- Percussion of the lungs Palpation of the chest

Содержание
- 2. Inspection of the chest (inspectio thoracis) This is the objective method of examination based on visual
- 3. Static inspection Physiological shapes : Normosthenic, Hypersthenic, Asthenic The asymmetry of the chest (enlarged volume of
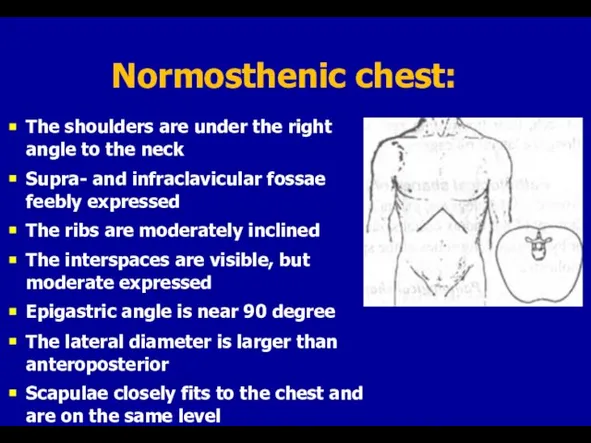
- 4. Normosthenic chest: The shoulders are under the right angle to the neck Supra- and infraclavicular fossae
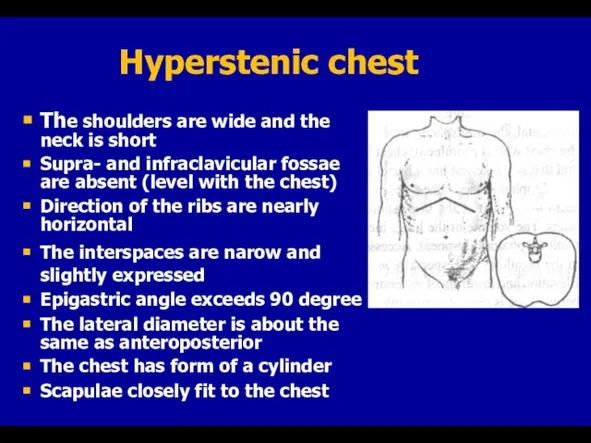
- 5. Hyperstenic chest The shoulders are wide and the neck is short Supra- and infraclavicular fossae are
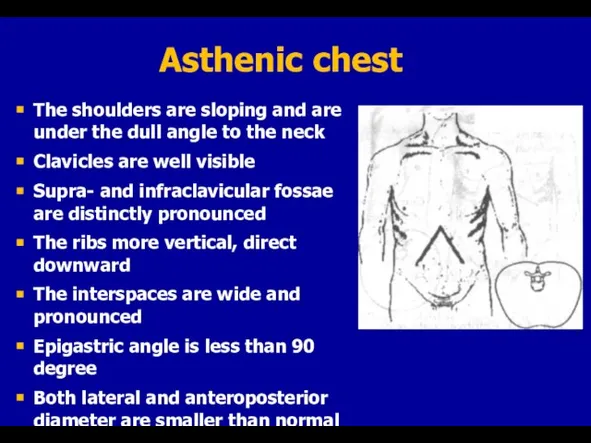
- 6. Asthenic chest The shoulders are sloping and are under the dull angle to the neck Clavicles
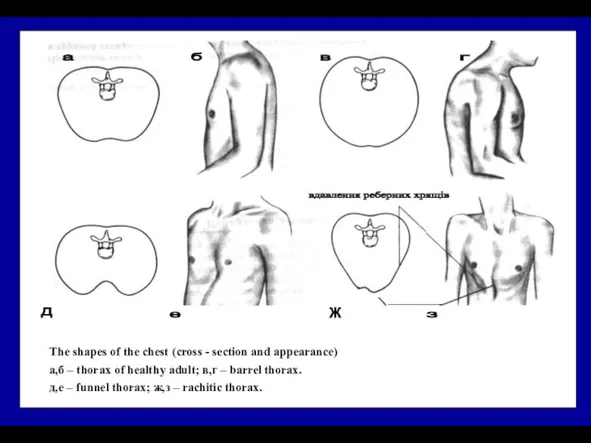
- 7. The shapes of the chest (cross - section and appearance) а,б – thorax of healthy adult;
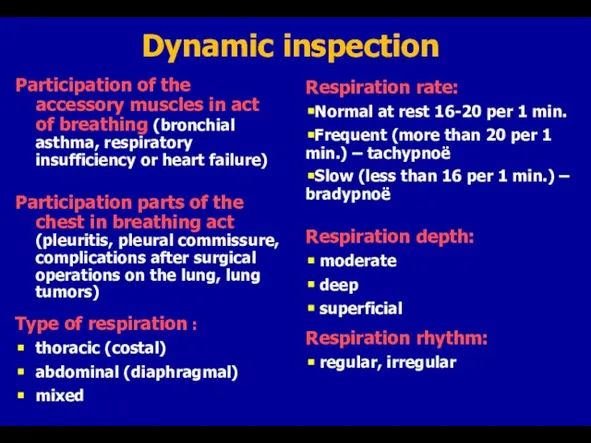
- 8. Dynamic inspection Participation of the accessory muscles in act of breathing (bronchial asthma, respiratory insufficiency or
- 9. Palpation Identification of tender areas (widespread or local, in Valle points ) Thorax resistance (normal, increased,
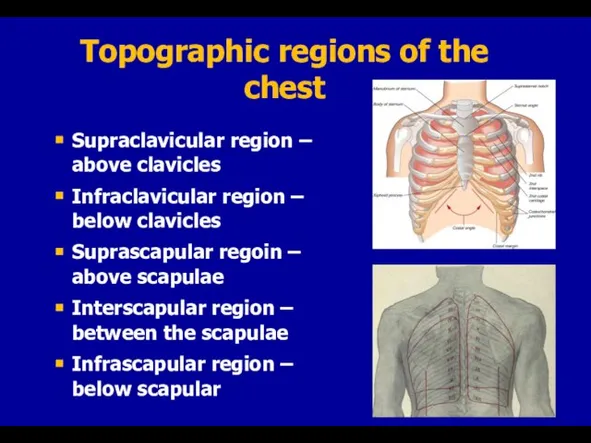
- 10. Topographic regions of the chest Supraclavicular region – above clavicles Infraclavicular region – below clavicles Suprascapular
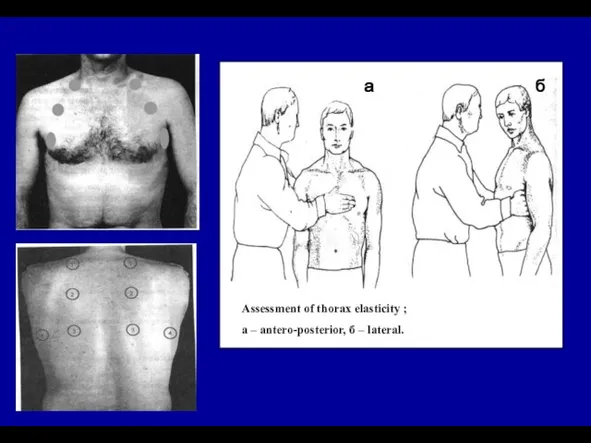
- 11. Assessment of thorax elasticity ; а – antero-posterior, б – lateral.
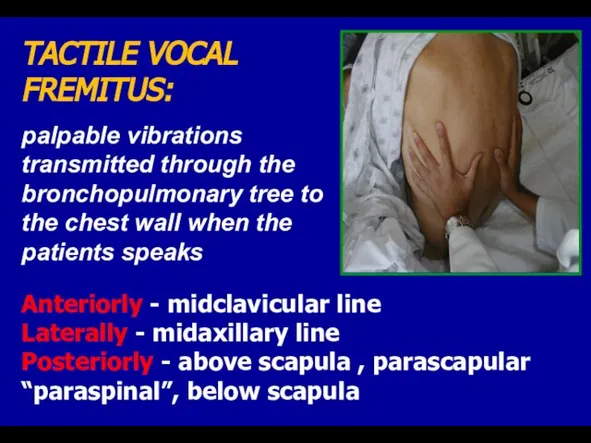
- 12. TACTILE VOCAL FREMITUS: palpable vibrations transmitted through the bronchopulmonary tree to the chest wall when the
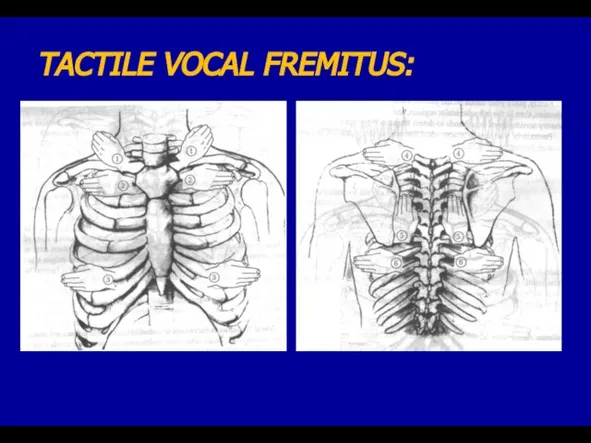
- 13. TACTILE VOCAL FREMITUS:
- 14. Increased TVF Thin chest wall Lobar pneumonia Lungs infarction Pulmonary tumor Tuberculosis Compressive atelectasis Air cavity
- 15. Palpation of the chest
- 16. Palpation of the chest
- 17. (L.Auenbrugger, 1722-1809) (Jean Nicholas Corvisart, 1755-1821)
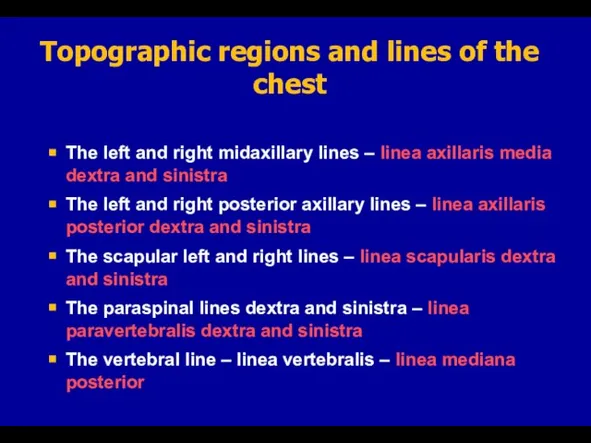
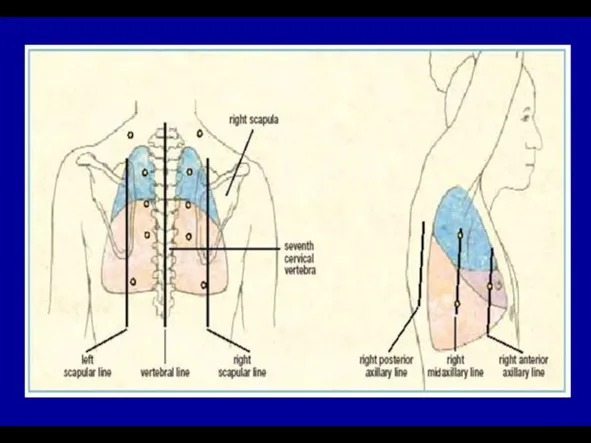
- 18. Topographic regions and lines of the chest
- 19. The left and right midaxillary lines – linea axillaris media dextra and sinistra The left and
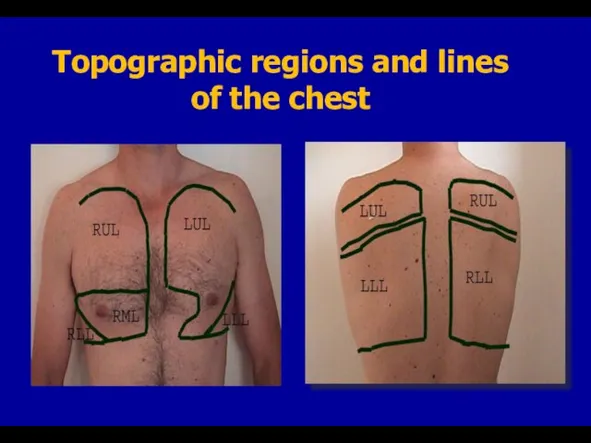
- 21. Topographic regions and lines of the chest
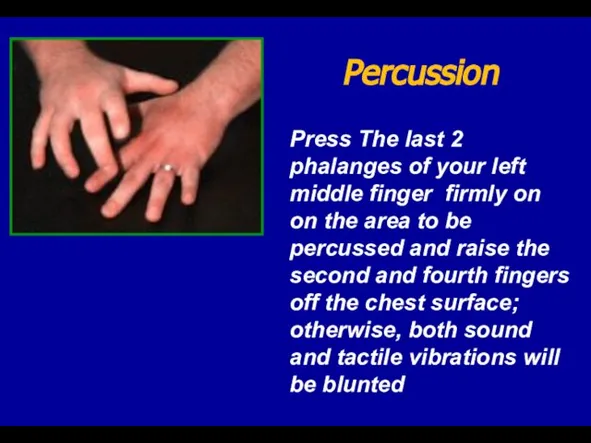
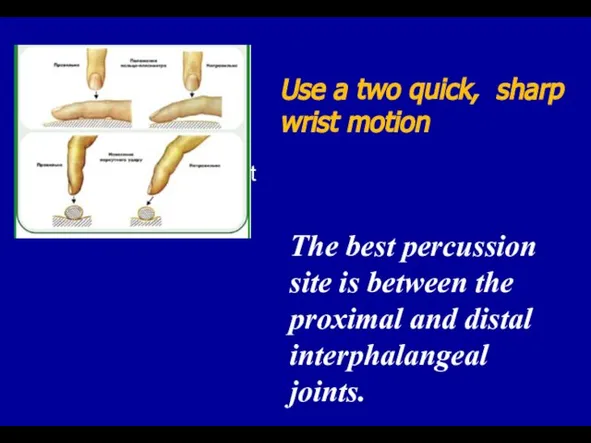
- 22. Press The last 2 phalanges of your left middle finger firmly on on the area to
- 23. Movement from wrist The best percussion site is between the proximal and distal interphalangeal joints. Use
- 24. Comparative – revealing of percussion sound features on symmetrical areas of the chest: Supraclavicularis Clavicularis Subclavicularis
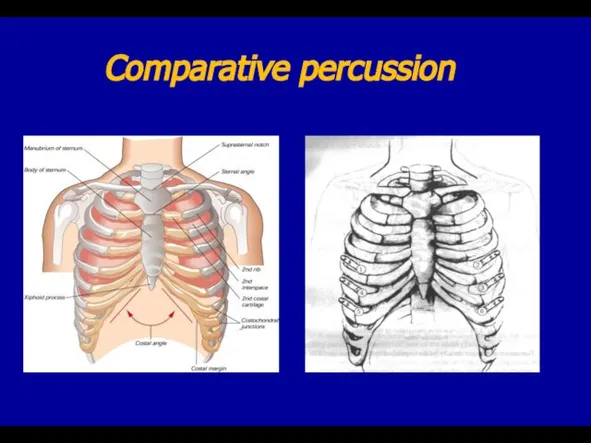
- 25. Comparative percussion
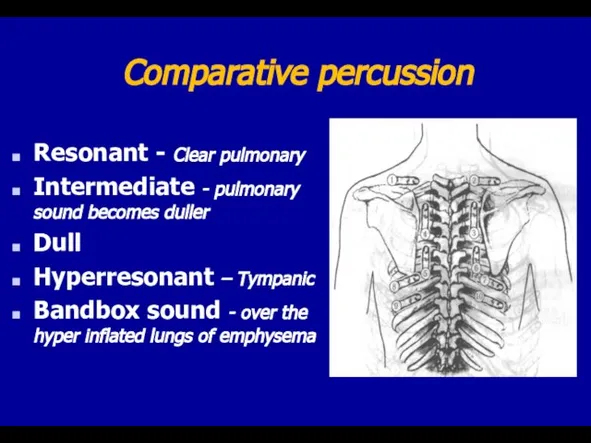
- 26. Comparative percussion Resonant - Clear pulmonary Intermediate - pulmonary sound becomes duller Dull Hyperresonant – Tympanic
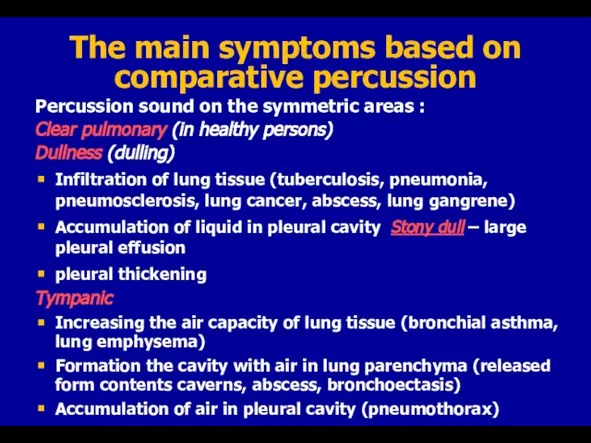
- 27. The main symptoms based on comparative percussion Percussion sound on the symmetric areas : Clear pulmonary
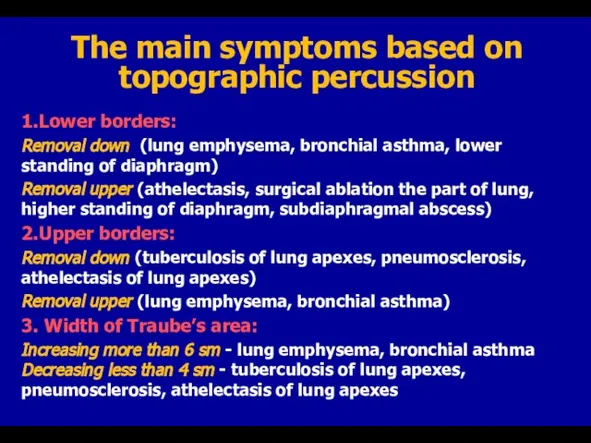
- 28. The main symptoms based on topographic percussion 1.Lower borders: Removal down (lung emphysema, bronchial asthma, lower
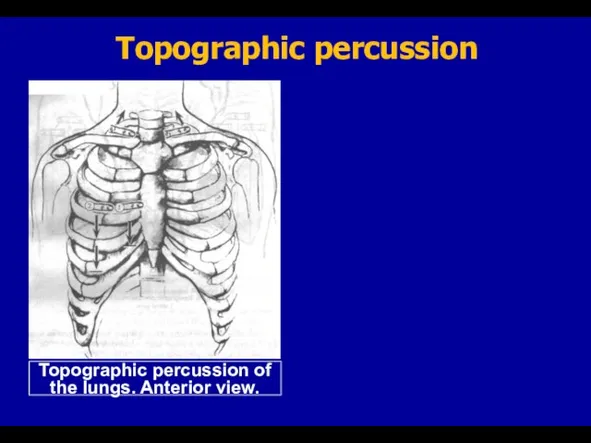
- 29. Topographic percussion
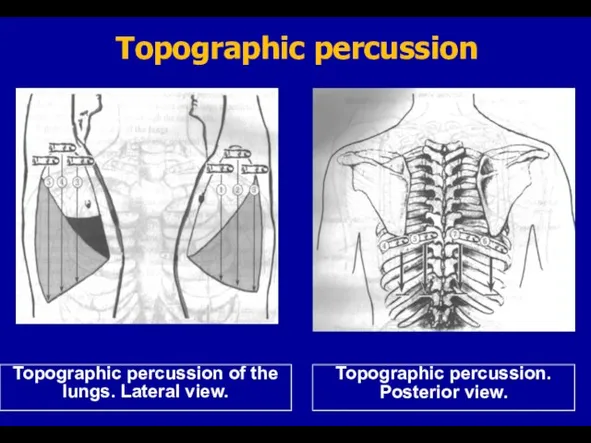
- 30. Topographic percussion
- 31. Topographic percussion lower borders of the lung
- 32. 4. Active and passive mobility of the lungs – the significance of lung tissue elasticity state
- 33. Determining of the mobility of lower borders of the lungs
- 35. Скачать презентацию
Слайд 3Static inspection
Physiological shapes :
Normosthenic,
Hypersthenic,
Asthenic
The asymmetry of the chest (enlarged
Static inspection
Physiological shapes :
Normosthenic,
Hypersthenic,
Asthenic
The asymmetry of the chest (enlarged
Слайд 4Normosthenic chest:
The shoulders are under the right angle to the neck
Supra- and
Normosthenic chest:
The shoulders are under the right angle to the neck
Supra- and
Слайд 5Hyperstenic chest
The shoulders are wide and the neck is short
Supra- and infraclavicular
Hyperstenic chest
The shoulders are wide and the neck is short
Supra- and infraclavicular
Слайд 6Asthenic chest
The shoulders are sloping and are under the dull angle to
Asthenic chest
The shoulders are sloping and are under the dull angle to
Слайд 7The shapes of the chest (cross - section and appearance)
а,б – thorax
The shapes of the chest (cross - section and appearance)
а,б – thorax
Слайд 8Dynamic inspection
Participation of the accessory muscles in act of breathing (bronchial asthma,
Dynamic inspection
Participation of the accessory muscles in act of breathing (bronchial asthma,
Слайд 9Palpation
Identification of tender areas (widespread or local, in Valle points )
Thorax resistance
Palpation
Identification of tender areas (widespread or local, in Valle points )
Thorax resistance
Слайд 10Topographic regions of the chest
Supraclavicular region – above clavicles
Infraclavicular region – below
Topographic regions of the chest
Supraclavicular region – above clavicles
Infraclavicular region – below
Слайд 11
Assessment of thorax elasticity ;
а – antero-posterior, б – lateral.
Assessment of thorax elasticity ;
а – antero-posterior, б – lateral.
Слайд 12TACTILE VOCAL FREMITUS:
palpable vibrations transmitted through the bronchopulmonary tree to the chest
TACTILE VOCAL FREMITUS:
palpable vibrations transmitted through the bronchopulmonary tree to the chest
Слайд 13TACTILE VOCAL FREMITUS:
TACTILE VOCAL FREMITUS:
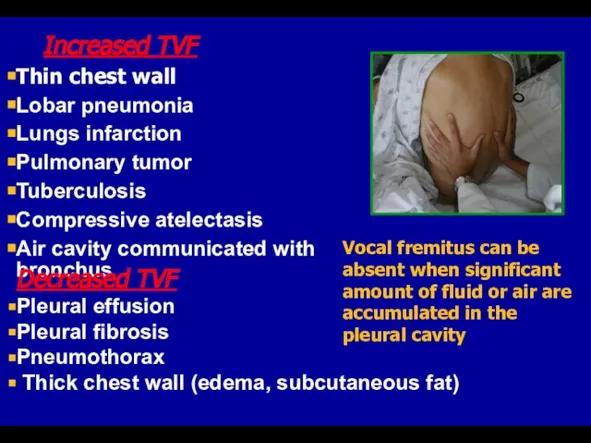
Слайд 14 Increased TVF
Thin chest wall
Lobar pneumonia
Lungs infarction
Pulmonary tumor
Tuberculosis
Compressive atelectasis
Air cavity communicated with bronchus
Decreased
Increased TVF
Thin chest wall
Lobar pneumonia
Lungs infarction
Pulmonary tumor
Tuberculosis
Compressive atelectasis
Air cavity communicated with bronchus
Decreased
Слайд 15Palpation of the chest
Palpation of the chest
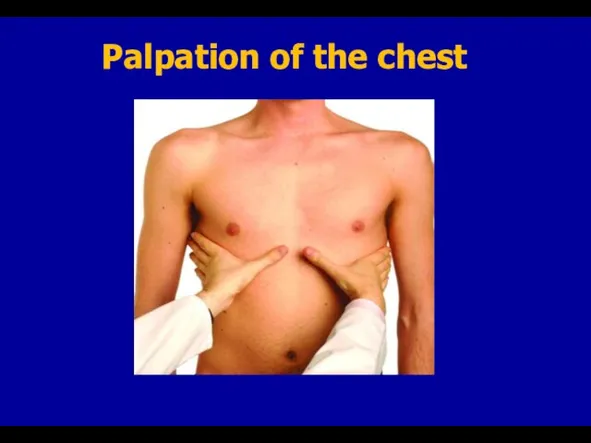
Слайд 16Palpation of the chest
Palpation of the chest

Слайд 17(L.Auenbrugger, 1722-1809)
(Jean Nicholas Corvisart, 1755-1821)
(L.Auenbrugger, 1722-1809)
(Jean Nicholas Corvisart, 1755-1821)
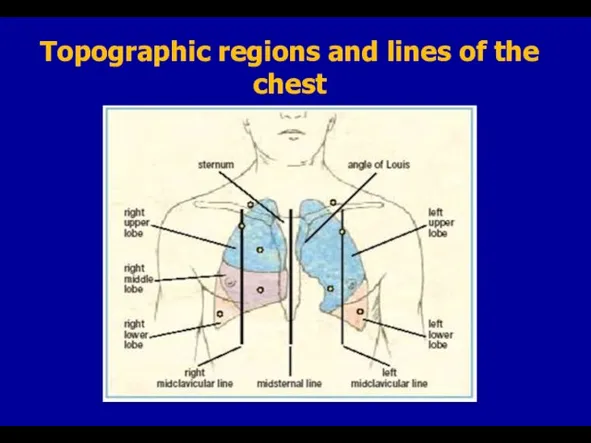
Слайд 18Topographic regions and lines of the chest
Topographic regions and lines of the chest
Слайд 19The left and right midaxillary lines – linea axillaris media dextra and
The left and right midaxillary lines – linea axillaris media dextra and
Слайд 21Topographic regions and lines of the chest
Topographic regions and lines of the chest
Слайд 22Press The last 2 phalanges of your left middle finger firmly on
Press The last 2 phalanges of your left middle finger firmly on
Слайд 23Movement from wrist
The best percussion site is between the proximal and distal
Movement from wrist
The best percussion site is between the proximal and distal
Слайд 24Comparative – revealing of percussion sound features on symmetrical areas of the
Comparative – revealing of percussion sound features on symmetrical areas of the
Слайд 25Comparative percussion
Comparative percussion
Слайд 26Comparative percussion
Resonant - Clear pulmonary
Intermediate - pulmonary sound becomes duller
Dull
Hyperresonant –
Comparative percussion
Resonant - Clear pulmonary
Intermediate - pulmonary sound becomes duller
Dull
Hyperresonant –
Слайд 27The main symptoms based on comparative percussion
Percussion sound on the symmetric areas
The main symptoms based on comparative percussion
Percussion sound on the symmetric areas
Слайд 28The main symptoms based on topographic percussion
1.Lower borders:
Removal down (lung emphysema,
The main symptoms based on topographic percussion
1.Lower borders:
Removal down (lung emphysema,
Слайд 29Topographic percussion
Topographic percussion
Слайд 30Topographic percussion
Topographic percussion
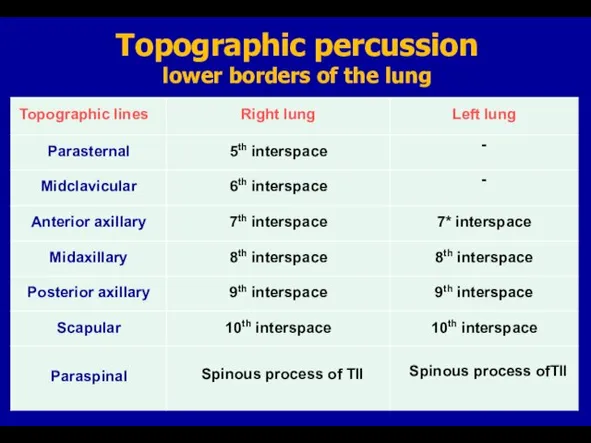
Слайд 31Topographic percussion
lower borders of the lung
Topographic percussion
lower borders of the lung
Слайд 324. Active and passive mobility of the lungs – the significance of
4. Active and passive mobility of the lungs – the significance of
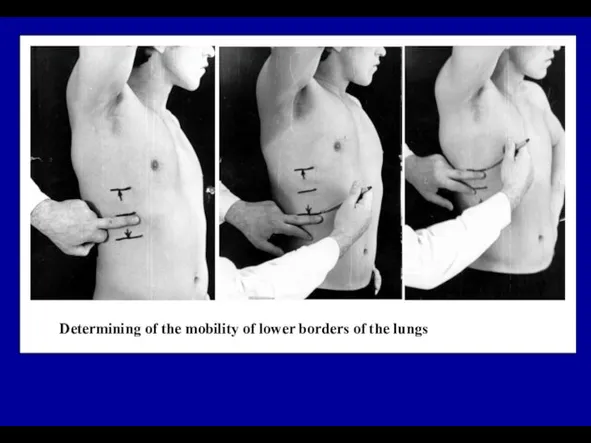
Слайд 33Determining of the mobility of lower borders of the lungs
Determining of the mobility of lower borders of the lungs
 Финансы в экономике
Финансы в экономике Дополнительное телематическое оборудование в авто Remoto
Дополнительное телематическое оборудование в авто Remoto The sights of America
The sights of America 98696487
98696487 Собака динго
Собака динго Презентация на тему Этическая основа культуры
Презентация на тему Этическая основа культуры Влияние воды и водных процедур на здоровье человека
Влияние воды и водных процедур на здоровье человека 제5과. 말하기
제5과. 말하기 Создавать видимость активной работы Минимизировать ответственность и риски Сохранить хорошую мину Получать большую зарплату КАК
Создавать видимость активной работы Минимизировать ответственность и риски Сохранить хорошую мину Получать большую зарплату КАК Химия атмосферы и поверхности.
Химия атмосферы и поверхности. Насилие в произведениях искусства
Насилие в произведениях искусства Основы мировых религиозных культур « Вся культура – из храма» Дж. Фрэзер Автор: д.и.н., доцент Сушко А.В. Омск – 2012.
Основы мировых религиозных культур « Вся культура – из храма» Дж. Фрэзер Автор: д.и.н., доцент Сушко А.В. Омск – 2012. Что изучает история Древнего мира (5 класс)
Что изучает история Древнего мира (5 класс) Алесь Разанау
Алесь Разанау 8Г2_2022-10-12_урок 11_devoir (1)
8Г2_2022-10-12_урок 11_devoir (1) Первая постановка комедии «Ревизор»
Первая постановка комедии «Ревизор» Гипоталамус
Гипоталамус  Современная концепция управления проектом
Современная концепция управления проектом Маковельская Инна Николаевна
Маковельская Инна Николаевна Соотношение финансового права и финансового законодательства
Соотношение финансового права и финансового законодательства Организация наставничества на государственной гражданской службе
Организация наставничества на государственной гражданской службе Федорко Надежда Никифоровна
Федорко Надежда Никифоровна Present simple versus present continuous
Present simple versus present continuous Почему кошки так называются?
Почему кошки так называются? Фонетика (урок-повторение, 6 класс)
Фонетика (урок-повторение, 6 класс) Особые образовательные потребности
Особые образовательные потребности Уважаемые преподаватели, аспиранты и студенты РГЭУ (РИНХ)! Представляем вам новую специальную литературу (учебники и монографии),
Уважаемые преподаватели, аспиранты и студенты РГЭУ (РИНХ)! Представляем вам новую специальную литературу (учебники и монографии), Работа со списками. Колонки. Буквица. Стили
Работа со списками. Колонки. Буквица. Стили