- PATH.ANATOMY PPT

Содержание
- 2. Definition Cirrhosis, which can be the final stage of any chronic liver disease, is a diffuse
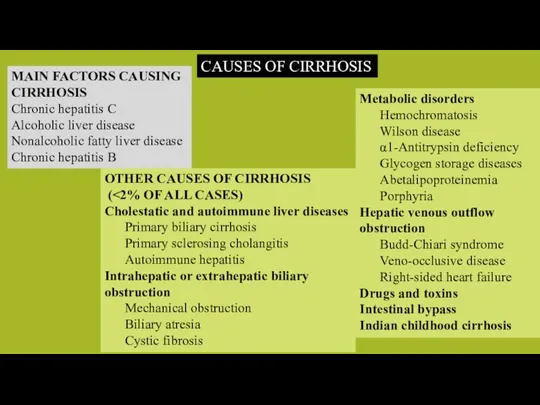
- 3. MAIN FACTORS CAUSING CIRRHOSIS Chronic hepatitis C Alcoholic liver disease Nonalcoholic fatty liver disease Chronic hepatitis
- 4. PATHOBIOLOGY & PATHOGENESIS Liver Fibrosis and Cirrhosis
- 5. 1. The key pathogenic feature underlying liver fibrosis and cirrhosis is activation of hepatic stellate cells.
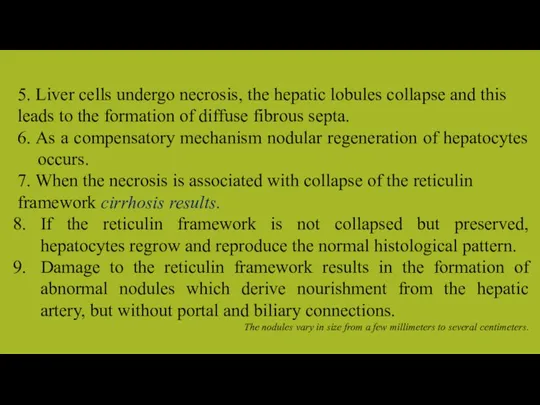
- 6. 5. Liver cells undergo necrosis, the hepatic lobules collapse and this leads to the formation of
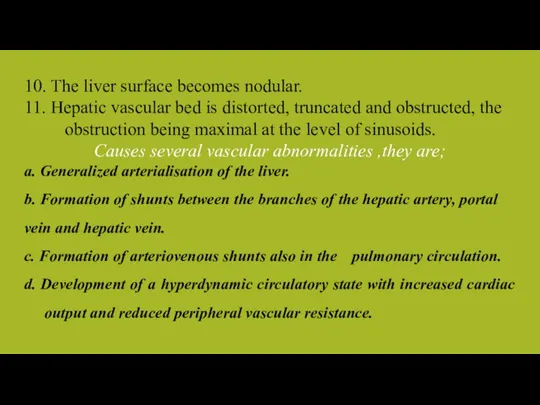
- 7. 10. The liver surface becomes nodular. 11. Hepatic vascular bed is distorted, truncated and obstructed, the
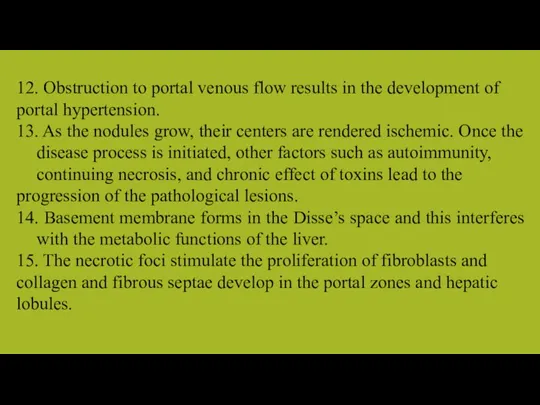
- 8. 12. Obstruction to portal venous flow results in the development of portal hypertension. 13. As the
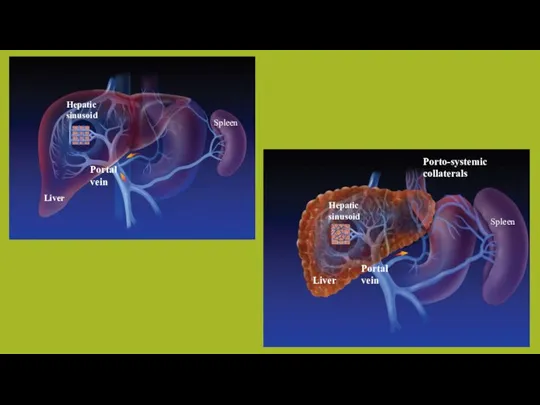
- 9. Hepatic sinusoid Hepatic sinusoid Spleen Spleen Liver Liver Portal vein Portal vein Porto-systemic collaterals
- 10. Morphological Classification The morphological types are: a. micronodular, b. macronodular, and c. mixed.
- 11. In this stage, cirrhosis is mostly asymptomatic and is diagnosed either during the evaluation of chronic
- 12. At this stage, there are signs of decompensation: ascites, variceal hemorrhage, jaundice, hepatic encephalopathy, or any
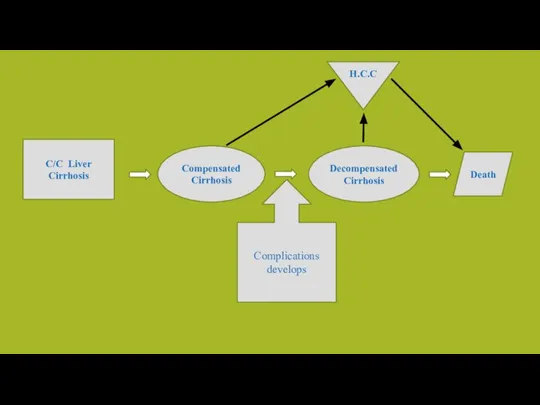
- 13. C/C Liver Cirrhosis Compensated Cirrhosis Decompensated Cirrhosis Death Complications develops H.C.C
- 14. Early stages of the disease are asymptomatic. Vague illhealth, anorexia, loss of weight, loss of libido,
- 15. In the compensated phase, liver synthetic function is mostly normal, and portal pressure, although increased, is
- 16. Variceal Hemorrhage Ascites and Hyponatremia Spontaneous Bacterial Peritonitis Hepatic Encephalopathy Pulmonary Complications Complications
- 18. Скачать презентацию
Слайд 3MAIN FACTORS CAUSING CIRRHOSIS
Chronic hepatitis C
Alcoholic liver disease
Nonalcoholic fatty liver disease
Chronic hepatitis
MAIN FACTORS CAUSING CIRRHOSIS
Chronic hepatitis C
Alcoholic liver disease
Nonalcoholic fatty liver disease
Chronic hepatitis
Слайд 4PATHOBIOLOGY & PATHOGENESIS
Liver Fibrosis and Cirrhosis
PATHOBIOLOGY & PATHOGENESIS
Liver Fibrosis and Cirrhosis
Слайд 51. The key pathogenic feature underlying liver fibrosis and cirrhosis is activation
1. The key pathogenic feature underlying liver fibrosis and cirrhosis is activation
Слайд 65. Liver cells undergo necrosis, the hepatic lobules collapse and this leads
5. Liver cells undergo necrosis, the hepatic lobules collapse and this leads
Слайд 710. The liver surface becomes nodular.
11. Hepatic vascular bed is distorted,
10. The liver surface becomes nodular.
11. Hepatic vascular bed is distorted,
Слайд 812. Obstruction to portal venous flow results in the development of portal
12. Obstruction to portal venous flow results in the development of portal
Слайд 9Hepatic
sinusoid
Hepatic
sinusoid
Spleen
Spleen
Liver
Liver
Portal
vein
Portal
vein
Porto-systemic
collaterals
Hepatic
sinusoid
Hepatic
sinusoid
Spleen
Spleen
Liver
Liver
Portal
vein
Portal
vein
Porto-systemic
collaterals
Слайд 10Morphological Classification
The morphological types are:
a. micronodular,
b. macronodular, and
c. mixed.
Morphological Classification
The morphological types are:
a. micronodular,
b. macronodular, and
c. mixed.
Слайд 11In this stage, cirrhosis is mostly asymptomatic and is diagnosed either during
In this stage, cirrhosis is mostly asymptomatic and is diagnosed either during
Слайд 12At this stage, there are signs of decompensation: ascites, variceal hemorrhage, jaundice,
At this stage, there are signs of decompensation: ascites, variceal hemorrhage, jaundice,
Слайд 13C/C Liver
Cirrhosis
Compensated
Cirrhosis
Decompensated
Cirrhosis
Death
Complications develops
H.C.C
C/C Liver
Cirrhosis
Compensated
Cirrhosis
Decompensated
Cirrhosis
Death
Complications develops
H.C.C
Слайд 14Early stages of the disease are asymptomatic.
Vague illhealth,
anorexia,
loss of
Early stages of the disease are asymptomatic.
Vague illhealth,
anorexia,
loss of
Слайд 15In the compensated phase, liver synthetic function is mostly normal, and portal
In the compensated phase, liver synthetic function is mostly normal, and portal
Слайд 16Variceal Hemorrhage
Ascites and Hyponatremia
Spontaneous Bacterial Peritonitis
Hepatic Encephalopathy
Pulmonary Complications
Complications
Variceal Hemorrhage
Ascites and Hyponatremia
Spontaneous Bacterial Peritonitis
Hepatic Encephalopathy
Pulmonary Complications
Complications
 Жүйке талшықтарының физиологиялық қасиеттері. Парабиоз
Жүйке талшықтарының физиологиялық қасиеттері. Парабиоз Всё ли мы знаем о ГЭРБ
Всё ли мы знаем о ГЭРБ Восточная и западная медицина
Восточная и западная медицина Пиелонефрит. Фитотерапия как компонент комплексной терапии (2)
Пиелонефрит. Фитотерапия как компонент комплексной терапии (2) Послеродовый баллон Бакри
Послеродовый баллон Бакри Гидрогель, способный остановить артериальное кровотечение
Гидрогель, способный остановить артериальное кровотечение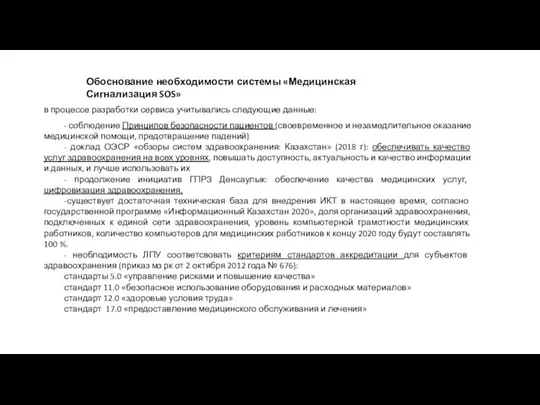 Обоснование необходимости системы Медицинская Сигнализация SOS
Обоснование необходимости системы Медицинская Сигнализация SOS Аяқ - қолдың хирургиялық және туа біткен аурулары
Аяқ - қолдың хирургиялық және туа біткен аурулары Комплексная реабилитация больных и инвалидов
Комплексная реабилитация больных и инвалидов Правила наложения повязок
Правила наложения повязок Акушерские кровотечения
Акушерские кровотечения Туберкулез
Туберкулез Национальный медицинский исследовательский центр профилактической медицины
Национальный медицинский исследовательский центр профилактической медицины Формирование терапевтической школы Российской империи 18-19 веков
Формирование терапевтической школы Российской империи 18-19 веков Электромиография в неврологии. Бионические протезы
Электромиография в неврологии. Бионические протезы Залог здоровья - правильное питание!
Залог здоровья - правильное питание! III Научно-практическая конференция Комплексная реабилитация и ресоциализация потребителей наркотиков: проблемы и перспективы
III Научно-практическая конференция Комплексная реабилитация и ресоциализация потребителей наркотиков: проблемы и перспективы Колоректальная хирургия
Колоректальная хирургия Язва желудка
Язва желудка Синдром Меллори-Вейса
Синдром Меллори-Вейса Аритмии сердца
Аритмии сердца Баротерапия - физиотерапия әдісі
Баротерапия - физиотерапия әдісі Отчет по производственной практике. Социальная работа с семьей и детьми. Поликлиника №114. Детское поликлиническое отделение №75
Отчет по производственной практике. Социальная работа с семьей и детьми. Поликлиника №114. Детское поликлиническое отделение №75 Неотложные состояния в диабетологии
Неотложные состояния в диабетологии Музеи Факультета Ветеринарной медицины и зоотехнии
Музеи Факультета Ветеринарной медицины и зоотехнии Андрогенный дефицит Современный взгляд на проблему возрастного андрогенного дефицита у мужчин
Андрогенный дефицит Современный взгляд на проблему возрастного андрогенного дефицита у мужчин Оценка степени тяжести митральной недостаточности
Оценка степени тяжести митральной недостаточности Основы оперативной хирургической техники, современный инструментарий, нанотехнологии в хирургии
Основы оперативной хирургической техники, современный инструментарий, нанотехнологии в хирургии