- Cognitive Behavioral Treatment of Bipolar Disorder

Содержание
- 2. Use of this Slide Set Presentation information is listed in the notes section below the slide
- 3. Diagnostic Considerations Manic Episode 1 week high, euphoric, or irritable mood plus 3 (4) of the
- 4. Diagnostic Considerations Bipolar I At least one manic or mixed episode May or may not have
- 5. Characteristics of Patients With Bipolar Disorder Prevalence 1-2% of the population Age of Onset Late teens
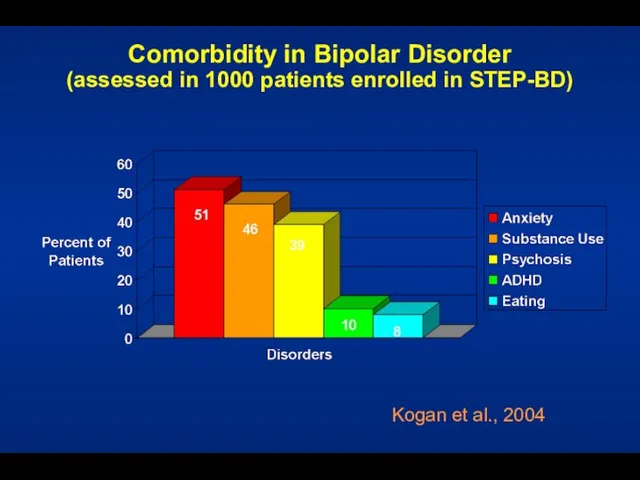
- 6. Comorbidity in Bipolar Disorder (assessed in 1000 patients enrolled in STEP-BD) Kogan et al., 2004
- 7. Diagnostic Issues – Major Depression Depression: Youth hospitalized for severe depression (young and severe) – 41%
- 8. Presentation with Psychosis Is it mania? Schizophrenia? Substance Induced? Schizoaffective? History and family help
- 9. An Abundance of Distress and Disability Family, job, personal Post-episode studies 6 months after: 30% unable
- 10. Psychosocial Treatment
- 11. Topics What is the evidence for the efficacy of psychotherapy for bipolar disorder? What are the
- 12. Psychosocial Treatment for Bipolar Disorder Initial Encouragement: Psychosocial Predictors of Bipolar Course Incomplete Efficacy of Mood
- 13. Role of Psychosocial Factors in Bipolar Disorder Psychosocial stressors impact the course of bipolar disorder: Family
- 14. Pharmacotherapy for Bipolar Disorder Advances in the field, but among patients taking medications: Half relapse first
- 15. Focused Psychosocial Treatments for Bipolar Disorder The product of diverse theoretical orientations, but with a high
- 16. Common Treatment Elements Among CBT, IPSRT, FFT Psychoeducation providing a model of the disorder and risk
- 17. 1. Cochran (1983) 2. Perry et al. (1999) 3. Lam et al. (2000), Lam et al.
- 18. Cochran S. J Consult Clin Psychol. 1984;52:873-878. Cognitive-Behavioral Therapy (CBT) for Medication Adherence (Cochran, 1984) Relapse
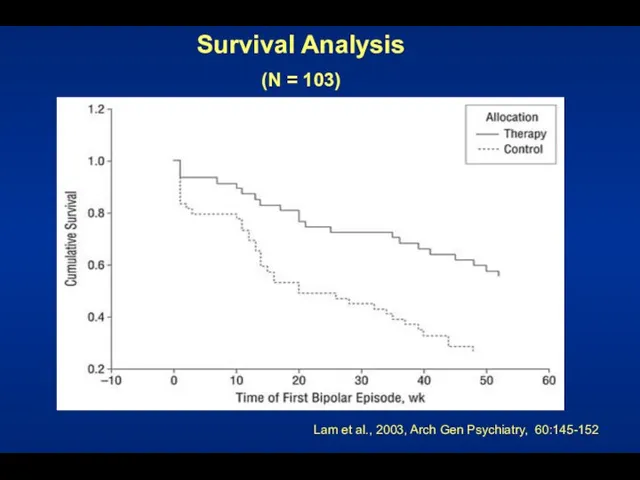
- 19. Lam et al. - An Early CBT Success 103 bipolar patients randomized to CBT or TAU
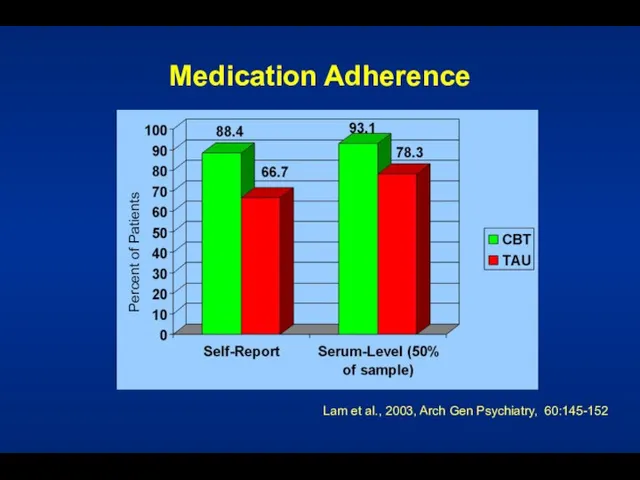
- 20. Medication Adherence Lam et al., 2003, Arch Gen Psychiatry, 60:145-152 Percent of Patients
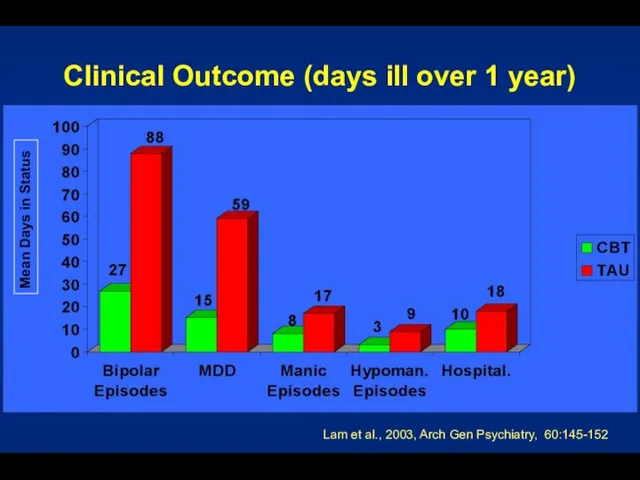
- 21. Clinical Outcome (days ill over 1 year) Lam et al., 2003, Arch Gen Psychiatry, 60:145-152 Mean
- 22. Survival Analysis (N = 103) Lam et al., 2003, Arch Gen Psychiatry, 60:145-152
- 23. Family-Focused Treatment Elements Psychoeducation about bipolar disorder Communication-enhancement training Problem-solving training1 Outcome Adjunctive FFT appears to
- 24. 0 0.2 0.4 0.6 0.8 1 0 5 10 15 20 25 30 35 40 45
- 25. Six Objectives of FFT Help the patient and her or his relatives to: Understand the nature
- 26. Interpersonal and Social Rhythm Therapy Educate patient about bipolar disorder Identify current interpersonal problem areas (e.g.,
- 27. Colom F, et al. Arch Gen Psychiatry. 2003;60:402-407. Group Psychoeducation vs. Standard Care 21 Weeks of
- 28. Colom F, et al. Arch Gen Psychiatry. 2003;60:402-407. Psychoeducation? Psychoeducation What is bipolar illness Symptoms Treatments
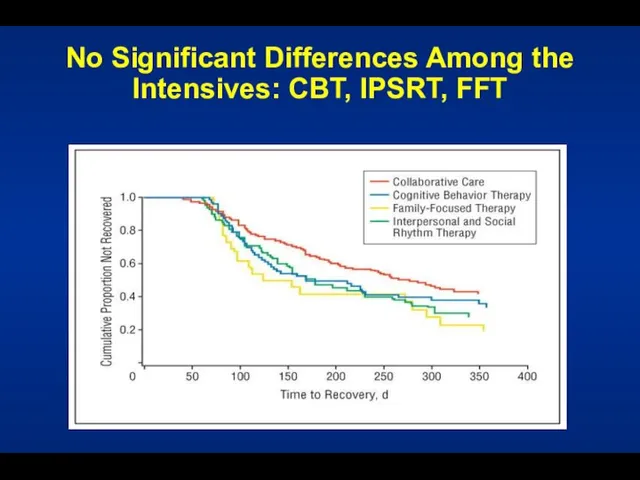
- 29. CBT, IPSRT, FFT vs. Collab Care for Bipolar Depression Miklowitz et al., 2007, Archives Gen Psychiatry
- 30. No Significant Differences Among the Intensives: CBT, IPSRT, FFT
- 31. Given this Evidence... ...What are Some Targets for Psychotherapy? Medication adherence Early detection and intervention Stress
- 32. Medication Non-Adherence in Mood Disorder 98 patients taking mood stabilizers (80% bipolar) 50% non-adherence rate last
- 33. Relapse Prevention Patient as cotherapist Treatment contract Training in early detection Use of treatment team
- 34. Individualized Treatment Contract Why contract? Formulate a plan for the future How I know I am
- 35. Mood Charting Enables early and accurate identification of changes in mood Allows for early intervention prior
- 36. Strategies for Hypomania Explore medical solutions (e.g., dosage or medication changes) Counteract impulsivity Give car keys
- 37. Cognitive-Behavioral Therapy for Bipolar Depression/Relapse Prevention Structure of Sessions Review of symptoms, progress, and problems Construction
- 38. Cognitive Restructuring and Skill Acquisition Restructuring Education (role and nature of thoughts) Self-monitoring of thoughts Identification
- 39. Cognitive Restructuring Examine the evidence for the thought Generate alternative explanations De-catastrophize Debunk “shoulds” Find the
- 40. Questions Used to Formulate Rational Response What is the evidence that the automatic thought is true?
- 41. Questions Used to Formulate Rational Response (Cont’d) What is the effect of my believing the automatic
- 42. Respecting Hot Emotions Interventions are in relation to, not in spite of, the patient’s current mood.
- 43. Activity Assignments: Bipolar Disorder Management of sleep Management of over/under activity Management of destructive activities (substance
- 44. Activity Assignments - 1 Independent Intervention or used in conjunction with cognitive restructuring Help ensure that
- 45. Activity Assignments - 2 Monitor current Activities For change: Start small (where the patient is) Be
- 46. Activity Assignments - 3 Review performance relative to objective criteria (and the degree of mood disturbance)
- 47. Well-Being Therapy Phase In this phase, therapeutic effort and monitoring is devoted to increasing periods of
- 48. End of Treatment Patient has skills to act as his or her own therapist Patient focuses
- 49. Cognitive-Behavioral Therapy for Comorbid Disorders Anxiety disorders Substance use disorders Eating disorders
- 51. Скачать презентацию
Слайд 3Diagnostic Considerations
Manic Episode
1 week high, euphoric, or irritable mood plus 3 (4)
Diagnostic Considerations
Manic Episode
1 week high, euphoric, or irritable mood plus 3 (4)
Слайд 4Diagnostic Considerations
Bipolar I
At least one manic or mixed episode
May or may not
Diagnostic Considerations
Bipolar I
At least one manic or mixed episode
May or may not
Слайд 5Characteristics of Patients With Bipolar Disorder
Prevalence
1-2% of the population
Age of Onset
Late teens
Characteristics of Patients With Bipolar Disorder
Prevalence
1-2% of the population
Age of Onset
Late teens
Слайд 6Comorbidity in Bipolar Disorder
(assessed in 1000 patients enrolled in STEP-BD)
Kogan et al.,
Comorbidity in Bipolar Disorder
(assessed in 1000 patients enrolled in STEP-BD)
Kogan et al.,
Слайд 7Diagnostic Issues – Major Depression
Depression:
Youth hospitalized for severe depression (young and
Diagnostic Issues – Major Depression
Depression:
Youth hospitalized for severe depression (young and
Слайд 8Presentation with Psychosis
Is it mania?
Schizophrenia?
Substance Induced?
Schizoaffective?
History and family help
Presentation with Psychosis
Is it mania?
Schizophrenia?
Substance Induced?
Schizoaffective?
History and family help
Слайд 9An Abundance of Distress and Disability
Family, job, personal
Post-episode studies
6 months after: 30%
An Abundance of Distress and Disability
Family, job, personal
Post-episode studies
6 months after: 30%
Слайд 10Psychosocial Treatment
Psychosocial Treatment
Слайд 11Topics
What is the evidence for the efficacy of psychotherapy for bipolar disorder?
What
Topics
What is the evidence for the efficacy of psychotherapy for bipolar disorder?
What
Слайд 12Psychosocial Treatment for Bipolar Disorder
Initial Encouragement:
Psychosocial Predictors of Bipolar Course
Incomplete Efficacy of
Psychosocial Treatment for Bipolar Disorder
Initial Encouragement:
Psychosocial Predictors of Bipolar Course
Incomplete Efficacy of
Слайд 13Role of Psychosocial Factors
in Bipolar Disorder
Psychosocial stressors impact the course of bipolar
Role of Psychosocial Factors
in Bipolar Disorder
Psychosocial stressors impact the course of bipolar
Слайд 14Pharmacotherapy for Bipolar Disorder
Advances in the field, but among patients taking medications:
Half
Pharmacotherapy for Bipolar Disorder
Advances in the field, but among patients taking medications:
Half
Слайд 15Focused Psychosocial Treatments for Bipolar Disorder
The product of diverse theoretical orientations, but
Focused Psychosocial Treatments for Bipolar Disorder
The product of diverse theoretical orientations, but
Слайд 16Common Treatment Elements
Among CBT, IPSRT, FFT
Psychoeducation providing a model of the disorder
Common Treatment Elements
Among CBT, IPSRT, FFT
Psychoeducation providing a model of the disorder
Слайд 171. Cochran (1983)
2. Perry et al. (1999)
3. Lam et al. (2000), Lam
1. Cochran (1983)
2. Perry et al. (1999)
3. Lam et al. (2000), Lam
Слайд 18Cochran S. J Consult Clin Psychol. 1984;52:873-878.
Cognitive-Behavioral Therapy (CBT)
for Medication Adherence
Cochran S. J Consult Clin Psychol. 1984;52:873-878.
Cognitive-Behavioral Therapy (CBT) for Medication Adherence
Слайд 19Lam et al. - An Early CBT Success
103 bipolar patients randomized to
Lam et al. - An Early CBT Success
103 bipolar patients randomized to
Слайд 20Medication Adherence
Lam et al., 2003, Arch Gen Psychiatry, 60:145-152
Percent of Patients
Medication Adherence
Lam et al., 2003, Arch Gen Psychiatry, 60:145-152
Percent of Patients
Слайд 21Clinical Outcome (days ill over 1 year)
Lam et al., 2003, Arch Gen
Clinical Outcome (days ill over 1 year)
Lam et al., 2003, Arch Gen
Слайд 22Survival Analysis
(N = 103)
Lam et al., 2003, Arch Gen Psychiatry, 60:145-152
Survival Analysis
(N = 103)
Lam et al., 2003, Arch Gen Psychiatry, 60:145-152
Слайд 23Family-Focused Treatment
Elements
Psychoeducation about bipolar disorder
Communication-enhancement training
Problem-solving training1
Outcome
Adjunctive FFT appears to effect1
Depressive symptoms
Manic
Family-Focused Treatment
Elements
Psychoeducation about bipolar disorder
Communication-enhancement training
Problem-solving training1
Outcome
Adjunctive FFT appears to effect1
Depressive symptoms
Manic
Слайд 240
0.2
0.4
0.6
0.8
1
0
5
10
15
20
25
30
35
40
45
50
55
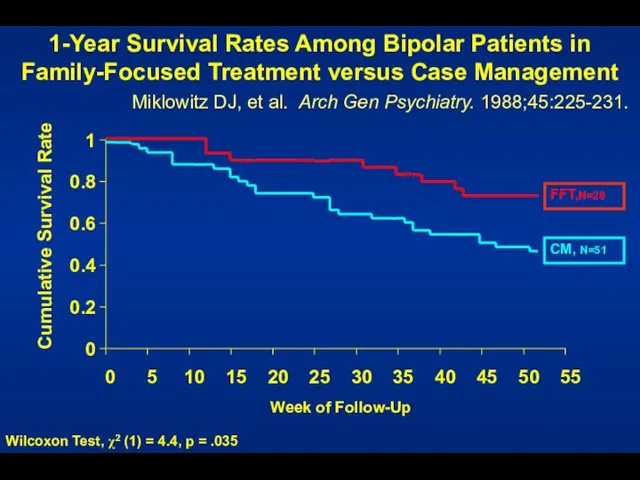
Week of Follow-Up
Cumulative Survival Rate
1-Year Survival Rates Among Bipolar Patients in Family-Focused
0
0.2
0.4
0.6
0.8
1
0
5
10
15
20
25
30
35
40
45
50
55
Week of Follow-Up
Cumulative Survival Rate
1-Year Survival Rates Among Bipolar Patients in Family-Focused
Слайд 25Six Objectives of FFT
Help the patient and her or his relatives to:
Understand
Six Objectives of FFT
Help the patient and her or his relatives to:
Understand
Слайд 26Interpersonal and Social Rhythm Therapy
Educate patient about bipolar disorder
Identify current interpersonal
Interpersonal and Social Rhythm Therapy
Educate patient about bipolar disorder
Identify current interpersonal
Слайд 27Colom F, et al. Arch Gen Psychiatry. 2003;60:402-407.
Group Psychoeducation vs. Standard
Colom F, et al. Arch Gen Psychiatry. 2003;60:402-407.
Group Psychoeducation vs. Standard
Слайд 28Colom F, et al. Arch Gen Psychiatry. 2003;60:402-407.
Psychoeducation?
Psychoeducation
What is bipolar illness
Symptoms
Treatments
Serum
Colom F, et al. Arch Gen Psychiatry. 2003;60:402-407.
Psychoeducation?
Psychoeducation
What is bipolar illness
Symptoms
Treatments
Serum
Слайд 29CBT, IPSRT, FFT vs. Collab Care
for Bipolar Depression
Miklowitz et al., 2007, Archives
CBT, IPSRT, FFT vs. Collab Care for Bipolar Depression Miklowitz et al., 2007, Archives
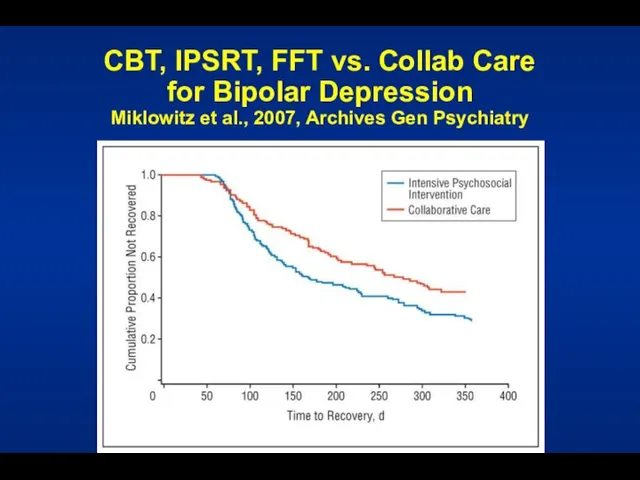
Слайд 30No Significant Differences Among the Intensives: CBT, IPSRT, FFT
No Significant Differences Among the Intensives: CBT, IPSRT, FFT
Слайд 31Given this Evidence...
...What are Some Targets for Psychotherapy?
Medication adherence
Early detection and intervention
Stress
Given this Evidence...
...What are Some Targets for Psychotherapy?
Medication adherence
Early detection and intervention
Stress
Слайд 32Medication Non-Adherence
in Mood Disorder
98 patients taking mood stabilizers (80% bipolar)
50% non-adherence
Medication Non-Adherence
in Mood Disorder
98 patients taking mood stabilizers (80% bipolar)
50% non-adherence
Слайд 33Relapse Prevention
Patient as cotherapist
Treatment contract
Training in early detection
Use of treatment team
Relapse Prevention
Patient as cotherapist
Treatment contract
Training in early detection
Use of treatment team
Слайд 34Individualized Treatment Contract
Why contract?
Formulate a plan for the future
How I know I
Individualized Treatment Contract
Why contract?
Formulate a plan for the future
How I know I
Слайд 35Mood Charting
Enables early and accurate identification of
changes in mood
Allows for early intervention
Mood Charting
Enables early and accurate identification of
changes in mood
Allows for early intervention
Слайд 36Strategies for Hypomania
Explore medical solutions
(e.g., dosage or medication changes)
Counteract impulsivity
Give car keys
Strategies for Hypomania
Explore medical solutions
(e.g., dosage or medication changes)
Counteract impulsivity
Give car keys
Слайд 37Cognitive-Behavioral Therapy
for Bipolar Depression/Relapse Prevention
Structure of Sessions
Review of symptoms, progress, and problems
Construction
Cognitive-Behavioral Therapy
for Bipolar Depression/Relapse Prevention
Structure of Sessions
Review of symptoms, progress, and problems
Construction
Слайд 38Cognitive Restructuring and Skill Acquisition
Restructuring
Education (role and
nature of thoughts)
Self-monitoring
of thoughts
Identification of errors
Substitution
Cognitive Restructuring and Skill Acquisition
Restructuring
Education (role and
nature of thoughts)
Self-monitoring
of thoughts
Identification of errors
Substitution
Слайд 39Cognitive Restructuring
Examine the evidence for the thought
Generate alternative explanations
De-catastrophize
Debunk “shoulds”
Find the logical
Cognitive Restructuring
Examine the evidence for the thought
Generate alternative explanations
De-catastrophize
Debunk “shoulds”
Find the logical
Слайд 40Questions Used to Formulate Rational Response
What is the evidence that the automatic
Questions Used to Formulate Rational Response
What is the evidence that the automatic
Слайд 41Questions Used to Formulate Rational Response (Cont’d)
What is the effect of my
Questions Used to Formulate Rational Response (Cont’d)
What is the effect of my
Слайд 42Respecting Hot Emotions
Interventions are in relation to, not in spite of, the
Respecting Hot Emotions
Interventions are in relation to, not in spite of, the
Слайд 43Activity Assignments:
Bipolar Disorder
Management of sleep
Management of over/under activity
Management of destructive
Activity Assignments:
Bipolar Disorder
Management of sleep
Management of over/under activity
Management of destructive
Слайд 44Activity Assignments - 1
Independent Intervention or used in conjunction with cognitive restructuring
Help
Activity Assignments - 1
Independent Intervention or used in conjunction with cognitive restructuring
Help
Слайд 45Activity Assignments - 2
Monitor current Activities
For change:
Start small (where the patient is)
Be
Activity Assignments - 2
Monitor current Activities
For change:
Start small (where the patient is)
Be
Слайд 46Activity Assignments - 3
Review performance relative to objective criteria (and the degree
Activity Assignments - 3
Review performance relative to objective criteria (and the degree
Слайд 47Well-Being Therapy Phase
In this phase, therapeutic effort and monitoring is devoted to
Well-Being Therapy Phase
In this phase, therapeutic effort and monitoring is devoted to
Слайд 48End of Treatment
Patient has skills to act as his or her own
End of Treatment
Patient has skills to act as his or her own
Слайд 49Cognitive-Behavioral Therapy
for Comorbid Disorders
Anxiety disorders
Substance use disorders
Eating disorders
Cognitive-Behavioral Therapy
for Comorbid Disorders
Anxiety disorders
Substance use disorders
Eating disorders
 Нанороботы
Нанороботы Отходы. Утилизация отходов
Отходы. Утилизация отходов Лидия Прхиповна Кузнецова (Уварова). Скульптор города Лысьвы 15.01.1934 – 15.08.2014
Лидия Прхиповна Кузнецова (Уварова). Скульптор города Лысьвы 15.01.1934 – 15.08.2014 Лекция 6. Показатели эффективности
Лекция 6. Показатели эффективности ВЗАИМОДЕЙСТВИЕ КЛАССНОГО РУКОВОДИТЕЛЯ С РОДИТЕЛЯМИ ( из практического опыта)
ВЗАИМОДЕЙСТВИЕ КЛАССНОГО РУКОВОДИТЕЛЯ С РОДИТЕЛЯМИ ( из практического опыта) Всеобщая декларация прав человека
Всеобщая декларация прав человека Фильтры/кондиционеры охлаждающей жидкости
Фильтры/кондиционеры охлаждающей жидкости Блок обучения. Для сотрудников Компании “Шин Line”
Блок обучения. Для сотрудников Компании “Шин Line” Der Dolmetscher
Der Dolmetscher Синтез наночастиц серебра
Синтез наночастиц серебра Высокий старт. Билимбай 1941-1943 гг. Реактивное самолётостроение. Вертолётостроение. Космонавтика
Высокий старт. Билимбай 1941-1943 гг. Реактивное самолётостроение. Вертолётостроение. Космонавтика Все люди от природы стремятся к знанию.Аристотель.
Все люди от природы стремятся к знанию.Аристотель. Экономические школы
Экономические школы Шаблон презентации проекта
Шаблон презентации проекта Национальная книжная палата БеларусиЕрмолич Елена Ивановна
Национальная книжная палата БеларусиЕрмолич Елена Ивановна Субъекты гражданского права
Субъекты гражданского права Как выводить глубоко офлайновые компании в есот
Как выводить глубоко офлайновые компании в есот 1Национальный центр развития философии и искусств «Большая Волхонка»
1Национальный центр развития философии и искусств «Большая Волхонка» Церковь и государство в XV - начале XVI вв
Церковь и государство в XV - начале XVI вв Мастер-классы
Мастер-классы Москва - город, в котором мы живем
Москва - город, в котором мы живем Тех лет не смолкнет слава. Герои - артековцы
Тех лет не смолкнет слава. Герои - артековцы Введение ФГОС
Введение ФГОС 11. КТтрон от ТехПром
11. КТтрон от ТехПром Кома
Кома  Вышивка крестом 7 класс
Вышивка крестом 7 класс Русский язык. 2 класс
Русский язык. 2 класс Лепка из пластилина. Резьба по кости
Лепка из пластилина. Резьба по кости