- LUNG Diseases

Содержание
- 2. Function of the Respiratory System Slide 13.2 Oversees gas exchanges (oxygen and carbon dioxide) between the
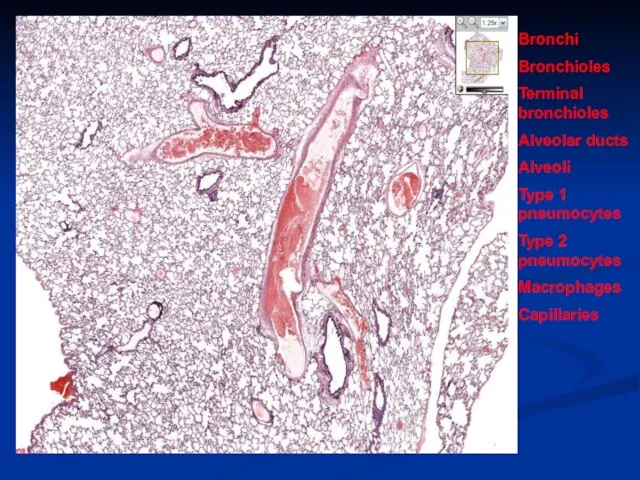
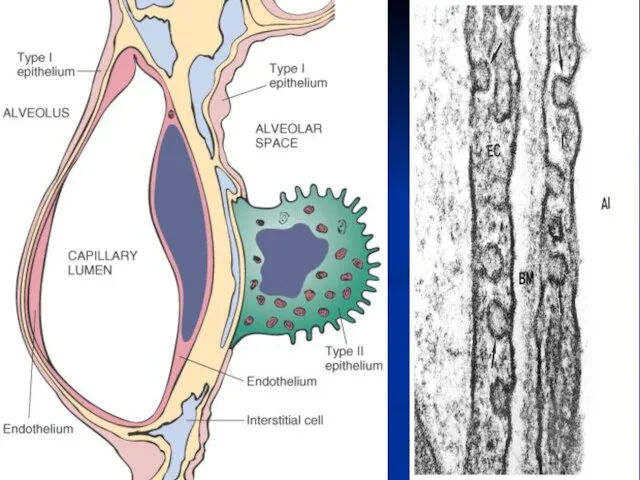
- 3. Bronchi Bronchioles Terminal bronchioles Alveolar ducts Alveoli Type 1 pneumocytes Type 2 pneumocytes Macrophages Capillaries
- 5. N O R M A L C X R
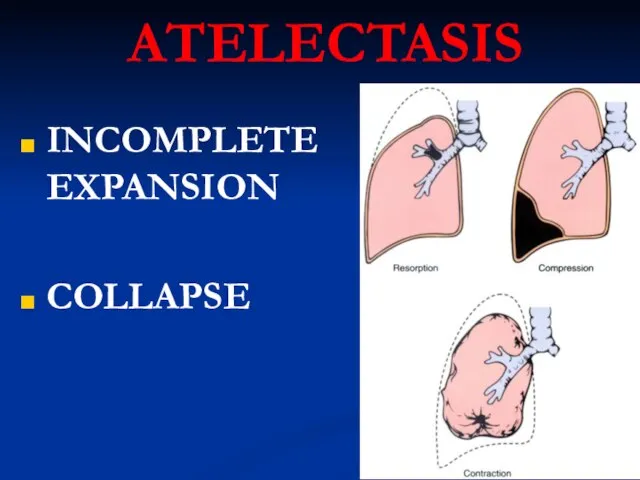
- 6. ATELECTASIS INCOMPLETE EXPANSION COLLAPSE
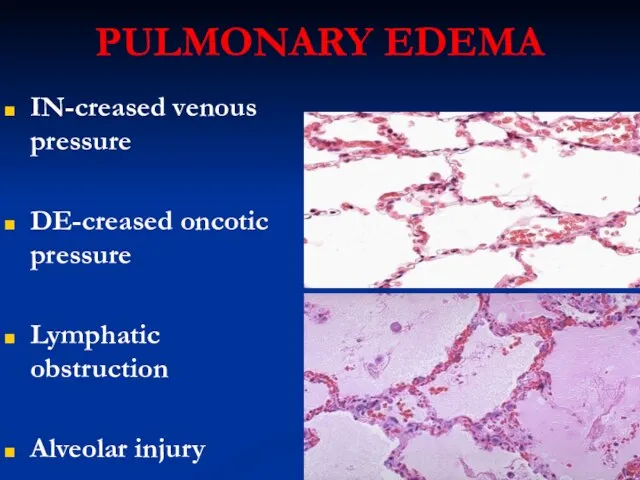
- 7. PULMONARY EDEMA IN-creased venous pressure DE-creased oncotic pressure Lymphatic obstruction Alveolar injury
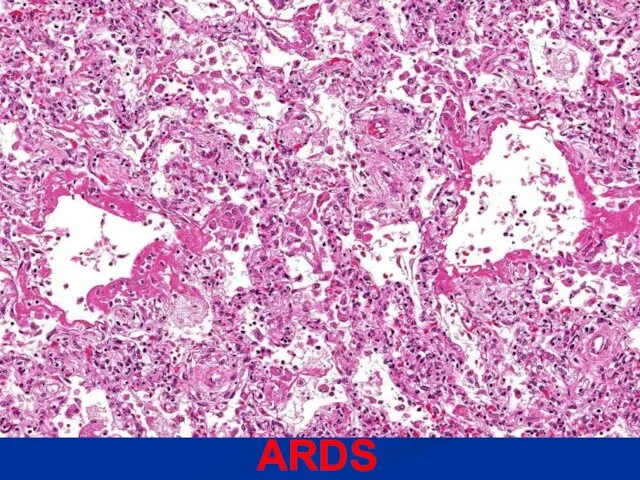
- 8. ARDS
- 9. ACUTE INTERSTITIAL PNEUMONIA Think of it as ARDS with NO known etiology!
- 10. OBSTRUCTION v. RESTRICTION OBSTRUCTION Air or blood? Large or small? Inspiration or Expiration? Obstruction is SMALL
- 11. OBSTRUCTION (cOPD) EMPHYSEMA (almost always chronic) CHRONIC BRONCHITIS? emphysema ASTHMA BRONCHIECTASIS
- 12. EMPHYSEMA COPD, or “END-STAGE” lung disease Centri-acinar, Pan-acinar, Paraseptal, Irregular Like cirrhosis, thought of as END-STAGE
- 13. CENTRO-acinar PAN-acinar EMPHYSEMA
- 14. Bullae, or “peripheral blebs” are hallmarks of chronic obstructive lung disease, COPD.
- 15. CHRONIC BRONCHITIS INHALANTS, POLLUTION, CIGARETTES CHRONIC COUGH CAN OFTEN PROGRESS TO EMPHYSEMA MUCUS hypersecretion, early, i.e.
- 16. ASTHMA Similar to chronic bronchitis but: Wheezing is hallmark (bronchospasm, i.e. “wheezing”) STRONG allergic role, i.e.,
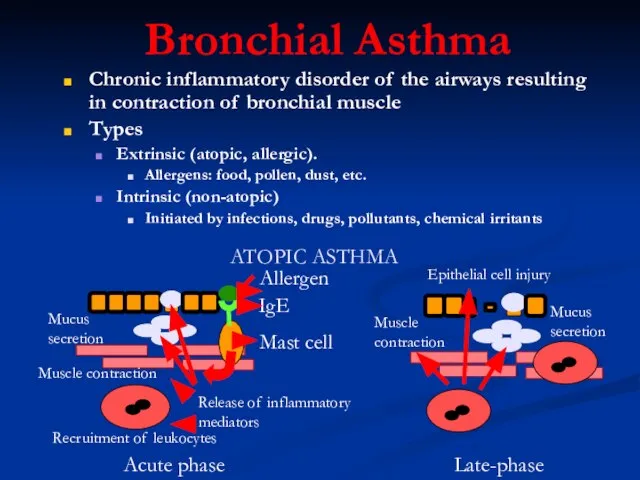
- 17. Bronchial Asthma Chronic inflammatory disorder of the airways resulting in contraction of bronchial muscle Types Extrinsic
- 18. Note the heavy inflammatory cell infiltrate around bronchioles and small bronchi.
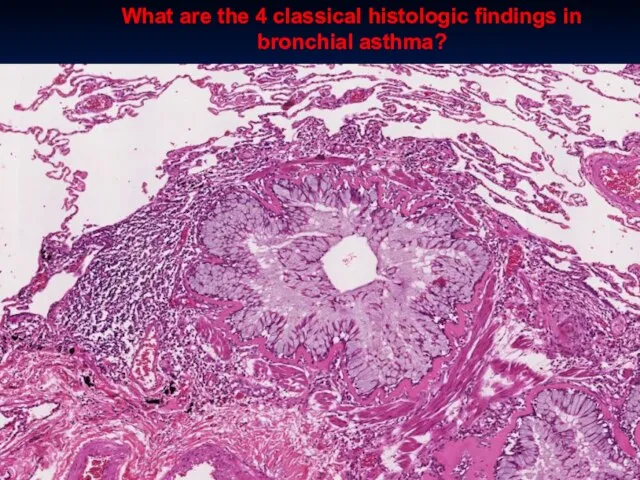
- 19. What are the 4 classical histologic findings in bronchial asthma?
- 20. BRONCHIECTASIS DILATATION of the BRONCHUS, associated with, often, necrotizing inflammation CONGENITAL TB, other bacteria, many viruses
- 21. BRONCHIECTASIS
- 22. RESTRICTIVE (INFILTRATIVE) REDUCED COMPLIANCE, reduced gas exchange) Are also DIFFUSE HETEROGENEOUS FIBROSING GRANULOMATOUS EOSINOPHILIC SMOKING RELATED
- 23. FIBROSING “IDIOPATHIC” PULMONARY FIBROSIS (IPF) NONSPECIFIC INTERSTITIAL FIBROSIS “CRYPTOGENIC” ORGANIZING PNEUMONIA “COLLAGEN” VASCULAR DISEASES PNEUMOCONIOSES DRUG
- 24. IPF (UIP) IDIOPATHIC, i.e., not from any usual caused, like lupus, scleroderma FIBROSIS
- 25. NON-SPECIFIC INTERSTITIAL PNEUMONIA WASTEBASKET DIAGNOSIS, of ANY pneumonia (pneumonitis) of any known or unknown etiology FIBROSIS
- 26. CRYPTOGENIC ORGANIZING PNEUMONIA (COP) IDIOPATHIC “BRONCHIOLITIS OBLITERANS”
- 27. “COLLAGEN” VASCULAR DISEASES Rheumatoid Arthritis SLE (“Lupus”) Progressive Systemic Sclerosis (Scleroderma)
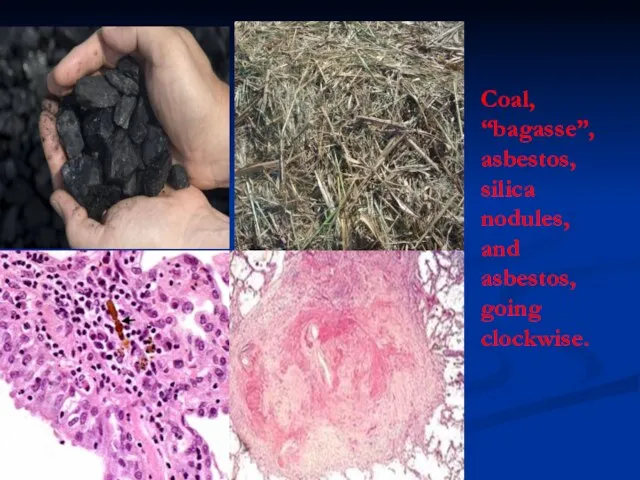
- 28. PNEUMOCONIOSES “OCCUPATIONAL” “COAL MINERS LUNG” DUST OR CHEMICALS OR ORGANIC MATERIALS Coal (anthracosis) Silica Asbestos Be,
- 29. Coal, “bagasse”, asbestos, silica nodules, and asbestos, going clockwise.
- 30. GRANULOMATOUS SARCOIDOSIS, i.e., NON-caseating granulomas (IDIOPATHIC) HYPERSENSITIVITY (DUSTS, bacteria, fungi, Farmer’s Lung, Pigeon Breeder’s Lung)
- 31. SARCOIDOSIS Mainly LUNG, but eye, skin or ANYWHERE UNKNOWN ETIOLOGY IMMUNE, GENETIC factors F>>M B>>W YOUNG
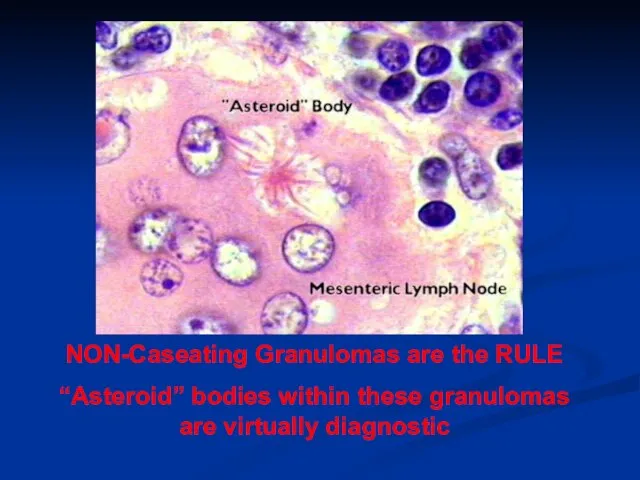
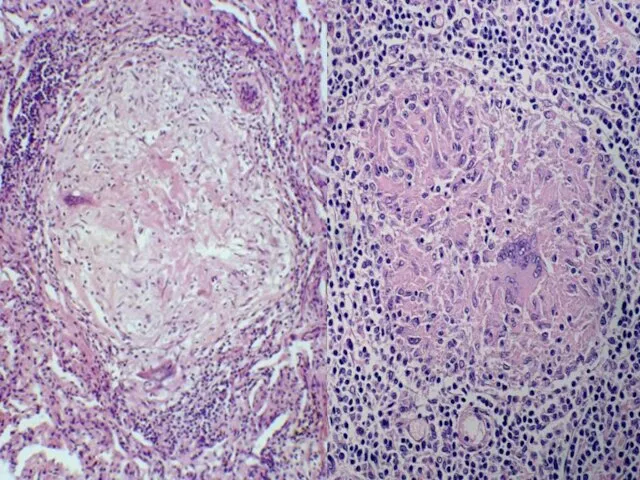
- 32. NON-Caseating Granulomas are the RULE “Asteroid” bodies within these granulomas are virtually diagnostic
- 34. SMOKING RELATED DIP (Desquamative Interstitial Pneumonia) M>>F CIGARETTES 100% Survival Alveolar Macrophages
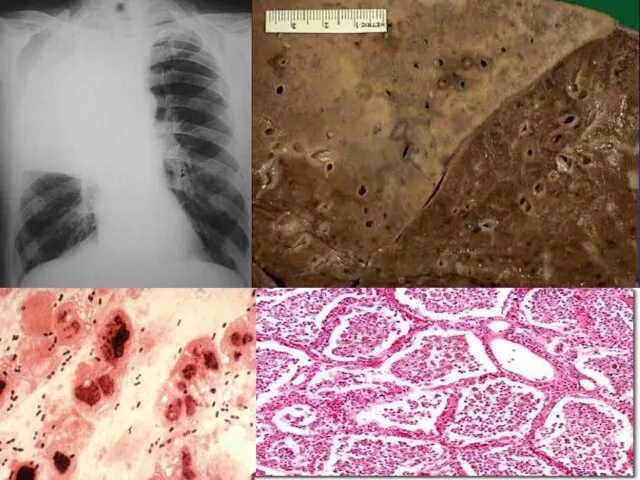
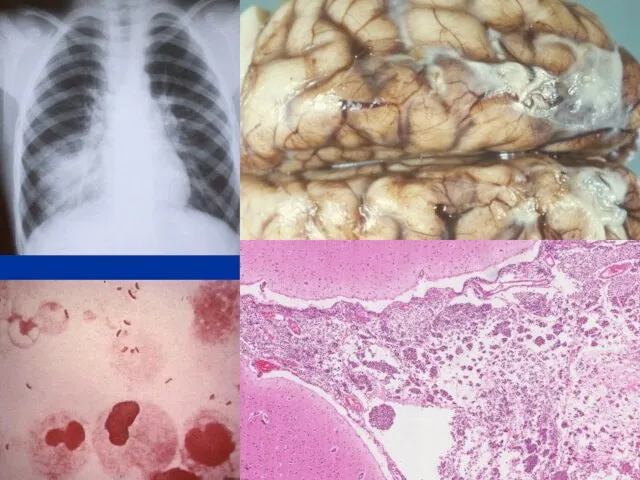
- 35. Pulmonary tuberculosis Caused by Mycobacterium tuberculosis. Transmitted through inhalation of infected droplets Primary Single granuloma within
- 36. Pulmonary tuberculosis Secondary Infection (mostly through reactivation) in a previously sensitized individual. Pathology Cavitary fibrocaseous lesions
- 37. VASCULAR PULMONARY DISEASES PULMONARY EMBOLISM (with or usually WITHOUT infarction) PULMONARY HYPERTENSION, leading to cor pulmonale
- 38. P.E. Usually secondary to debilitated states with immobilization, or following surgery Usually deep leg and deep
- 39. GROSS “saddle” embolism
- 40. PULMONARY HYPERTENSION COPD, C”I”PD (vicious cycle) CHD (Congenital HD, increased left atrial pressure) Recurrent PEs Autoimmune,
- 41. VERY thickened arteriole in pulmonary hypertension NORMAL pulmonary arteriole
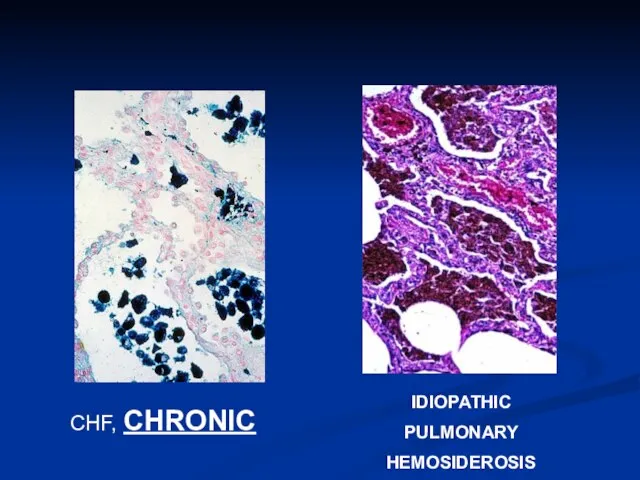
- 42. CHF, CHRONIC IDIOPATHIC PULMONARY HEMOSIDEROSIS
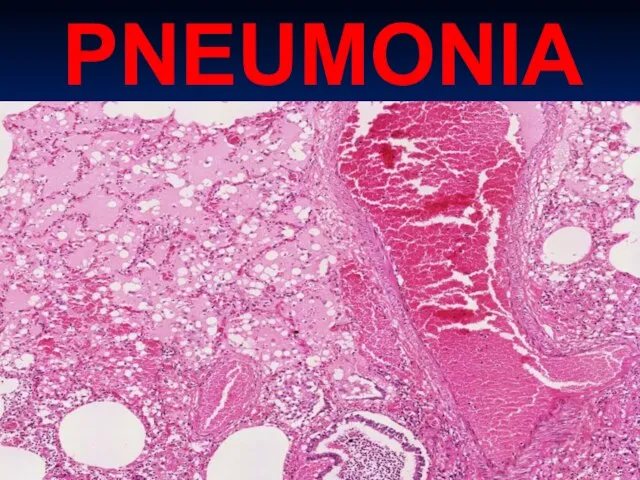
- 43. PNEUMONIA
- 44. PULMONARY INFECTIONS COMMUNITY-ACQUIRED BACTERIAL ACUTE PNEUMONIAS Streptococcus Pneumoniae Haemophilus Influenzae Moraxella Catarrhalis Staphylococcus Aureus Klebsiella Pneumoniae
- 45. BASIC CONSIDERATIONS PNEUMONIA vs. PNEUMONITIS DIFFERENTIATION from INJURIES, OBSTRUCTIVE DISEASES, RESTRICTIVE DISEASES, VASCULAR DISEASES DIFFERENTIATION FROM
- 46. PREDISPOSING FACTORS LOSS OF COUGH REFLEX DIMINISHED MUCIN or CILIA FUNCTION ALVEOLAR MACROPHAGE INTERFERENCE VASCULAR FLOW
- 47. Although pneumonia is one of the most common causes of death, it usually does NOT occur
- 48. Classifications of PNEUMONIAS COMMUNITY ACQUIRED COMMUNITY ACQUIRED, ATYPICAL NOSOCOMIAL ASPIRATION CHRONIC NECROTIZING/ABSCESS FORMATION PNEUMONIAS in IMMUNOCOMPROMISED
- 49. COMMUNITY ACQUIRED STREPTOCOCCUS PNEUMONIAE (i.e., “diplococcus”) HAEMOPHILUS INFLUENZAE (“H-Flu”) MORAXELLA STAPHYLOCOCCUS (STAPH) KLEBSIELLA PNEUMONIAE PSEUDOMONAS AERUGINOSA
- 50. STREPTOCOCCUS The classic LOBAR pneumonia Normal flora in 20% of adults Only 20% of victims have
- 53. MORPHOLOGY ACUTE ORGANIZING CHRONIC FIBROSIS vs. FULL RESOLUTION “HEPATIZATION”, RED vs. GREY CONSOLIDATION “INFILTRATE”, XRAY vs.
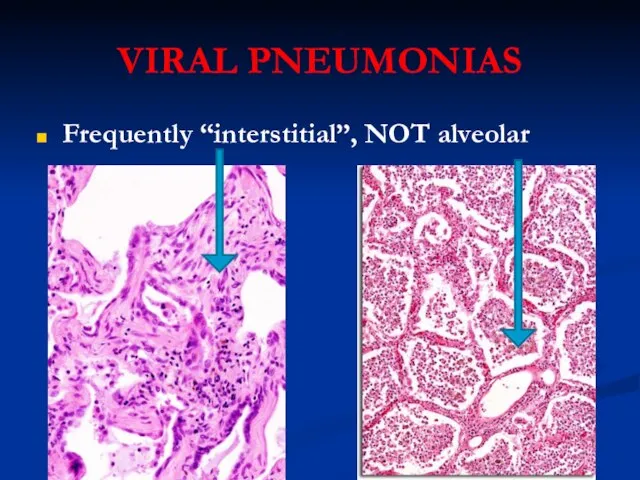
- 54. VIRAL PNEUMONIAS Frequently “interstitial”, NOT alveolar
- 55. ASPIRATION PNEUMONIAS UNCONSCIOUS PATIENTS PATIENTS IN PROLONGED BEDREST LACK OF ABILITY TO SWALLOW OR GAG USUALLY
- 56. LUNG ABSCESSES ASPIRATION SEPTIC EMBOLIZATION NEOPLASIA From NEIGHBORING structures: ESOPHAGUS SPINE PLEURA DIAPHRAGM ANY pneumonia which
- 57. Lung abscess Localized suppurative necrosis Organisms commonly cultured: Staphylococci Streptococci Gram-negative Anaerobes Frequent mixed infections Pathogenesis:
- 58. An abscess can be thought of as a pneumonia in which all of the normal lung
- 59. CHRONIC Pneumonias USUALLY NOT persistences of the community or nosocomial bacterial infections, but CAN BE, at
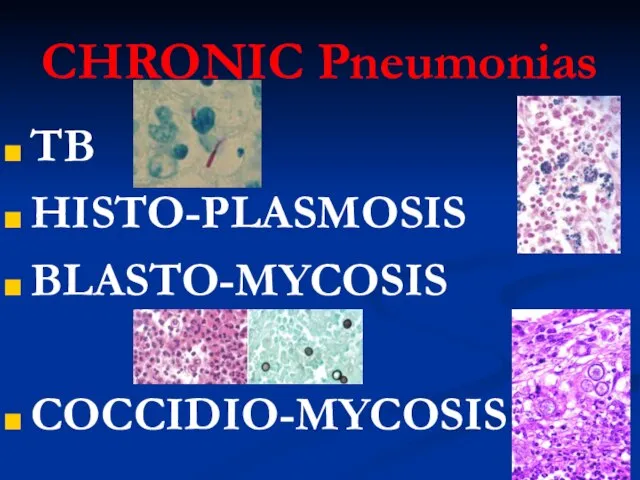
- 60. CHRONIC Pneumonias TB HISTO-PLASMOSIS BLASTO-MYCOSIS COCCIDIO-MYCOSIS
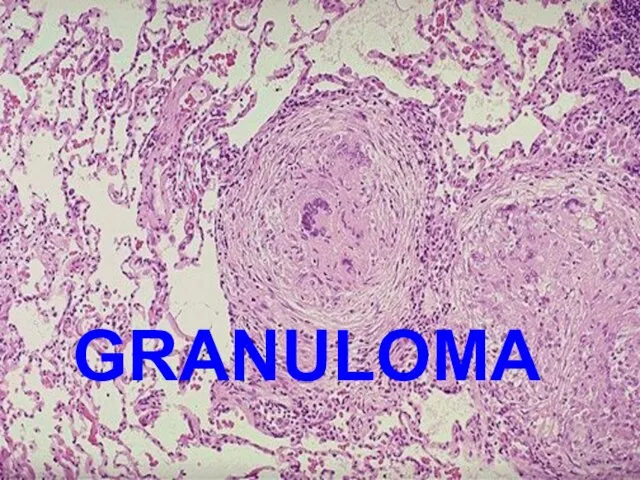
- 61. GRANULOMA
- 62. LUNG TUMORS Benign, malignant, epithelial, mesenchymal, but 90% are CARCINOMAS BIGGEST USA killer. Why? Ans: Prevalence
- 63. PATHOGENESIS NORMAL BRONCHIAL MUCOSA METAPLASTIC/DYSPLASTIC MUCOSA CARCINOMA-IN-SITU (squamous, adeno) INFILTRATING (i.e., “INVASIVE”) cancer
- 64. TWO TYPES NON-SMALL CELL SQUAMOUS CELL CARCINOMA ADENOCARCINOMA LARGE CELL CARCINOMA SMALL CELL CARCINOMA
- 65. The BIG list Squamous cell carcinoma Small cell carcinoma Combined small cell carcinoma Adenocarcinoma: Acinar, papillary,
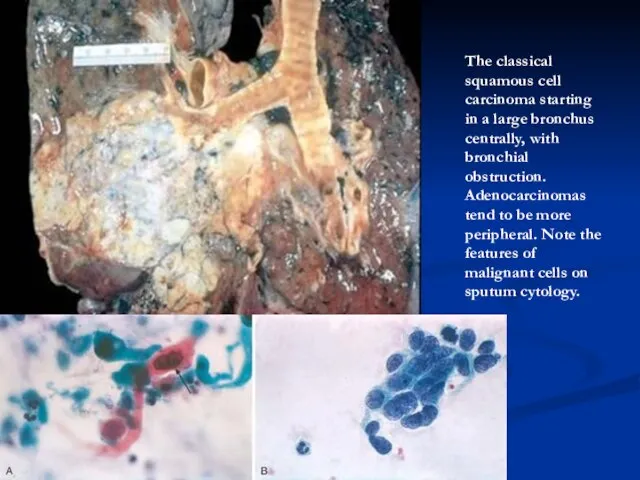
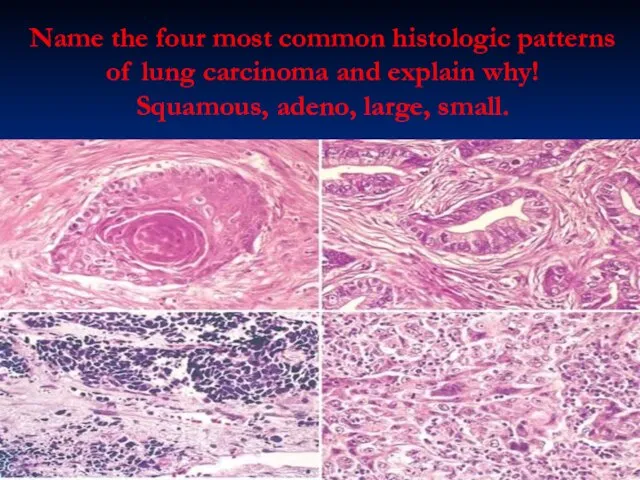
- 66. The classical squamous cell carcinoma starting in a large bronchus centrally, with bronchial obstruction. Adenocarcinomas tend
- 67. Name the four most common histologic patterns of lung carcinoma and explain why! Squamous, adeno, large,
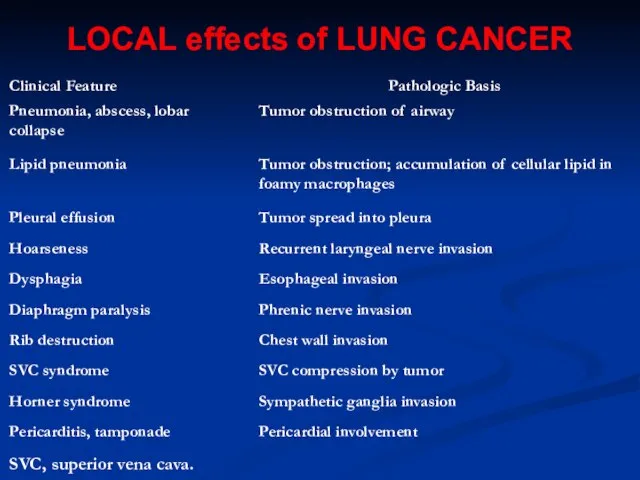
- 68. LOCAL effects of LUNG CANCER
- 69. METASTATIC TUMORS LUNG is the MOST COMMON site for all metastatic tumors, regardless of site of
- 70. PLEURA PLEURITIS PNEUMOTHORAX EFFUSIONS HYDROTHORAX HEMOTHORAX CHYLOTHORAX MESOTHELIOMAS
- 71. PLEURITIS Usual bacteria, viruses, etc. Infarcts Lung abscesses, empyema TB “Collagen” diseases, e.g., RA, SLE Uremia
- 72. PNEUMOTHORAX SPONTANEOUS, TRAUMATIC, THERAPEUTIC OPEN or CLOSED “TENSION” pneumothorax, “valvular” effect “Bleb” rupture Perforating injuries Post
- 73. EFFUSIONS TRANSUDATE (HYDROTHORAX) EXUDATE (HYDROTHORAX) BLOOD (HEMOTHORAX) LYMPH (CHYLOTHORAX)
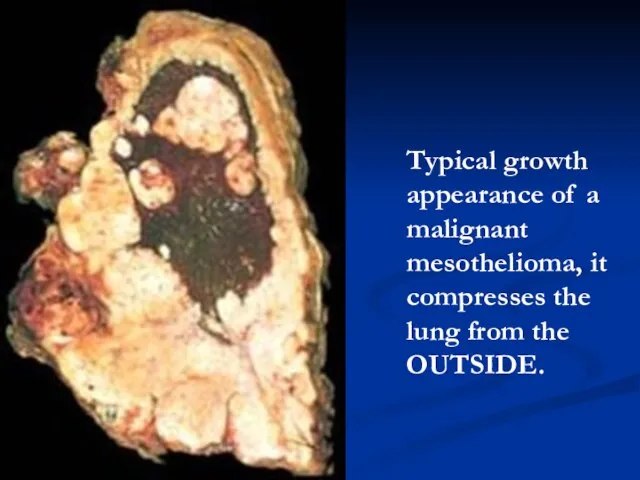
- 74. MESOTHELIOMAS “Benign” vs. “Malignant” differentiation does not matter, but a self limited localized nodule can be
- 75. Typical growth appearance of a malignant mesothelioma, it compresses the lung from the OUTSIDE.
- 77. Скачать презентацию
Слайд 2Function of the Respiratory System
Slide 13.2
Oversees gas exchanges (oxygen and carbon dioxide)
Function of the Respiratory System
Slide 13.2
Oversees gas exchanges (oxygen and carbon dioxide)
Слайд 3Bronchi
Bronchioles
Terminal bronchioles
Alveolar ducts
Alveoli
Type 1 pneumocytes
Type 2 pneumocytes
Macrophages
Capillaries
Bronchi
Bronchioles
Terminal bronchioles
Alveolar ducts
Alveoli
Type 1 pneumocytes
Type 2 pneumocytes
Macrophages
Capillaries
Слайд 5N
O
R
M
A
L
C
X
R
N
O
R
M
A
L
C
X
R

Слайд 6ATELECTASIS
INCOMPLETE EXPANSION
COLLAPSE
ATELECTASIS
INCOMPLETE EXPANSION
COLLAPSE
Слайд 7PULMONARY EDEMA
IN-creased venous pressure
DE-creased oncotic pressure
Lymphatic obstruction
Alveolar injury
PULMONARY EDEMA
IN-creased venous pressure
DE-creased oncotic pressure
Lymphatic obstruction
Alveolar injury
Слайд 8ARDS
ARDS
Слайд 9ACUTE INTERSTITIAL PNEUMONIA
Think of it as ARDS with NO known etiology!
ACUTE INTERSTITIAL PNEUMONIA
Think of it as ARDS with NO known etiology!
Слайд 10OBSTRUCTION v. RESTRICTION
OBSTRUCTION
Air or blood?
Large or small?
Inspiration or Expiration?
Obstruction is SMALL AIRWAY
OBSTRUCTION v. RESTRICTION
OBSTRUCTION
Air or blood?
Large or small?
Inspiration or Expiration?
Obstruction is SMALL AIRWAY
Слайд 11OBSTRUCTION (cOPD)
EMPHYSEMA (almost always chronic)
CHRONIC BRONCHITIS? emphysema
ASTHMA
BRONCHIECTASIS
OBSTRUCTION (cOPD)
EMPHYSEMA (almost always chronic)
CHRONIC BRONCHITIS? emphysema
ASTHMA
BRONCHIECTASIS
Слайд 12EMPHYSEMA
COPD, or “END-STAGE” lung disease
Centri-acinar, Pan-acinar, Paraseptal, Irregular
Like cirrhosis, thought of as
EMPHYSEMA
COPD, or “END-STAGE” lung disease
Centri-acinar, Pan-acinar, Paraseptal, Irregular
Like cirrhosis, thought of as
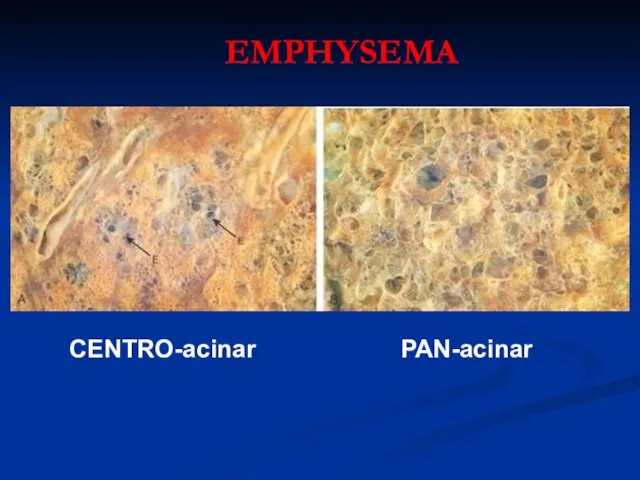
Слайд 13CENTRO-acinar
PAN-acinar
EMPHYSEMA
CENTRO-acinar
PAN-acinar
EMPHYSEMA
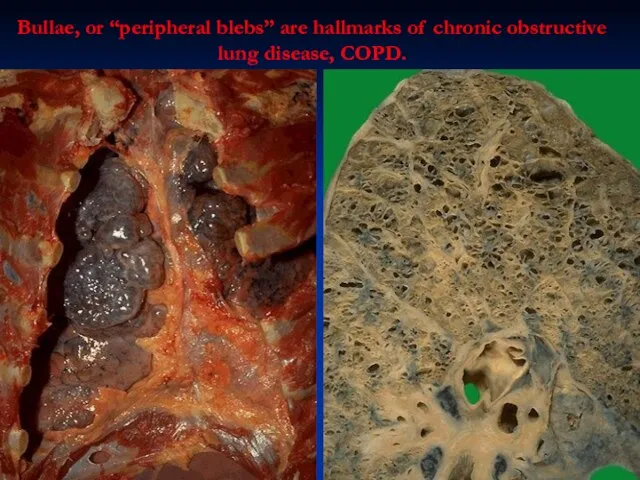
Слайд 14Bullae, or “peripheral blebs” are hallmarks of chronic obstructive lung disease, COPD.
Bullae, or “peripheral blebs” are hallmarks of chronic obstructive lung disease, COPD.
Слайд 15CHRONIC BRONCHITIS
INHALANTS, POLLUTION, CIGARETTES
CHRONIC COUGH
CAN OFTEN PROGRESS TO EMPHYSEMA
MUCUS hypersecretion, early, i.e.
CHRONIC BRONCHITIS
INHALANTS, POLLUTION, CIGARETTES
CHRONIC COUGH
CAN OFTEN PROGRESS TO EMPHYSEMA
MUCUS hypersecretion, early, i.e.
Слайд 16ASTHMA
Similar to chronic bronchitis but:
Wheezing is hallmark (bronchospasm, i.e. “wheezing”)
STRONG allergic role,
ASTHMA
Similar to chronic bronchitis but:
Wheezing is hallmark (bronchospasm, i.e. “wheezing”)
STRONG allergic role,
Слайд 17Bronchial Asthma
Chronic inflammatory disorder of the airways resulting in contraction of bronchial
Bronchial Asthma
Chronic inflammatory disorder of the airways resulting in contraction of bronchial
Слайд 18Note the heavy inflammatory cell infiltrate around bronchioles and small bronchi.
Note the heavy inflammatory cell infiltrate around bronchioles and small bronchi.

Слайд 19What are the 4 classical histologic findings in bronchial asthma?
What are the 4 classical histologic findings in bronchial asthma?
Слайд 20BRONCHIECTASIS
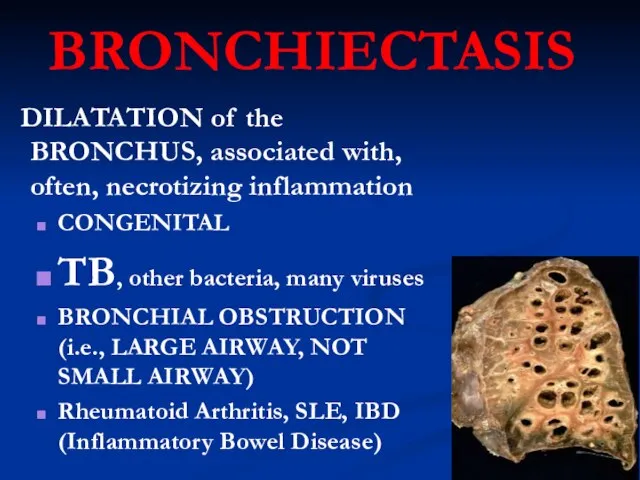
DILATATION of the BRONCHUS, associated with, often, necrotizing inflammation
CONGENITAL
TB, other bacteria,
BRONCHIECTASIS
DILATATION of the BRONCHUS, associated with, often, necrotizing inflammation
CONGENITAL
TB, other bacteria,
Слайд 21BRONCHIECTASIS
BRONCHIECTASIS

Слайд 22RESTRICTIVE
(INFILTRATIVE)
REDUCED COMPLIANCE, reduced gas exchange)
Are also DIFFUSE
HETEROGENEOUS
FIBROSING
GRANULOMATOUS
EOSINOPHILIC
SMOKING RELATED
PAP (Pulmonary Alveolar Proteinosis
RESTRICTIVE
(INFILTRATIVE)
REDUCED COMPLIANCE, reduced gas exchange)
Are also DIFFUSE
HETEROGENEOUS
FIBROSING
GRANULOMATOUS
EOSINOPHILIC
SMOKING RELATED
PAP (Pulmonary Alveolar Proteinosis
Слайд 23FIBROSING
“IDIOPATHIC” PULMONARY FIBROSIS (IPF)
NONSPECIFIC INTERSTITIAL FIBROSIS
“CRYPTOGENIC” ORGANIZING PNEUMONIA
“COLLAGEN” VASCULAR DISEASES
PNEUMOCONIOSES
DRUG REACTIONS
RADIATION CHANGES
FIBROSING
“IDIOPATHIC” PULMONARY FIBROSIS (IPF)
NONSPECIFIC INTERSTITIAL FIBROSIS
“CRYPTOGENIC” ORGANIZING PNEUMONIA
“COLLAGEN” VASCULAR DISEASES
PNEUMOCONIOSES
DRUG REACTIONS
RADIATION CHANGES
Слайд 24IPF (UIP)
IDIOPATHIC, i.e., not from any usual caused, like lupus, scleroderma
FIBROSIS
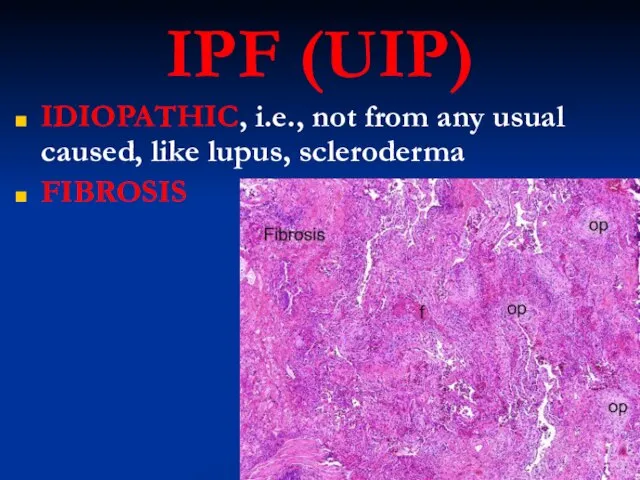
IPF (UIP)
IDIOPATHIC, i.e., not from any usual caused, like lupus, scleroderma
FIBROSIS
Слайд 25NON-SPECIFIC INTERSTITIAL PNEUMONIA
WASTEBASKET DIAGNOSIS, of ANY pneumonia (pneumonitis) of any known or
NON-SPECIFIC INTERSTITIAL PNEUMONIA
WASTEBASKET DIAGNOSIS, of ANY pneumonia (pneumonitis) of any known or
Слайд 26CRYPTOGENIC ORGANIZING PNEUMONIA (COP)
IDIOPATHIC
“BRONCHIOLITIS OBLITERANS”
CRYPTOGENIC ORGANIZING PNEUMONIA (COP)
IDIOPATHIC
“BRONCHIOLITIS OBLITERANS”
Слайд 27“COLLAGEN” VASCULAR DISEASES
Rheumatoid Arthritis
SLE (“Lupus”)
Progressive Systemic Sclerosis (Scleroderma)
“COLLAGEN” VASCULAR DISEASES
Rheumatoid Arthritis
SLE (“Lupus”)
Progressive Systemic Sclerosis (Scleroderma)
Слайд 28PNEUMOCONIOSES
“OCCUPATIONAL”
“COAL MINERS LUNG”
DUST OR CHEMICALS OR ORGANIC MATERIALS
Coal (anthracosis)
Silica
Asbestos
Be, FeO, BaSO4, CHEMO
HAY,
PNEUMOCONIOSES
“OCCUPATIONAL”
“COAL MINERS LUNG”
DUST OR CHEMICALS OR ORGANIC MATERIALS
Coal (anthracosis)
Silica
Asbestos
Be, FeO, BaSO4, CHEMO
HAY,
Слайд 29Coal, “bagasse”, asbestos, silica nodules, and asbestos, going clockwise.
Coal, “bagasse”, asbestos, silica nodules, and asbestos, going clockwise.
Слайд 30GRANULOMATOUS
SARCOIDOSIS, i.e., NON-caseating granulomas (IDIOPATHIC)
HYPERSENSITIVITY (DUSTS, bacteria, fungi, Farmer’s Lung, Pigeon Breeder’s
GRANULOMATOUS
SARCOIDOSIS, i.e., NON-caseating granulomas (IDIOPATHIC)
HYPERSENSITIVITY (DUSTS, bacteria, fungi, Farmer’s Lung, Pigeon Breeder’s

Слайд 31SARCOIDOSIS
Mainly LUNG, but eye, skin or ANYWHERE
UNKNOWN ETIOLOGY
IMMUNE, GENETIC factors
F>>M
B>>W
YOUNG ADULT BLACK
SARCOIDOSIS
Mainly LUNG, but eye, skin or ANYWHERE
UNKNOWN ETIOLOGY
IMMUNE, GENETIC factors
F>>M
B>>W
YOUNG ADULT BLACK
Слайд 32NON-Caseating Granulomas are the RULE
“Asteroid” bodies within these granulomas are virtually diagnostic
NON-Caseating Granulomas are the RULE
“Asteroid” bodies within these granulomas are virtually diagnostic
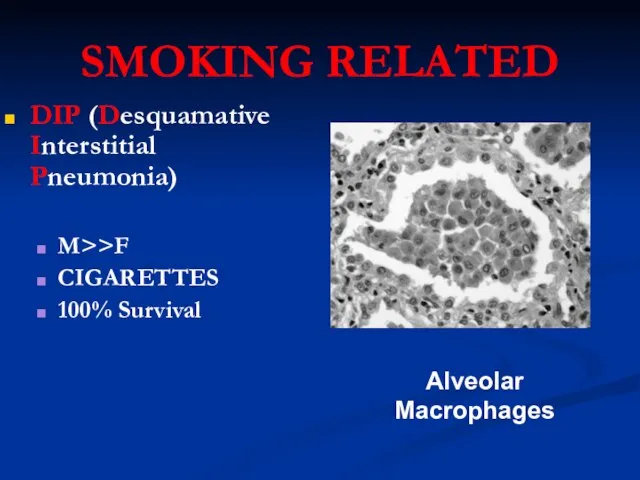
Слайд 34SMOKING RELATED
DIP (Desquamative Interstitial Pneumonia)
M>>F
CIGARETTES
100% Survival
Alveolar Macrophages
SMOKING RELATED
DIP (Desquamative Interstitial Pneumonia)
M>>F
CIGARETTES
100% Survival
Alveolar Macrophages
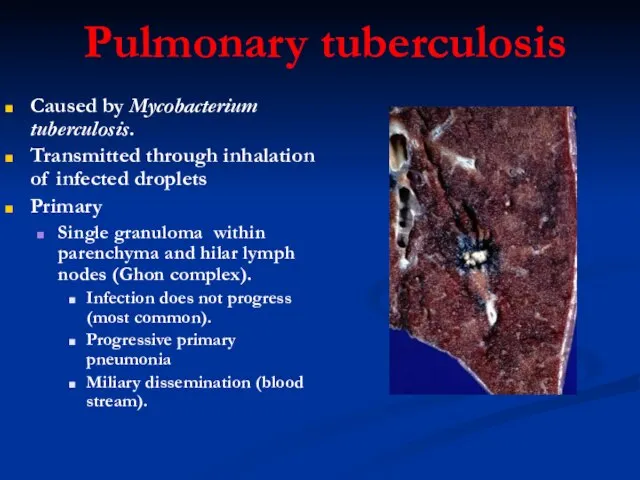
Слайд 35Pulmonary tuberculosis
Caused by Mycobacterium tuberculosis.
Transmitted through inhalation of infected droplets
Primary
Single granuloma within
Pulmonary tuberculosis
Caused by Mycobacterium tuberculosis.
Transmitted through inhalation of infected droplets
Primary
Single granuloma within
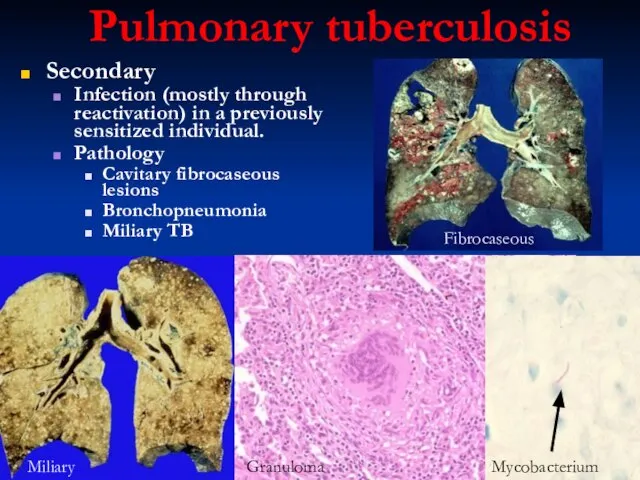
Слайд 36Pulmonary tuberculosis
Secondary
Infection (mostly through reactivation) in a previously sensitized individual.
Pathology
Cavitary fibrocaseous lesions
Bronchopneumonia
Miliary
Pulmonary tuberculosis
Secondary
Infection (mostly through reactivation) in a previously sensitized individual.
Pathology
Cavitary fibrocaseous lesions
Bronchopneumonia
Miliary
Слайд 37VASCULAR PULMONARY DISEASES
PULMONARY EMBOLISM (with or usually WITHOUT infarction)
PULMONARY HYPERTENSION, leading to
VASCULAR PULMONARY DISEASES
PULMONARY EMBOLISM (with or usually WITHOUT infarction)
PULMONARY HYPERTENSION, leading to
Слайд 38P.E.
Usually secondary to debilitated states with immobilization, or following surgery
Usually deep leg
P.E.
Usually secondary to debilitated states with immobilization, or following surgery
Usually deep leg
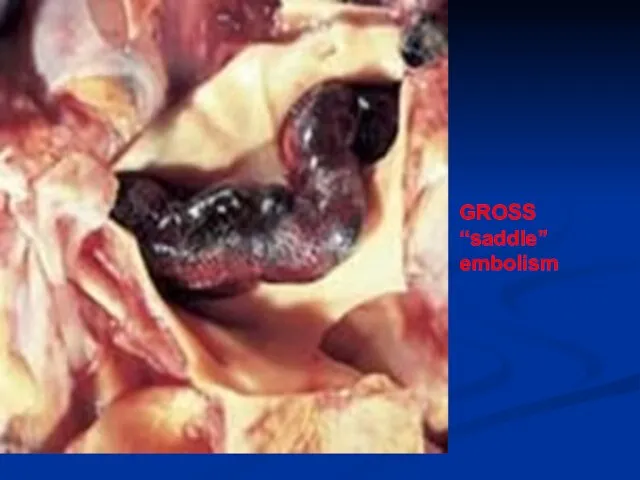
Слайд 39GROSS “saddle” embolism
Слайд 40PULMONARY HYPERTENSION
COPD, C”I”PD (vicious cycle)
CHD (Congenital HD, increased left atrial pressure)
Recurrent PEs
Autoimmune,
PULMONARY HYPERTENSION
COPD, C”I”PD (vicious cycle)
CHD (Congenital HD, increased left atrial pressure)
Recurrent PEs
Autoimmune,
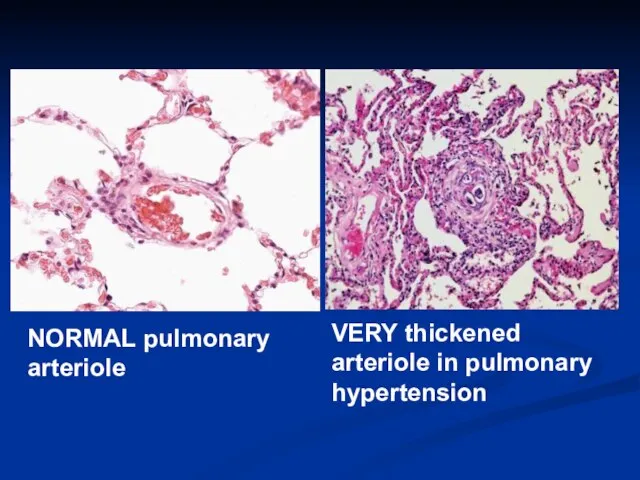
Слайд 41VERY thickened arteriole in pulmonary hypertension
NORMAL pulmonary arteriole
VERY thickened arteriole in pulmonary hypertension
NORMAL pulmonary arteriole
Слайд 42CHF, CHRONIC
IDIOPATHIC
PULMONARY
HEMOSIDEROSIS
CHF, CHRONIC
IDIOPATHIC
PULMONARY
HEMOSIDEROSIS
Слайд 43PNEUMONIA
PNEUMONIA
Слайд 44PULMONARY INFECTIONS
COMMUNITY-ACQUIRED BACTERIAL ACUTE PNEUMONIAS
Streptococcus Pneumoniae
Haemophilus Influenzae
Moraxella Catarrhalis
Staphylococcus Aureus
Klebsiella Pneumoniae
Pseudomonas Aeruginosa
Legionella Pneumophila
COMMUNITY-ACQUIRED
PULMONARY INFECTIONS
COMMUNITY-ACQUIRED BACTERIAL ACUTE PNEUMONIAS
Streptococcus Pneumoniae
Haemophilus Influenzae
Moraxella Catarrhalis
Staphylococcus Aureus
Klebsiella Pneumoniae
Pseudomonas Aeruginosa
Legionella Pneumophila
COMMUNITY-ACQUIRED
Слайд 45BASIC CONSIDERATIONS
PNEUMONIA vs. PNEUMONITIS
DIFFERENTIATION from INJURIES, OBSTRUCTIVE DISEASES, RESTRICTIVE DISEASES, VASCULAR DISEASES
DIFFERENTIATION
BASIC CONSIDERATIONS
PNEUMONIA vs. PNEUMONITIS
DIFFERENTIATION from INJURIES, OBSTRUCTIVE DISEASES, RESTRICTIVE DISEASES, VASCULAR DISEASES
DIFFERENTIATION

Слайд 46PREDISPOSING FACTORS
LOSS OF COUGH REFLEX
DIMINISHED MUCIN or CILIA FUNCTION
ALVEOLAR MACROPHAGE INTERFERENCE
VASCULAR FLOW
PREDISPOSING FACTORS
LOSS OF COUGH REFLEX
DIMINISHED MUCIN or CILIA FUNCTION
ALVEOLAR MACROPHAGE INTERFERENCE
VASCULAR FLOW
Слайд 47Although pneumonia is one of the most common causes of death, it
Although pneumonia is one of the most common causes of death, it
Слайд 48Classifications of PNEUMONIAS
COMMUNITY ACQUIRED
COMMUNITY ACQUIRED, ATYPICAL
NOSOCOMIAL
ASPIRATION
CHRONIC
NECROTIZING/ABSCESS FORMATION
PNEUMONIAS in IMMUNOCOMPROMISED HOSTS
Classifications of PNEUMONIAS
COMMUNITY ACQUIRED
COMMUNITY ACQUIRED, ATYPICAL
NOSOCOMIAL
ASPIRATION
CHRONIC
NECROTIZING/ABSCESS FORMATION
PNEUMONIAS in IMMUNOCOMPROMISED HOSTS
Слайд 49COMMUNITY ACQUIRED
STREPTOCOCCUS PNEUMONIAE (i.e., “diplococcus”)
HAEMOPHILUS INFLUENZAE (“H-Flu”)
MORAXELLA
STAPHYLOCOCCUS (STAPH)
KLEBSIELLA PNEUMONIAE
PSEUDOMONAS AERUGINOSA
LEGIONELLA PNEUMOPHILIA
COMMUNITY ACQUIRED
STREPTOCOCCUS PNEUMONIAE (i.e., “diplococcus”)
HAEMOPHILUS INFLUENZAE (“H-Flu”)
MORAXELLA
STAPHYLOCOCCUS (STAPH)
KLEBSIELLA PNEUMONIAE
PSEUDOMONAS AERUGINOSA
LEGIONELLA PNEUMOPHILIA
Слайд 50STREPTOCOCCUS
The classic LOBAR pneumonia
Normal flora in 20% of adults
Only 20% of victims
STREPTOCOCCUS
The classic LOBAR pneumonia
Normal flora in 20% of adults
Only 20% of victims
Слайд 53MORPHOLOGY
ACUTE
ORGANIZING
CHRONIC
FIBROSIS vs. FULL RESOLUTION
“HEPATIZATION”, RED vs. GREY
CONSOLIDATION
“INFILTRATE”, XRAY vs. HISTOPATH
Loss of “CREPITANCE”
MORPHOLOGY
ACUTE
ORGANIZING
CHRONIC
FIBROSIS vs. FULL RESOLUTION
“HEPATIZATION”, RED vs. GREY
CONSOLIDATION
“INFILTRATE”, XRAY vs. HISTOPATH
Loss of “CREPITANCE”
Слайд 54VIRAL PNEUMONIAS
Frequently “interstitial”, NOT alveolar
VIRAL PNEUMONIAS
Frequently “interstitial”, NOT alveolar
Слайд 55ASPIRATION PNEUMONIAS
UNCONSCIOUS PATIENTS
PATIENTS IN PROLONGED BEDREST
LACK OF ABILITY TO SWALLOW OR GAG
USUALLY
ASPIRATION PNEUMONIAS
UNCONSCIOUS PATIENTS
PATIENTS IN PROLONGED BEDREST
LACK OF ABILITY TO SWALLOW OR GAG
USUALLY
Слайд 56LUNG ABSCESSES
ASPIRATION
SEPTIC EMBOLIZATION
NEOPLASIA
From NEIGHBORING structures:
ESOPHAGUS
SPINE
PLEURA
DIAPHRAGM
ANY pneumonia which is severe and destructive, and
LUNG ABSCESSES
ASPIRATION
SEPTIC EMBOLIZATION
NEOPLASIA
From NEIGHBORING structures:
ESOPHAGUS
SPINE
PLEURA
DIAPHRAGM
ANY pneumonia which is severe and destructive, and
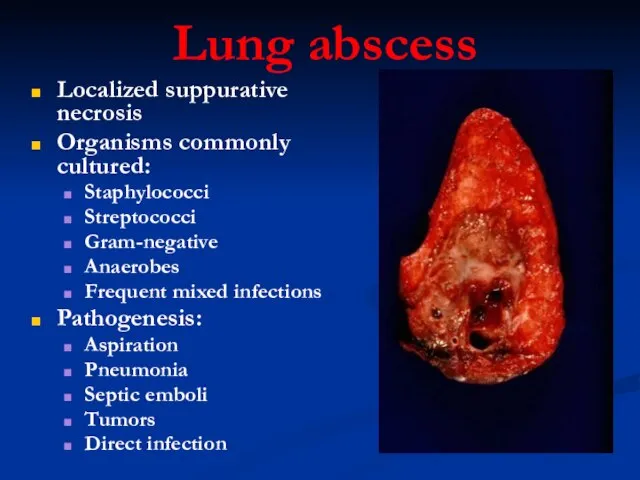
Слайд 57Lung abscess
Localized suppurative necrosis
Organisms commonly cultured:
Staphylococci
Streptococci
Gram-negative
Anaerobes
Frequent mixed infections
Pathogenesis:
Aspiration
Pneumonia
Septic emboli
Tumors
Direct infection
Lung abscess
Localized suppurative necrosis
Organisms commonly cultured:
Staphylococci
Streptococci
Gram-negative
Anaerobes
Frequent mixed infections
Pathogenesis:
Aspiration
Pneumonia
Septic emboli
Tumors
Direct infection
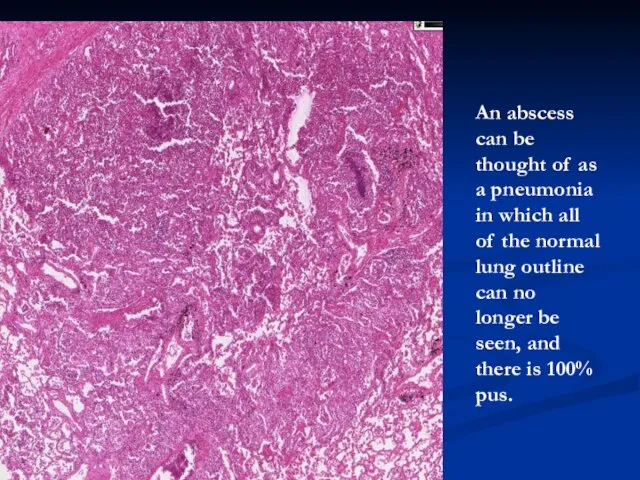
Слайд 58An abscess can be thought of as a pneumonia in which all
An abscess can be thought of as a pneumonia in which all
Слайд 59CHRONIC Pneumonias
USUALLY NOT persistences of the community or nosocomial bacterial infections, but
CHRONIC Pneumonias
USUALLY NOT persistences of the community or nosocomial bacterial infections, but
Слайд 60CHRONIC Pneumonias
TB
HISTO-PLASMOSIS
BLASTO-MYCOSIS
COCCIDIO-MYCOSIS
CHRONIC Pneumonias
TB
HISTO-PLASMOSIS
BLASTO-MYCOSIS
COCCIDIO-MYCOSIS
Слайд 61GRANULOMA
GRANULOMA
Слайд 62LUNG TUMORS
Benign, malignant, epithelial, mesenchymal, but 90% are CARCINOMAS
BIGGEST USA killer. Why?
LUNG TUMORS
Benign, malignant, epithelial, mesenchymal, but 90% are CARCINOMAS
BIGGEST USA killer. Why?
Слайд 63PATHOGENESIS
NORMAL BRONCHIAL MUCOSA
METAPLASTIC/DYSPLASTIC MUCOSA
CARCINOMA-IN-SITU (squamous, adeno)
INFILTRATING (i.e., “INVASIVE”) cancer
PATHOGENESIS
NORMAL BRONCHIAL MUCOSA
METAPLASTIC/DYSPLASTIC MUCOSA
CARCINOMA-IN-SITU (squamous, adeno)
INFILTRATING (i.e., “INVASIVE”) cancer
Слайд 64TWO TYPES
NON-SMALL CELL
SQUAMOUS CELL CARCINOMA
ADENOCARCINOMA
LARGE CELL CARCINOMA
SMALL CELL CARCINOMA
TWO TYPES
NON-SMALL CELL
SQUAMOUS CELL CARCINOMA
ADENOCARCINOMA
LARGE CELL CARCINOMA
SMALL CELL CARCINOMA
Слайд 65The BIG list
Squamous cell carcinoma
Small cell carcinoma
Combined small cell carcinoma
Adenocarcinoma: Acinar, papillary,
The BIG list
Squamous cell carcinoma
Small cell carcinoma
Combined small cell carcinoma
Adenocarcinoma: Acinar, papillary,
Слайд 66The classical squamous cell carcinoma starting in a large bronchus centrally, with
The classical squamous cell carcinoma starting in a large bronchus centrally, with
Слайд 67Name the four most common histologic patterns of lung carcinoma and explain
Name the four most common histologic patterns of lung carcinoma and explain
Слайд 68LOCAL effects of LUNG CANCER
LOCAL effects of LUNG CANCER
Слайд 69METASTATIC TUMORS
LUNG is the MOST COMMON site for all metastatic tumors, regardless
METASTATIC TUMORS
LUNG is the MOST COMMON site for all metastatic tumors, regardless
Слайд 70PLEURA
PLEURITIS
PNEUMOTHORAX
EFFUSIONS
HYDROTHORAX
HEMOTHORAX
CHYLOTHORAX
MESOTHELIOMAS
PLEURA
PLEURITIS
PNEUMOTHORAX
EFFUSIONS
HYDROTHORAX
HEMOTHORAX
CHYLOTHORAX
MESOTHELIOMAS
Слайд 71PLEURITIS
Usual bacteria, viruses, etc.
Infarcts
Lung abscesses, empyema
TB
“Collagen” diseases, e.g., RA, SLE
Uremia
Metastatic
PLEURITIS
Usual bacteria, viruses, etc.
Infarcts
Lung abscesses, empyema
TB
“Collagen” diseases, e.g., RA, SLE
Uremia
Metastatic
Слайд 72PNEUMOTHORAX
SPONTANEOUS, TRAUMATIC, THERAPEUTIC
OPEN or CLOSED
“TENSION” pneumothorax, “valvular” effect
“Bleb” rupture
Perforating injuries
Post needle biopsy
PNEUMOTHORAX
SPONTANEOUS, TRAUMATIC, THERAPEUTIC
OPEN or CLOSED
“TENSION” pneumothorax, “valvular” effect
“Bleb” rupture
Perforating injuries
Post needle biopsy
Слайд 73EFFUSIONS
TRANSUDATE (HYDROTHORAX)
EXUDATE (HYDROTHORAX)
BLOOD (HEMOTHORAX)
LYMPH (CHYLOTHORAX)
EFFUSIONS
TRANSUDATE (HYDROTHORAX)
EXUDATE (HYDROTHORAX)
BLOOD (HEMOTHORAX)
LYMPH (CHYLOTHORAX)
Слайд 74MESOTHELIOMAS
“Benign” vs. “Malignant” differentiation does not matter, but a self limited localized
MESOTHELIOMAS
“Benign” vs. “Malignant” differentiation does not matter, but a self limited localized
Слайд 75Typical growth appearance of a malignant mesothelioma, it compresses the lung from
Typical growth appearance of a malignant mesothelioma, it compresses the lung from
 Установки для подъема высокотемпературной жидкости, геотермальной энергетики
Установки для подъема высокотемпературной жидкости, геотермальной энергетики Постановка задачи
Постановка задачи Отчет команды об участии в онлайн-конкурсе кулинарного искусства Мастер Шеф
Отчет команды об участии в онлайн-конкурсе кулинарного искусства Мастер Шеф Россия на карте мира
Россия на карте мира НЕСПЕЦИФИЧЕСКИЕ И СПЕЦИФИЧЕСКИЕ ВТОРИЧНЫЕ КАРДИОМИОПАТИИ
НЕСПЕЦИФИЧЕСКИЕ И СПЕЦИФИЧЕСКИЕ ВТОРИЧНЫЕ КАРДИОМИОПАТИИ Внешняя среда ПАО Калориферный завод
Внешняя среда ПАО Калориферный завод Учебный план профильного обучения Методические аспекты составления в условиях перехода
Учебный план профильного обучения Методические аспекты составления в условиях перехода Оптимизация структуры активов и пассивов предпринимательской структуры в условиях неопределенности
Оптимизация структуры активов и пассивов предпринимательской структуры в условиях неопределенности Корпоративное мероприятие в клубном формате
Корпоративное мероприятие в клубном формате Диагностика. Психологическое сопровождение процесса реабилитации
Диагностика. Психологическое сопровождение процесса реабилитации Презентация на тему Как христианство пришло на Русь (4 класс)
Презентация на тему Как христианство пришло на Русь (4 класс) Презентация на тему Лекарства дома
Презентация на тему Лекарства дома  Вечный двигатель 10 класс
Вечный двигатель 10 класс Презентация на тему МЧС России
Презентация на тему МЧС России Строительство хозяйственно-бытовой канализации. Разработка проектно-сметной документации
Строительство хозяйственно-бытовой канализации. Разработка проектно-сметной документации Презентация на тему Рыночные отношения в здравоохранении
Презентация на тему Рыночные отношения в здравоохранении  Лекция 1
Лекция 1 ДЕНЬ НАРОДНОГО ЕДИНСТВА
ДЕНЬ НАРОДНОГО ЕДИНСТВА Презентация на тему Антуан де Монкретьен
Презентация на тему Антуан де Монкретьен Владимиро - Суздальская Русь
Владимиро - Суздальская Русь ГОУ СПО «Балаковское медицинское училище»Название исследования (например: Я и моё имя)Авторы: ФИО, группа, отделениеРуково
ГОУ СПО «Балаковское медицинское училище»Название исследования (например: Я и моё имя)Авторы: ФИО, группа, отделениеРуково Фиксированные ударения в языках
Фиксированные ударения в языках Галуа
Галуа Муртадха - презентация
Муртадха - презентация Dream Team - онлайн платформа в IT сфере
Dream Team - онлайн платформа в IT сфере Презентация на тему Петр Павлович Ершов
Презентация на тему Петр Павлович Ершов Система профориентации и основные её направления
Система профориентации и основные её направления Маски для волос. Выбираем расческу
Маски для волос. Выбираем расческу