- Independent work

Содержание
- 2. Crohn’s Disease Aim of this module To increase the understanding of Crohn’s disease by looking at
- 3. How to use this module This module is designed by a student for students. The data
- 4. Epidemiology & Pathology of Crohn’s Disease
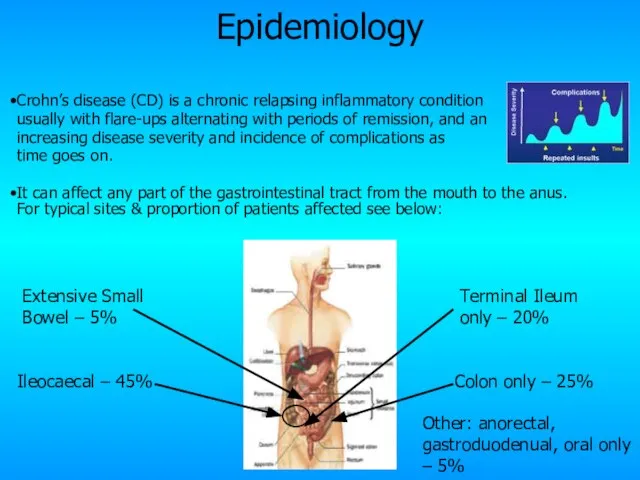
- 5. Crohn’s disease (CD) is a chronic relapsing inflammatory condition usually with flare-ups alternating with periods of
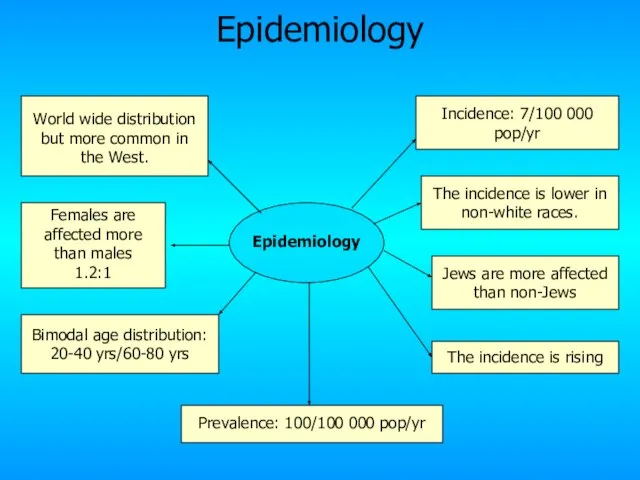
- 6. Epidemiology Incidence: 7/100 000 pop/yr Prevalence: 100/100 000 pop/yr World wide distribution but more common in
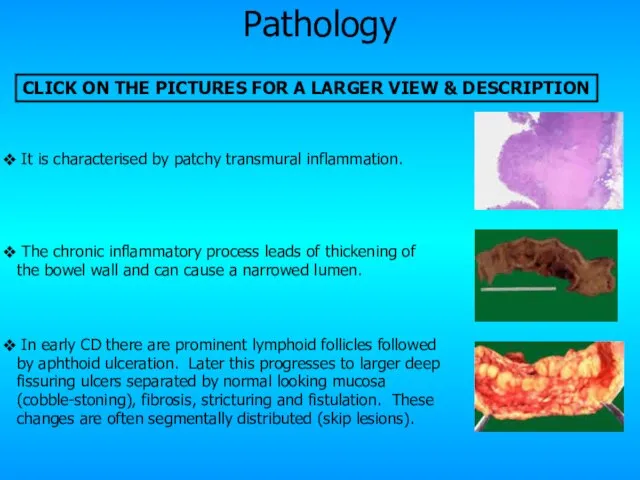
- 7. Pathology It is characterised by patchy transmural inflammation. The chronic inflammatory process leads of thickening of
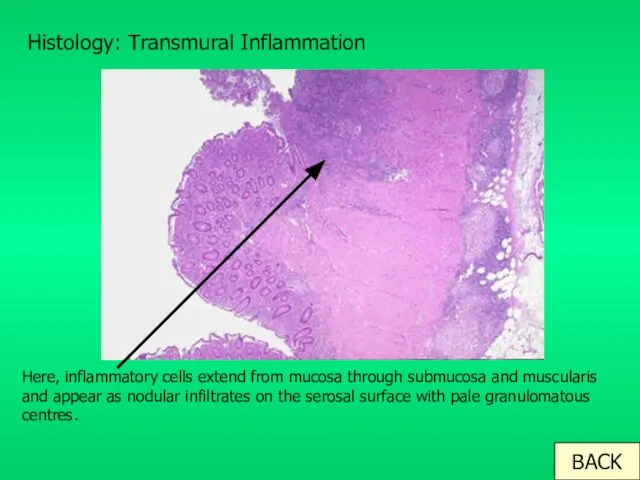
- 8. Histology: Transmural Inflammation Here, inflammatory cells extend from mucosa through submucosa and muscularis and appear as
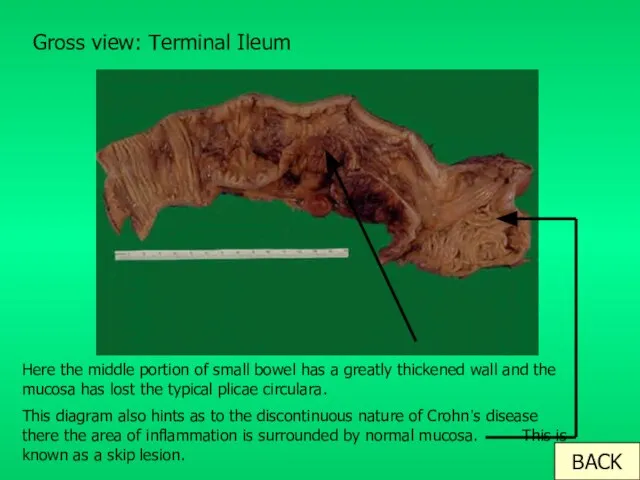
- 9. Gross view: Terminal Ileum Here the middle portion of small bowel has a greatly thickened wall
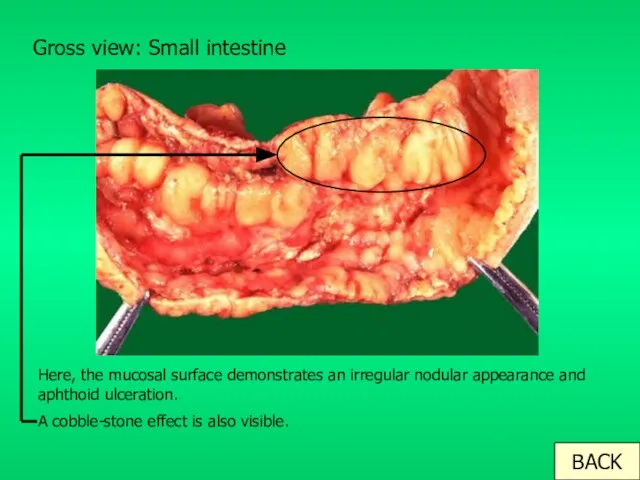
- 10. Gross view: Small intestine Here, the mucosal surface demonstrates an irregular nodular appearance and aphthoid ulceration.
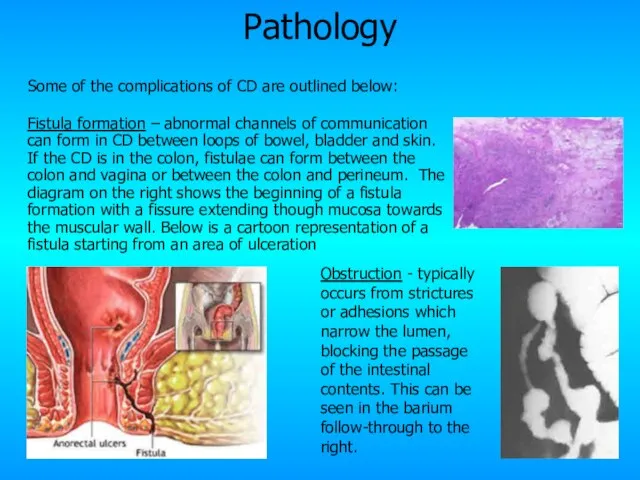
- 11. Pathology Some of the complications of CD are outlined below: Fistula formation – abnormal channels of
- 12. Aetiology and Pathogenesis of Crohn’s Disease
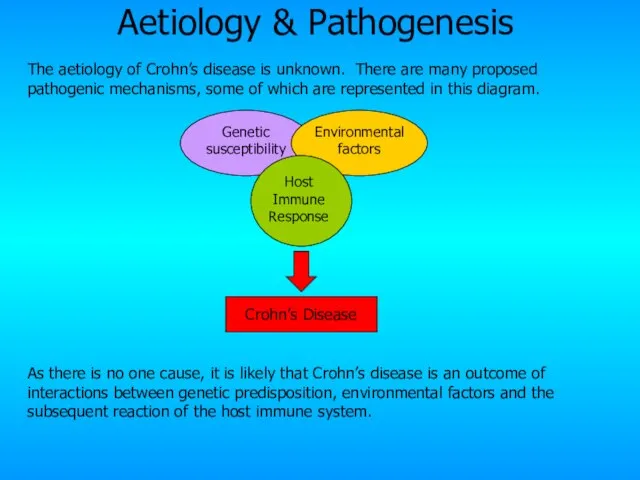
- 13. Aetiology & Pathogenesis The aetiology of Crohn’s disease is unknown. There are many proposed pathogenic mechanisms,
- 14. Genetic Factors There are 3 mutations on the CARD15 gene on Chromosome 16 that are associated
- 15. Environmental Factors A wide range of environmental factors have been found to play a role: Smoking
- 16. Immune response Host Immune Response Both the potential genetics underlying CD and the environmental and host
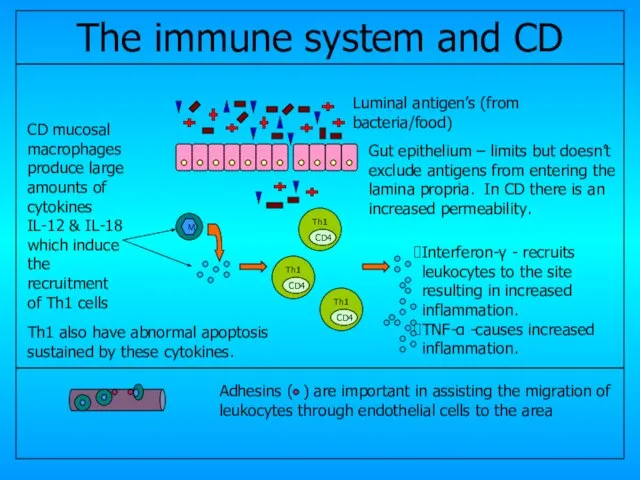
- 17. CD4 CD4 CD4 Gut epithelium – limits but doesn’t exclude antigens from entering the lamina propria.
- 18. Clinical features of Crohn’s Disease
- 19. Clinical Features The clinical presentation can be very variable depending upon the site and predominant pathology
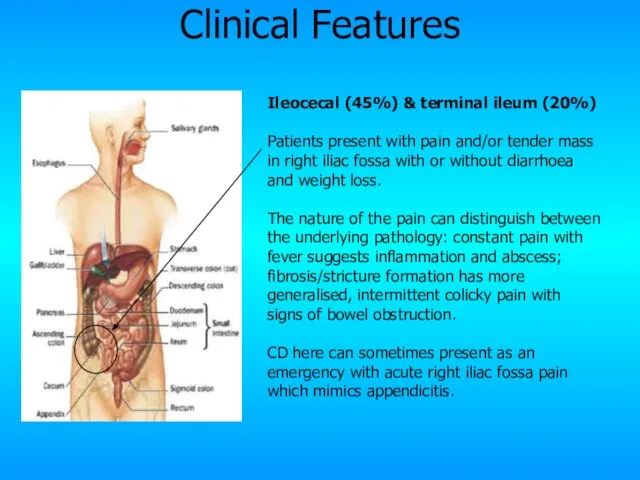
- 20. Ileocecal (45%) & terminal ileum (20%) Patients present with pain and/or tender mass in right iliac
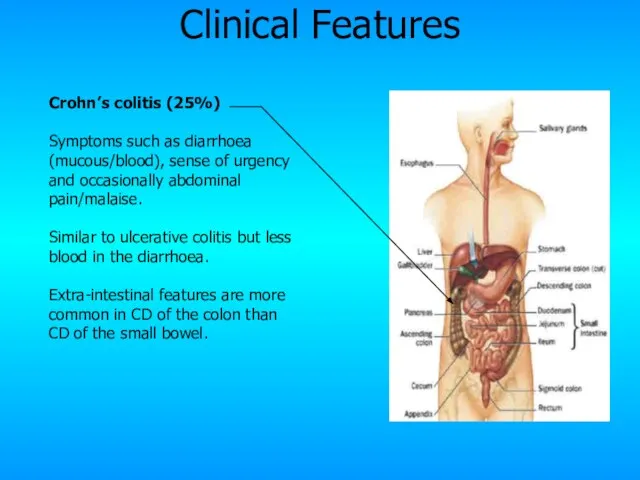
- 21. Crohn’s colitis (25%) Symptoms such as diarrhoea (mucous/blood), sense of urgency and occasionally abdominal pain/malaise. Similar
- 22. Gastroduodenal & oral (5%) Very rare. The former presents with upper abdominal pain or dyspepsia with
- 23. Extensive small bowel (5%) Presents with typical pain, diarrhoea and weight loss in addition to features
- 24. Perianal CD – complication Characterised by perianal pain and/or discharge. It’s due to fistula, fissure or
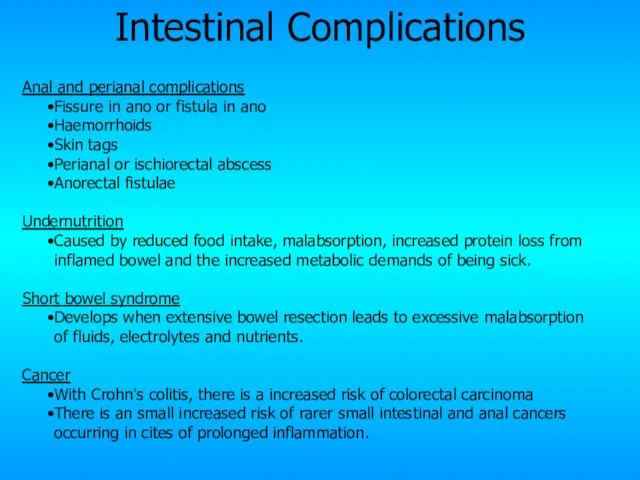
- 25. Intestinal Complications Anal and perianal complications Fissure in ano or fistula in ano Haemorrhoids Skin tags
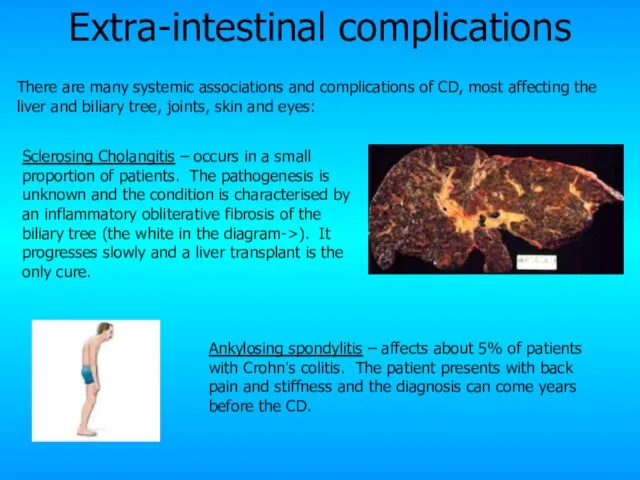
- 26. Extra-intestinal complications Sclerosing Cholangitis – occurs in a small proportion of patients. The pathogenesis is unknown
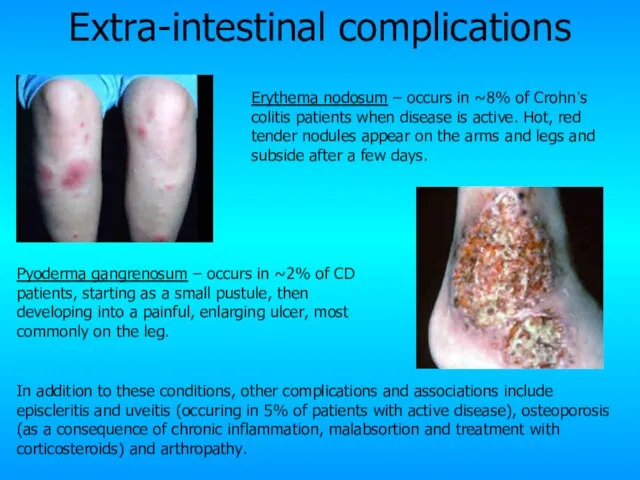
- 27. Extra-intestinal complications Pyoderma gangrenosum – occurs in ~2% of CD patients, starting as a small pustule,
- 28. Diagnosis and Management of Crohn’s Disease
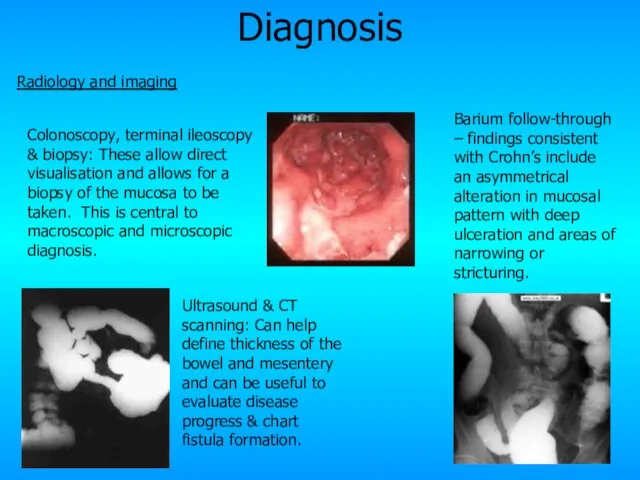
- 29. Diagnosis Radiology and imaging Ultrasound & CT scanning: Can help define thickness of the bowel and
- 30. Diagnosis Blood tests Haematology: results suggesting anaemia, ? platelet count & ? ESR suggests an inflammatory
- 31. Differential Diagnosis There are many differential diagnosis for Crohn’s disease, complicated further by the differing presentations
- 32. Management Management is best if a MDT approach is adopted, including physicians, surgeons, specialist nurses, dieticians
- 33. Medical management Dietary advice and nutritional support including vitamin supplementation to counter-act any deficiencies that develop.
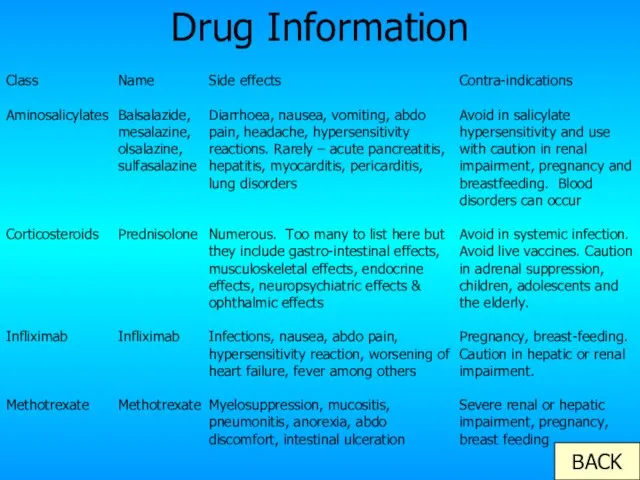
- 34. Drug Information BACK Class Aminosalicylates Corticosteroids Infliximab Methotrexate Name Balsalazide, mesalazine, olsalazine, sulfasalazine Prednisolone Infliximab Methotrexate
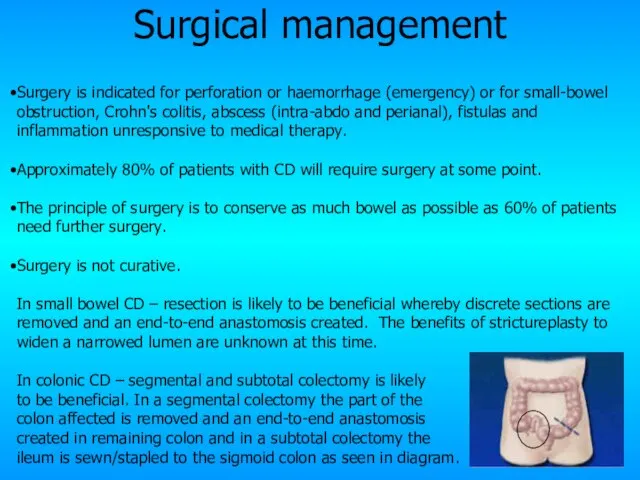
- 35. Surgical management Surgery is indicated for perforation or haemorrhage (emergency) or for small-bowel obstruction, Crohn's colitis,
- 36. Prognosis Mortality The cumulative mortality is approximately twice that of the general population. Death is primarily
- 37. Summary Crohn’s disease is a chronic inflammatory condition of the gastrointestinal tract characterised by transmural inflammation,
- 38. The different sections If you want to revisit any of the sections of this module please
- 39. Case Study 30-year-old woman was admitted with a 4-week history of increasing bloody diarrhoea and abdominal
- 40. Case Study The rectal biopsy taken at sigmoidoscopy showed a small area of ulceration of the
- 41. Thank you I hope this has been of some help to your studies!
- 43. Скачать презентацию
Слайд 3How to use this module
This module is designed by a student for
How to use this module
This module is designed by a student for
Слайд 4Epidemiology & Pathology
of Crohn’s Disease
Epidemiology & Pathology
of Crohn’s Disease
Слайд 5Crohn’s disease (CD) is a chronic relapsing inflammatory condition
usually with flare-ups
Crohn’s disease (CD) is a chronic relapsing inflammatory condition
usually with flare-ups
Слайд 6Epidemiology
Incidence: 7/100 000 pop/yr
Prevalence: 100/100 000 pop/yr
World wide distribution but more common
Epidemiology
Incidence: 7/100 000 pop/yr
Prevalence: 100/100 000 pop/yr
World wide distribution but more common
Слайд 7Pathology
It is characterised by patchy transmural inflammation.
The chronic inflammatory process
Pathology
It is characterised by patchy transmural inflammation.
The chronic inflammatory process
Слайд 8Histology: Transmural Inflammation
Here, inflammatory cells extend from mucosa through submucosa and muscularis
Histology: Transmural Inflammation
Here, inflammatory cells extend from mucosa through submucosa and muscularis
Слайд 9Gross view: Terminal Ileum
Here the middle portion of small bowel has a
Gross view: Terminal Ileum
Here the middle portion of small bowel has a
Слайд 10Gross view: Small intestine
Here, the mucosal surface demonstrates an irregular nodular appearance
Gross view: Small intestine
Here, the mucosal surface demonstrates an irregular nodular appearance
Слайд 11Pathology
Some of the complications of CD are outlined below:
Fistula formation – abnormal
Pathology
Some of the complications of CD are outlined below:
Fistula formation – abnormal
Слайд 12Aetiology and Pathogenesis of Crohn’s Disease
Aetiology and Pathogenesis of Crohn’s Disease
Слайд 13Aetiology & Pathogenesis
The aetiology of Crohn’s disease is unknown. There are many
Aetiology & Pathogenesis
The aetiology of Crohn’s disease is unknown. There are many
Слайд 14Genetic Factors
There are 3 mutations on the CARD15 gene on Chromosome 16
Genetic Factors
There are 3 mutations on the CARD15 gene on Chromosome 16
Слайд 15Environmental Factors
A wide range of environmental factors have been found to play
Environmental Factors
A wide range of environmental factors have been found to play
Слайд 16Immune response
Host
Immune
Response
Both the potential genetics underlying CD and the environmental and host
Immune response
Host
Immune
Response
Both the potential genetics underlying CD and the environmental and host
Слайд 17CD4
CD4
CD4
Gut epithelium – limits but doesn’t exclude antigens from entering the lamina
CD4
CD4
CD4
Gut epithelium – limits but doesn’t exclude antigens from entering the lamina
Слайд 18Clinical features of Crohn’s Disease
Clinical features of Crohn’s Disease
Слайд 19Clinical Features
The clinical presentation can be very variable depending upon the site
Clinical Features
The clinical presentation can be very variable depending upon the site
Слайд 20Ileocecal (45%) & terminal ileum (20%)
Patients present with pain and/or tender mass
Ileocecal (45%) & terminal ileum (20%)
Patients present with pain and/or tender mass
Слайд 21Crohn’s colitis (25%)
Symptoms such as diarrhoea (mucous/blood), sense of urgency and occasionally
Crohn’s colitis (25%)
Symptoms such as diarrhoea (mucous/blood), sense of urgency and occasionally
Слайд 22Gastroduodenal & oral (5%)
Very rare.
The former presents with upper abdominal pain
Gastroduodenal & oral (5%)
Very rare.
The former presents with upper abdominal pain
Слайд 23Extensive small bowel (5%)
Presents with typical pain, diarrhoea and weight loss in
Extensive small bowel (5%)
Presents with typical pain, diarrhoea and weight loss in
Слайд 24Perianal CD – complication
Characterised by perianal pain and/or discharge. It’s due to
Perianal CD – complication
Characterised by perianal pain and/or discharge. It’s due to
Слайд 25Intestinal Complications
Anal and perianal complications
Fissure in ano or fistula in ano
Haemorrhoids
Skin
Intestinal Complications
Anal and perianal complications
Fissure in ano or fistula in ano
Haemorrhoids
Skin
Слайд 26Extra-intestinal complications
Sclerosing Cholangitis – occurs in a small proportion of patients. The
Extra-intestinal complications
Sclerosing Cholangitis – occurs in a small proportion of patients. The
Слайд 27Extra-intestinal complications
Pyoderma gangrenosum – occurs in ~2% of CD patients, starting as
Extra-intestinal complications
Pyoderma gangrenosum – occurs in ~2% of CD patients, starting as
Слайд 28Diagnosis and Management of Crohn’s Disease
Diagnosis and Management of Crohn’s Disease
Слайд 29Diagnosis
Radiology and imaging
Ultrasound & CT scanning: Can help define thickness of the
Diagnosis
Radiology and imaging
Ultrasound & CT scanning: Can help define thickness of the
Слайд 30Diagnosis
Blood tests
Haematology: results suggesting anaemia, ? platelet count & ? ESR suggests
Diagnosis
Blood tests
Haematology: results suggesting anaemia, ? platelet count & ? ESR suggests
Слайд 31Differential Diagnosis
There are many differential diagnosis for Crohn’s disease, complicated further by
Differential Diagnosis
There are many differential diagnosis for Crohn’s disease, complicated further by
Слайд 32Management
Management is best if a MDT approach is adopted, including physicians, surgeons,
Management
Management is best if a MDT approach is adopted, including physicians, surgeons,
Слайд 33Medical management
Dietary advice and nutritional support including vitamin supplementation to counter-act any
Medical management
Dietary advice and nutritional support including vitamin supplementation to counter-act any
Слайд 34Drug Information
BACK
Class
Aminosalicylates
Corticosteroids
Infliximab
Methotrexate
Name
Balsalazide, mesalazine, olsalazine, sulfasalazine
Prednisolone
Infliximab
Methotrexate
Side effects
Diarrhoea, nausea, vomiting, abdo pain, headache, hypersensitivity
Drug Information
BACK
Class
Aminosalicylates
Corticosteroids
Infliximab
Methotrexate
Name
Balsalazide, mesalazine, olsalazine, sulfasalazine
Prednisolone
Infliximab
Methotrexate
Side effects
Diarrhoea, nausea, vomiting, abdo pain, headache, hypersensitivity
Слайд 35Surgical management
Surgery is indicated for perforation or haemorrhage (emergency) or for small-bowel
Surgical management
Surgery is indicated for perforation or haemorrhage (emergency) or for small-bowel
Слайд 36Prognosis
Mortality
The cumulative mortality is approximately twice that of the general population. Death
Prognosis
Mortality
The cumulative mortality is approximately twice that of the general population. Death
Слайд 37Summary
Crohn’s disease is a chronic inflammatory condition of the gastrointestinal tract characterised
Summary
Crohn’s disease is a chronic inflammatory condition of the gastrointestinal tract characterised
Слайд 38The different sections
If you want to revisit any of the sections of
The different sections
If you want to revisit any of the sections of
Слайд 39Case Study
30-year-old woman was admitted with a 4-week history of increasing bloody
Case Study
30-year-old woman was admitted with a 4-week history of increasing bloody
Слайд 40Case Study
The rectal biopsy taken at sigmoidoscopy showed a small area of
Case Study
The rectal biopsy taken at sigmoidoscopy showed a small area of
Слайд 41Thank you
I hope this has been of some help to your studies!
Thank you
I hope this has been of some help to your studies!
 Презентация на тему Ренессанс
Презентация на тему Ренессанс  Типы и структура уроков по ФГОС
Типы и структура уроков по ФГОС ГРИПОЛИКТИН
ГРИПОЛИКТИН Отрасль в системе национальной экономике
Отрасль в системе национальной экономике Лизинговые продукты
Лизинговые продукты Зайка из фетра. Мастер-класс
Зайка из фетра. Мастер-класс Практические приложения подобия треугольников
Практические приложения подобия треугольников Сочинение-описание "Лисица" 2 класс
Сочинение-описание "Лисица" 2 класс Суп-лапша на мясном бульоне
Суп-лапша на мясном бульоне Деятельность судов РФв представлениях россиян Результаты социологического исследования
Деятельность судов РФв представлениях россиян Результаты социологического исследования Печи и печная утварь XIX - начала XX веков
Печи и печная утварь XIX - начала XX веков Анализ корпоративного имиджа IKEA Выполнила Орлова Мария, 401 гр.
Анализ корпоративного имиджа IKEA Выполнила Орлова Мария, 401 гр. VITAL & ESSENTIAL ТРУДНОСТИ ПЕРЕВОДА
VITAL & ESSENTIAL ТРУДНОСТИ ПЕРЕВОДА Презентация на тему ,, ТЕРРОРЕСТИЧЕСКИЙ АКТ В Беслане,,. Подготовила ученица 4а класса Логинова Валерия.
Презентация на тему ,, ТЕРРОРЕСТИЧЕСКИЙ АКТ В Беслане,,. Подготовила ученица 4а класса Логинова Валерия. Формы бухгалтерского учета. Тема №11
Формы бухгалтерского учета. Тема №11 Избирательная система РФ
Избирательная система РФ отделения ГОДОВОЕ СОБРАНИЕ 2022
отделения ГОДОВОЕ СОБРАНИЕ 2022 Горячий этап холодно-горячей обкатки (ХГО) оборудования
Горячий этап холодно-горячей обкатки (ХГО) оборудования Автоматизация маршрута согласования и отражения в учете заявлений работников на замену выдачи молока денежной компенсацией
Автоматизация маршрута согласования и отражения в учете заявлений работников на замену выдачи молока денежной компенсацией «Многослойные и комбинированные пленочные материалы и изделия из них»
«Многослойные и комбинированные пленочные материалы и изделия из них» Окружающая среда маркетинга
Окружающая среда маркетинга Геродот
Геродот Устройство сверлильного станка. Приемы работы на сверлильном станке
Устройство сверлильного станка. Приемы работы на сверлильном станке Достопримечательности Омска
Достопримечательности Омска Кожа
Кожа Организация учебного кабинета английского языка
Организация учебного кабинета английского языка Что такое энергия?
Что такое энергия? Презентация на тему Потребность организма человека в кислороде. Строение органов дыхания
Презентация на тему Потребность организма человека в кислороде. Строение органов дыхания