- ВРТ / ИКСИ в позднем репродуктивном возрасте

Содержание
- 2. Advanced Maternal Age Definition Chronological : Age above 35yrs Biological Ovarian reserve markers FSH AMH AFC
- 3. Introduction Worldwide tendency to postpone pregnancy until later reproductive life : Building up a career Late
- 4. Oocyte pool decreases from 1-2 millions at birth to 300,000 - 500,000 at puberty to few
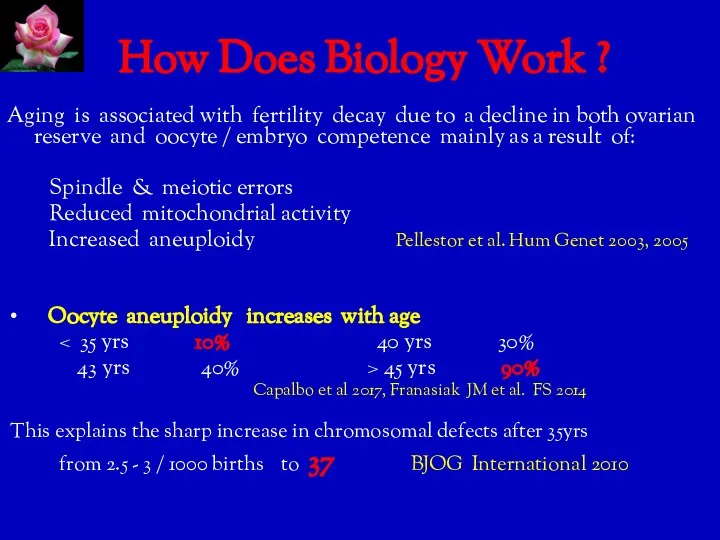
- 5. How Does Biology Work ? Aging is associated with fertility decay due to a decline in
- 6. Infertility Work-up in AMA Recommended after 6 months of seeking pregnancy SOGC 2011 Exclude age related
- 7. Ovarian Reserve Markers Correlate with egg quantity / not quality Predict response to stimulation Poor predictors
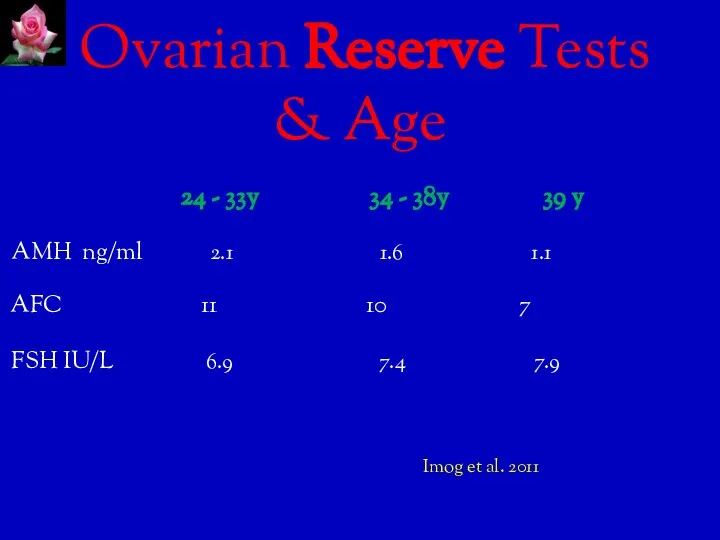
- 8. Ovarian Reserve Tests & Age 24 - 33y 34 - 38y 39 y AMH ng/ml 2.1
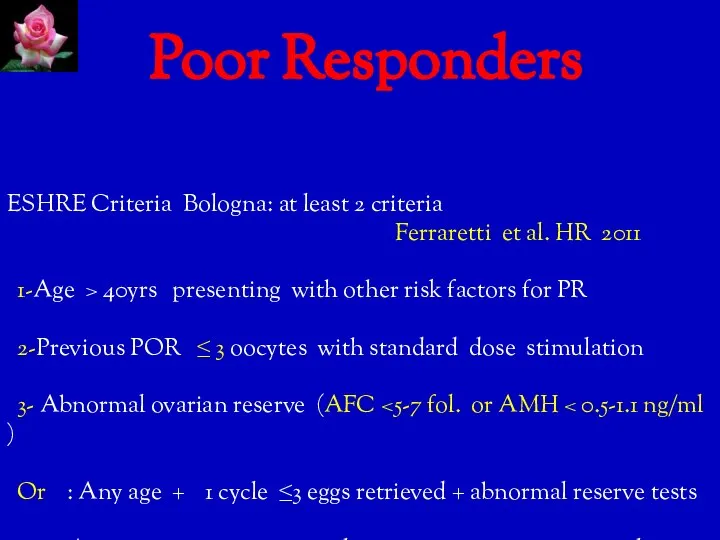
- 9. Poor Responders ESHRE Criteria Bologna: at least 2 criteria Ferraretti et al. HR 2011 1-Age >
- 10. POSEIDON Groups of Poor Response Patient- Oriented Strategies Encompassing IndividualizeD Oocyte Number New measure : Number
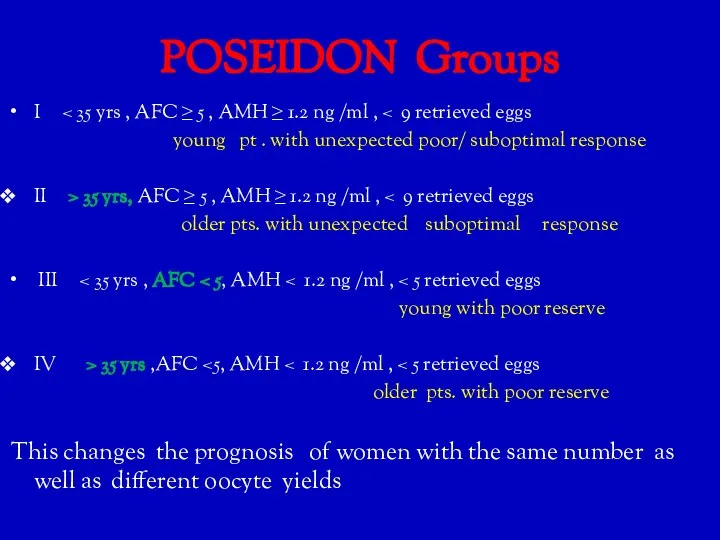
- 11. POSEIDON Groups I young pt . with unexpected poor/ suboptimal response II > 35 yrs, AFC
- 14. Treatment Strategies in Practice Current strategies Maximizing ovarian response Natural or mild stimulation IVF protocol Personalized
- 15. Maximizing Ovarian Response Keep in mind : Gns can not generate follicles ex-novo Max. threshold dose
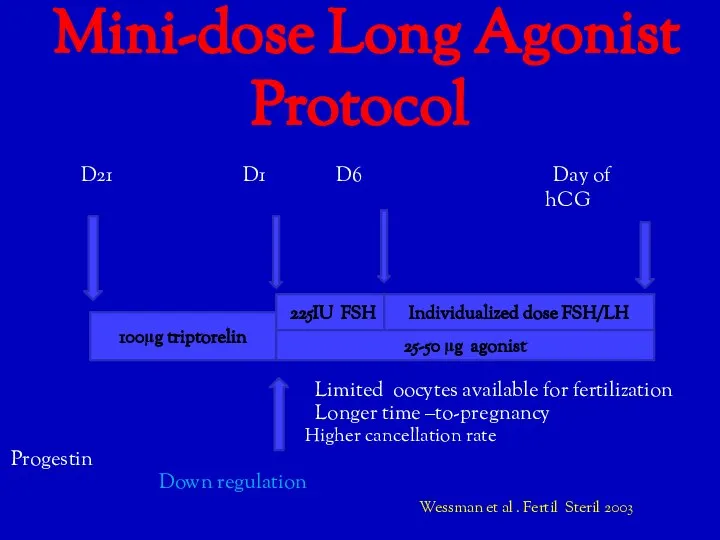
- 16. Mini-dose Long Agonist Protocol D21 D1 D6 Day of hCG Limited oocytes available for fertilization Longer
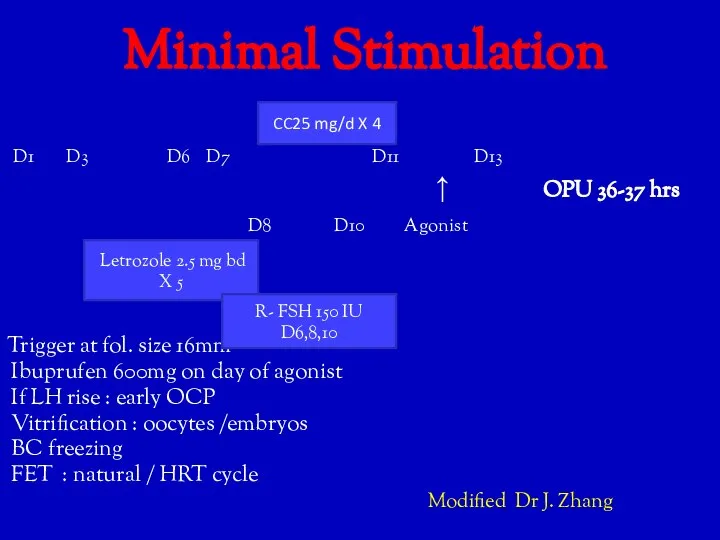
- 17. Minimal Stimulation D1 D3 D6 D7 D11 D13 ↑ OPU 36-37 hrs D8 D10 Agonist Trigger
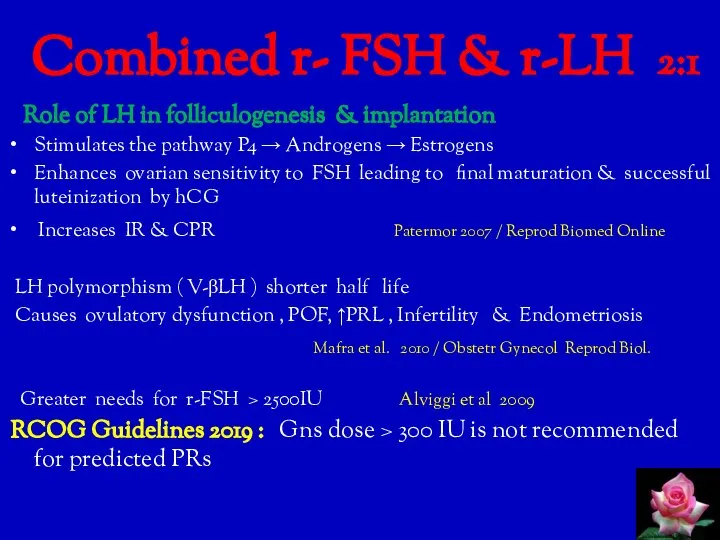
- 18. Combined r- FSH & r-LH 2:1 Role of LH in folliculogenesis & implantation Stimulates the pathway
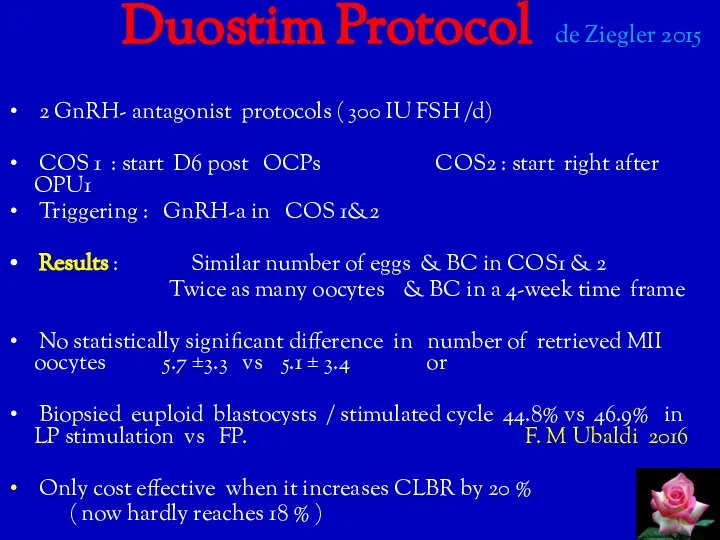
- 21. Duostim Protocol de Ziegler 2015 2 GnRH- antagonist protocols ( 300 IU FSH /d) COS 1
- 22. Double Ovulation Trigger GnRH-a with a reduced or standard dose of hCG 40 hrs and 34hrs
- 23. Natural & Modified Natural Cycle Natural : Less cost & side effects with more natural hormonal
- 24. Freeze - all Policy Rationale : Improves endometrial receptivity ↓ OHSS & MPR ↑ Cumulative PR
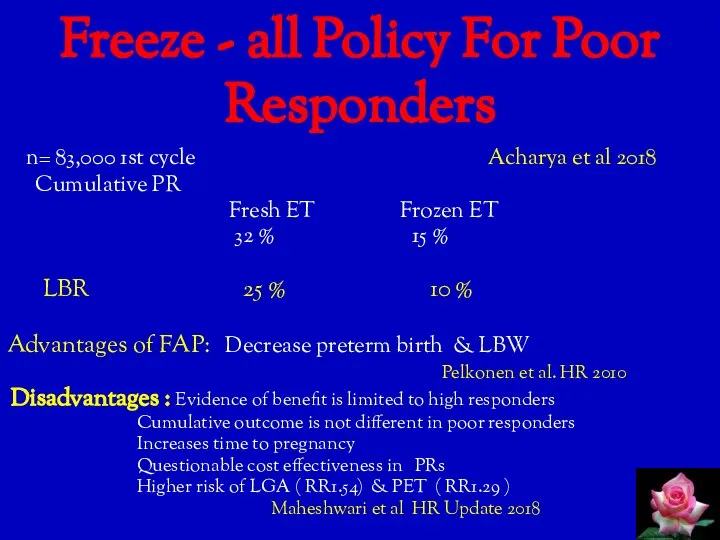
- 25. Freeze - all Policy For Poor Responders n= 83,000 1st cycle Acharya et al 2018 Cumulative
- 26. Oocyte cryopreservation : eggs, ovarian tissue , IVM oocytes Postpone parenthood: Pre-cancer Rx Social issues (
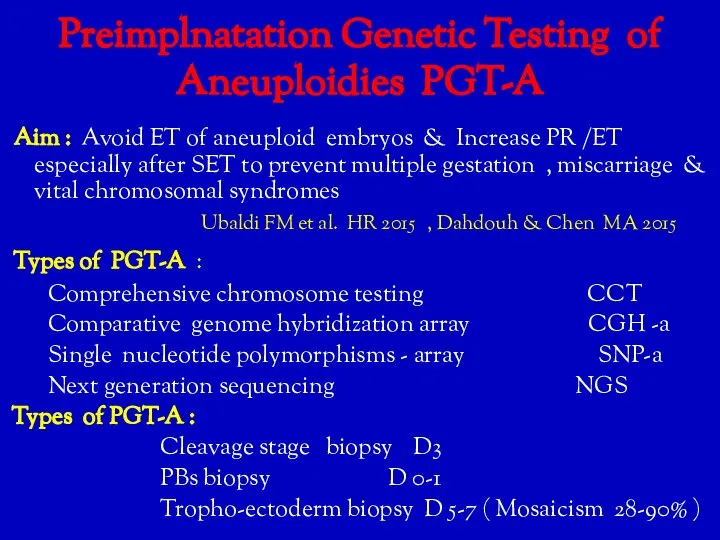
- 27. Preimplnatation Genetic Testing of Aneuploidies PGT-A Aim : Avoid ET of aneuploid embryos & Increase PR
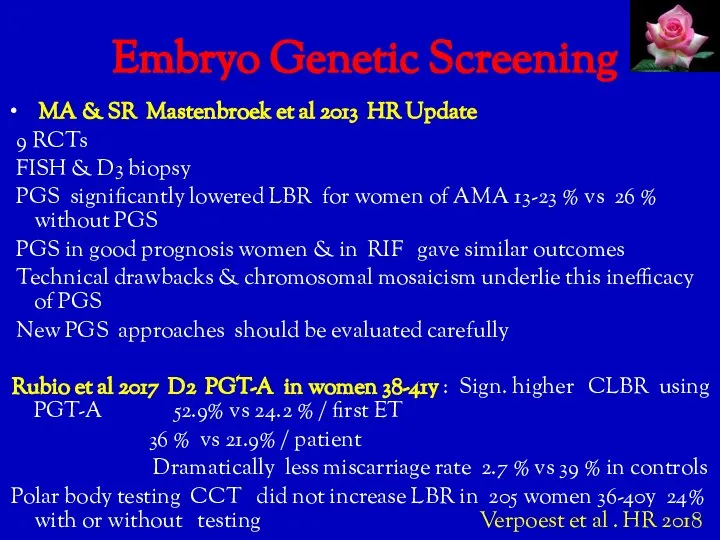
- 28. Embryo Genetic Screening MA & SR Mastenbroek et al 2013 HR Update 9 RCTs FISH &
- 29. Endometrial Scratching Mechanisms : Induce endometrial decidualization Timeya T. et al J. Reprod & Infertility 2014
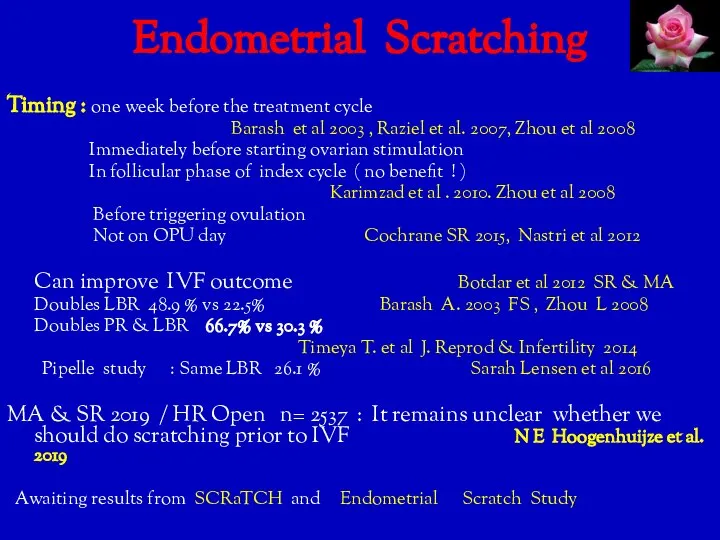
- 30. Endometrial Scratching Timing : one week before the treatment cycle Barash et al 2003 , Raziel
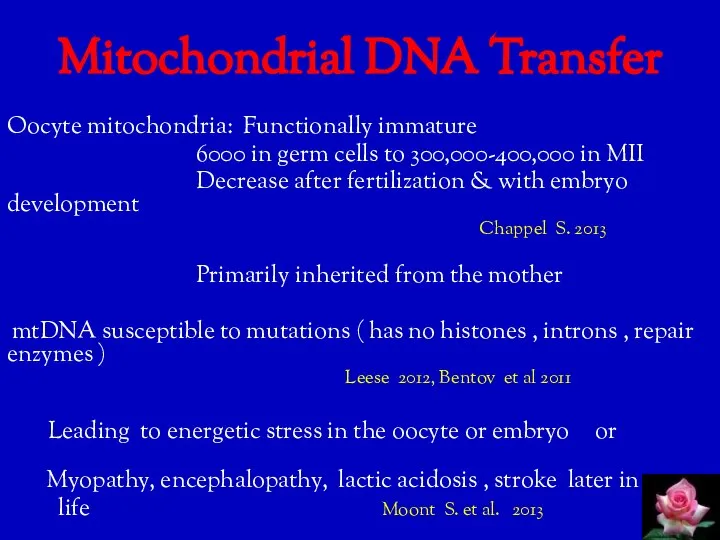
- 31. Mitochondrial DNA Transfer Oocyte mitochondria: Functionally immature 6000 in germ cells to 300,000-400,000 in MII Decrease
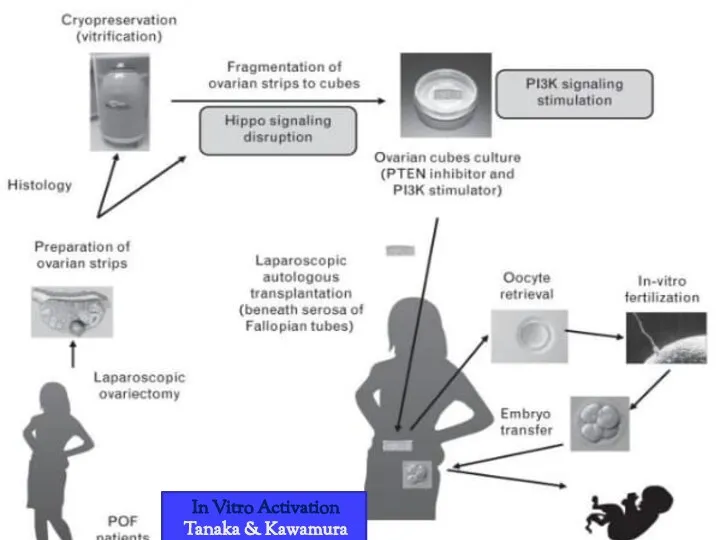
- 32. In Vitro Activation Tanaka & Kawamura 2017
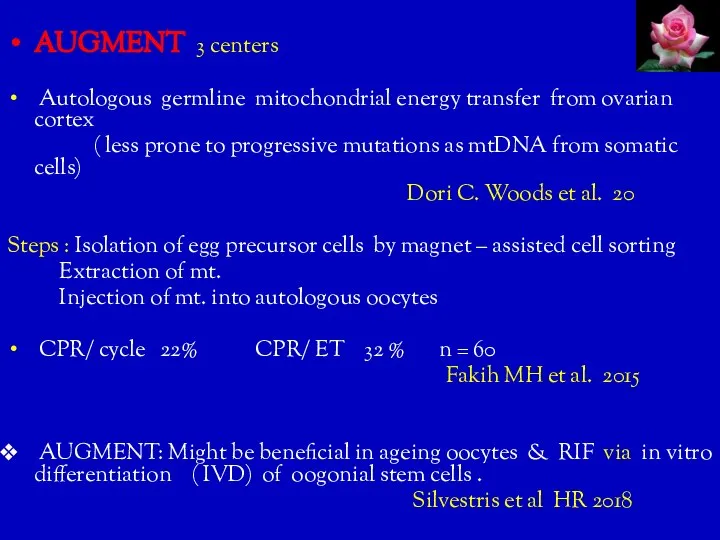
- 33. AUGMENT 3 centers Autologous germline mitochondrial energy transfer from ovarian cortex ( less prone to progressive
- 34. AUGMENT E. Labarta et al 2019 FS : Triple blind RCT in PRs . mean age
- 35. Adjuvant Therapy GH Stimulates FSH receptor expression on granulosa cells Increases intra-ovarian IGF-1 4-18 IU sc
- 36. Adjuvant Therapy Cont... Androgens : DHEA / Testosterone Augment FSH receptor expression Promote GCs development Increase
- 37. Anti -estrogen, Aromatase inhibitors : Better embryo quality, less eggs Baart et al 2007 ↑Endometrial receptivity
- 38. Potential Future Approaches to Treat AMA Inferility Minimally / non-invasive embryo biopsy : investigate leftover IVF
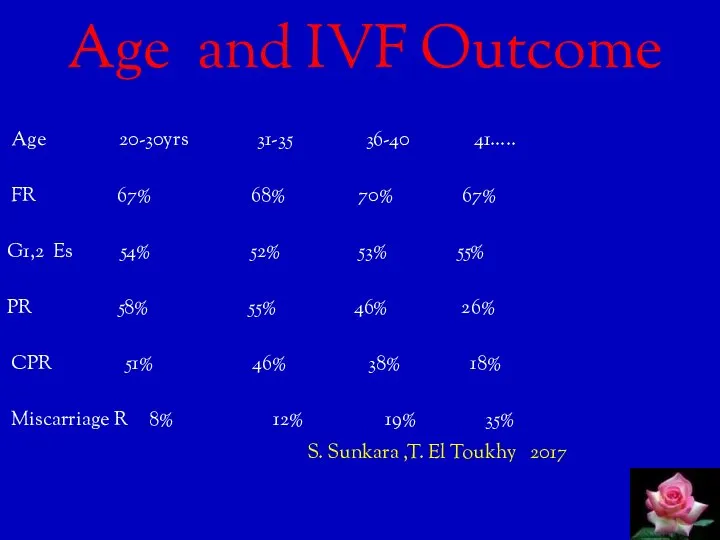
- 39. Age and IVF Outcome Age 20-30yrs 31-35 36-40 41….. FR 67% 68% 70% 67% G1,2 Es
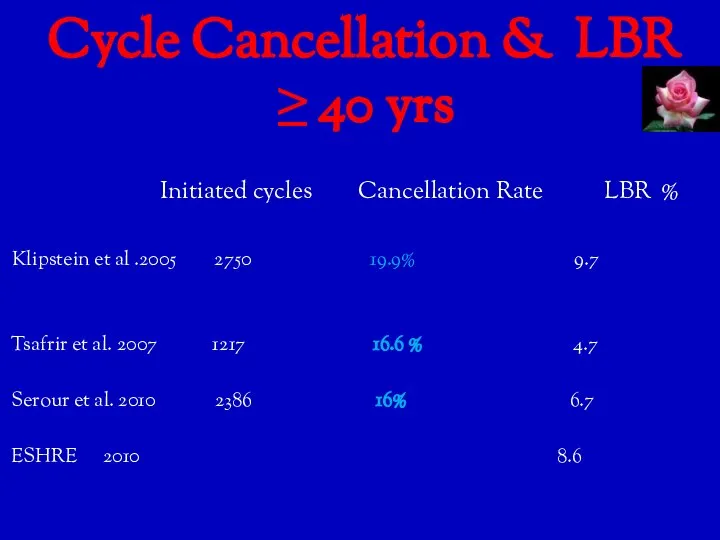
- 40. Cycle Cancellation & LBR ≥ 40 yrs Initiated cycles Cancellation Rate LBR % Klipstein et al
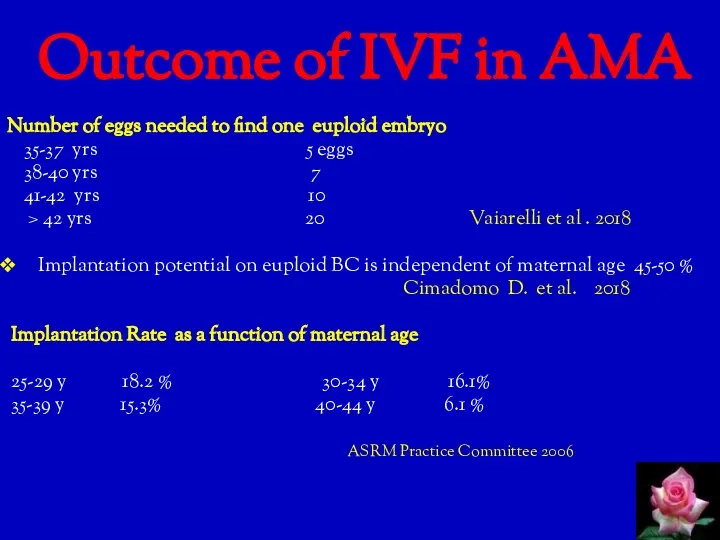
- 41. Outcome of IVF in AMA Number of eggs needed to find one euploid embryo 35-37 yrs
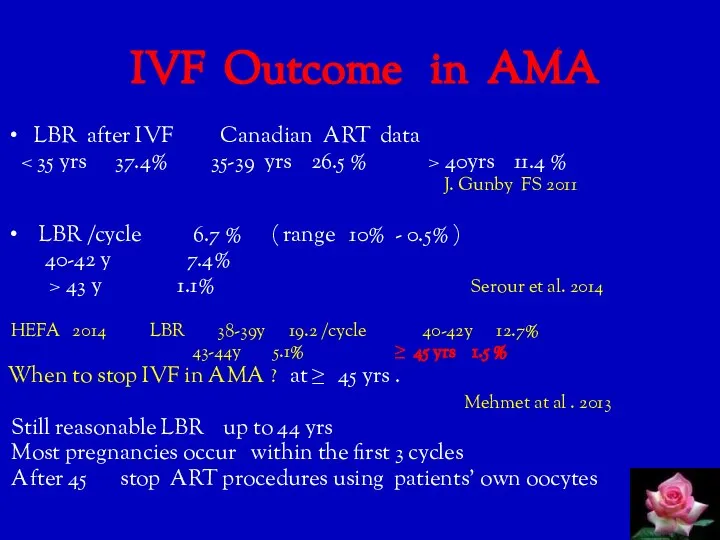
- 42. IVF Outcome in AMA LBR after IVF Canadian ART data 40yrs 11.4 % J. Gunby FS
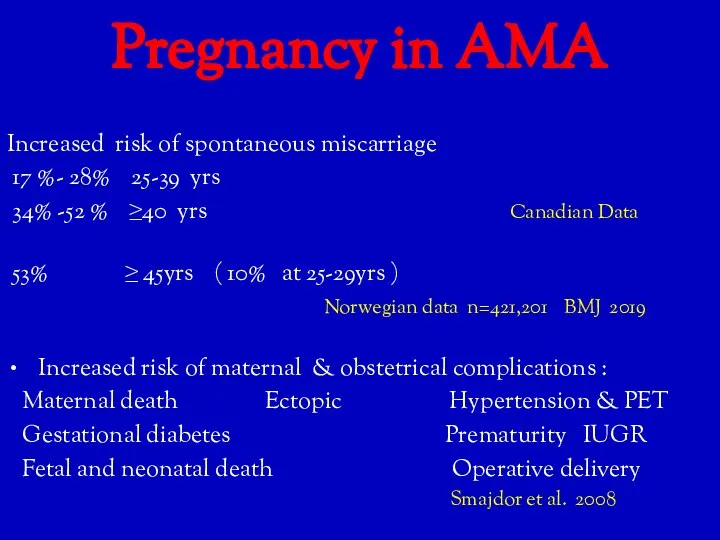
- 43. Pregnancy in AMA Increased risk of spontaneous miscarriage 17 %- 28% 25-39 yrs 34% -52 %
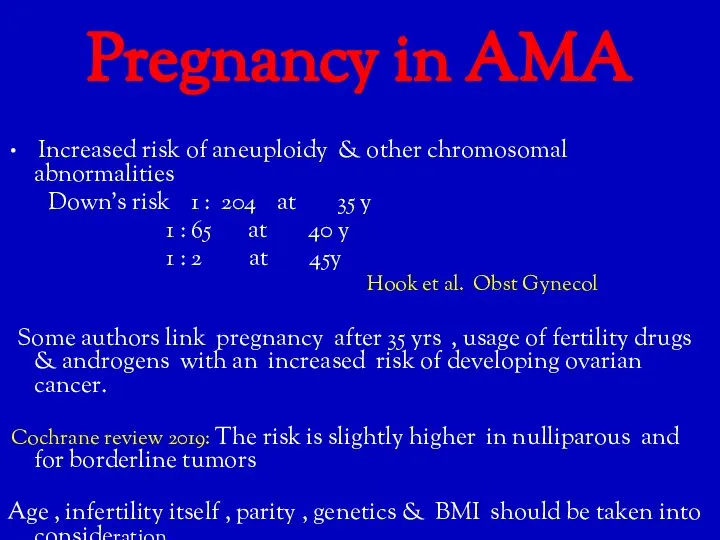
- 44. Pregnancy in AMA Increased risk of aneuploidy & other chromosomal abnormalities Down’s risk 1 : 204
- 45. So ,What is the Magic Formula ? None Fertility preservation ( oocyte / ovarian tissue freezing)
- 46. Conclusions ATR outcome is adversely affected by AMA Launching social campaigns & educating young generations are
- 47. Have you Guessed What FONA stands for ? Friend of Natalia Artymuk If you have a
- 48. THANK YOU For Listening
- 50. Скачать презентацию
Слайд 3 Introduction
Worldwide tendency to postpone pregnancy until later reproductive life
Introduction
Worldwide tendency to postpone pregnancy until later reproductive life
Слайд 4
Oocyte pool decreases from 1-2 millions at birth to
300,000 -
Oocyte pool decreases from 1-2 millions at birth to
300,000 -
Слайд 5 How Does Biology Work ?
Aging is associated with fertility decay due
How Does Biology Work ?
Aging is associated with fertility decay due
Слайд 6 Infertility Work-up in AMA
Recommended after 6 months of seeking pregnancy
Infertility Work-up in AMA
Recommended after 6 months of seeking pregnancy
Слайд 7 Ovarian Reserve Markers
Correlate with egg quantity / not quality
Predict
Ovarian Reserve Markers
Correlate with egg quantity / not quality
Predict
Слайд 8 Ovarian Reserve Tests
& Age
24 - 33y 34 -
Ovarian Reserve Tests
& Age
24 - 33y 34 -
Слайд 9 Poor Responders
ESHRE Criteria Bologna: at least 2 criteria
Poor Responders
ESHRE Criteria Bologna: at least 2 criteria
Слайд 10 POSEIDON Groups of Poor Response
Patient- Oriented Strategies Encompassing IndividualizeD Oocyte Number
POSEIDON Groups of Poor Response
Patient- Oriented Strategies Encompassing IndividualizeD Oocyte Number
Слайд 11POSEIDON Groups
I < 35 yrs , AFC ≥ 5 , AMH ≥
POSEIDON Groups
I < 35 yrs , AFC ≥ 5 , AMH ≥
Слайд 14Treatment Strategies in Practice
Current strategies
Maximizing ovarian response
Natural
Treatment Strategies in Practice
Current strategies
Maximizing ovarian response
Natural
Слайд 15 Maximizing Ovarian Response
Keep in mind :
Gns can not generate
Maximizing Ovarian Response
Keep in mind :
Gns can not generate
Слайд 16 Mini-dose Long Agonist Protocol
D21 D1 D6 Day of
hCG
Mini-dose Long Agonist Protocol
D21 D1 D6 Day of
hCG
Слайд 17 Minimal Stimulation
D1 D3 D6 D7 D11 D13
↑ OPU
Minimal Stimulation
D1 D3 D6 D7 D11 D13
↑ OPU
Слайд 18Combined r- FSH & r-LH 2:1
Role of LH in folliculogenesis &
Combined r- FSH & r-LH 2:1
Role of LH in folliculogenesis &
Слайд 21 Duostim Protocol de Ziegler 2015
2 GnRH- antagonist protocols (
Duostim Protocol de Ziegler 2015
2 GnRH- antagonist protocols (
Слайд 22 Double Ovulation Trigger
GnRH-a with a reduced or standard dose of hCG
Double Ovulation Trigger
GnRH-a with a reduced or standard dose of hCG
Слайд 23 Natural & Modified Natural Cycle
Natural : Less cost
Natural & Modified Natural Cycle
Natural : Less cost
Слайд 24 Freeze - all Policy
Rationale : Improves endometrial receptivity
↓
Freeze - all Policy
Rationale : Improves endometrial receptivity
↓
Слайд 25Freeze - all Policy For Poor Responders
n= 83,000 1st cycle
Freeze - all Policy For Poor Responders
n= 83,000 1st cycle
Слайд 26Oocyte cryopreservation : eggs, ovarian tissue , IVM oocytes
Postpone parenthood:
Postpone parenthood:
Слайд 27Preimplnatation Genetic Testing of Aneuploidies PGT-A
Aim : Avoid ET of aneuploid
Preimplnatation Genetic Testing of Aneuploidies PGT-A
Aim : Avoid ET of aneuploid
Слайд 28 Embryo Genetic Screening
MA & SR Mastenbroek et al 2013
Embryo Genetic Screening
MA & SR Mastenbroek et al 2013
Слайд 29Endometrial Scratching
Mechanisms :
Induce endometrial decidualization Timeya T. et al J.
Endometrial Scratching
Mechanisms :
Induce endometrial decidualization Timeya T. et al J.
Слайд 30Endometrial Scratching
Timing : one week before the treatment cycle
Barash et
Endometrial Scratching
Timing : one week before the treatment cycle
Barash et
Слайд 31
Mitochondrial DNA Transfer
Oocyte mitochondria: Functionally immature
6000 in germ cells
Mitochondrial DNA Transfer
Oocyte mitochondria: Functionally immature
6000 in germ cells
Слайд 32 In Vitro Activation
Tanaka & Kawamura 2017
In Vitro Activation
Tanaka & Kawamura 2017
Слайд 33AUGMENT 3 centers
Autologous germline mitochondrial energy transfer from ovarian cortex
Autologous germline mitochondrial energy transfer from ovarian cortex
Слайд 34 AUGMENT
E. Labarta et al 2019 FS : Triple blind
AUGMENT
E. Labarta et al 2019 FS : Triple blind
Слайд 35 Adjuvant Therapy
GH Stimulates FSH receptor expression on granulosa cells
Adjuvant Therapy
GH Stimulates FSH receptor expression on granulosa cells
Слайд 36Adjuvant Therapy Cont...
Androgens : DHEA / Testosterone
Augment FSH receptor
Adjuvant Therapy Cont...
Androgens : DHEA / Testosterone
Augment FSH receptor
Слайд 37Anti -estrogen, Aromatase inhibitors :
Better embryo quality, less eggs Baart et
Better embryo quality, less eggs Baart et
Слайд 38 Potential Future Approaches to Treat AMA Inferility
Minimally / non-invasive
Potential Future Approaches to Treat AMA Inferility
Minimally / non-invasive
Слайд 39 Age and IVF Outcome
Age 20-30yrs 31-35 36-40 41…..
FR
Age and IVF Outcome
Age 20-30yrs 31-35 36-40 41…..
FR
Слайд 40 Cycle Cancellation & LBR ≥ 40 yrs
Initiated cycles
Cycle Cancellation & LBR ≥ 40 yrs
Initiated cycles
Слайд 41 Outcome of IVF in AMA
Number of eggs needed to find
Outcome of IVF in AMA
Number of eggs needed to find
Слайд 42 IVF Outcome in AMA
LBR after IVF Canadian ART data
IVF Outcome in AMA
LBR after IVF Canadian ART data
Слайд 43Pregnancy in AMA
Increased risk of spontaneous miscarriage
17 %- 28% 25-39
Pregnancy in AMA
Increased risk of spontaneous miscarriage
17 %- 28% 25-39
Слайд 44Pregnancy in AMA
Increased risk of aneuploidy & other chromosomal abnormalities
Pregnancy in AMA
Increased risk of aneuploidy & other chromosomal abnormalities
Слайд 45So ,What is the Magic Formula ?
None
Fertility preservation (
So ,What is the Magic Formula ?
None
Fertility preservation (
Слайд 46 Conclusions
ATR outcome is adversely affected by AMA
Launching social
Conclusions
ATR outcome is adversely affected by AMA
Launching social
Слайд 47 Have you Guessed
What FONA stands for ?
Friend of
Have you Guessed
What FONA stands for ?
Friend of
Слайд 48 THANK YOU
For
Listening
THANK YOU
For
Listening

 Виды медицинского страхования
Виды медицинского страхования Пуринергиялық синапстарда қозудың берілуіне әсер ететін дәрілер
Пуринергиялық синапстарда қозудың берілуіне әсер ететін дәрілер Вечерние беседы о прекрасном. ЗППП, часть1
Вечерние беседы о прекрасном. ЗППП, часть1 Patogennye_mikobakterii_korinebakterii_i_bordetelly
Patogennye_mikobakterii_korinebakterii_i_bordetelly Осложнение инъекций
Осложнение инъекций Альтернативное питание
Альтернативное питание Мембранозная нефропатия
Мембранозная нефропатия Патофизиология наследственных заболеваний. Основы медицинской генетики
Патофизиология наследственных заболеваний. Основы медицинской генетики Гемотрансфузия
Гемотрансфузия Осложнения острого аппендицита
Осложнения острого аппендицита НЕфрология
НЕфрология Правила наложения повязок
Правила наложения повязок Ядерные и радиационные технологии на службе здоровья человека. Перспективы развития в УрФО
Ядерные и радиационные технологии на службе здоровья человека. Перспективы развития в УрФО Методы исследования в гигиенической практике. Санитария. Структура Роспотребнадзора
Методы исследования в гигиенической практике. Санитария. Структура Роспотребнадзора Первая степень атрио-вентрикулярной блокады
Первая степень атрио-вентрикулярной блокады Шизофрения — эндогенное психическое заболевание
Шизофрения — эндогенное психическое заболевание Лимфопоэз и иммуногенез. Органы иммунной защиты
Лимфопоэз и иммуногенез. Органы иммунной защиты Заключение по гипертонической болезни Обмен Са и его нарушения Нейродегенеративные заболевания (Лекция 6)
Заключение по гипертонической болезни Обмен Са и его нарушения Нейродегенеративные заболевания (Лекция 6) Роль медицинской сестры в организации работы с пациентами, входящими в группу риска по развитию варикозного расширения вен
Роль медицинской сестры в организации работы с пациентами, входящими в группу риска по развитию варикозного расширения вен Виды инъекций
Виды инъекций Психопатология как следствие или часть инфекционного процесса
Психопатология как следствие или часть инфекционного процесса Послеоперационные грыжи
Послеоперационные грыжи Заболевание, вызванное нарушением питания: панкреатит
Заболевание, вызванное нарушением питания: панкреатит История развития психопатологии в России
История развития психопатологии в России Желчно-каменная болезнь
Желчно-каменная болезнь Оказание первой помощи при наружном кровотечении
Оказание первой помощи при наружном кровотечении Миома (маточный фиброид). Этиология, патогенез, клиника, диагностика, лечение
Миома (маточный фиброид). Этиология, патогенез, клиника, диагностика, лечение ЛП в педиатрии
ЛП в педиатрии