- Diseases of gallbladder

Содержание
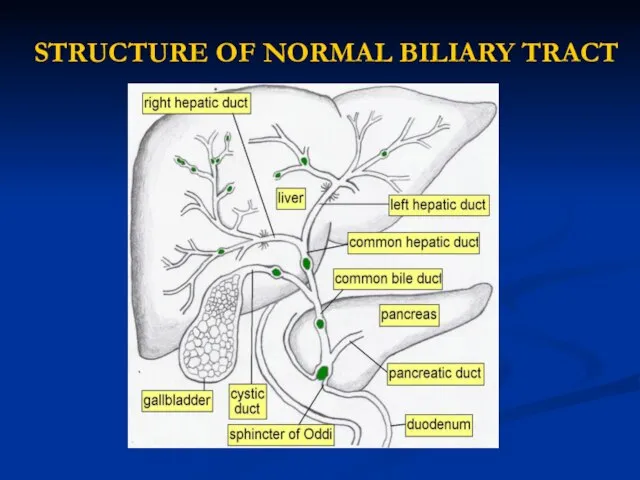
- 2. STRUCTURE OF NORMAL BILIARY TRACT
- 3. LIST OF DISEASES OF THE GALLBLADDER CONGENITAL ANOMALIES GALLSTONES ACUTE CHOLECYSTITIS ACALCULOUS CHOLECYSTITIS EMPHYSEMATOUS CHOLECYSTITIS CHRONIC
- 4. GALLSTONE DISEASE Types of gallstones Cholesterol stones (85%): These are divided into 2 subtypes—pure (90-100% cholesterol)
- 5. Predisposing Factors for Cholesterol Gallstone Formation 1. Demographic/genetic factors. Prevalence highest in North American Indians, Chilean
- 6. Predisposing Factors for Cholesterol Gallstone Formation 5. Increasing age. Increased biliary secretion of cholesterol, decreased size
- 7. Predisposing Factors for Pigment Gallstone Formation 1. Demographic/genetic factors: Asia, rural setting 2. Chronic hemolysis 3.
- 8. STAGES OF STONE FORMATION Cholesterol supersaturation in bile. Cholesterol is held in solution in bile by
- 9. Symptoms of Gallstone Disease Gallstones usually produce symptoms by causing inflammation or obstruction following their migration
- 10. Symptoms of Gallstone Disease Dyspeptic syndrome (Nausea and vomiting) frequently accompany episodes of biliary pain. General
- 11. EXAMINATION Ultrasonography of the gallbladder is very accurate in the identification of cholelithiasis. Stones as small
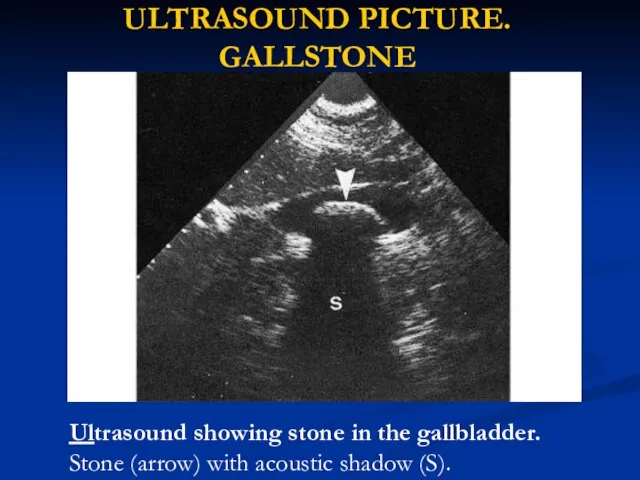
- 12. ULTRASOUND PICTURE. GALLSTONE Ultrasound showing stone in the gallbladder. Stone (arrow) with acoustic shadow (S).
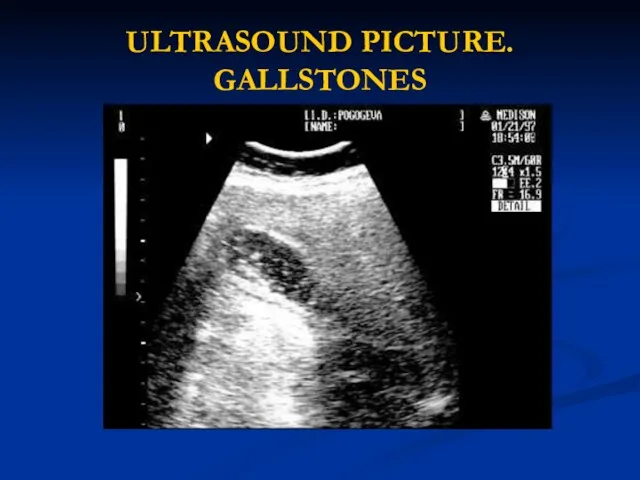
- 13. ULTRASOUND PICTURE. GALLSTONES
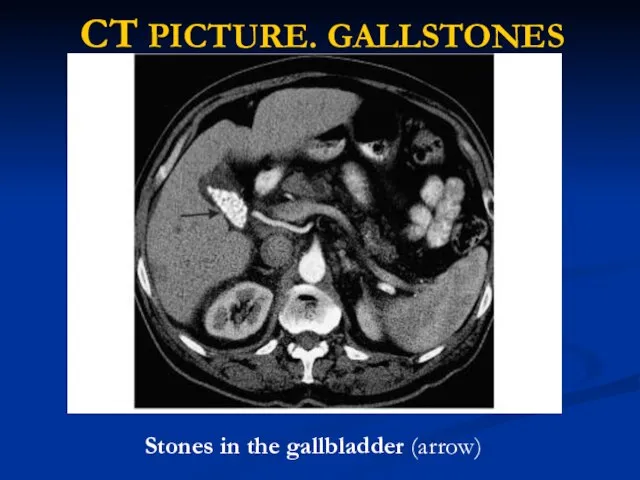
- 14. CT PICTURE. GALLSTONES Stones in the gallbladder (arrow)
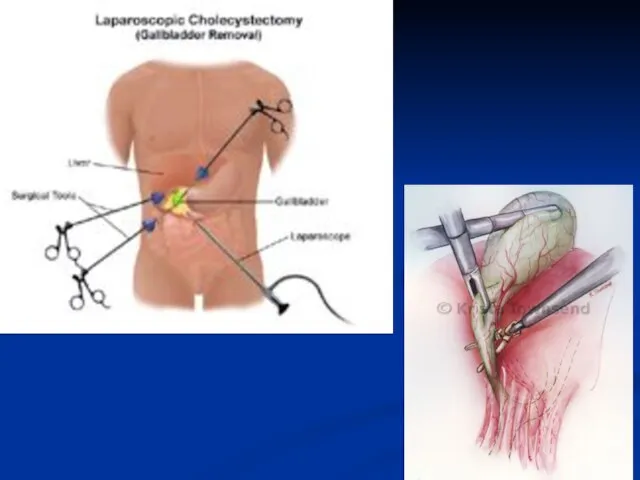
- 15. TREATMENT. Surgical Therapy Laparoscopic cholecystectomy has become the “gold standard” for treating symptomatic cholelithiasis. Recommendations for
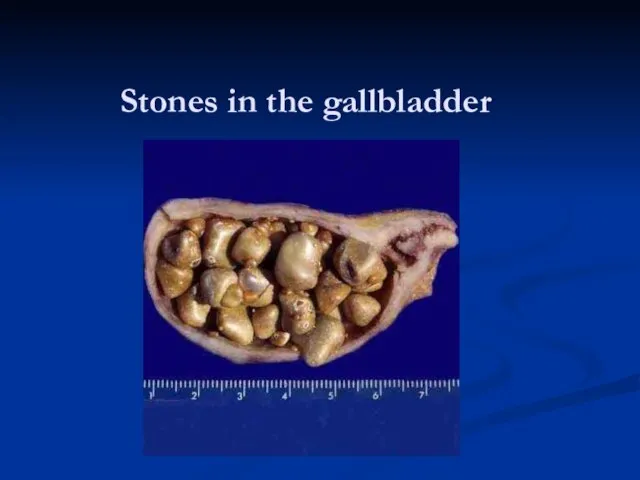
- 17. Stones in the gallbladder
- 18. TREATMENT Medical Therapy—Gallstone Dissolution UDCA (Actigall, URSO 250, URSO, Ursofalk, ursodeoxycholic acid) decreases cholesterol saturation of
- 19. Medical Therapy—Gallstone Dissolution
- 20. ACUTE CHOLECYSTITIS ETHIOLOGY Acute inflammation of the gallbladder wall usually follows obstruction of the cystic duct
- 21. ACUTE CHOLECYSTITIS. SYMPTOMS AND SIGHNS Acute cholecystitis often begins as an attack of biliary pain (abdominal
- 22. ACUTE CHOLECYSTITIS. SYMPTOMS AND SIGHNS Jaundice is unusual early in the course of acute cholecystitis but
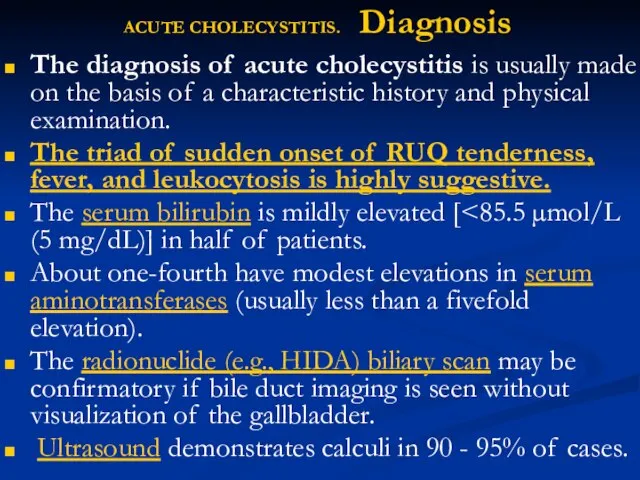
- 23. ACUTE CHOLECYSTITIS. Diagnosis The diagnosis of acute cholecystitis is usually made on the basis of a
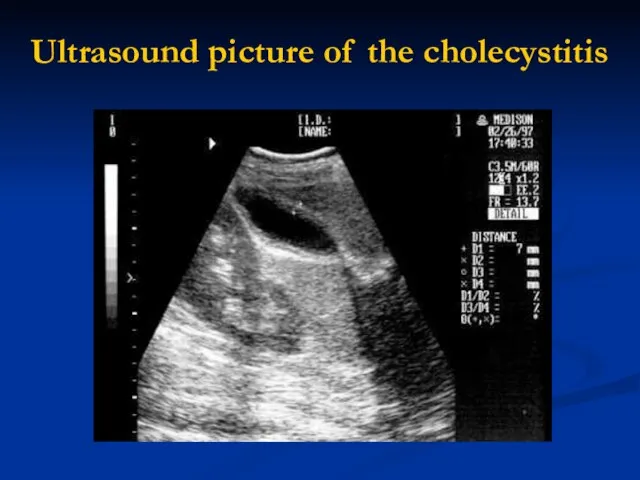
- 24. Ultrasound picture of the cholecystitis
- 25. ACUTE CHOLECYSTITIS. Outcomes. Approximately 75% of patients treated medically have remission of acute symptoms within 2
- 26. ACALCULOUS CHOLECYSTITIS ETHIOLOGY. In 5 to 10% of patients with acute cholecystitis, calculi obstructing the cystic
- 27. ACALCULOUS CHOLECYSTITIS CLINICAL PICTURE. The clinical manifestations of acalculous cholecystitis are the same as calculous cholecystitis,
- 28. CHRONIC CHOLECYSTITIS ETHIOLOGY, CLINICAL PICTURE Chronic inflammation of the gallbladder wall is almost always associated with
- 29. CHRONIC CHOLECYSTITIS. Complications EMPYEMA of the gallbladder usually results from progression of acute cholecystitis with persistent
- 30. CHRONIC CHOLECYSTITIS. Complications HYDROPS or MUCOCELE of the gallbladder may also result from prolonged obstruction of
- 31. CHRONIC CHOLECYSTITIS. Complications GANGRENE of the gallbladder results from ischemia of the wall and patchy or
- 32. CHRONIC CHOLECYSTITIS. MEDICAL TREATMENT Although surgical intervention remains the mainstay of therapy for acute cholecystitis and
- 33. CHRONIC CHOLECYSTITIS. MEDICAL TREATMENT Intravenous antibiotic therapy is usually indicated in patients with severe acute cholecystitis
- 34. CHRONIC CHOLECYSTITIS. SURGICAL TREATMENT The optimal timing of surgical intervention in patients with acute cholecystitis depends
- 35. CHRONIC CHOLECYSTITIS. SURGICAL TREATMENT Delayed surgical intervention is probably best reserved for (1) patients with very
- 36. Postcholecystectomy Complications Early complications following cholecystectomy include atelectasis and other pulmonary disorders, abscess formation (often subphrenic),
- 37. LIST OF DISEASES OF THE BILE DUCTS CONGENITAL ANOMALIES CHOLEDOCHOLITHIASIS CHOLANGITIS PAPILLARY DYSFUNCTION PAPILLARY STENOSIS SPASM
- 38. DISEASES OF THE BILE DUCTS. CONGENITAL ANOMALIES Biliary Atresia and Hypoplasia Atretic and hypoplastic lesions of
- 39. DISEASES OF THE BILE DUCTS. CONGENITAL ANOMALIES Congenital Biliary Ectasia Dilatation of intrahepatic bile ducts may
- 40. DISEASES OF THE BILE DUCTS. CHOLEDOCHOLITHIASIS Passage of gallstones into the CBD occurs in approximately 10
- 41. DISEASES OF THE BILE DUCTS CHOLEDOCHOLITHIASIS Primary calculi arising de novo in the ducts are usually
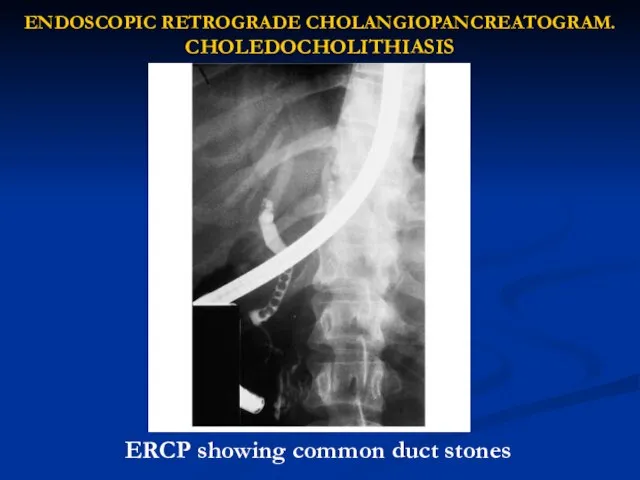
- 42. ENDOSCOPIC RETROGRADE CHOLANGIOPANCREATOGRAM. CHOLEDOCHOLITHIASIS ERCP showing common duct stones
- 43. CHOLEDOCHOLITHIASIS. Complications CHOLANGITIS Cholangitis may be acute or chronic, and symptoms result from inflammation, which usually
- 44. CHOLEDOCHOLITHIASIS. Complications Nonsuppurative acute cholangitis is most common and may respond relatively rapidly to supportive measures
- 45. CHOLEDOCHOLITHIASIS Complications. OBSTRUCTIVE JAUNDICE Gradual obstruction of the CBD over a period of weeks or months
- 46. CHOLEDOCHOLITHIASIS Complications. OBSTRUCTIVE JAUNDICE CBD stones should be suspected in any patient with cholecystitis whose serum
- 47. PAPILLARY DYSFUNCTION, STENOSIS, SPASM OF THE SPHINCTER OF ODDI, BILIARY DYSKINESIA Symptoms of biliary colic accompanied
- 48. PAPILLARY DYSFUNCTION, STENOSIS, SPASM OF THE SPHINCTER OF ODDI, BILIARY DYSKINESIA An alternative to ERCP is
- 49. Proposed mechanisms of Dyskinesia of the sphincter of Oddi include spasm of the sphincter, denervation sensitivity
- 50. Neoplasms of the biliary tract: Carcinoma of the biliary system manifests with clinical symptoms of weight
- 51. SCLEROSING CHOLANGITIS Definition. Primary or idiopathic sclerosing cholangitis is characterized by a progressive, inflammatory, sclerosing, and
- 52. SCLEROSING CHOLANGITIS Secondary sclerosing cholangitis may occur as a long-term complication of choledocholithiasis, cholangiocarcinoma, operative or
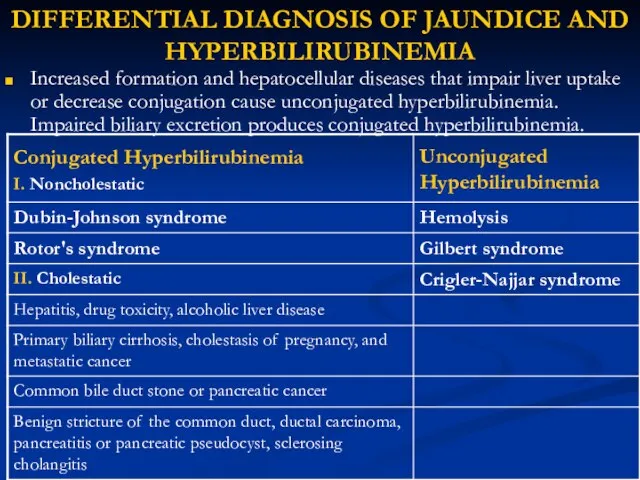
- 53. DIFFERENTIAL DIAGNOSIS OF JAUNDICE AND HYPERBILIRUBINEMIA Increased formation and hepatocellular diseases that impair liver uptake or
- 54. Noncholestatic Conjugated Hyperbilirubinemia Disorders of bilirubin metabolism causing conjugated hyperbilirubinemia without cholestasis produce no symptoms. Bilirubin
- 55. Unconjugated Hyperbilirubinemia Unconjugated hyperbilirubinemia is a disorder of bilirubin metabolism consisting of overproduction or defective conjugation
- 56. Unconjugated Hyperbilirubinemia Crigler-Najjar syndrome: This rare inherited disorder is caused by deficiency of the enzyme glucuronyl
- 58. Скачать презентацию
Слайд 3LIST OF DISEASES OF THE GALLBLADDER
CONGENITAL ANOMALIES
GALLSTONES
ACUTE CHOLECYSTITIS
ACALCULOUS CHOLECYSTITIS
EMPHYSEMATOUS CHOLECYSTITIS
CHRONIC CHOLECYSTITIS
GALLBLADDER CANCER
LIST OF DISEASES OF THE GALLBLADDER
CONGENITAL ANOMALIES
GALLSTONES
ACUTE CHOLECYSTITIS
ACALCULOUS CHOLECYSTITIS
EMPHYSEMATOUS CHOLECYSTITIS
CHRONIC CHOLECYSTITIS
GALLBLADDER CANCER
Слайд 4GALLSTONE DISEASE
Types of gallstones
Cholesterol stones (85%): These are divided into 2
GALLSTONE DISEASE
Types of gallstones
Cholesterol stones (85%): These are divided into 2
Слайд 5Predisposing Factors for Cholesterol Gallstone Formation
1. Demographic/genetic factors. Prevalence highest in North American
Predisposing Factors for Cholesterol Gallstone Formation
1. Demographic/genetic factors. Prevalence highest in North American
Слайд 6Predisposing Factors for Cholesterol Gallstone Formation
5. Increasing age. Increased biliary secretion of cholesterol,
Predisposing Factors for Cholesterol Gallstone Formation
5. Increasing age. Increased biliary secretion of cholesterol,
Слайд 7 Predisposing Factors for Pigment Gallstone Formation
1. Demographic/genetic factors: Asia, rural setting
Predisposing Factors for Pigment Gallstone Formation
1. Demographic/genetic factors: Asia, rural setting
Слайд 8STAGES OF STONE FORMATION
Cholesterol supersaturation in bile. Cholesterol is held in solution
STAGES OF STONE FORMATION
Cholesterol supersaturation in bile. Cholesterol is held in solution
Слайд 9Symptoms of Gallstone Disease
Gallstones usually produce symptoms by causing inflammation or obstruction
Symptoms of Gallstone Disease
Gallstones usually produce symptoms by causing inflammation or obstruction
Слайд 10Symptoms of Gallstone Disease
Dyspeptic syndrome (Nausea and vomiting) frequently accompany episodes of
Symptoms of Gallstone Disease
Dyspeptic syndrome (Nausea and vomiting) frequently accompany episodes of
Слайд 11 EXAMINATION
Ultrasonography of the gallbladder is very accurate in the identification of
EXAMINATION
Ultrasonography of the gallbladder is very accurate in the identification of
Слайд 12ULTRASOUND PICTURE. GALLSTONE
Ultrasound showing stone in the gallbladder. Stone (arrow) with acoustic
ULTRASOUND PICTURE. GALLSTONE
Ultrasound showing stone in the gallbladder. Stone (arrow) with acoustic
Слайд 13ULTRASOUND PICTURE. GALLSTONES
ULTRASOUND PICTURE. GALLSTONES
Слайд 14CT PICTURE. GALLSTONES
Stones in the gallbladder (arrow)
CT PICTURE. GALLSTONES
Stones in the gallbladder (arrow)
Слайд 15TREATMENT. Surgical Therapy
Laparoscopic cholecystectomy has become the “gold standard” for treating symptomatic
TREATMENT. Surgical Therapy
Laparoscopic cholecystectomy has become the “gold standard” for treating symptomatic
Слайд 17Stones in the gallbladder
Stones in the gallbladder
Слайд 18TREATMENT
Medical Therapy—Gallstone Dissolution
UDCA (Actigall, URSO 250, URSO, Ursofalk, ursodeoxycholic acid) decreases cholesterol
TREATMENT
Medical Therapy—Gallstone Dissolution
UDCA (Actigall, URSO 250, URSO, Ursofalk, ursodeoxycholic acid) decreases cholesterol
Слайд 19Medical Therapy—Gallstone Dissolution
Medical Therapy—Gallstone Dissolution

Слайд 20ACUTE CHOLECYSTITIS
ETHIOLOGY
Acute inflammation of the gallbladder wall usually follows obstruction of
ACUTE CHOLECYSTITIS
ETHIOLOGY
Acute inflammation of the gallbladder wall usually follows obstruction of
Слайд 21ACUTE CHOLECYSTITIS. SYMPTOMS AND SIGHNS
Acute cholecystitis often begins as an attack
ACUTE CHOLECYSTITIS. SYMPTOMS AND SIGHNS
Acute cholecystitis often begins as an attack
Слайд 22ACUTE CHOLECYSTITIS. SYMPTOMS AND SIGHNS
Jaundice is unusual early in the course of
ACUTE CHOLECYSTITIS. SYMPTOMS AND SIGHNS
Jaundice is unusual early in the course of
Слайд 23ACUTE CHOLECYSTITIS. Diagnosis
The diagnosis of acute cholecystitis is usually made on the
ACUTE CHOLECYSTITIS. Diagnosis
The diagnosis of acute cholecystitis is usually made on the
Слайд 24Ultrasound picture of the cholecystitis
Ultrasound picture of the cholecystitis
Слайд 25ACUTE CHOLECYSTITIS. Outcomes.
Approximately 75% of patients treated medically have remission of acute
ACUTE CHOLECYSTITIS. Outcomes.
Approximately 75% of patients treated medically have remission of acute
Слайд 26ACALCULOUS CHOLECYSTITIS
ETHIOLOGY. In 5 to 10% of patients with acute cholecystitis, calculi
ACALCULOUS CHOLECYSTITIS
ETHIOLOGY. In 5 to 10% of patients with acute cholecystitis, calculi
Слайд 27ACALCULOUS CHOLECYSTITIS
CLINICAL PICTURE. The clinical manifestations of acalculous cholecystitis are the same
ACALCULOUS CHOLECYSTITIS
CLINICAL PICTURE. The clinical manifestations of acalculous cholecystitis are the same
Слайд 28CHRONIC CHOLECYSTITIS
ETHIOLOGY, CLINICAL PICTURE
Chronic inflammation of the gallbladder wall is almost always
CHRONIC CHOLECYSTITIS
ETHIOLOGY, CLINICAL PICTURE
Chronic inflammation of the gallbladder wall is almost always
Слайд 29CHRONIC CHOLECYSTITIS. Complications
EMPYEMA of the gallbladder usually results from progression of acute
CHRONIC CHOLECYSTITIS. Complications
EMPYEMA of the gallbladder usually results from progression of acute
Слайд 30CHRONIC CHOLECYSTITIS. Complications
HYDROPS or MUCOCELE of the gallbladder may also result from
CHRONIC CHOLECYSTITIS. Complications
HYDROPS or MUCOCELE of the gallbladder may also result from
Слайд 31CHRONIC CHOLECYSTITIS. Complications
GANGRENE of the gallbladder results from ischemia of the wall
CHRONIC CHOLECYSTITIS. Complications
GANGRENE of the gallbladder results from ischemia of the wall
Слайд 32CHRONIC CHOLECYSTITIS. MEDICAL TREATMENT
Although surgical intervention remains the mainstay of therapy for
CHRONIC CHOLECYSTITIS. MEDICAL TREATMENT
Although surgical intervention remains the mainstay of therapy for
Слайд 33CHRONIC CHOLECYSTITIS. MEDICAL TREATMENT
Intravenous antibiotic therapy is usually indicated in patients with
CHRONIC CHOLECYSTITIS. MEDICAL TREATMENT
Intravenous antibiotic therapy is usually indicated in patients with
Слайд 34CHRONIC CHOLECYSTITIS. SURGICAL TREATMENT
The optimal timing of surgical intervention in patients with
CHRONIC CHOLECYSTITIS. SURGICAL TREATMENT
The optimal timing of surgical intervention in patients with
Слайд 35CHRONIC CHOLECYSTITIS. SURGICAL TREATMENT
Delayed surgical intervention is probably best reserved for
(1)
CHRONIC CHOLECYSTITIS. SURGICAL TREATMENT
Delayed surgical intervention is probably best reserved for
(1)
Слайд 36Postcholecystectomy Complications
Early complications following cholecystectomy include atelectasis and other pulmonary disorders, abscess
Postcholecystectomy Complications
Early complications following cholecystectomy include atelectasis and other pulmonary disorders, abscess
Слайд 37LIST OF DISEASES OF THE BILE DUCTS
CONGENITAL ANOMALIES
CHOLEDOCHOLITHIASIS
CHOLANGITIS
PAPILLARY DYSFUNCTION
PAPILLARY STENOSIS
SPASM OF THE
LIST OF DISEASES OF THE BILE DUCTS
CONGENITAL ANOMALIES
CHOLEDOCHOLITHIASIS
CHOLANGITIS
PAPILLARY DYSFUNCTION
PAPILLARY STENOSIS
SPASM OF THE
Слайд 38DISEASES OF THE BILE DUCTS. CONGENITAL ANOMALIES
Biliary Atresia and Hypoplasia
Atretic and hypoplastic
DISEASES OF THE BILE DUCTS. CONGENITAL ANOMALIES
Biliary Atresia and Hypoplasia
Atretic and hypoplastic
Слайд 39DISEASES OF THE BILE DUCTS. CONGENITAL ANOMALIES
Congenital Biliary Ectasia
Dilatation of intrahepatic bile
DISEASES OF THE BILE DUCTS. CONGENITAL ANOMALIES
Congenital Biliary Ectasia
Dilatation of intrahepatic bile
Слайд 40DISEASES OF THE BILE DUCTS.
CHOLEDOCHOLITHIASIS
Passage of gallstones into the CBD occurs in
DISEASES OF THE BILE DUCTS.
CHOLEDOCHOLITHIASIS
Passage of gallstones into the CBD occurs in
Слайд 41DISEASES OF THE BILE DUCTS
CHOLEDOCHOLITHIASIS
Primary calculi arising de novo in the ducts
DISEASES OF THE BILE DUCTS
CHOLEDOCHOLITHIASIS
Primary calculi arising de novo in the ducts
Слайд 42ENDOSCOPIC RETROGRADE CHOLANGIOPANCREATOGRAM. CHOLEDOCHOLITHIASIS
ERCP showing common duct stones
ENDOSCOPIC RETROGRADE CHOLANGIOPANCREATOGRAM. CHOLEDOCHOLITHIASIS
ERCP showing common duct stones
Слайд 43CHOLEDOCHOLITHIASIS. Complications
CHOLANGITIS
Cholangitis may be acute or chronic, and symptoms result from
CHOLEDOCHOLITHIASIS. Complications
CHOLANGITIS
Cholangitis may be acute or chronic, and symptoms result from
Слайд 44CHOLEDOCHOLITHIASIS. Complications
Nonsuppurative acute cholangitis is most common and may respond relatively rapidly
CHOLEDOCHOLITHIASIS. Complications
Nonsuppurative acute cholangitis is most common and may respond relatively rapidly
Слайд 45CHOLEDOCHOLITHIASIS
Complications. OBSTRUCTIVE JAUNDICE
Gradual obstruction of the CBD over a period of weeks
CHOLEDOCHOLITHIASIS
Complications. OBSTRUCTIVE JAUNDICE
Gradual obstruction of the CBD over a period of weeks
Слайд 46CHOLEDOCHOLITHIASIS
Complications. OBSTRUCTIVE JAUNDICE
CBD stones should be suspected in any patient with cholecystitis
CHOLEDOCHOLITHIASIS
Complications. OBSTRUCTIVE JAUNDICE
CBD stones should be suspected in any patient with cholecystitis
Слайд 47PAPILLARY DYSFUNCTION, STENOSIS, SPASM OF THE SPHINCTER OF ODDI, BILIARY DYSKINESIA
Symptoms of
PAPILLARY DYSFUNCTION, STENOSIS, SPASM OF THE SPHINCTER OF ODDI, BILIARY DYSKINESIA
Symptoms of
Слайд 48PAPILLARY DYSFUNCTION, STENOSIS, SPASM OF THE SPHINCTER OF ODDI, BILIARY DYSKINESIA
An alternative
PAPILLARY DYSFUNCTION, STENOSIS, SPASM OF THE SPHINCTER OF ODDI, BILIARY DYSKINESIA
An alternative
Слайд 49 Proposed mechanisms of Dyskinesia of the sphincter of Oddi include spasm
Proposed mechanisms of Dyskinesia of the sphincter of Oddi include spasm
Слайд 50Neoplasms of the biliary tract: Carcinoma of the biliary system manifests with
Neoplasms of the biliary tract: Carcinoma of the biliary system manifests with
Слайд 51SCLEROSING CHOLANGITIS
Definition. Primary or idiopathic sclerosing cholangitis is characterized by a progressive,
SCLEROSING CHOLANGITIS
Definition. Primary or idiopathic sclerosing cholangitis is characterized by a progressive,
Слайд 52SCLEROSING CHOLANGITIS
Secondary sclerosing cholangitis may occur as a long-term complication of choledocholithiasis,
SCLEROSING CHOLANGITIS
Secondary sclerosing cholangitis may occur as a long-term complication of choledocholithiasis,
Слайд 53DIFFERENTIAL DIAGNOSIS OF JAUNDICE AND HYPERBILIRUBINEMIA
Increased formation and hepatocellular diseases that impair
DIFFERENTIAL DIAGNOSIS OF JAUNDICE AND HYPERBILIRUBINEMIA
Increased formation and hepatocellular diseases that impair
Слайд 54Noncholestatic Conjugated Hyperbilirubinemia
Disorders of bilirubin metabolism causing conjugated hyperbilirubinemia without cholestasis produce
Noncholestatic Conjugated Hyperbilirubinemia
Disorders of bilirubin metabolism causing conjugated hyperbilirubinemia without cholestasis produce
Слайд 55Unconjugated Hyperbilirubinemia
Unconjugated hyperbilirubinemia is a disorder of bilirubin metabolism consisting of overproduction
Unconjugated Hyperbilirubinemia
Unconjugated hyperbilirubinemia is a disorder of bilirubin metabolism consisting of overproduction
Слайд 56Unconjugated Hyperbilirubinemia
Crigler-Najjar syndrome: This rare inherited disorder is caused by deficiency of
Unconjugated Hyperbilirubinemia
Crigler-Najjar syndrome: This rare inherited disorder is caused by deficiency of
 Организация учебно-туристской работы в школе и учебные походы
Организация учебно-туристской работы в школе и учебные походы Планшеты для профессиональной работы
Планшеты для профессиональной работы Культура Великобританії 19 ст
Культура Великобританії 19 ст Химические свойства алкенов
Химические свойства алкенов Что такое проектный метод?
Что такое проектный метод? Аҳду амалиётҳои бонки исломӣ
Аҳду амалиётҳои бонки исломӣ SOCIAL-UP Уникальная бизнес возможность
SOCIAL-UP Уникальная бизнес возможность Complete each sentence with has/have and a participle from the box
Complete each sentence with has/have and a participle from the box АИС Аптекарь 8.1 Конструирование отчетов
АИС Аптекарь 8.1 Конструирование отчетов Брендинг
Брендинг Презентация - Ошибки в разработке интернет-магазина
Презентация - Ошибки в разработке интернет-магазина 7 Чудес Коми
7 Чудес Коми Презентация на тему Реформы Хрущева
Презентация на тему Реформы Хрущева Подъёмные механизмы. Профессии этой сферы
Подъёмные механизмы. Профессии этой сферы Основы моделирования изделия
Основы моделирования изделия Виконання зварного з'єднання
Виконання зварного з'єднання Профессия электрик
Профессия электрик Вселенная
Вселенная Игристые вина
Игристые вина Презентация на тему Как человек реагирует на явления в жизни и искусстве
Презентация на тему Как человек реагирует на явления в жизни и искусстве Презентация на тему Режим дня дошкольника
Презентация на тему Режим дня дошкольника Complex Object
Complex Object Кавказ в русской поэзии
Кавказ в русской поэзии Профилактика
Профилактика Число и цифра 2 (1 класс)
Число и цифра 2 (1 класс) Предлагаемая стоимость объекта – 41 000$
Предлагаемая стоимость объекта – 41 000$ Фелтинг
Фелтинг Изменения в ЕГЭ по русскому языку в 2012 году
Изменения в ЕГЭ по русскому языку в 2012 году