- Spinal Injuries M. Jamous M. D.

Содержание
- 2. Spinal Injuries Incidence 30-40/ 1,000,000 person The mortality rate 40-50% Most common in the cervical region
- 3. Acute evaluation and ER management Strict spine precautions (immobilization) Emergency resuscitation (ABC..) Comprehensive approach Always expect
- 4. Neurological and radiological evaluation In awake patients, both motor and sensory examinations in all extremeties Unconcious
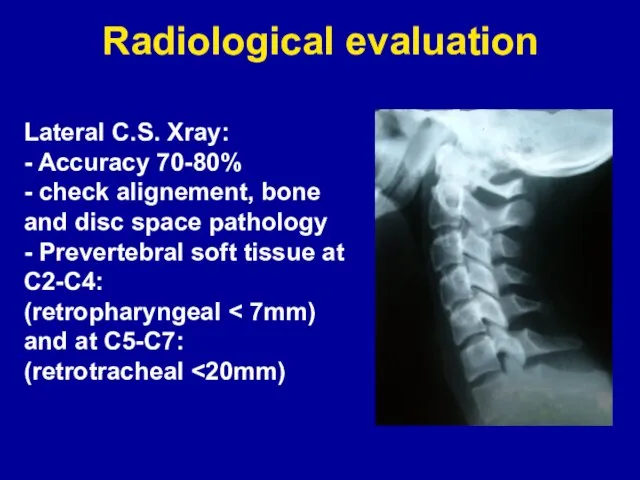
- 5. Radiological evaluation Lateral C.S. Xray: - Accuracy 70-80% - check alignement, bone and disc space pathology
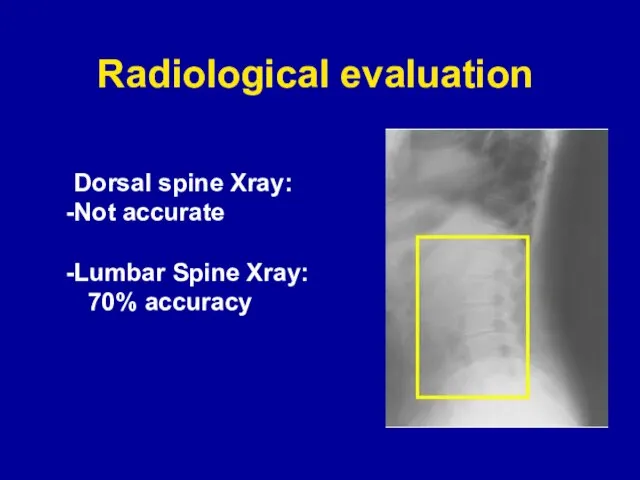
- 6. Radiological evaluation Dorsal spine Xray: Not accurate Lumbar Spine Xray: 70% accuracy
- 7. Radiological evaluation CT scan and MRI in case of clinical suspicion or abnormal Xray
- 8. Spinal Injuries Spinal Column Injuries Injuries to Neural Structures (spinal cord, nerve roots) ±
- 9. Neural injury secondary injury • local swelling at the site of injury which pinches off blood
- 10. General Management Guidelines Role of steroids The North American Spinal Cord Injury Study (NASCIS) showed definite
- 11. Spinal Shock Transient loss of all neurological function (motor, sensory, and autonomic) below the injury level
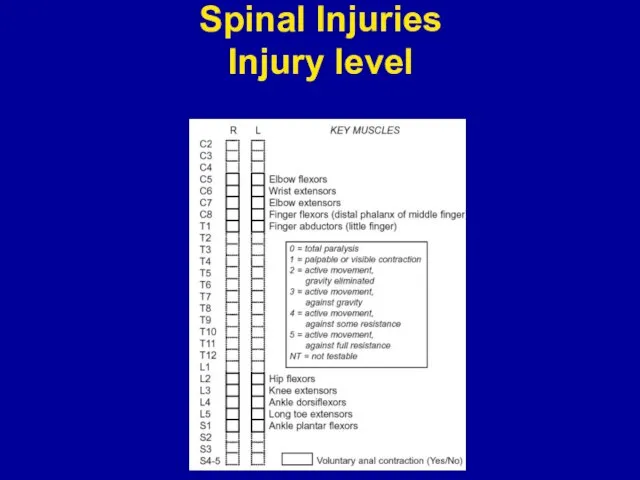
- 12. Spinal Injuries Injury level
- 13. Spinal Injuries ASIA IMPAIRMENT SCALE: A =Complete: No motor or sensory function is preserved B =Incomplete:
- 14. Incomplete Spinal Injuries CLINICAL SYNDROMES: Central Cord: greater motor deficit in the upper extremities Brown-Sequard: dissociated
- 15. Incomplete Spinal Injuries CLINICAL SYNDROMES: Conus Medullaris: saddle anesthesia, incontinence (painless, symmetrical) Cauda Equina: saddle anesthesia,
- 16. Spinal Column Injury Atlanto-occipital dislocation Atlanto-occipital dislocation (AOD) is a devastating condition that frequently results in
- 17. Spinal Column Injury Atlanto-Axial dislocation Lower mortality than Atlanto-occipital dislocation 1/3 of patients have deficit Transverse
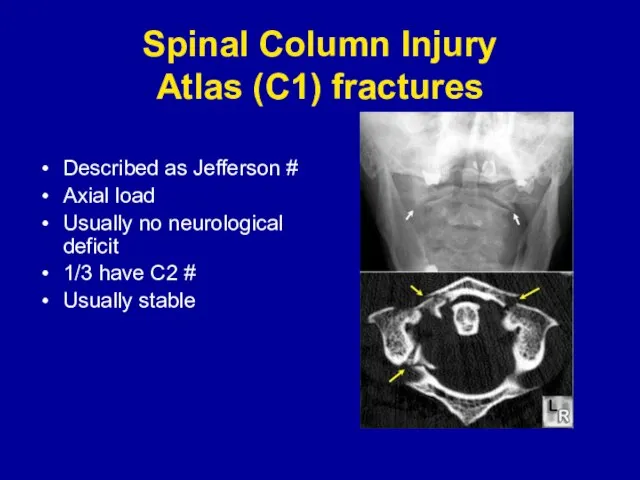
- 18. Spinal Column Injury Atlas (C1) fractures Described as Jefferson # Axial load Usually no neurological deficit
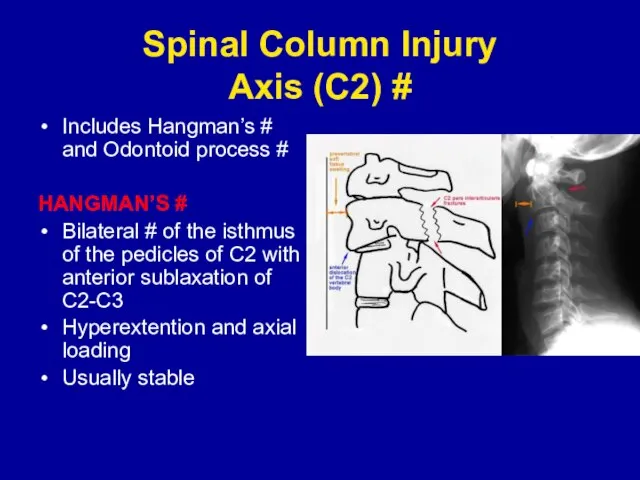
- 19. Spinal Column Injury Axis (C2) # Includes Hangman’s # and Odontoid process # HANGMAN’S # Bilateral
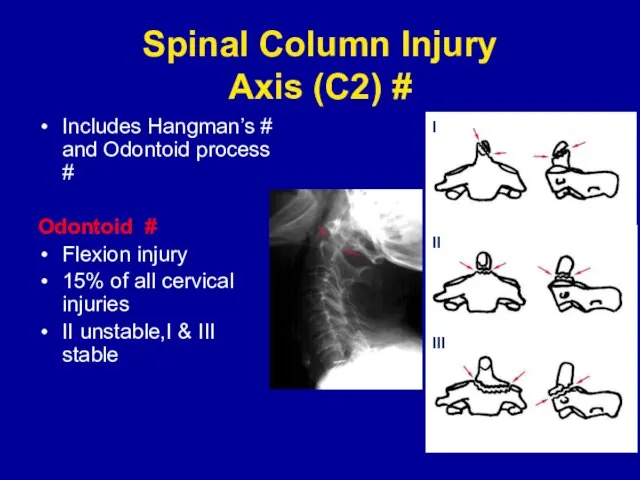
- 20. Spinal Column Injury Axis (C2) # Includes Hangman’s # and Odontoid process # Odontoid # Flexion
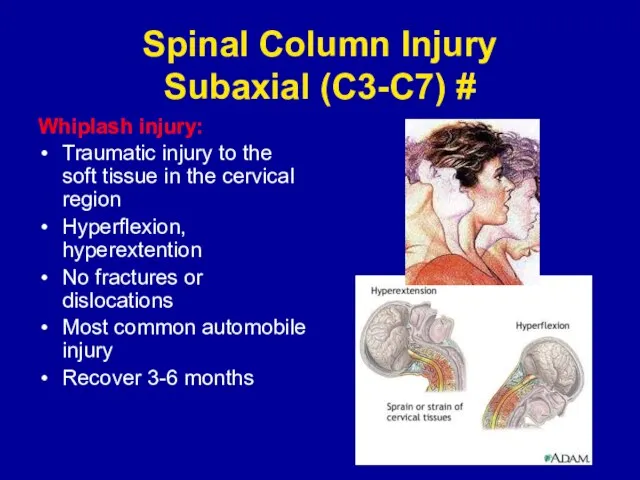
- 21. Spinal Column Injury Subaxial (C3-C7) # Whiplash injury: Traumatic injury to the soft tissue in the
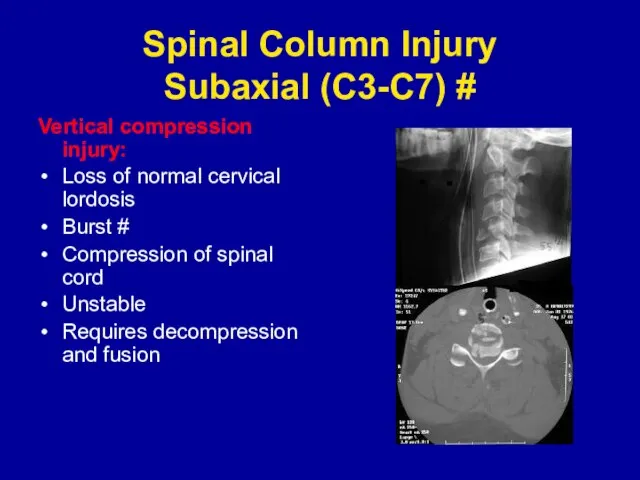
- 22. Spinal Column Injury Subaxial (C3-C7) # Vertical compression injury: Loss of normal cervical lordosis Burst #
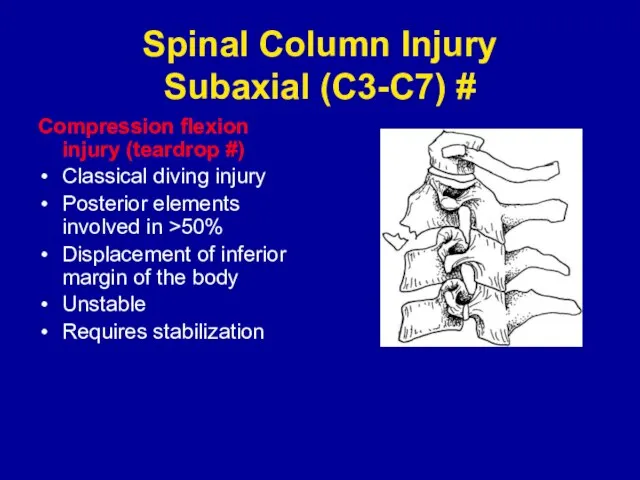
- 23. Spinal Column Injury Subaxial (C3-C7) # Compression flexion injury (teardrop #) Classical diving injury Posterior elements
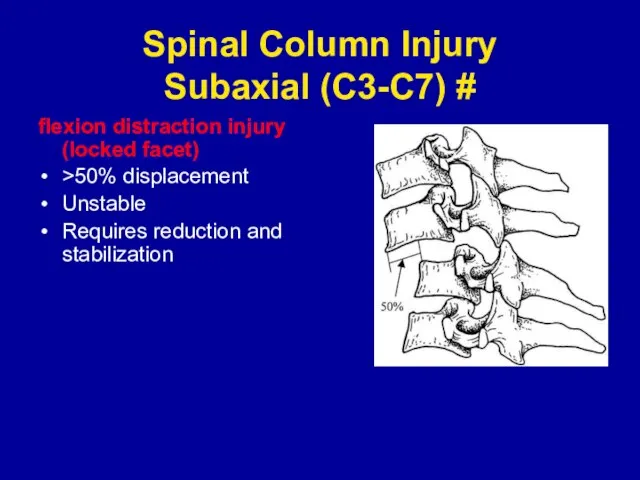
- 24. Spinal Column Injury Subaxial (C3-C7) # flexion distraction injury (locked facet) >50% displacement Unstable Requires reduction
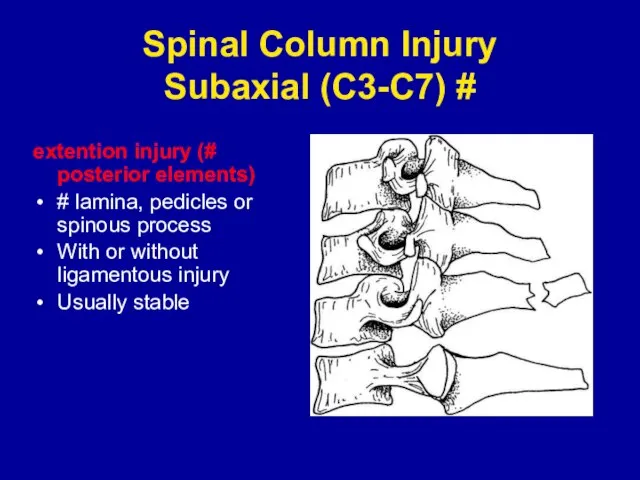
- 25. Spinal Column Injury Subaxial (C3-C7) # extention injury (# posterior elements) # lamina, pedicles or spinous
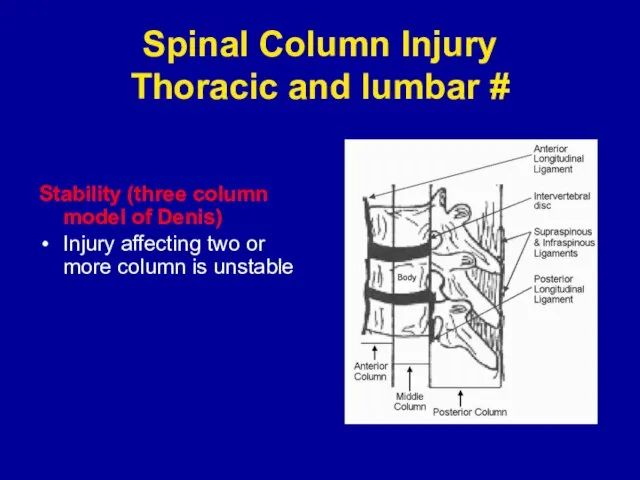
- 26. Spinal Column Injury Thoracic and lumbar # Stability (three column model of Denis) Injury affecting two
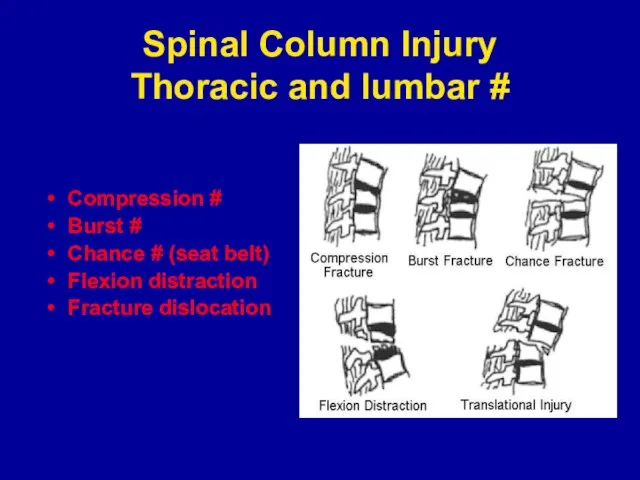
- 27. Spinal Column Injury Thoracic and lumbar # Compression # Burst # Chance # (seat belt) Flexion
- 28. General Management Guidelines Strict spine precautions (immobilization) Emergency resuscitation (ABC..) Comprehensive approach Neurological and Radiological assesment.
- 30. Скачать презентацию
Слайд 2Spinal Injuries
Incidence 30-40/ 1,000,000 person
The mortality rate 40-50%
Most common in the cervical
Spinal Injuries
Incidence 30-40/ 1,000,000 person
The mortality rate 40-50%
Most common in the cervical
Слайд 3Acute evaluation and ER management
Strict spine precautions (immobilization)
Emergency resuscitation (ABC..)
Comprehensive approach
Always expect
Acute evaluation and ER management
Strict spine precautions (immobilization)
Emergency resuscitation (ABC..)
Comprehensive approach
Always expect
Слайд 4Neurological and radiological evaluation
In awake patients, both motor and sensory examinations in
Neurological and radiological evaluation
In awake patients, both motor and sensory examinations in
Слайд 5Radiological evaluation
Lateral C.S. Xray:
- Accuracy 70-80%
- check alignement, bone and disc
Radiological evaluation
Lateral C.S. Xray:
- Accuracy 70-80%
- check alignement, bone and disc
Слайд 6Radiological evaluation
Dorsal spine Xray:
Not accurate
Lumbar Spine Xray:
70% accuracy
Radiological evaluation
Dorsal spine Xray:
Not accurate
Lumbar Spine Xray:
70% accuracy
Слайд 7Radiological evaluation
CT scan and
MRI in case of
clinical suspicion
or abnormal
Radiological evaluation
CT scan and
MRI in case of
clinical suspicion
or abnormal
Слайд 8Spinal Injuries
Spinal Column Injuries
Injuries to Neural Structures (spinal cord, nerve
Spinal Injuries
Spinal Column Injuries
Injuries to Neural Structures (spinal cord, nerve
Слайд 9 Neural injury
secondary injury
• local swelling at the site of injury which
Neural injury
secondary injury
• local swelling at the site of injury which
Слайд 10General Management Guidelines
Role of steroids
The North American Spinal Cord Injury Study (NASCIS)
General Management Guidelines
Role of steroids
The North American Spinal Cord Injury Study (NASCIS)
Слайд 11Spinal Shock
Transient loss of all neurological function (motor, sensory, and autonomic) below
Spinal Shock
Transient loss of all neurological function (motor, sensory, and autonomic) below
Слайд 12Spinal Injuries
Injury level
Spinal Injuries
Injury level
Слайд 13Spinal Injuries
ASIA IMPAIRMENT SCALE:
A =Complete: No motor or sensory function is preserved
Spinal Injuries
ASIA IMPAIRMENT SCALE:
A =Complete: No motor or sensory function is preserved
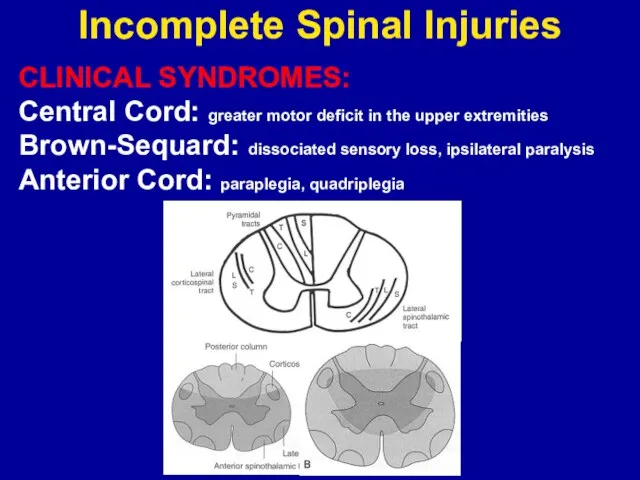
Слайд 14Incomplete Spinal Injuries
CLINICAL SYNDROMES:
Central Cord: greater motor deficit in the upper extremities
Brown-Sequard:
Incomplete Spinal Injuries
CLINICAL SYNDROMES:
Central Cord: greater motor deficit in the upper extremities
Brown-Sequard:
Слайд 15Incomplete Spinal Injuries
CLINICAL SYNDROMES:
Conus Medullaris: saddle anesthesia, incontinence (painless, symmetrical)
Cauda Equina: saddle
Incomplete Spinal Injuries
CLINICAL SYNDROMES:
Conus Medullaris: saddle anesthesia, incontinence (painless, symmetrical)
Cauda Equina: saddle
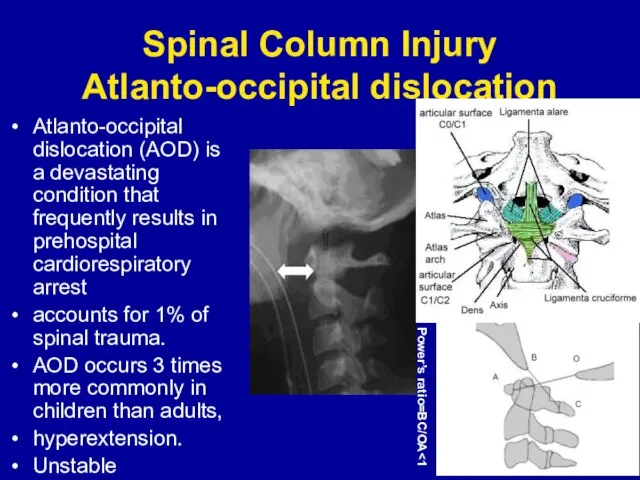
Слайд 16Spinal Column Injury
Atlanto-occipital dislocation
Atlanto-occipital dislocation (AOD) is a devastating condition that frequently
Spinal Column Injury
Atlanto-occipital dislocation
Atlanto-occipital dislocation (AOD) is a devastating condition that frequently
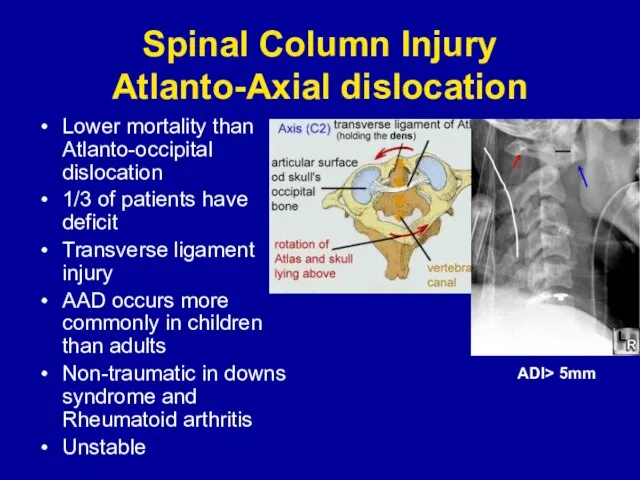
Слайд 17Spinal Column Injury
Atlanto-Axial dislocation
Lower mortality than Atlanto-occipital dislocation
1/3 of patients have deficit
Transverse
Spinal Column Injury
Atlanto-Axial dislocation
Lower mortality than Atlanto-occipital dislocation
1/3 of patients have deficit
Transverse
Слайд 18Spinal Column Injury
Atlas (C1) fractures
Described as Jefferson #
Axial load
Usually no neurological
Spinal Column Injury
Atlas (C1) fractures
Described as Jefferson #
Axial load
Usually no neurological
Слайд 19Spinal Column Injury
Axis (C2) #
Includes Hangman’s # and Odontoid process #
HANGMAN’S #
Bilateral
Spinal Column Injury
Axis (C2) #
Includes Hangman’s # and Odontoid process #
HANGMAN’S #
Bilateral
Слайд 20Spinal Column Injury
Axis (C2) #
Includes Hangman’s # and Odontoid process #
Odontoid #
Flexion
Spinal Column Injury
Axis (C2) #
Includes Hangman’s # and Odontoid process #
Odontoid #
Flexion
Слайд 21Spinal Column Injury
Subaxial (C3-C7) #
Whiplash injury:
Traumatic injury to the soft tissue in
Spinal Column Injury
Subaxial (C3-C7) #
Whiplash injury:
Traumatic injury to the soft tissue in
Слайд 22Spinal Column Injury
Subaxial (C3-C7) #
Vertical compression injury:
Loss of normal cervical lordosis
Burst #
Compression
Spinal Column Injury
Subaxial (C3-C7) #
Vertical compression injury:
Loss of normal cervical lordosis
Burst #
Compression
Слайд 23Spinal Column Injury
Subaxial (C3-C7) #
Compression flexion injury (teardrop #)
Classical diving injury
Posterior elements
Spinal Column Injury
Subaxial (C3-C7) #
Compression flexion injury (teardrop #)
Classical diving injury
Posterior elements
Слайд 24Spinal Column Injury
Subaxial (C3-C7) #
flexion distraction injury (locked facet)
>50% displacement
Unstable
Requires reduction and
Spinal Column Injury
Subaxial (C3-C7) #
flexion distraction injury (locked facet)
>50% displacement
Unstable
Requires reduction and
Слайд 25Spinal Column Injury
Subaxial (C3-C7) #
extention injury (# posterior elements)
# lamina, pedicles or
Spinal Column Injury
Subaxial (C3-C7) #
extention injury (# posterior elements)
# lamina, pedicles or
Слайд 26Spinal Column Injury
Thoracic and lumbar #
Stability (three column model of Denis)
Injury affecting
Spinal Column Injury
Thoracic and lumbar #
Stability (three column model of Denis)
Injury affecting
Слайд 27Spinal Column Injury
Thoracic and lumbar #
Compression #
Burst #
Chance # (seat belt)
Flexion distraction
Fracture
Spinal Column Injury
Thoracic and lumbar #
Compression #
Burst #
Chance # (seat belt)
Flexion distraction
Fracture
Слайд 28General Management Guidelines
Strict spine precautions (immobilization)
Emergency resuscitation (ABC..)
Comprehensive approach
Neurological and Radiological assesment.
Always
General Management Guidelines
Strict spine precautions (immobilization)
Emergency resuscitation (ABC..)
Comprehensive approach
Neurological and Radiological assesment.
Always
 Росиия родина моя
Росиия родина моя я быстро доделала
я быстро доделала London
London Абстрактные структуры данных
Абстрактные структуры данных My splendid friend
My splendid friend  ОРГАНИЗАЦИЯ ШКОЛЬНОГО ПИТАНИЯ
ОРГАНИЗАЦИЯ ШКОЛЬНОГО ПИТАНИЯ Презентация на тему Толстой "Филипок" 2 класс
Презентация на тему Толстой "Филипок" 2 класс Критерии и структура вида
Критерии и структура вида Pronominit. Ja miten viitata niitä käyttäen
Pronominit. Ja miten viitata niitä käyttäen SMC/BMC
SMC/BMC ВИЧ и СПИД
ВИЧ и СПИД Инвестиционный проект
Инвестиционный проект Российская империя в начале XX века. История России
Российская империя в начале XX века. История России Личный финансовый план
Личный финансовый план Премиум тариф курса: Покупки на ТаоВао и 1688. Доставка. Выбор транспортной компании
Премиум тариф курса: Покупки на ТаоВао и 1688. Доставка. Выбор транспортной компании тест игри
тест игри Создание каталога образовательных ресурсов школы Сколково
Создание каталога образовательных ресурсов школы Сколково Основы федерального и регионального законодательства по семейному устройству детей-сирот и детей, оставшихся без попечения родит
Основы федерального и регионального законодательства по семейному устройству детей-сирот и детей, оставшихся без попечения родит Игра, как метод подачи информации
Игра, как метод подачи информации Easter
Easter Твердые тела космического происхождения
Твердые тела космического происхождения Коллективные моды магнитного резонанса в спин-щелевых магнетиках
Коллективные моды магнитного резонанса в спин-щелевых магнетиках Население
Население Trend Micro: преимущества партнерства
Trend Micro: преимущества партнерства Плиточник. Подготовка плиток к облицовке
Плиточник. Подготовка плиток к облицовке А.Пушкин «Борис Годунов» (8 класс)
А.Пушкин «Борис Годунов» (8 класс) Михаил Евграфович Салтыков-Щедрин (1826 - 1889)
Михаил Евграфович Салтыков-Щедрин (1826 - 1889) Центр развития молодых аграриев. Направления работы
Центр развития молодых аграриев. Направления работы