- PEPTIC ULCER DISEASE

Содержание
- 2. History of epigastric pain present in 80-90 % of patient, but is nonspecific. Burning epigastric pain
- 3. PEPTIC ULCER DISEASE The term 'peptic ulcer' refers to an ulcer in the lower oesophagus, stomach
- 4. Ulcers are defined as a break in the mucosal surface >5 mm in size, with depth
- 5. Why does the ulcer appear ? Let’s remember the physiology of gastric secretion. Hydrochloric acid and
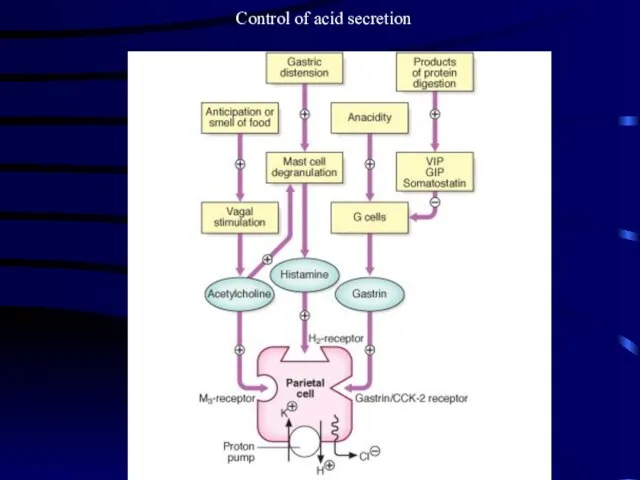
- 6. Control of acid secretion
- 7. The gastric epithelium is under a constant assault by a series of endogenous noxious factors including
- 8. The mucosal defense system can be envisioned as a three-level barrier, composed of preepithelial, epithelial, and
- 9. Surface epithelial cells provide the next line of defense through several factors, including mucus production, epithelial
- 10. Prostaglandins play a central role in gastric epithelial defense/repair. The gastric mucosa contains abundant levels of
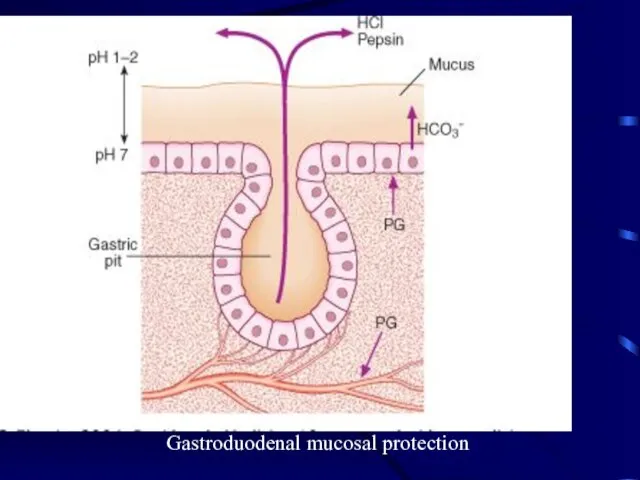
- 11. Gastroduodenal mucosal protection
- 12. GASTRIC AND DUODENAL ULCER Although the prevalence of peptic ulcer is decreasing in many Western communities,
- 13. Etiology: Helicobacter pylori In the industrialised world the prevalence of H. pylori infection in the general
- 14. The Bacterium initially named Campylobacter pyloridis, is a gram-negative microaerophilic rod found most commonly in the
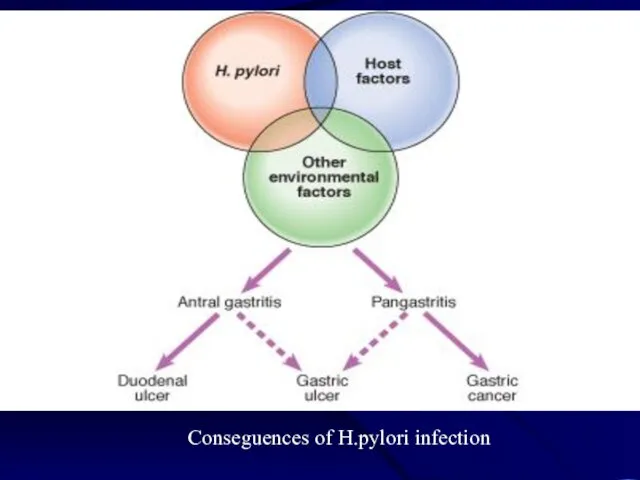
- 15. Conseguences of H.pylori infection
- 16. Pathogenesis and pathophysiology of infection
- 17. In most people H. pylori causes antral gastritis associated with depletion of somatostatin (from D cells)
- 18. In approximately 1% of infected people, H. pylori causes a pangastritis leading to gastric atrophy and
- 19. MISCELLANEOUS PATHOGENETIC FACTORS IN PEPTIC ULCER DISEASE Cigarette smoking Genetic predisposition Psychological stress Diet NSAID
- 20. Cigarette smoking has been implicated in the pathogenesis of PUD. Not only have smokers been found
- 21. Genetic predisposition has also been considered to play a role in ulcer development. First-degree relatives of
- 22. Psychological stress has been thought to contribute to PUD, but studies examining the role of psychological
- 23. Diet has also been thought to play a role in peptic diseases. Certain foods can cause
- 24. NSAIDs About 20,000 patients die each year from serious gastrointestinal complications from NSAIDs. Unfortunately, dyspeptic symptoms
- 25. Multiple factors play a role in the pathogenesis of PUD. The two predominant causes are H.
- 26. DUODENAL ULCERS DUs are estimated to occur in 6 to 15% of the western population. The
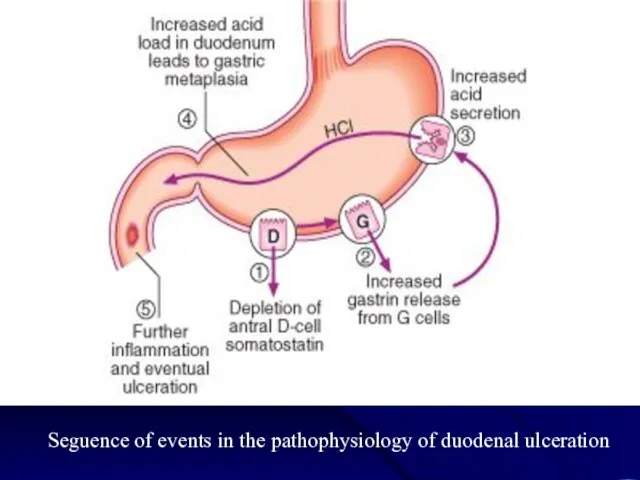
- 27. Seguence of events in the pathophysiology of duodenal ulceration
- 28. GASTRIC ULCERS As in DUs, the majority of GUs can be attributed to either H. pylori
- 29. Clinical features Abdominal pain is common to many gastrointestinal disorders, including DU and GU, but has
- 30. Epigastric pain described as a burning or gnawing discomfort can be present in both DU and
- 31. Variation in the intensity or distribution of the abdominal pain, as well as the onset of
- 32. Diagnostic Evaluation Including such methods as Barium studies of the proximal gastrointestinal tract, Endoscopy Several biopsy
- 33. Investigations The diagnosis can be made by double-contrast barium meal examination or by endoscopy. - Endoscopy
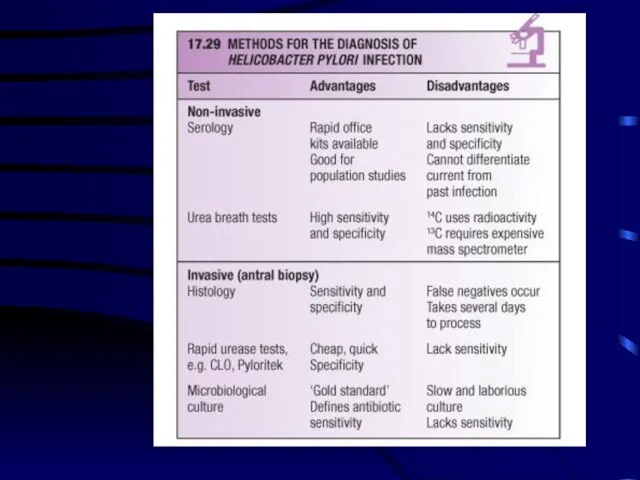
- 34. Tests for H. pylori Tests for H. pylori can be divided into two groups: invasive tests,
- 36. If endoscopy is performed, the most convenient biopsy-based test is the biopsy urease test, in which
- 37. The most consistently accurate test is the urea breath test. In this simple test, the patient
- 38. Management The aims of management are: - to relieve symptoms, - induce ulcer healing in the
- 39. H. pylori eradication First-line (triple) therapy: IPP at standart dose (12-hourly) for eg. - rabeprasol Amoxicillin
- 40. H. pylori eradication Second-line (quadruple) therapy: IPP at standart dose (12-hourly) bismuth 120 mg 6-hourly tetracicline
- 43. General measures Cigarette smoking, aspirin and NSAIDs should be avoided. Alcohol in moderation is not harmful
- 44. Short-term management Many different drugs are available for the short-term management of acid peptic symptoms -
- 45. Histamine H2-receptor antagonist drugs. These are competitive inhibitors of histamine at the H2-receptor on the parietal
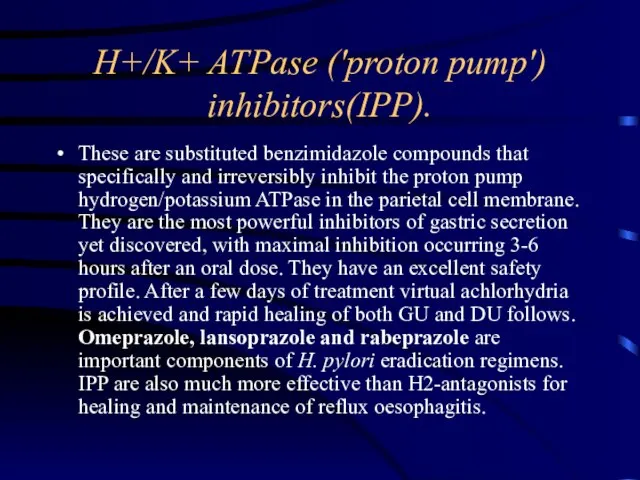
- 46. H+/K+ ATPase ('proton pump') inhibitors(IPP). These are substituted benzimidazole compounds that specifically and irreversibly inhibit the
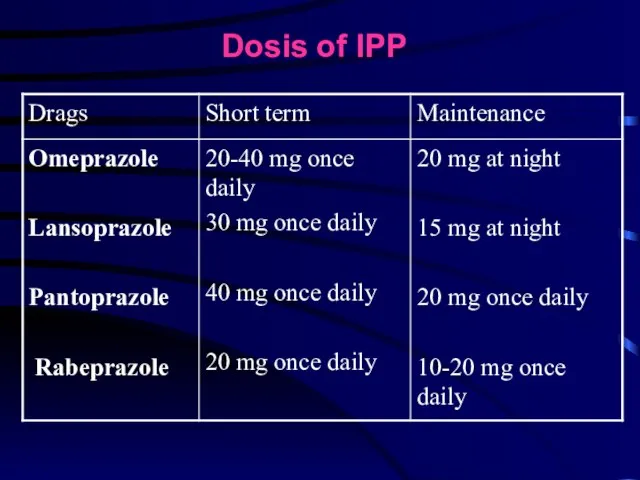
- 47. Dosis of IPP
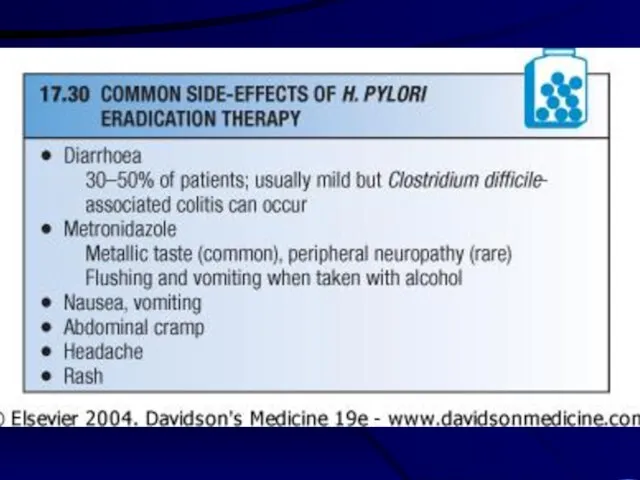
- 48. SIDE-EFFECTS of IPP Hipergastrinemia Diarrhoea Headache Rashes Interection with warfarin, phenytoin, fewer drugs
- 49. Colloidal bismuth compounds. Colloidal bismuth subcitrate (CBS) is an ammoniacal suspension of a complex colloidal bismuth
- 50. Synthetic prostaglandin analogues (misoprostol). Prostaglandins exert complex In low doses protect against injury induced by aspirin
- 51. Maintenance treatment Continuous maintenance treatment should not be necessary after successful H. pylori eradication. For the
- 52. INDICATIONS FOR SURGERY IN PEPTIC ULCER EMERGENCY - Perforation - Haemorrhage ELECTIVE - Gastric outflow obstruction
- 54. Скачать презентацию
Слайд 3PEPTIC ULCER DISEASE
The term 'peptic ulcer' refers to an ulcer in the
PEPTIC ULCER DISEASE
The term 'peptic ulcer' refers to an ulcer in the
Слайд 4Ulcers are defined as a break in the mucosal surface >5 mm
Ulcers are defined as a break in the mucosal surface >5 mm
Слайд 5Why does the ulcer appear ? Let’s remember the physiology of gastric
Why does the ulcer appear ? Let’s remember the physiology of gastric
Слайд 6Control of acid secretion
Control of acid secretion
Слайд 7The gastric epithelium is under a constant assault by a series of
The gastric epithelium is under a constant assault by a series of
Слайд 8The mucosal defense system can be envisioned as a three-level barrier, composed
The mucosal defense system can be envisioned as a three-level barrier, composed
Слайд 9Surface epithelial cells provide the next line of defense through several factors,
Surface epithelial cells provide the next line of defense through several factors,
Слайд 10Prostaglandins play a central role in gastric epithelial defense/repair. The gastric mucosa
Prostaglandins play a central role in gastric epithelial defense/repair. The gastric mucosa
Слайд 11Gastroduodenal mucosal protection
Gastroduodenal mucosal protection
Слайд 12GASTRIC AND DUODENAL ULCER
Although the prevalence of peptic ulcer is decreasing
GASTRIC AND DUODENAL ULCER
Although the prevalence of peptic ulcer is decreasing
Слайд 13Etiology: Helicobacter pylori
In the industrialised world the prevalence of H. pylori
Etiology: Helicobacter pylori
In the industrialised world the prevalence of H. pylori
Слайд 14The Bacterium initially named Campylobacter pyloridis, is a gram-negative microaerophilic rod found
The Bacterium initially named Campylobacter pyloridis, is a gram-negative microaerophilic rod found
Слайд 15Conseguences of H.pylori infection
Conseguences of H.pylori infection
Слайд 16Pathogenesis and pathophysiology of infection
Pathogenesis and pathophysiology of infection
Слайд 17In most people H. pylori causes antral gastritis associated with depletion of
In most people H. pylori causes antral gastritis associated with depletion of
Слайд 18In approximately 1% of infected people, H. pylori causes a pangastritis leading
In approximately 1% of infected people, H. pylori causes a pangastritis leading
Слайд 19MISCELLANEOUS PATHOGENETIC FACTORS IN PEPTIC ULCER DISEASE
Cigarette smoking
Genetic predisposition
Psychological stress
Diet
NSAID
MISCELLANEOUS PATHOGENETIC FACTORS IN PEPTIC ULCER DISEASE
Cigarette smoking
Genetic predisposition
Psychological stress
Diet
NSAID
Слайд 20Cigarette smoking
has been implicated in the pathogenesis of PUD. Not only
Cigarette smoking
has been implicated in the pathogenesis of PUD. Not only
Слайд 21Genetic predisposition
has also been considered to play a role in ulcer development.
Genetic predisposition
has also been considered to play a role in ulcer development.
Слайд 22Psychological stress
has been thought to contribute to PUD, but studies examining
Psychological stress
has been thought to contribute to PUD, but studies examining
Слайд 23Diet
has also been thought to play a role in peptic diseases. Certain
Diet
has also been thought to play a role in peptic diseases. Certain
Слайд 24NSAIDs
About 20,000 patients die each year from serious gastrointestinal complications from NSAIDs.
NSAIDs
About 20,000 patients die each year from serious gastrointestinal complications from NSAIDs.
Слайд 25Multiple factors play a role in the pathogenesis of PUD. The two
Multiple factors play a role in the pathogenesis of PUD. The two
Слайд 26DUODENAL ULCERS
DUs are estimated to occur in 6 to 15% of the
DUODENAL ULCERS
DUs are estimated to occur in 6 to 15% of the
Слайд 27Seguence of events in the pathophysiology of duodenal ulceration
Seguence of events in the pathophysiology of duodenal ulceration
Слайд 28GASTRIC ULCERS
As in DUs, the majority of GUs can be attributed to
GASTRIC ULCERS
As in DUs, the majority of GUs can be attributed to
Слайд 29Clinical features
Abdominal pain is common to many gastrointestinal disorders, including DU
Clinical features
Abdominal pain is common to many gastrointestinal disorders, including DU
Слайд 30Epigastric pain described as a burning or gnawing discomfort can be present
Epigastric pain described as a burning or gnawing discomfort can be present
Слайд 31Variation in the intensity or distribution of the abdominal pain, as well
Variation in the intensity or distribution of the abdominal pain, as well
Слайд 32Diagnostic Evaluation
Including such methods as
Barium studies of the proximal gastrointestinal tract,
Endoscopy
Several biopsy
Diagnostic Evaluation
Including such methods as
Barium studies of the proximal gastrointestinal tract,
Endoscopy
Several biopsy
Слайд 33Investigations
The diagnosis can be made by double-contrast barium meal examination or
Investigations
The diagnosis can be made by double-contrast barium meal examination or
Слайд 34Tests for H. pylori
Tests for H. pylori can be divided into two
Tests for H. pylori
Tests for H. pylori can be divided into two
Слайд 36If endoscopy is performed, the most convenient biopsy-based test is the biopsy
If endoscopy is performed, the most convenient biopsy-based test is the biopsy
Слайд 37The most consistently accurate test is the urea breath test. In this
The most consistently accurate test is the urea breath test. In this
Слайд 38Management
The aims of management are:
- to relieve symptoms,
- induce ulcer healing
Management
The aims of management are:
- to relieve symptoms,
- induce ulcer healing
Слайд 39H. pylori eradication
First-line (triple) therapy:
IPP at standart dose (12-hourly) for
H. pylori eradication
First-line (triple) therapy:
IPP at standart dose (12-hourly) for
Слайд 40H. pylori eradication
Second-line (quadruple) therapy:
IPP at standart dose (12-hourly)
bismuth 120 mg
H. pylori eradication
Second-line (quadruple) therapy:
IPP at standart dose (12-hourly)
bismuth 120 mg
Слайд 43General measures
Cigarette smoking, aspirin and NSAIDs should be avoided.
Alcohol in
General measures
Cigarette smoking, aspirin and NSAIDs should be avoided.
Alcohol in
Слайд 44Short-term management
Many different drugs are available for the short-term management
Short-term management
Many different drugs are available for the short-term management
Слайд 45 Histamine H2-receptor antagonist drugs.
These are competitive inhibitors of histamine at
Histamine H2-receptor antagonist drugs.
These are competitive inhibitors of histamine at
Слайд 46H+/K+ ATPase ('proton pump') inhibitors(IPP).
These are substituted benzimidazole compounds that specifically
H+/K+ ATPase ('proton pump') inhibitors(IPP).
These are substituted benzimidazole compounds that specifically
Слайд 47Dosis of IPP
Dosis of IPP
Слайд 48SIDE-EFFECTS of IPP
Hipergastrinemia
Diarrhoea
Headache
Rashes
Interection with warfarin, phenytoin, fewer drugs
SIDE-EFFECTS of IPP
Hipergastrinemia
Diarrhoea
Headache
Rashes
Interection with warfarin, phenytoin, fewer drugs
Слайд 49Colloidal bismuth compounds.
Colloidal bismuth subcitrate (CBS) is an ammoniacal suspension of
Colloidal bismuth compounds.
Colloidal bismuth subcitrate (CBS) is an ammoniacal suspension of
Слайд 50Synthetic prostaglandin analogues (misoprostol).
Prostaglandins exert complex In low doses protect against
Synthetic prostaglandin analogues (misoprostol).
Prostaglandins exert complex In low doses protect against
Слайд 51Maintenance treatment
Continuous maintenance treatment should not be necessary after successful H.
Maintenance treatment
Continuous maintenance treatment should not be necessary after successful H.
Слайд 52INDICATIONS FOR SURGERY IN PEPTIC ULCER
EMERGENCY
- Perforation
- Haemorrhage
ELECTIVE
-
INDICATIONS FOR SURGERY IN PEPTIC ULCER
EMERGENCY
- Perforation
- Haemorrhage
ELECTIVE
-
 Система национальных счетов (СНС)
Система национальных счетов (СНС) Foundation for sustainable ICT solutions MEC.mk - Model for Efficient Communication between the Commissions for Interethnic Relations and the Citizens.
Foundation for sustainable ICT solutions MEC.mk - Model for Efficient Communication between the Commissions for Interethnic Relations and the Citizens. крылов
крылов Студия декоративно - прикладного творчества
Студия декоративно - прикладного творчества Spotlight 5 Starter Ур 3 транскипция
Spotlight 5 Starter Ур 3 транскипция ФК "Приалит
ФК "Приалит 00
00 РМО учителей биологии и экологии
РМО учителей биологии и экологии МК_LbHqUSn
МК_LbHqUSn Информация как объект правовый отношений
Информация как объект правовый отношений Развитие творческих способностей учащихся начальной школы в процессе изучения английского языка
Развитие творческих способностей учащихся начальной школы в процессе изучения английского языка Роль Тюменских купцов в развитии образования г.Тюмени
Роль Тюменских купцов в развитии образования г.Тюмени Активные методы обучения как средство формирования устойчивой мотивации изучения иностранного языка
Активные методы обучения как средство формирования устойчивой мотивации изучения иностранного языка Новогодние мероприятия
Новогодние мероприятия Либералы, консерваторы, социалисты: какими должны быть общество и государство
Либералы, консерваторы, социалисты: какими должны быть общество и государство Источники финансирования бизнеса
Источники финансирования бизнеса Набросок фигуры человека с натуры
Набросок фигуры человека с натуры CoinCasher 2021 Convienience
CoinCasher 2021 Convienience Презентация на тему Основные направления налогово-бюджетной политики России в современных условиях
Презентация на тему Основные направления налогово-бюджетной политики России в современных условиях  Научные основания специальной педагогики. Психологические основы специальной педагогики
Научные основания специальной педагогики. Психологические основы специальной педагогики Решение для массовой печати бланков аттестатов выпускников учреждений образования
Решение для массовой печати бланков аттестатов выпускников учреждений образования Восстановительный способ разрешения конфликтов
Восстановительный способ разрешения конфликтов Арены (10 класс)
Арены (10 класс) ПОДРОСТОК КАК ГРАЖДАНИН
ПОДРОСТОК КАК ГРАЖДАНИН Мода 19 века.
Мода 19 века. Роль кластеров в развитии регионов
Роль кластеров в развитии регионов Школьная служба примирения «Апельсин» МОУ «СОШ №27» г. Перми,ул. Шишкина,18, 255-59-44,Руководител
Школьная служба примирения «Апельсин» МОУ «СОШ №27» г. Перми,ул. Шишкина,18, 255-59-44,Руководител Прямые и отрезки
Прямые и отрезки