- Human digestion

Содержание
- 2. Human digestion
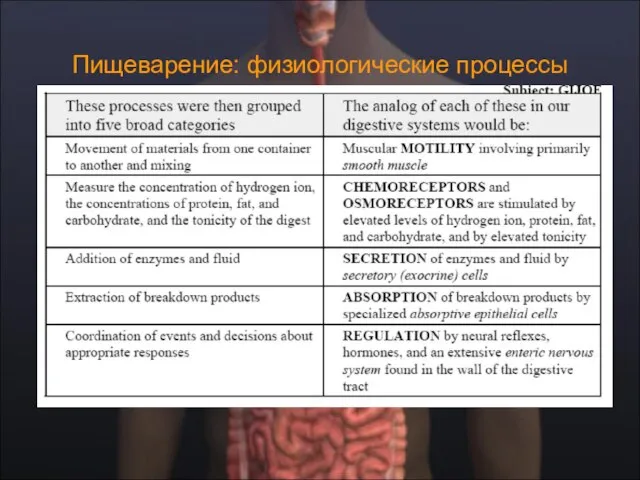
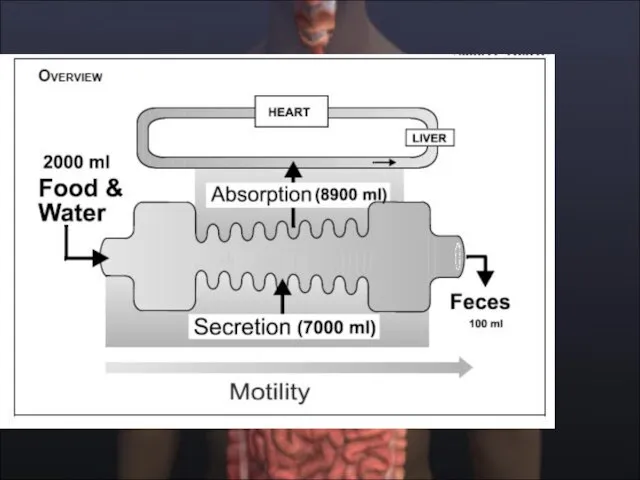
- 4. Пищеварение: физиологические процессы
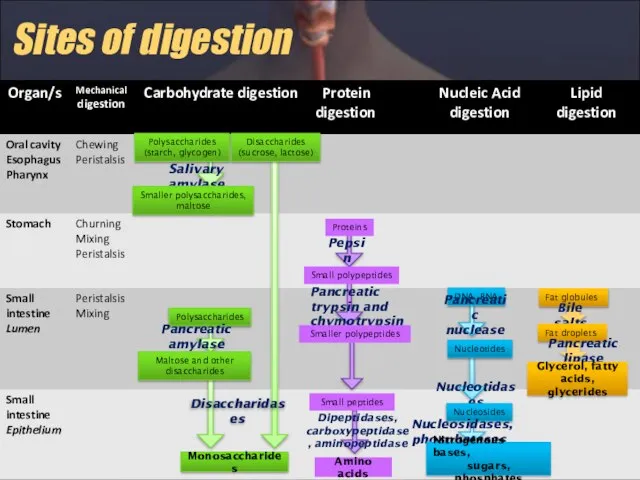
- 6. Sites of digestion
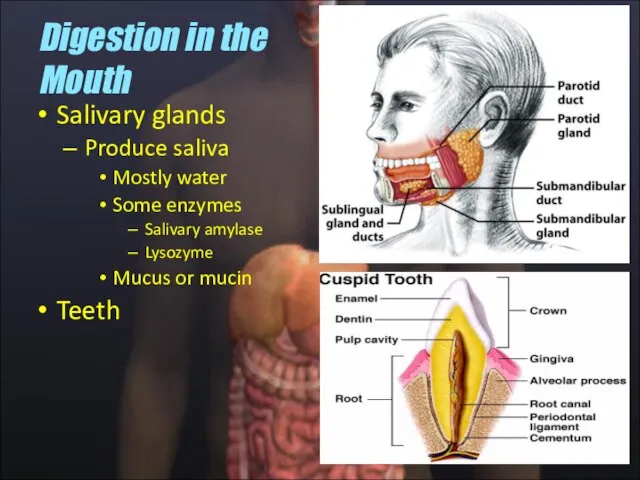
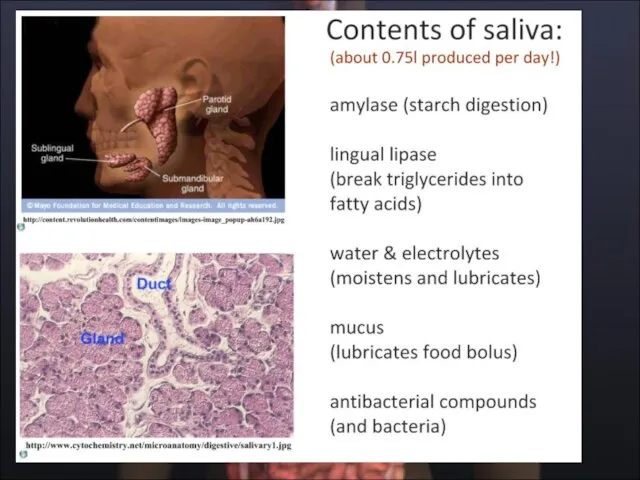
- 7. Salivary glands Produce saliva Mostly water Some enzymes Salivary amylase Lysozyme Mucus or mucin Teeth Digestion
- 8. Функции слюны ˆ увлажняет пищу, облегчает глотание, ˆпредупреждает аспирацию пищи в трахею, способствуя формированию пищевого комка,
- 10. Образование слюны
- 11. Функция протоков слюнных желез
- 13. Takehito Etani, Masticator triptych, 2005.
- 14. Mastication. masticatory cycle (chewing cycle) the complete pathway of the mandible
- 15. Mastication
- 16. The Muscles of Mastication (Chewing) Перетирание или жевание, выполняется скоординированной функцией четырех важных мышц, которые сжимают
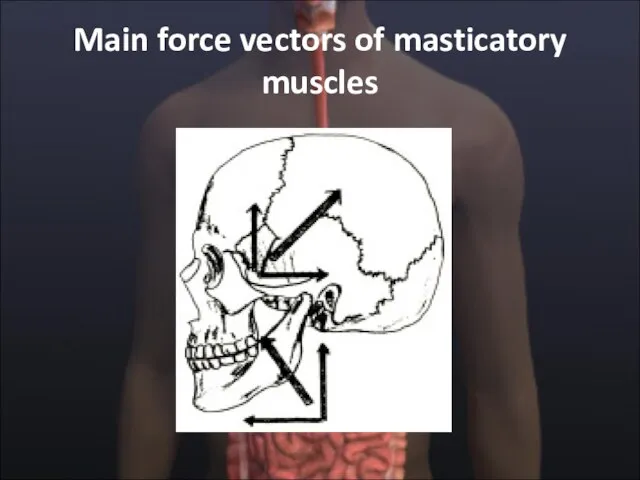
- 17. Main force vectors of masticatory muscles
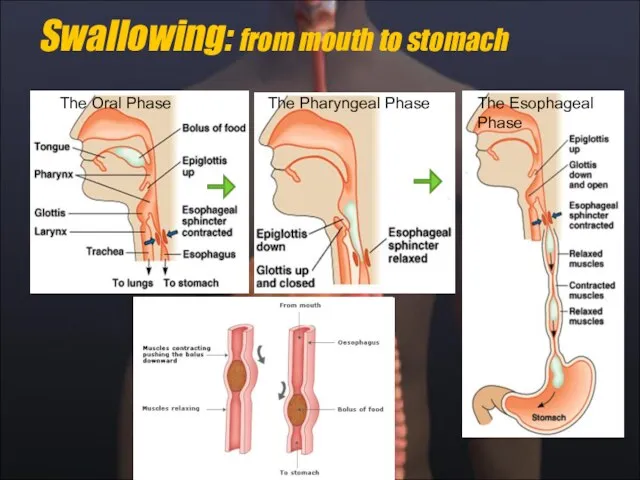
- 18. Swallowing: from mouth to stomach The Oral Phase The Pharyngeal Phase The Esophageal Phase
- 19. Oral Preparatory Stage Ротовая предварительная стадия по существу жевание. Это включает координацию губ, щек, челюсти, языка
- 20. Oral Stage Ротовая стадия - вторая стадия глотания. Это длится приблизительно 1 секунду, и не меняется
- 21. Pharyngeal Stage The pharyngeal stage begins when the bolus reaches the anterior faucial arches. Here, the
- 22. Swallowing Reflex (Pharyngeal Stage) When triggered, the swallowing reflex results in four neuromuscular functions, which occur
- 23. Laryngeal closure occurs at three sphincters: 1) the epiglottis and aryepiglottic folds, 2) the false vocal
- 24. Pharyngoesophageal segment opening depends on: 1) relaxation of the cricopharyngeus, 2) the upward, anterior pull of
- 25. Esophageal Stage The fourth and final stage of swallowing is the esophageal stage. It is more
- 26. Swallowing Centers In humans, the development of functional magnetic resonance imaging (fMRI) has allowed the identification
- 27. Swallowing Centers There is convincing evidence that the sequential and rhythmic patterns of swallowing are formed
- 28. Swallowing Centers The voluntary initiation of swallowing takes place in special brain areas located in the
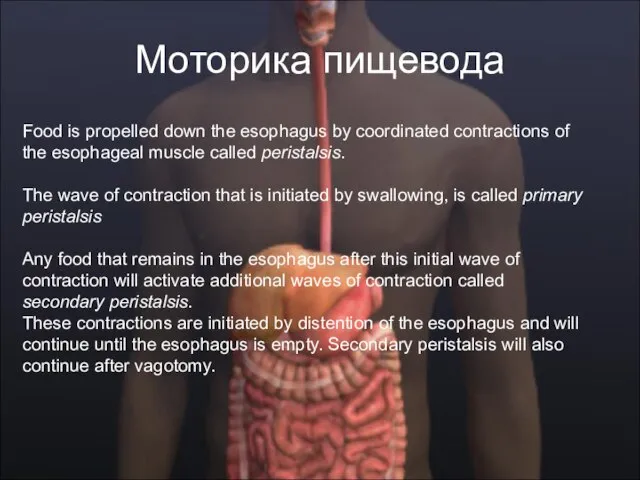
- 31. Моторика пищевода Food is propelled down the esophagus by coordinated contractions of the esophageal muscle called
- 32. Пищеварение в желудке
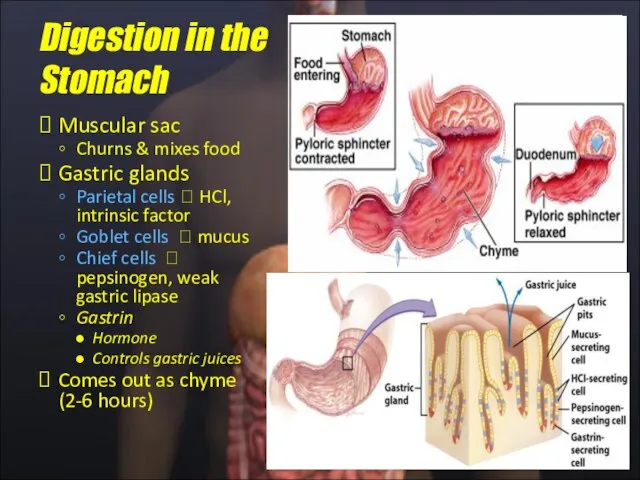
- 33. Muscular sac Churns & mixes food Gastric glands Parietal cells ? HCl, intrinsic factor Goblet cells
- 34. Функции желудка ˆ Serves as a reservoir that allows for the ingestion of food faster than
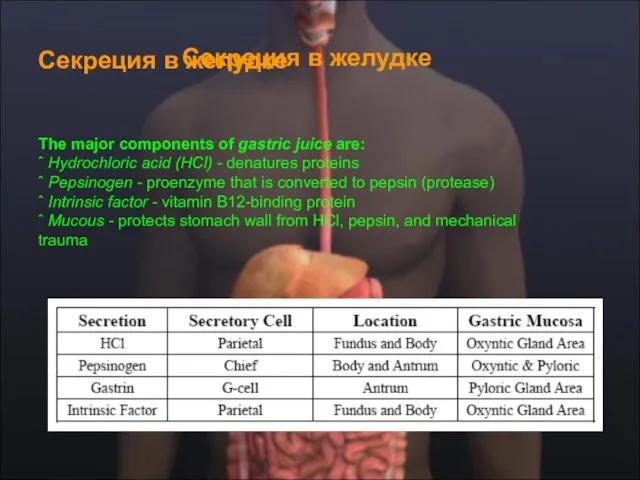
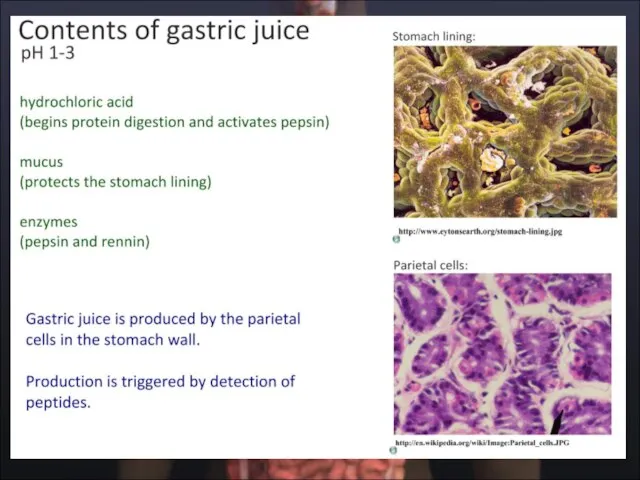
- 35. Секреция в желудке Секреция в желудке The major components of gastric juice are: ˆ Hydrochloric acid
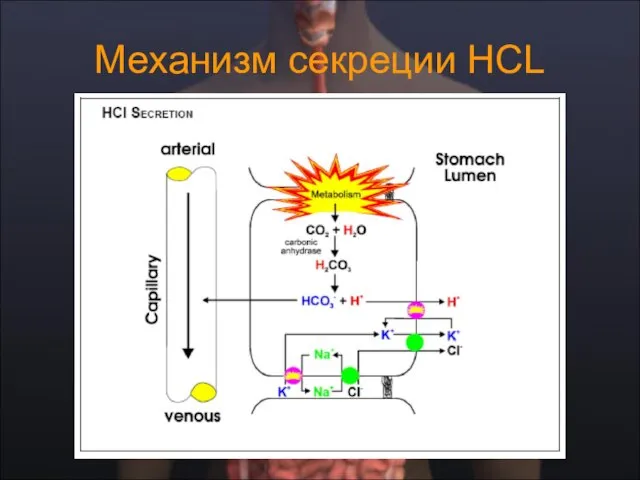
- 37. Механизм секреции НСL
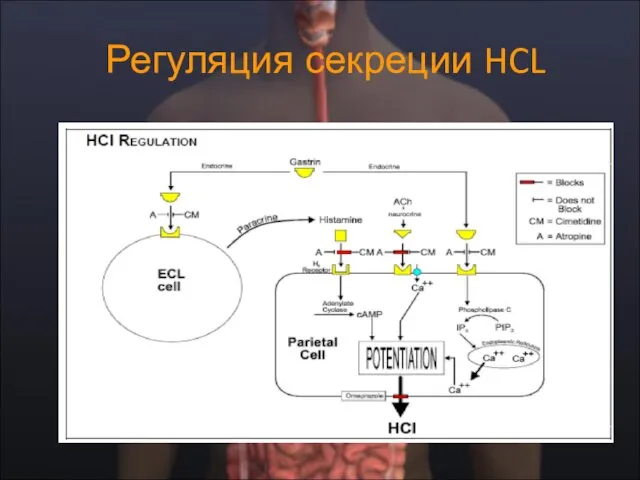
- 38. Регуляция секреции HCL
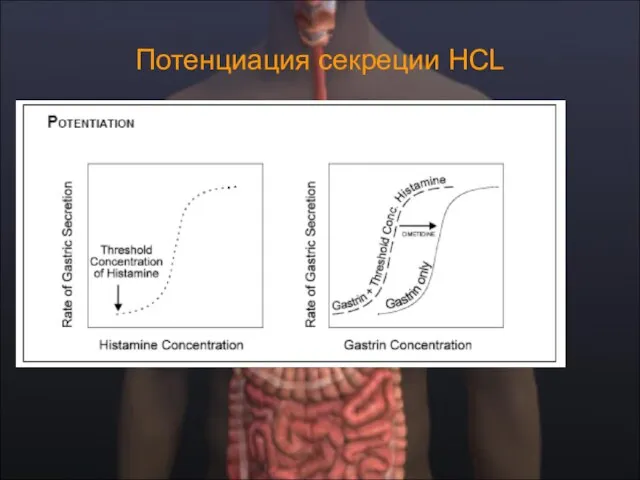
- 39. Потенциация секреции HCL
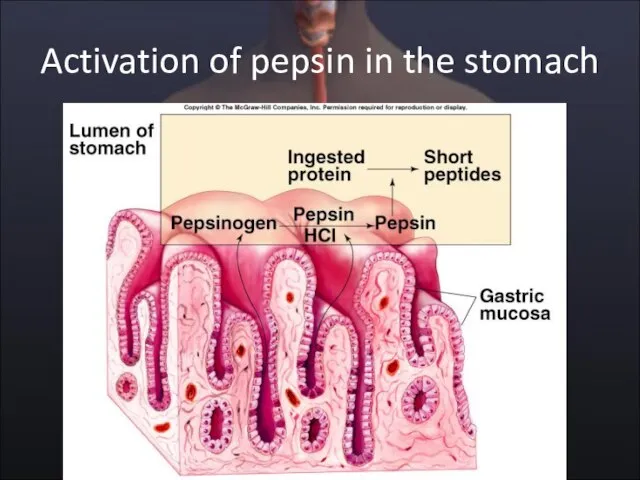
- 40. Activation of pepsin in the stomach
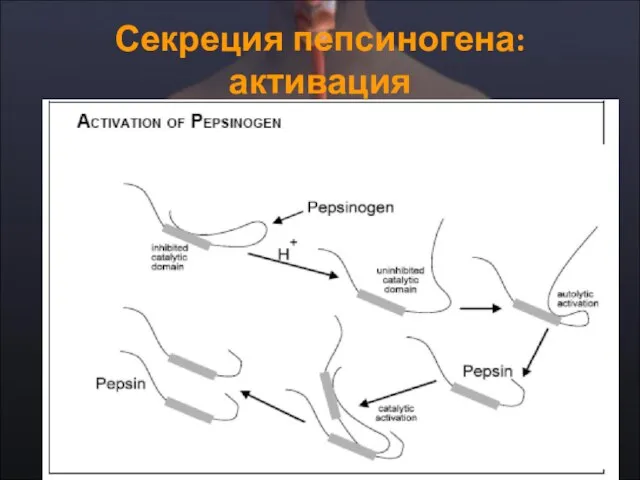
- 41. Секреция пепсиногена: активация
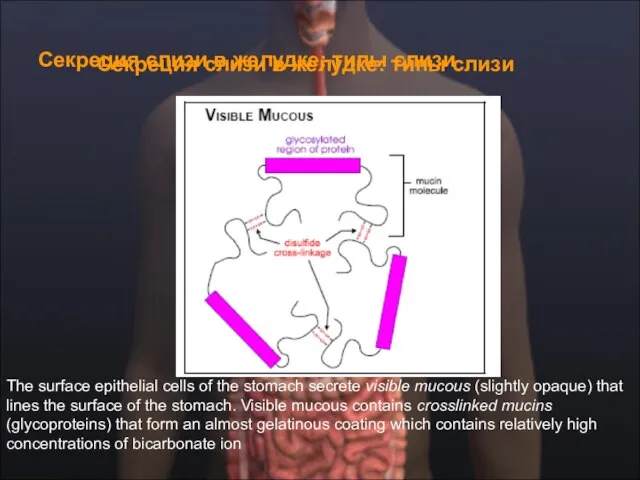
- 42. Секреция слизи в желудке: типы слизи Секреция слизи в желудке: типы слизи The surface epithelial cells
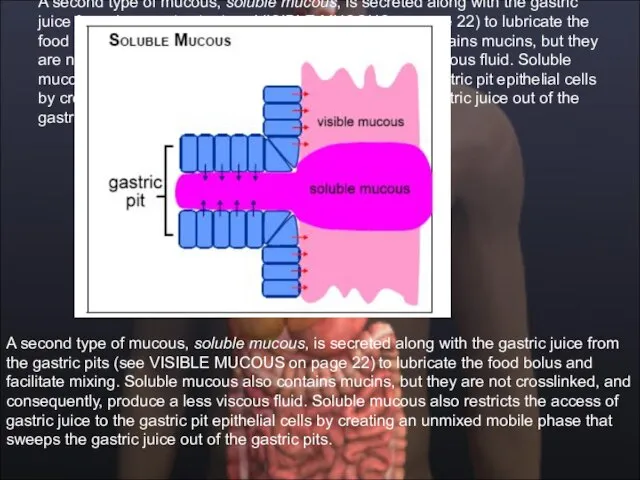
- 43. A second type of mucous, soluble mucous, is secreted along with the gastric juice from the
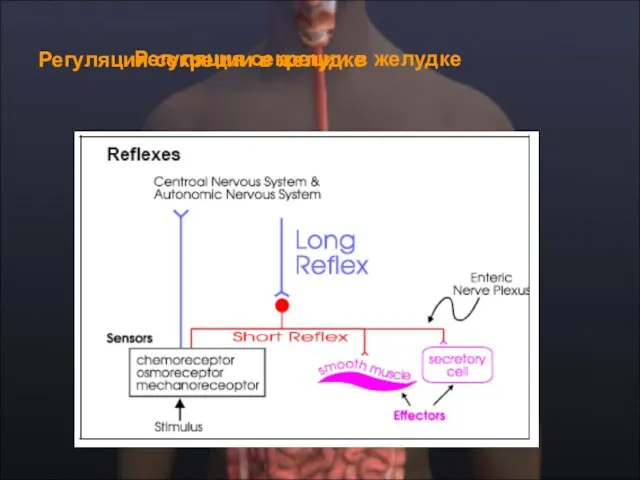
- 44. Регуляция секреции в желудке Регуляция секреции в желудке
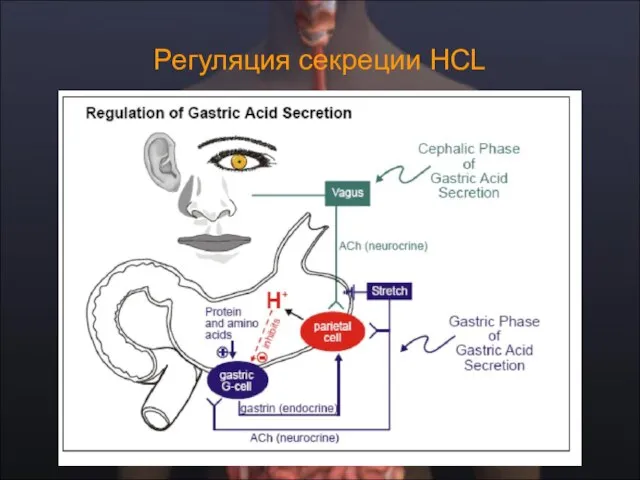
- 45. Регуляция секреции HCL
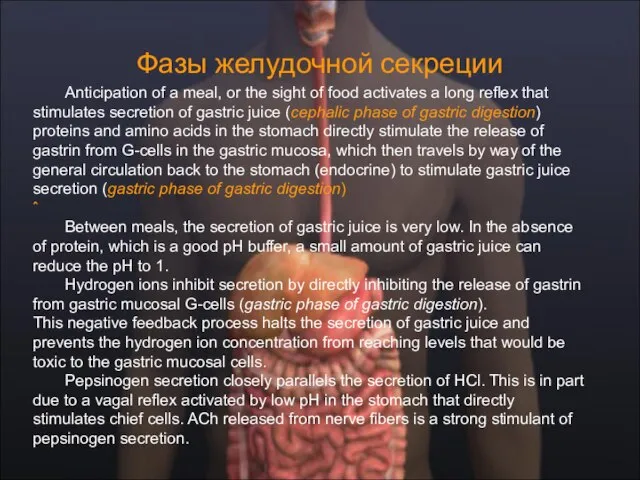
- 46. Фазы желудочной секреции Аnticipation of a meal, or the sight of food activates a long reflex
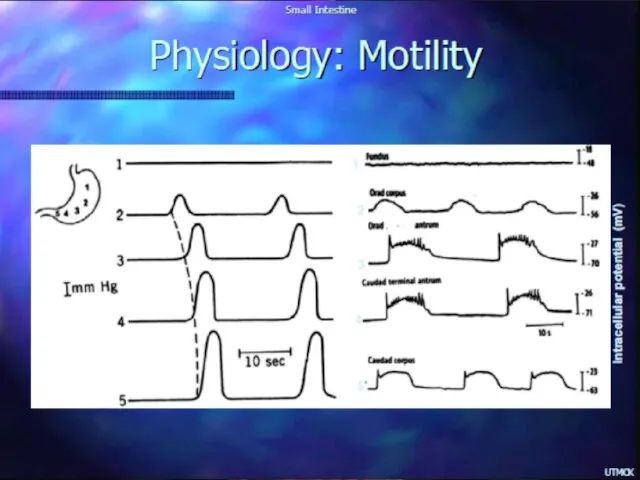
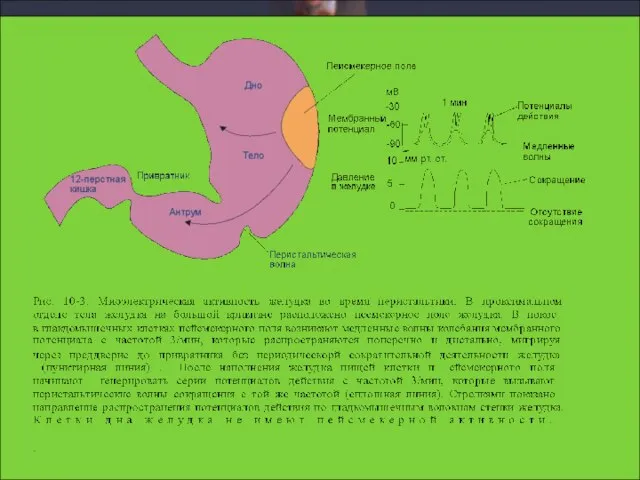
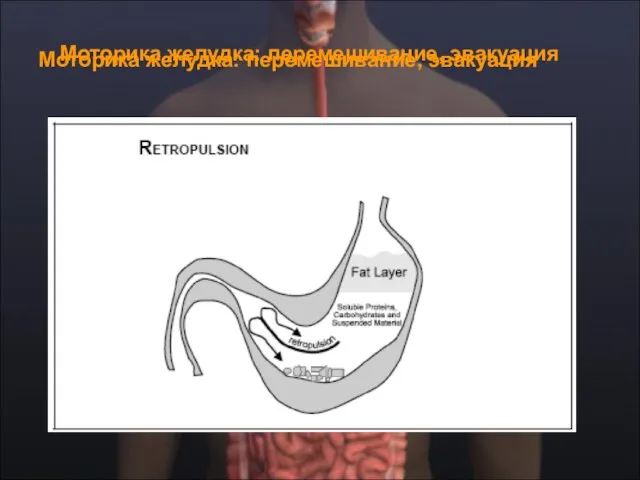
- 49. Моторика желудка: перемешивание, эвакуация Моторика желудка: перемешивание, эвакуация
- 50. Эвакуация: факторы регуляции The chyme coming from the stomach is normally hypertonic, acidic, and contains high
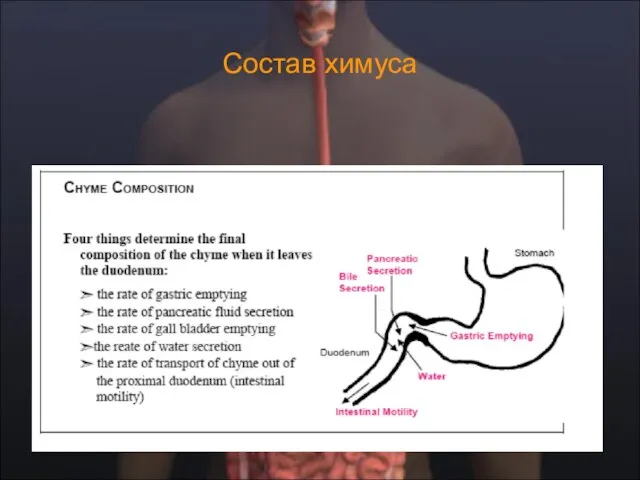
- 51. Состав химуса
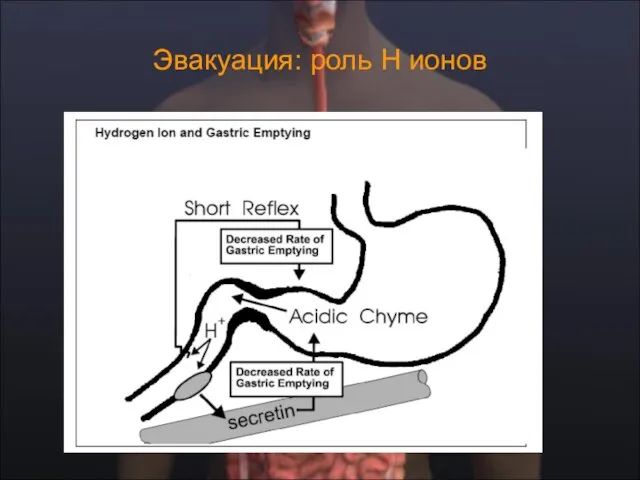
- 52. Эвакуация: роль Н ионов
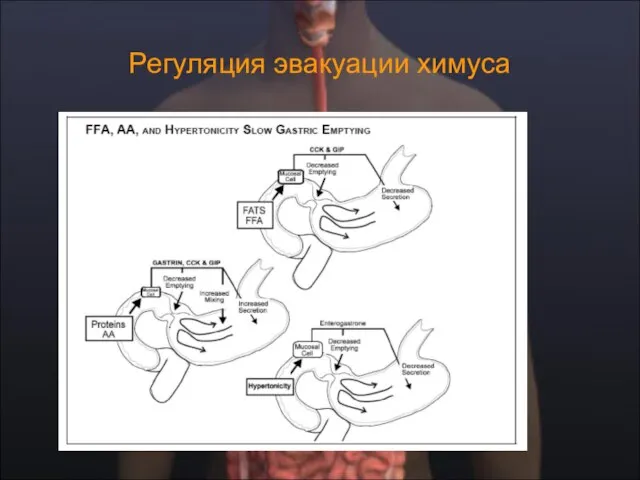
- 53. Регуляция эвакуации химуса
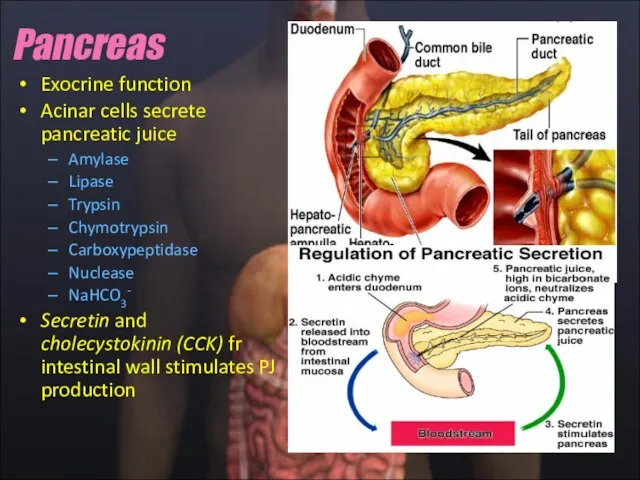
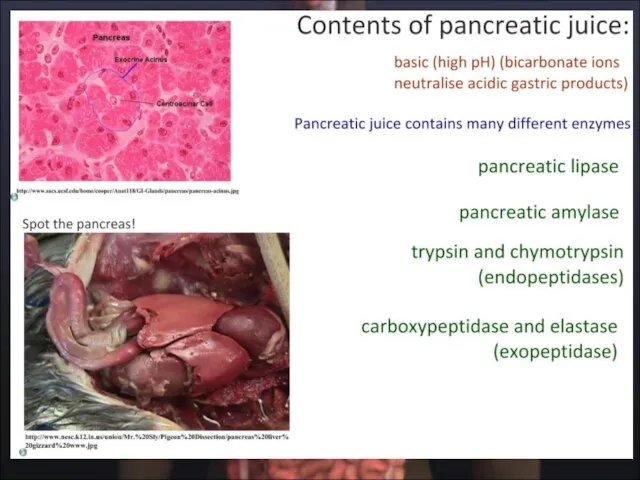
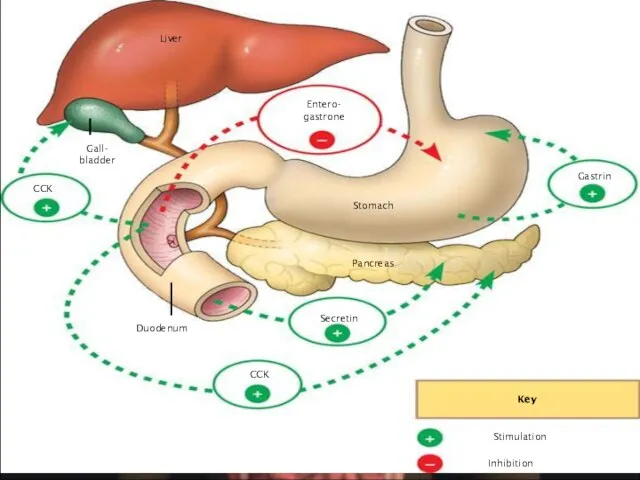
- 54. Exocrine function Acinar cells secrete pancreatic juice Amylase Lipase Trypsin Chymotrypsin Carboxypeptidase Nuclease NaHCO3- Secretin and
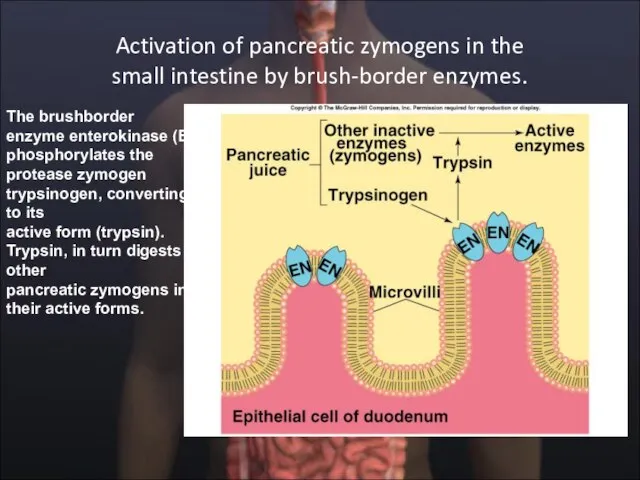
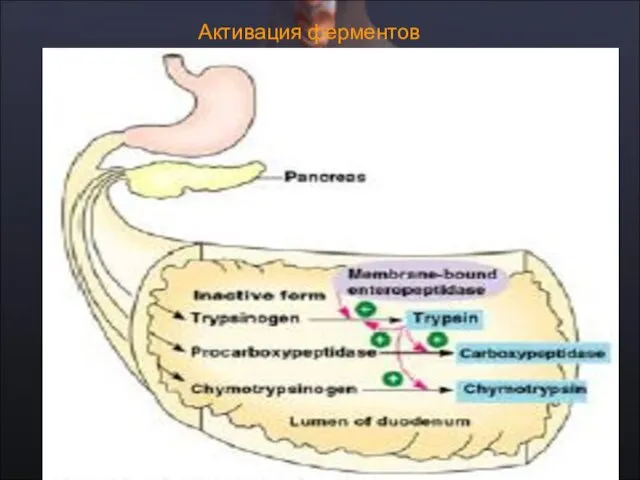
- 55. Activation of pancreatic zymogens in the small intestine by brush-border enzymes. The brushborder enzyme enterokinase (EN)
- 56. Активация ферментов
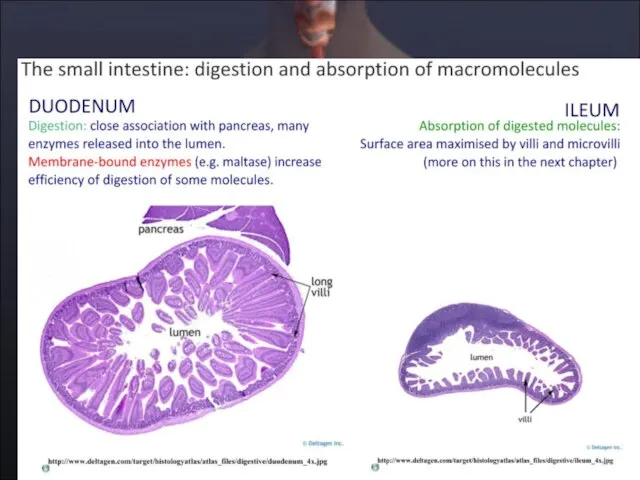
- 58. Пищеварение в duodenum
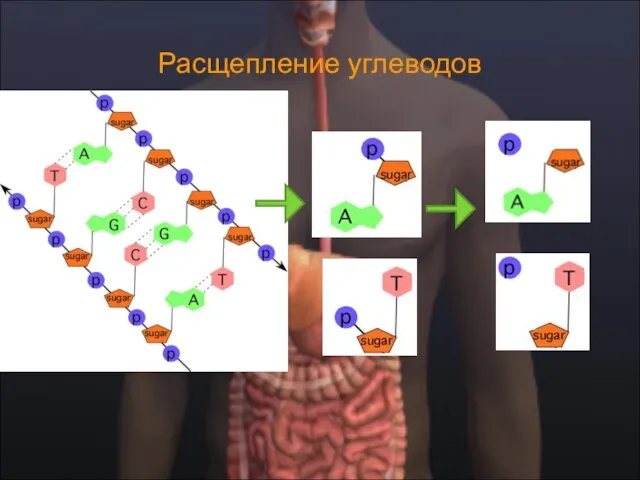
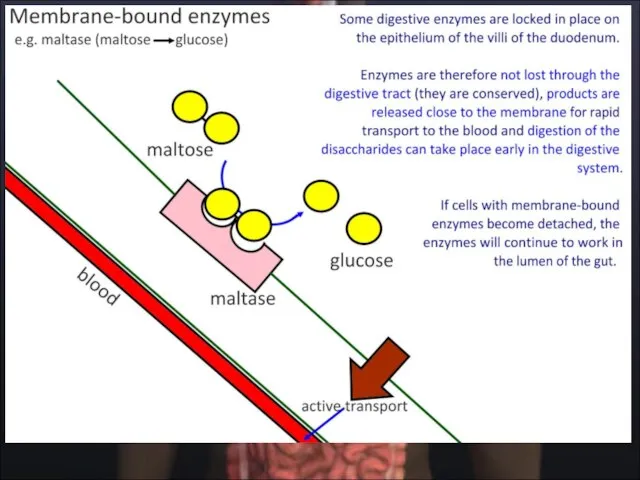
- 59. Расщепление углеводов
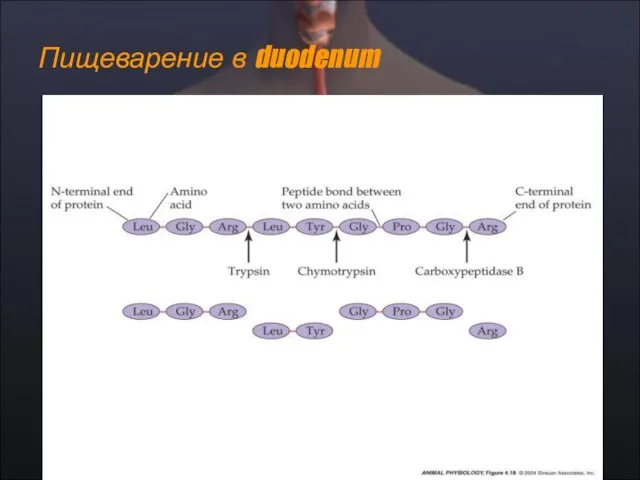
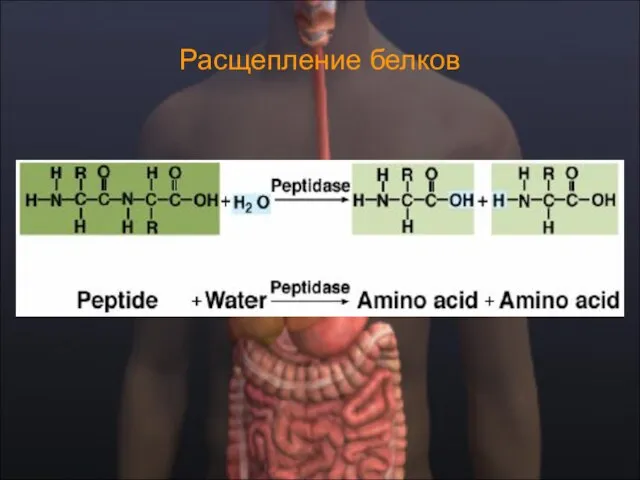
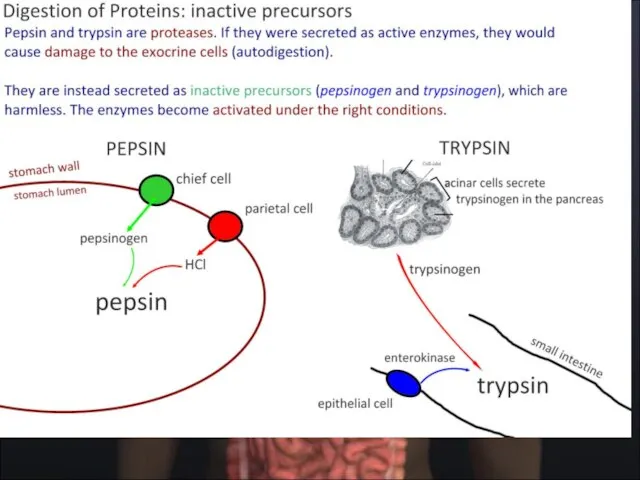
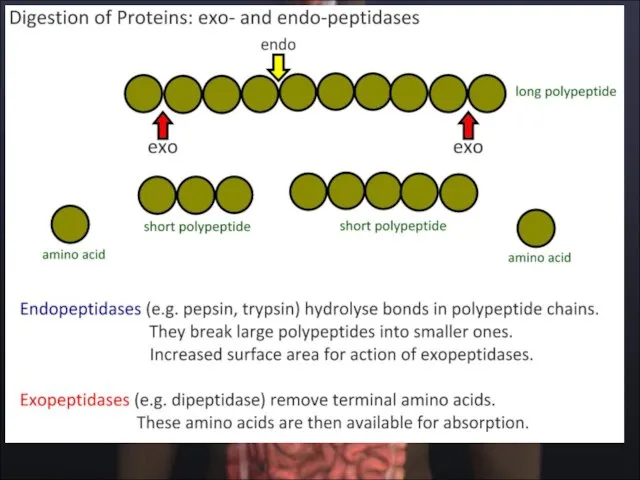
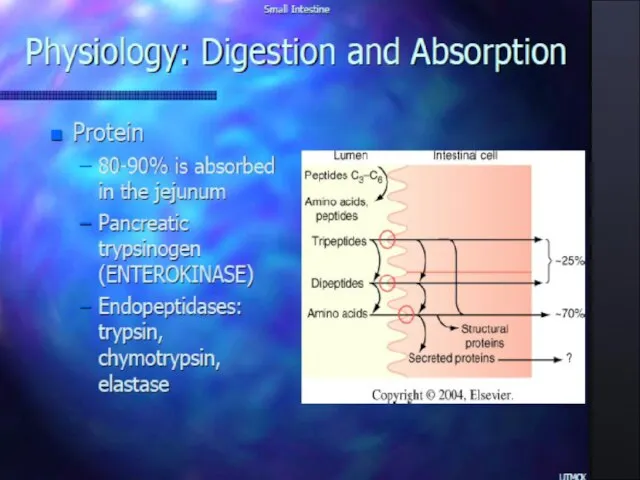
- 60. Расщепление белков
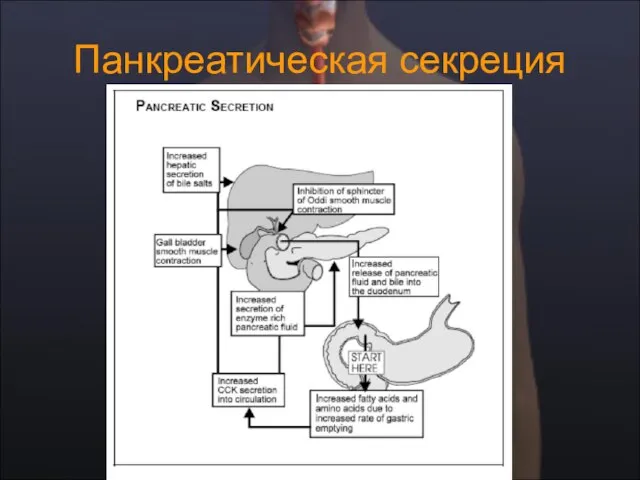
- 61. Панкреатическая секреция
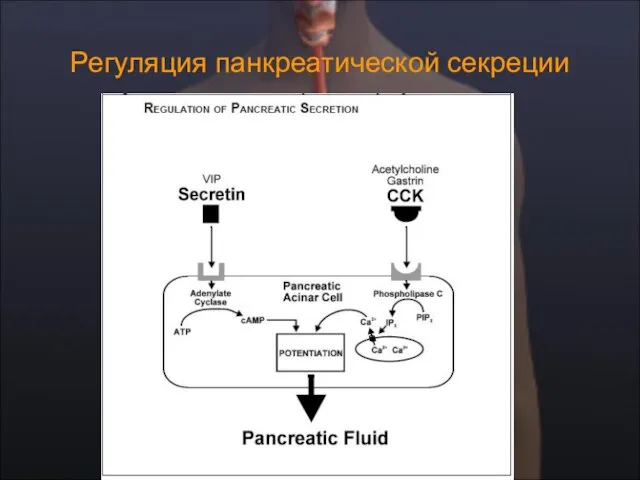
- 62. Регуляция панкреатической секреции
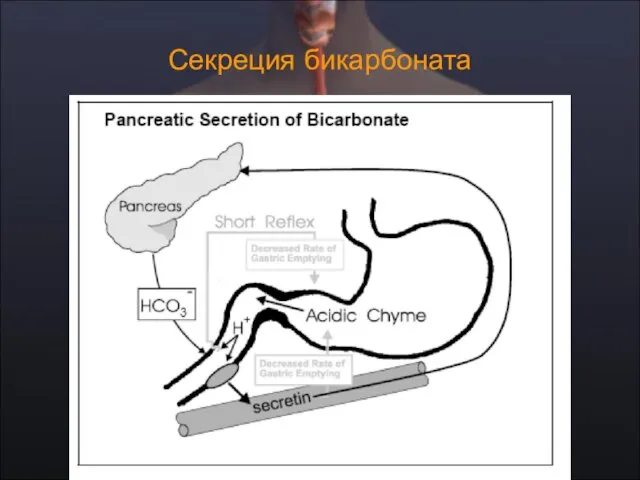
- 63. Секреция бикарбоната
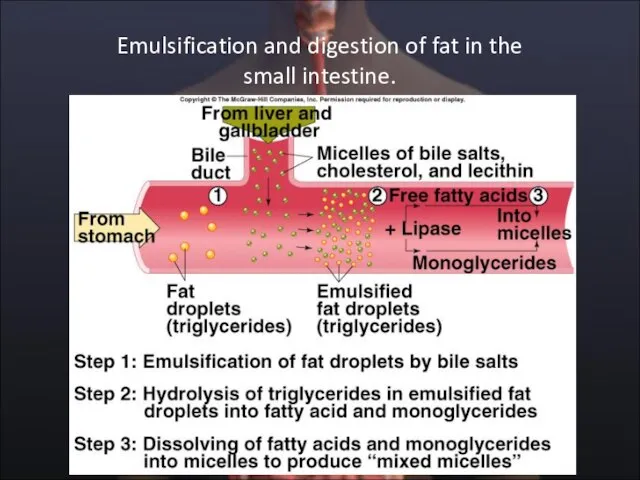
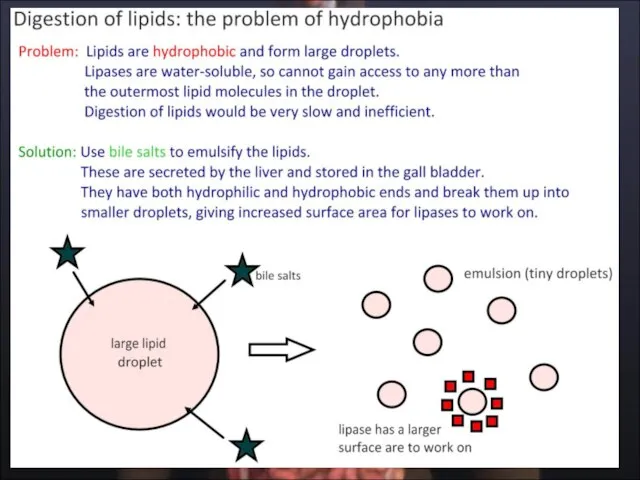
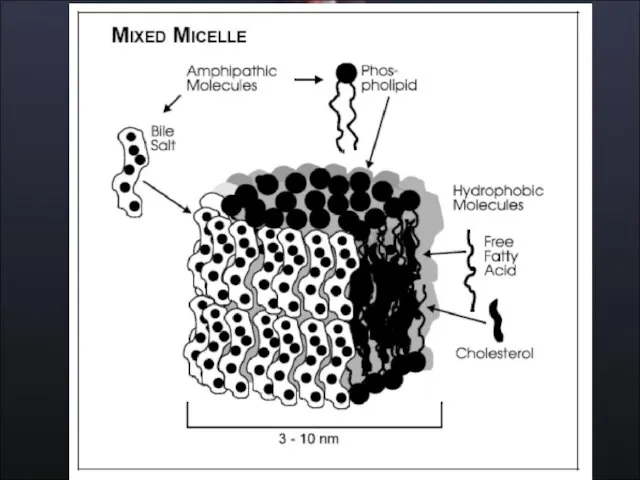
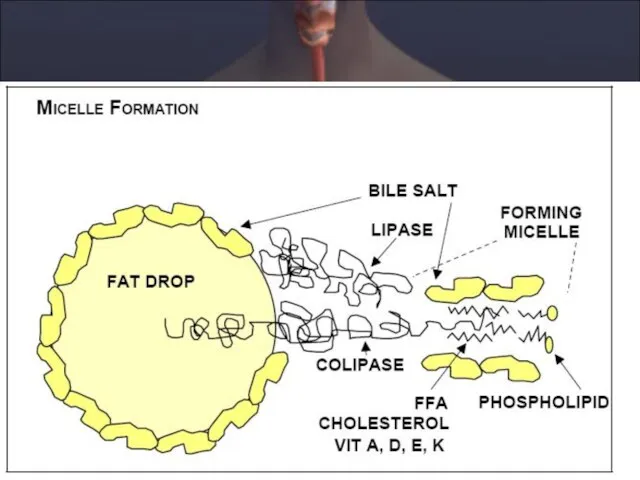
- 65. Emulsification and digestion of fat in the small intestine.
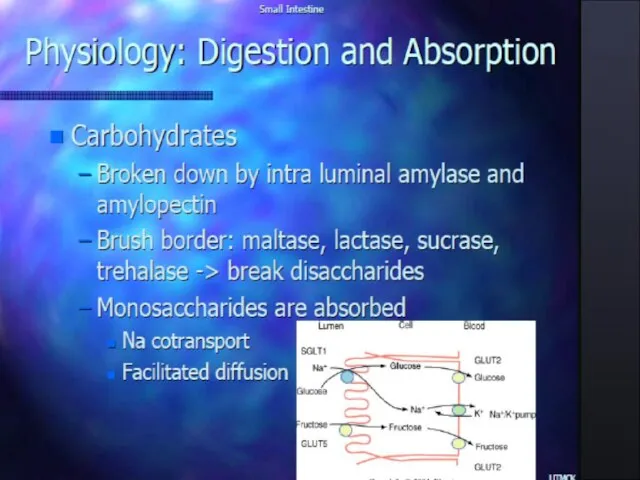
- 66. Пищеварение и всасывание углеводов и белков Пищеварение и всасывание углеводов и белков
- 75. Всасывание веществ в пищеварительном тракте
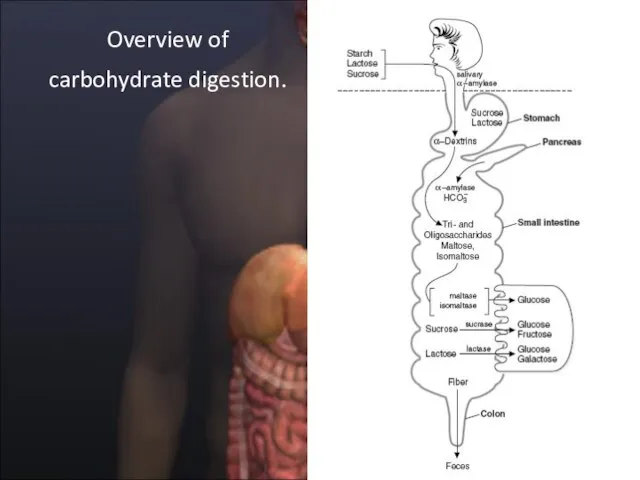
- 77. Overview of carbohydrate digestion.
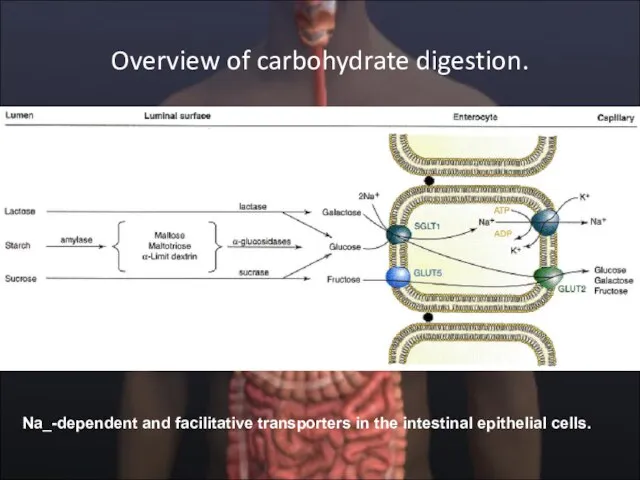
- 79. Overview of carbohydrate digestion. Na_-dependent and facilitative transporters in the intestinal epithelial cells.
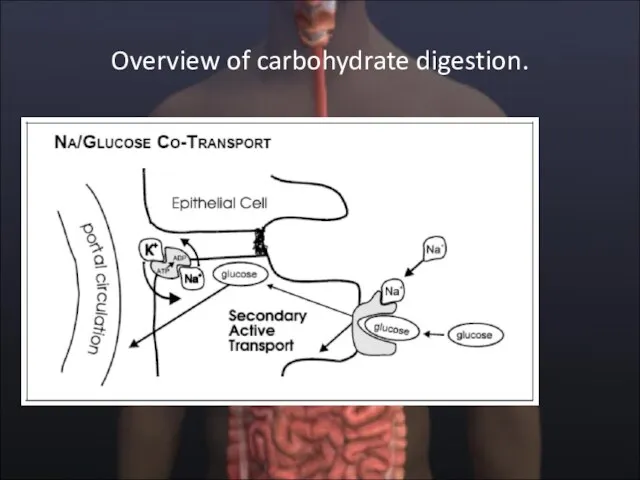
- 80. Overview of carbohydrate digestion.
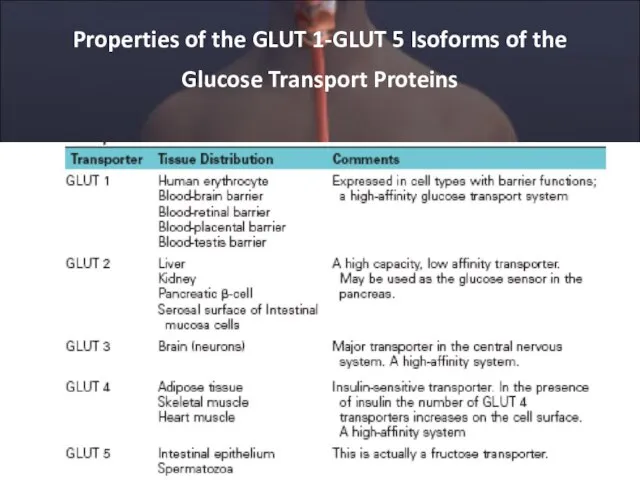
- 81. Properties of the GLUT 1-GLUT 5 Isoforms of the Glucose Transport Proteins
- 82. CLINICAL CORRELATION Disaccharidase Deficiency Intestinal disaccharidase deficiencies are encountered relatively frequently in humans. Deficiency can be
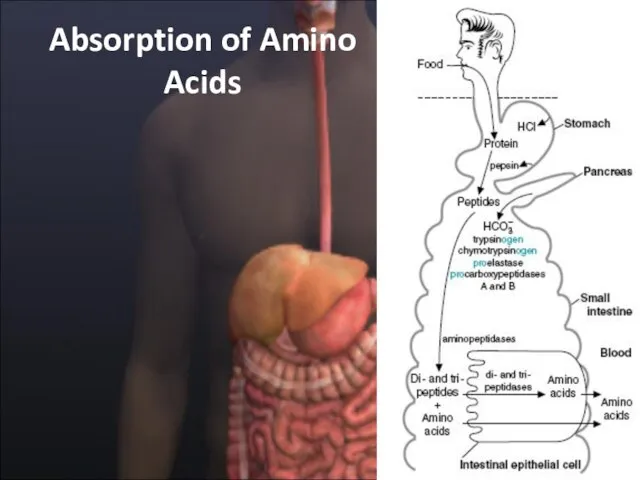
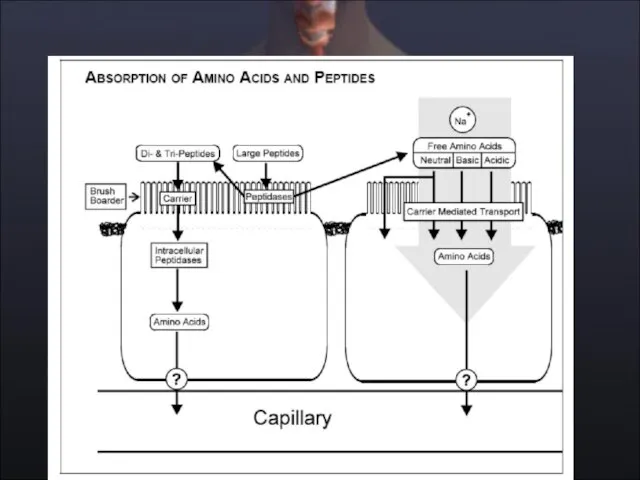
- 84. Absorption of Amino Acids
- 86. CLINICAL CORRELATION Neutral Amino Aciduria (Hartnup Disease) Transport functions, like enzymatic functions, are subject to modification
- 87. Kwashiorkor Kwashiorkor, A common problem of children in Third World countries, is caused by a deficiency
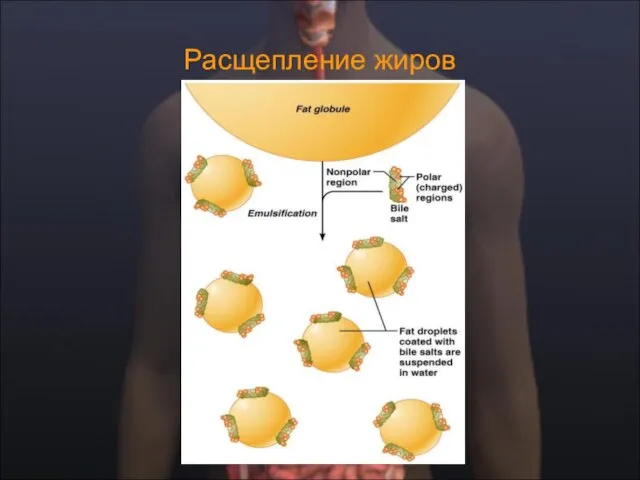
- 88. Расщепление жиров
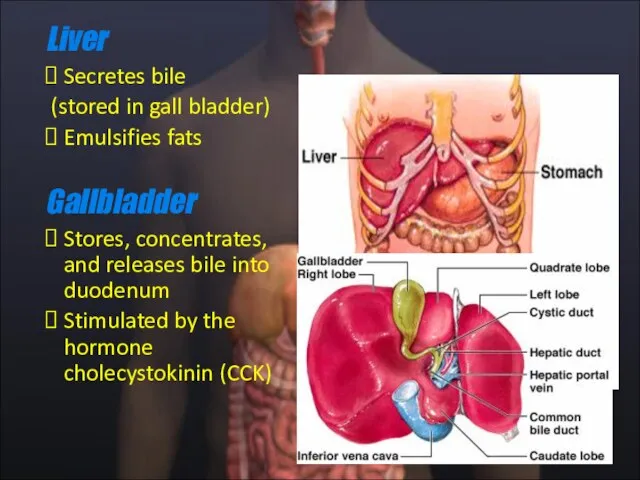
- 89. Liver Secretes bile (stored in gall bladder) Emulsifies fats Gallbladder Stores, concentrates, and releases bile into
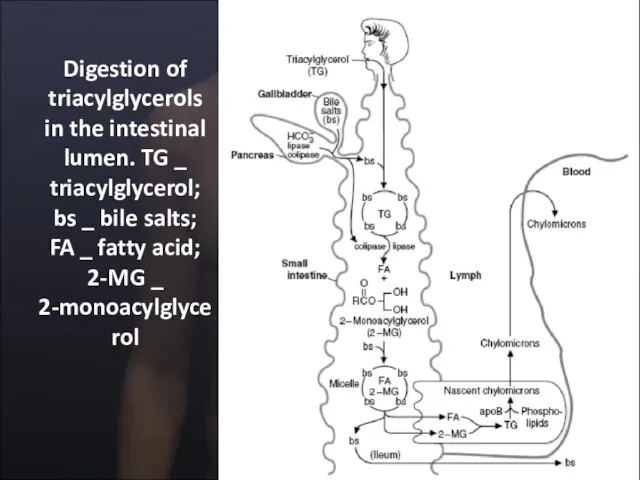
- 92. Digestion of triacylglycerols in the intestinal lumen. TG _ triacylglycerol; bs _ bile salts; FA _
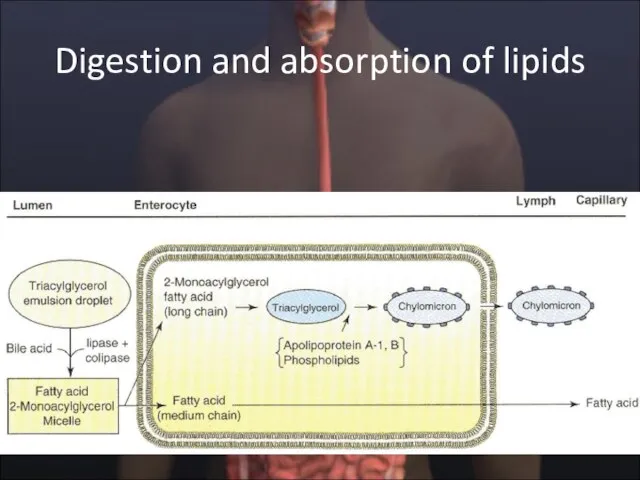
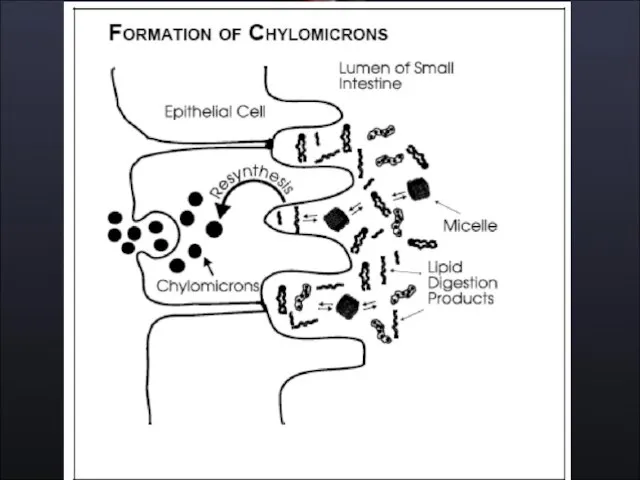
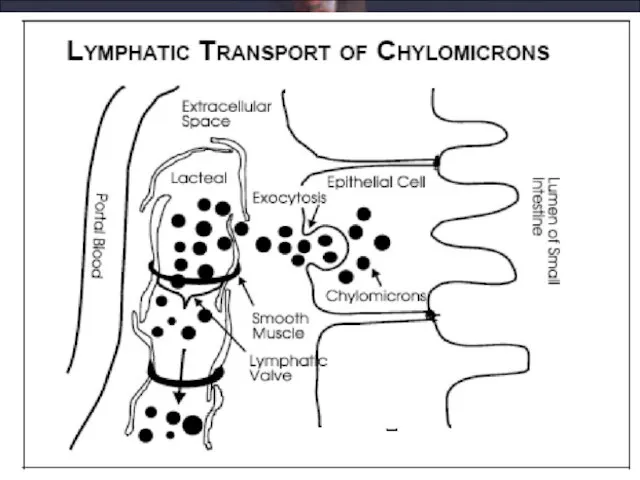
- 93. Digestion and absorption of lipids
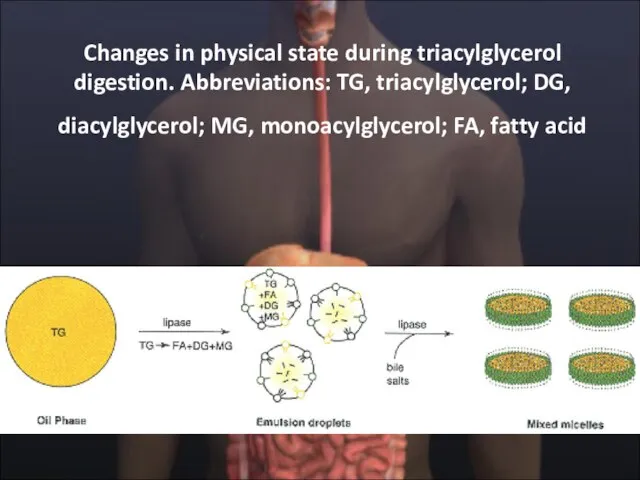
- 94. Changes in physical state during triacylglycerol digestion. Abbreviations: TG, triacylglycerol; DG, diacylglycerol; MG, monoacylglycerol; FA, fatty
- 101. CLINICAL CORRELATION A-β-Lipoproteinemia A-b-lipoproteinemia is an autosomal recessive disorder characterized by the absence of all lipoproteins
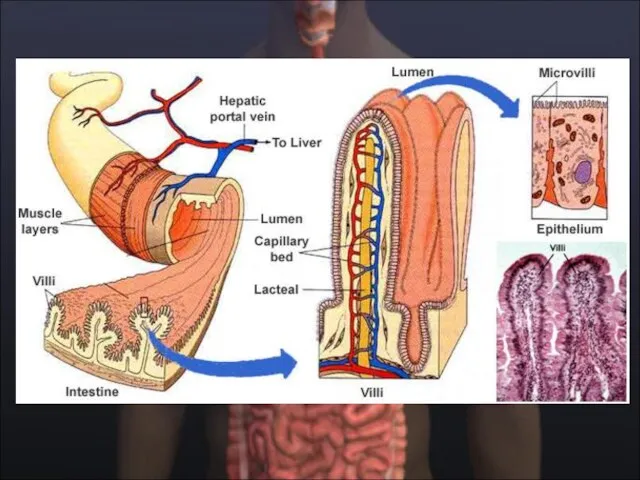
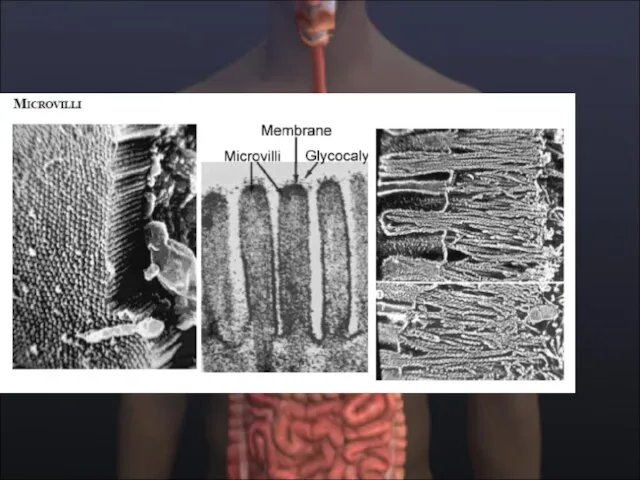
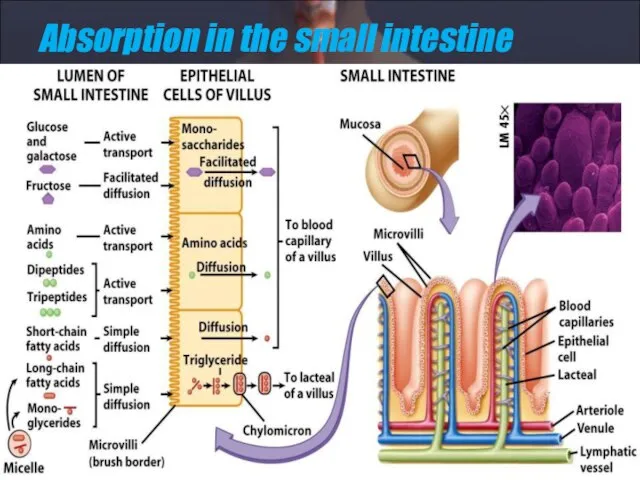
- 102. Absorption in the small intestine
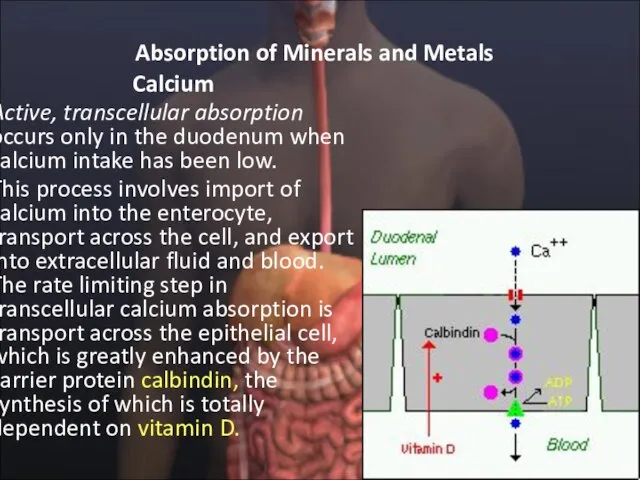
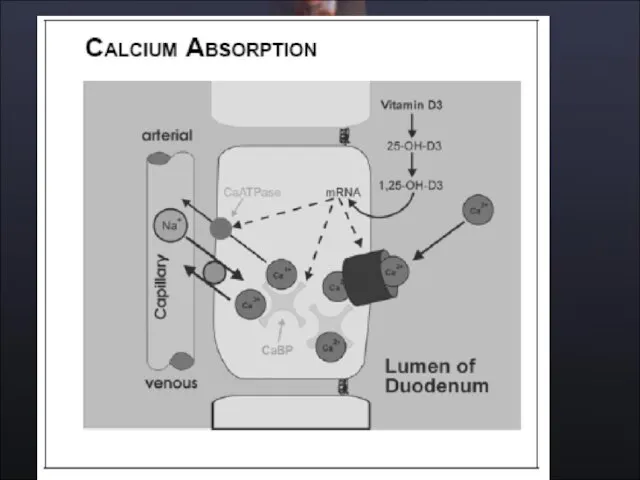
- 103. Absorption of Minerals and Metals Calcium Active, transcellular absorption occurs only in the duodenum when calcium
- 105. Calcium Passive, paracellular absorption occurs in the jejunum and ileum, and, to a much lesser extent,
- 106. Phosphorus Phosphorus is predominantly absorbed as inorganic phosphate in the upper small intestine. Phosphate is transported
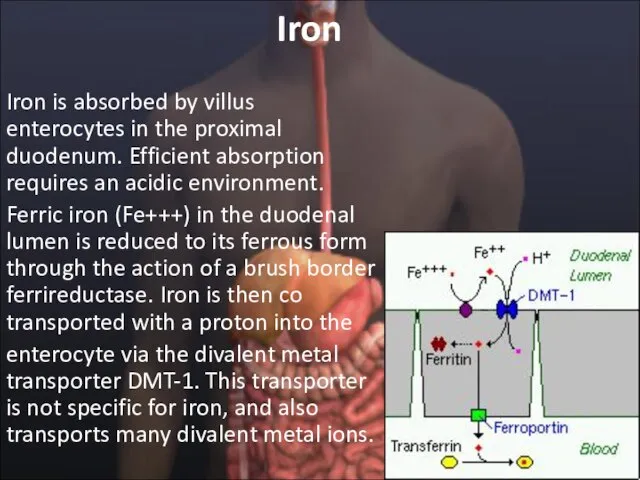
- 107. Iron Iron is absorbed by villus enterocytes in the proximal duodenum. Efficient absorption requires an acidic
- 108. Iron Once inside the enterocyte, iron follows one of two major pathways: • Iron abundance states:
- 109. Copper There appear to be two processes responsible for copper absorption: i) a rapid, low capacity
- 110. Zinc Zinc homeostasis is largely regulated by its uptake and loss through the small intestine. Although
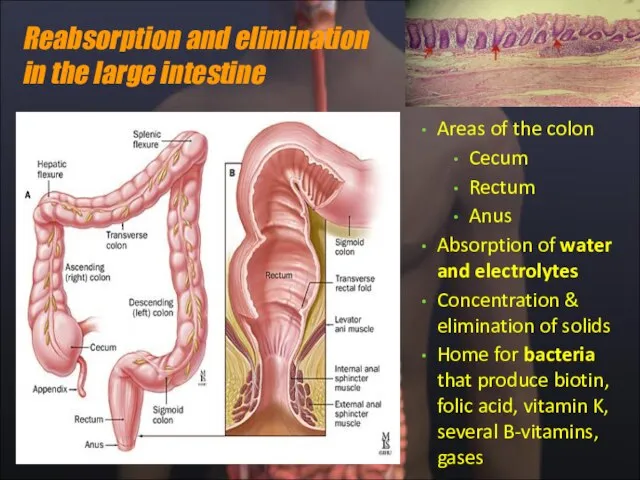
- 114. Reabsorption and elimination in the large intestine Areas of the colon Cecum Rectum Anus Absorption of
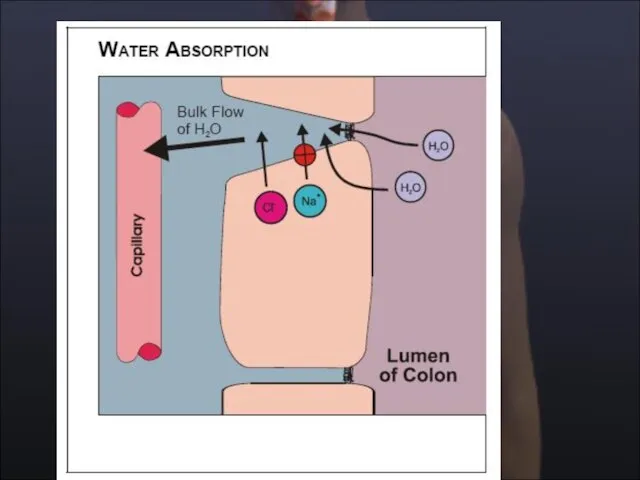
- 115. The Large Intestine: Introduction Recovery of water and electrolytes from ingesta: By the time ingesta reaches
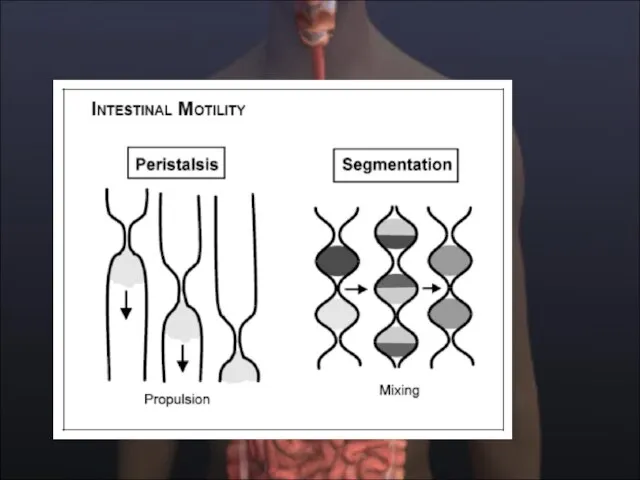
- 116. Large Intestinal Motility Segmentation contractions which chop and mix the ingesta, presenting it to the mucosa
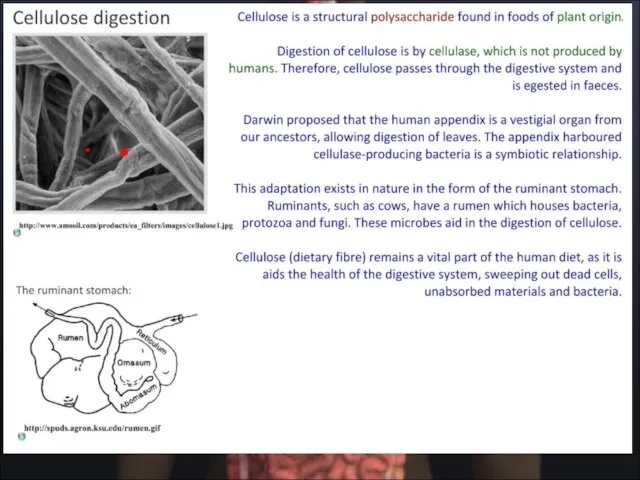
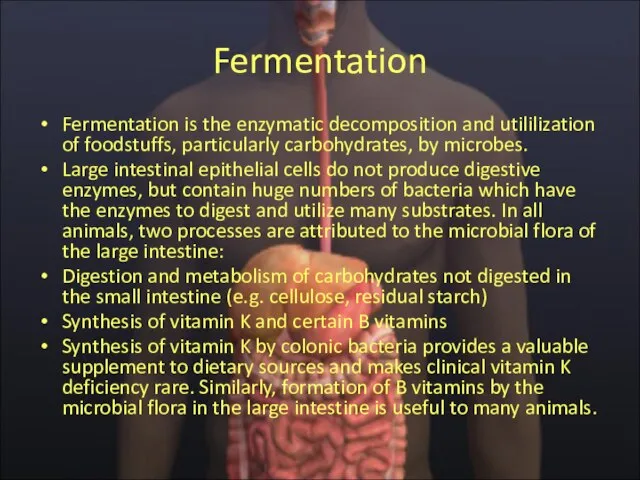
- 117. Fermentation Fermentation is the enzymatic decomposition and utililization of foodstuffs, particularly carbohydrates, by microbes. Large intestinal
- 119. Скачать презентацию
Слайд 4Пищеварение: физиологические процессы
Пищеварение: физиологические процессы
Слайд 6Sites of digestion
Sites of digestion
Слайд 7Salivary glands
Produce saliva
Mostly water
Some enzymes
Salivary amylase
Lysozyme
Mucus or mucin
Teeth
Digestion in the Mouth
Salivary glands
Produce saliva
Mostly water
Some enzymes
Salivary amylase
Lysozyme
Mucus or mucin
Teeth
Digestion in the Mouth
Слайд 8Функции слюны
ˆ увлажняет пищу, облегчает глотание,
ˆпредупреждает аспирацию пищи в трахею, способствуя
Функции слюны
ˆ увлажняет пищу, облегчает глотание,
ˆпредупреждает аспирацию пищи в трахею, способствуя
Слайд 10Образование слюны
Образование слюны
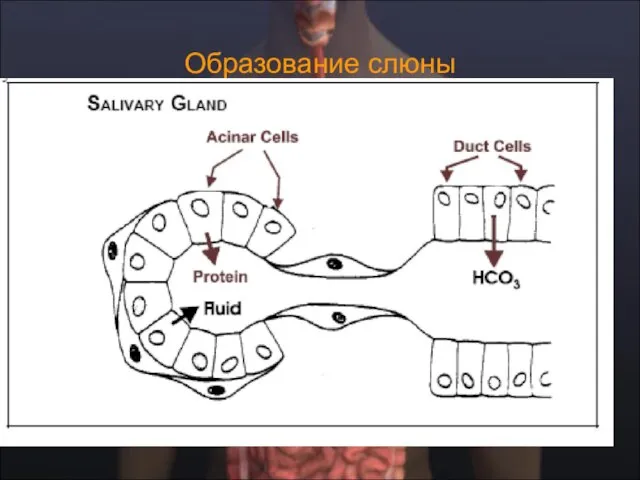
Слайд 11Функция протоков слюнных желез
Функция протоков слюнных желез

Слайд 13Takehito Etani, Masticator triptych, 2005.
Takehito Etani, Masticator triptych, 2005.
Слайд 14Mastication. masticatory cycle (chewing cycle) the complete pathway of the mandible
Mastication. masticatory cycle (chewing cycle) the complete pathway of the mandible
Слайд 15Mastication
Mastication
Слайд 16The Muscles of Mastication (Chewing)
Перетирание или жевание, выполняется скоординированной функцией четырех важных
The Muscles of Mastication (Chewing)
Перетирание или жевание, выполняется скоординированной функцией четырех важных
Слайд 17Main force vectors of masticatory muscles
Main force vectors of masticatory muscles
Слайд 18Swallowing: from mouth to stomach
The Oral Phase
The Pharyngeal Phase
The Esophageal Phase
Swallowing: from mouth to stomach
The Oral Phase
The Pharyngeal Phase
The Esophageal Phase
Слайд 19Oral Preparatory Stage
Ротовая предварительная стадия по существу жевание. Это включает координацию губ,
Oral Preparatory Stage
Ротовая предварительная стадия по существу жевание. Это включает координацию губ,
Слайд 20Oral Stage
Ротовая стадия - вторая стадия глотания. Это длится приблизительно 1 секунду,
Oral Stage
Ротовая стадия - вторая стадия глотания. Это длится приблизительно 1 секунду,
Слайд 21Pharyngeal Stage
The pharyngeal stage begins when the bolus reaches the anterior faucial
Pharyngeal Stage
The pharyngeal stage begins when the bolus reaches the anterior faucial
Слайд 22Swallowing Reflex (Pharyngeal Stage)
When triggered, the swallowing reflex results in four neuromuscular
Swallowing Reflex (Pharyngeal Stage)
When triggered, the swallowing reflex results in four neuromuscular
Слайд 23Laryngeal closure occurs at three sphincters:
1) the epiglottis and aryepiglottic folds,
2) the
Laryngeal closure occurs at three sphincters:
1) the epiglottis and aryepiglottic folds,
2) the
Слайд 24Pharyngoesophageal segment opening depends on:
1) relaxation of the cricopharyngeus,
2) the upward, anterior
Pharyngoesophageal segment opening depends on:
1) relaxation of the cricopharyngeus,
2) the upward, anterior
Слайд 25Esophageal Stage
The fourth and final stage of swallowing is the esophageal stage.
Esophageal Stage
The fourth and final stage of swallowing is the esophageal stage.
Слайд 26Swallowing Centers
In humans, the development of
functional magnetic resonance imaging (fMRI) has allowed
Swallowing Centers
In humans, the development of
functional magnetic resonance imaging (fMRI) has allowed
Слайд 27Swallowing Centers
There is convincing evidence that the sequential and rhythmic patterns of
Swallowing Centers
There is convincing evidence that the sequential and rhythmic patterns of
Слайд 28Swallowing Centers
The voluntary initiation of swallowing takes place in special brain areas
Swallowing Centers
The voluntary initiation of swallowing takes place in special brain areas
Слайд 31Моторика пищевода
Food is propelled down the esophagus by coordinated contractions of the
Моторика пищевода
Food is propelled down the esophagus by coordinated contractions of the
Слайд 32Пищеварение в желудке
Пищеварение в желудке

Слайд 33Muscular sac
Churns & mixes food
Gastric glands
Parietal cells ? HCl, intrinsic factor
Goblet cells
Muscular sac
Churns & mixes food
Gastric glands
Parietal cells ? HCl, intrinsic factor
Goblet cells
Слайд 34Функции желудка
ˆ
Serves as a reservoir that allows for the ingestion of
Функции желудка
ˆ
Serves as a reservoir that allows for the ingestion of
Слайд 35Секреция в желудке
Секреция в желудке
The major components of gastric juice
Секреция в желудке
Секреция в желудке
The major components of gastric juice
Слайд 37Механизм секреции НСL
Механизм секреции НСL
Слайд 38 Регуляция секреции HCL
Регуляция секреции HCL
Слайд 39Потенциация секреции HCL
Потенциация секреции HCL
Слайд 40Activation of pepsin in the stomach
Activation of pepsin in the stomach
Слайд 41Секреция пепсиногена: активация
Секреция пепсиногена: активация
Слайд 42Секреция слизи в желудке: типы слизи
Секреция слизи в желудке: типы слизи
Секреция слизи в желудке: типы слизи
Секреция слизи в желудке: типы слизи
Слайд 43A second type of mucous, soluble mucous, is secreted along with the
A second type of mucous, soluble mucous, is secreted along with the
Слайд 44Регуляция секреции в желудке
Регуляция секреции в желудке
Регуляция секреции в желудке
Регуляция секреции в желудке
Слайд 45Регуляция секреции HCL
Регуляция секреции HCL
Слайд 46Фазы желудочной секреции
Аnticipation of a meal, or the sight of food
Фазы желудочной секреции
Аnticipation of a meal, or the sight of food
Слайд 49Моторика желудка: перемешивание, эвакуация
Моторика желудка: перемешивание, эвакуация
Моторика желудка: перемешивание, эвакуация
Моторика желудка: перемешивание, эвакуация
Слайд 50Эвакуация: факторы регуляции
The chyme coming from the stomach is normally hypertonic,
Эвакуация: факторы регуляции
The chyme coming from the stomach is normally hypertonic,
Слайд 51Состав химуса
Состав химуса
Слайд 52Эвакуация: роль Н ионов
Эвакуация: роль Н ионов
Слайд 53Регуляция эвакуации химуса
Регуляция эвакуации химуса
Слайд 54Exocrine function
Acinar cells secrete pancreatic juice
Amylase
Lipase
Trypsin
Chymotrypsin
Carboxypeptidase
Nuclease
NaHCO3-
Secretin and cholecystokinin (CCK) fr intestinal wall
Exocrine function
Acinar cells secrete pancreatic juice
Amylase
Lipase
Trypsin
Chymotrypsin
Carboxypeptidase
Nuclease
NaHCO3-
Secretin and cholecystokinin (CCK) fr intestinal wall
Слайд 55Activation of pancreatic zymogens in the
small intestine by brush-border enzymes.
The brushborder
enzyme enterokinase
Activation of pancreatic zymogens in the
small intestine by brush-border enzymes.
The brushborder
enzyme enterokinase
Слайд 56Активация ферментов
Активация ферментов
Слайд 58Пищеварение в duodenum
Пищеварение в duodenum
Слайд 59Расщепление углеводов
Расщепление углеводов
Слайд 60Расщепление белков
Расщепление белков
Слайд 61Панкреатическая секреция
Панкреатическая секреция
Слайд 62Регуляция панкреатической секреции
Регуляция панкреатической секреции
Слайд 63Секреция бикарбоната
Секреция бикарбоната
Слайд 65Emulsification and digestion of fat in the
small intestine.
Emulsification and digestion of fat in the
small intestine.
Слайд 66Пищеварение и всасывание углеводов и белков
Пищеварение и всасывание углеводов и белков
Пищеварение и всасывание углеводов и белков
Пищеварение и всасывание углеводов и белков

Слайд 75Всасывание веществ в пищеварительном тракте
Всасывание веществ в пищеварительном тракте
Слайд 77Overview of carbohydrate digestion.
Overview of carbohydrate digestion.
Слайд 79Overview of carbohydrate digestion.
Na_-dependent and facilitative transporters in the intestinal epithelial cells.
Overview of carbohydrate digestion.
Na_-dependent and facilitative transporters in the intestinal epithelial cells.
Слайд 80Overview of carbohydrate digestion.
Overview of carbohydrate digestion.
Слайд 81Properties of the GLUT 1-GLUT 5 Isoforms of the Glucose Transport Proteins
Properties of the GLUT 1-GLUT 5 Isoforms of the Glucose Transport Proteins
Слайд 82CLINICAL CORRELATION
Disaccharidase Deficiency Intestinal disaccharidase deficiencies are encountered relatively frequently in
CLINICAL CORRELATION
Disaccharidase Deficiency Intestinal disaccharidase deficiencies are encountered relatively frequently in
Слайд 84Absorption of Amino Acids
Absorption of Amino Acids
Слайд 86CLINICAL CORRELATION
Neutral Amino Aciduria (Hartnup Disease)
Transport functions, like enzymatic functions, are
CLINICAL CORRELATION
Neutral Amino Aciduria (Hartnup Disease)
Transport functions, like enzymatic functions, are
Слайд 87Kwashiorkor
Kwashiorkor, A common problem of children in Third World countries, is caused
Kwashiorkor
Kwashiorkor, A common problem of children in Third World countries, is caused
Слайд 88Расщепление жиров
Расщепление жиров
Слайд 89Liver
Secretes bile
(stored in gall bladder)
Emulsifies fats
Gallbladder
Stores, concentrates, and releases bile into
Liver
Secretes bile
(stored in gall bladder)
Emulsifies fats
Gallbladder
Stores, concentrates, and releases bile into
Слайд 92Digestion of triacylglycerols in the intestinal lumen. TG _ triacylglycerol; bs _
Digestion of triacylglycerols in the intestinal lumen. TG _ triacylglycerol; bs _
Слайд 93Digestion and absorption of lipids
Digestion and absorption of lipids
Слайд 94Changes in physical state during triacylglycerol digestion. Abbreviations: TG, triacylglycerol; DG, diacylglycerol;
Changes in physical state during triacylglycerol digestion. Abbreviations: TG, triacylglycerol; DG, diacylglycerol;
Слайд 101CLINICAL CORRELATION
A-β-Lipoproteinemia
A-b-lipoproteinemia is an autosomal recessive disorder characterized by the
CLINICAL CORRELATION
A-β-Lipoproteinemia
A-b-lipoproteinemia is an autosomal recessive disorder characterized by the
Слайд 102Absorption in the small intestine
Absorption in the small intestine
Слайд 103Absorption of Minerals and Metals
Calcium
Active, transcellular absorption occurs only in
Absorption of Minerals and Metals
Calcium
Active, transcellular absorption occurs only in
Слайд 105Calcium
Passive, paracellular absorption occurs in the jejunum and ileum, and, to
Calcium
Passive, paracellular absorption occurs in the jejunum and ileum, and, to
Слайд 106Phosphorus
Phosphorus is predominantly absorbed as inorganic phosphate in the upper small
Phosphorus
Phosphorus is predominantly absorbed as inorganic phosphate in the upper small
Слайд 107Iron
Iron is absorbed by villus enterocytes in the proximal duodenum. Efficient
Iron
Iron is absorbed by villus enterocytes in the proximal duodenum. Efficient
Слайд 108Iron
Once inside the enterocyte, iron follows one of two major pathways:
•
Iron
Once inside the enterocyte, iron follows one of two major pathways:
•
Слайд 109Copper
There appear to be two processes responsible for copper absorption:
i)
Copper
There appear to be two processes responsible for copper absorption:
i)
Слайд 110Zinc
Zinc homeostasis is largely regulated by its uptake and loss through
Zinc
Zinc homeostasis is largely regulated by its uptake and loss through
Слайд 114Reabsorption and elimination in the large intestine
Areas of the colon
Cecum
Rectum
Anus
Absorption
Reabsorption and elimination in the large intestine
Areas of the colon
Cecum
Rectum
Anus
Absorption
Слайд 115The Large Intestine: Introduction
Recovery of water and electrolytes from ingesta: By
The Large Intestine: Introduction
Recovery of water and electrolytes from ingesta: By
Слайд 116Large Intestinal Motility
Segmentation contractions which chop and mix the ingesta, presenting it
Large Intestinal Motility
Segmentation contractions which chop and mix the ingesta, presenting it
Слайд 117Fermentation
Fermentation is the enzymatic decomposition and utililization of foodstuffs, particularly carbohydrates, by
Fermentation
Fermentation is the enzymatic decomposition and utililization of foodstuffs, particularly carbohydrates, by
 Как подготовить конспект урока
Как подготовить конспект урока ОГБОУНПОПрофессиональное училище №12.
ОГБОУНПОПрофессиональное училище №12. Многожанровость музыкального искусства
Многожанровость музыкального искусства Организация трансграничного электронного документооборота на основе доверенной третьей стороны
Организация трансграничного электронного документооборота на основе доверенной третьей стороны Антинея
Антинея Мониторинг гражданского обществав Российской Федерации
Мониторинг гражданского обществав Российской Федерации Арктические тундры
Арктические тундры Презентация на тему Знаки препинания при вводных словах и предложениях
Презентация на тему Знаки препинания при вводных словах и предложениях История полиции в Новониколаевске
История полиции в Новониколаевске Физики и деньги
Физики и деньги Кроссплатформенное СПО как альтернатива проприетарному
Кроссплатформенное СПО как альтернатива проприетарному Пасхальный калейдоскоп
Пасхальный калейдоскоп Презентация
Презентация Правописание частицы НЕ с разным частями речи
Правописание частицы НЕ с разным частями речи Мощные производители из наиболее развитых провинций - Цзянсу
Мощные производители из наиболее развитых провинций - Цзянсу Горы России 4 КЛАСС
Горы России 4 КЛАСС Советская музыка
Советская музыка Школьный этап конкурса «Учитель года -2010»
Школьный этап конкурса «Учитель года -2010» Презентация на тему Скорость сближения и удаления
Презентация на тему Скорость сближения и удаления Цели внедрения системы бюджетирования
Цели внедрения системы бюджетирования Презентация на тему Отряд Подёнки
Презентация на тему Отряд Подёнки Повторение темы «Наречие».
Повторение темы «Наречие». Миф о Персее. Созвездия Цефея, Кассиопеи, Персея, Андромеды и Пегаса.
Миф о Персее. Созвездия Цефея, Кассиопеи, Персея, Андромеды и Пегаса. Звуковые колебания
Звуковые колебания Не умри, и мы отстанем
Не умри, и мы отстанем Презентация на тему Международные отношения в 1920-30-е годы
Презентация на тему Международные отношения в 1920-30-е годы  Художественный стиль:
Художественный стиль: Программа курса по выбору «Основы уголовного права».
Программа курса по выбору «Основы уголовного права».