культурного наследия Действия с рациональными числами (интерактивный тест)
Действия с рациональными числами (интерактивный тест) Расчёт напряженно-деформированного состояния лопатки компрессора авиационного двигателя
Расчёт напряженно-деформированного состояния лопатки компрессора авиационного двигателя ПРАВИЛА ДОРОЖНОГО ДВИЖЕНИЯ
ПРАВИЛА ДОРОЖНОГО ДВИЖЕНИЯ Событийная палитра Нурмольской Карелии 2019 г
Событийная палитра Нурмольской Карелии 2019 г Эрнст Кречмер
Эрнст Кречмер Cредства, влияющие на функции органов пищеварения
Cредства, влияющие на функции органов пищеварения Основы композиции
Основы композиции Планирование обустройства участка
Планирование обустройства участка Мойдодыр (1 класс)
Мойдодыр (1 класс) Детский оздоровительно-образовательный Комитет по образованию СПб туристский центр
Детский оздоровительно-образовательный Комитет по образованию СПб туристский центр Командная игра ринго
Командная игра ринго Права детей
Права детей Зятикова Светлана Андреевнаучитель истории и обществознаниявысшей квалификационной категории МБОУ СОШ №74 г.Воронежа
Зятикова Светлана Андреевнаучитель истории и обществознаниявысшей квалификационной категории МБОУ СОШ №74 г.Воронежа Компания Фукс Ойл
Компания Фукс Ойл Синтоизм или синто
Синтоизм или синто Новый фискальный регистратор?
Новый фискальный регистратор? БЕЛО- СИНЕЕ ЧУДО
БЕЛО- СИНЕЕ ЧУДО 3 урок Древние корни.pptx
3 урок Древние корни.pptx Строительство 2-х энергоблоков по 225 мВт с установкой котлоагрегатов с циркулирующим кипящим слоем на Черепетской ГРЭС
Строительство 2-х энергоблоков по 225 мВт с установкой котлоагрегатов с циркулирующим кипящим слоем на Черепетской ГРЭС Системысчисления.
Системысчисления. Единая государственная система предупреждения и ликвидации чрезвычайных ситуаций (РСЧС)
Единая государственная система предупреждения и ликвидации чрезвычайных ситуаций (РСЧС) Патология иммунной системы
Патология иммунной системы Деятельность учителя в условиях реализации ФГОС
Деятельность учителя в условиях реализации ФГОС