- Masticatory Anatomy

Содержание
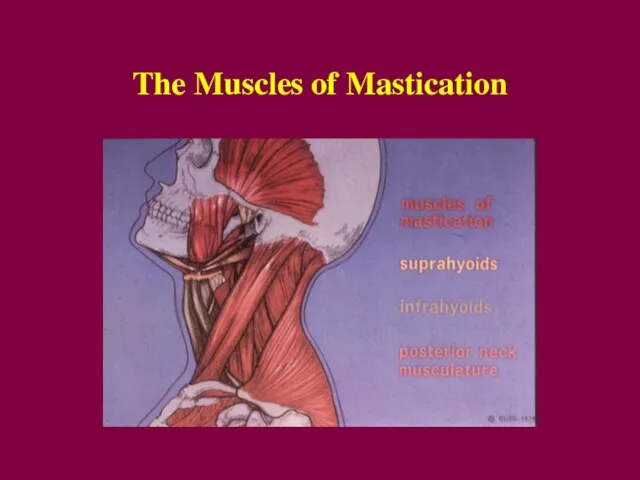
- 2. The Muscles of Mastication
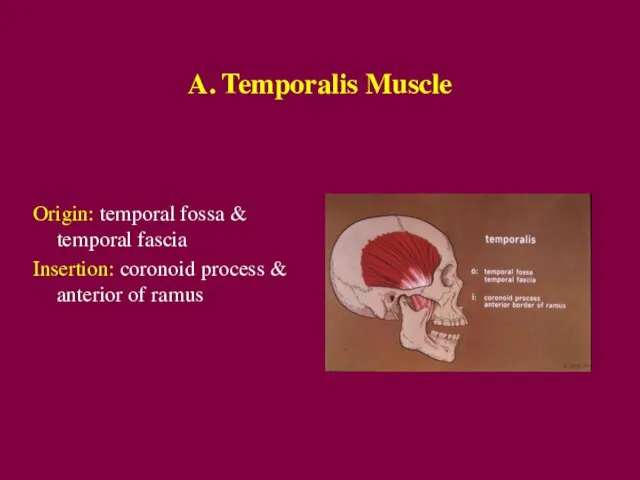
- 3. A. Temporalis Muscle Origin: temporal fossa & temporal fascia Insertion: coronoid process & anterior of ramus
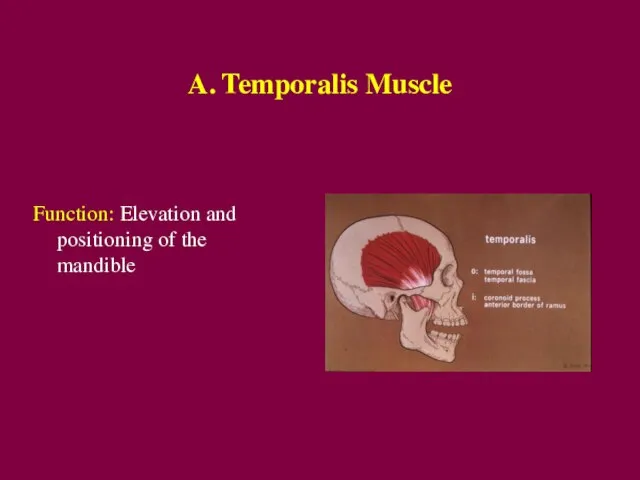
- 4. A. Temporalis Muscle Function: Elevation and positioning of the mandible
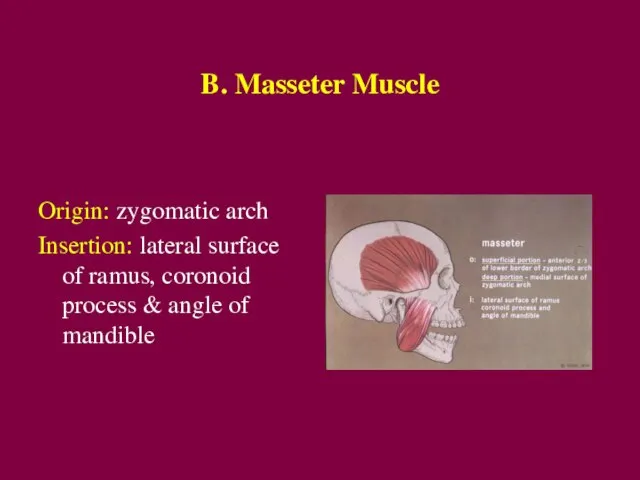
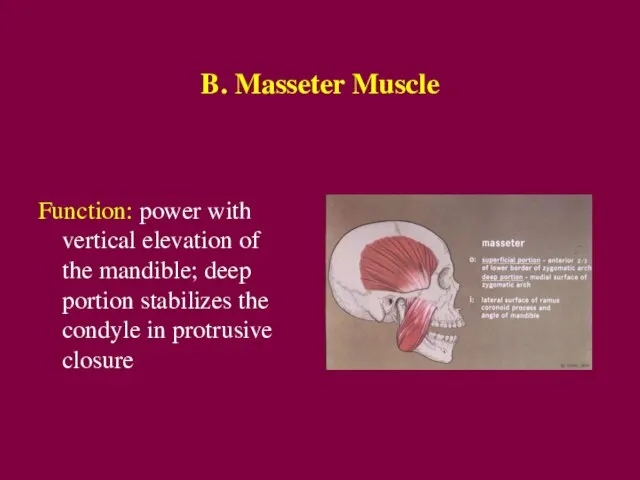
- 5. B. Masseter Muscle Origin: zygomatic arch Insertion: lateral surface of ramus, coronoid process & angle of
- 6. B. Masseter Muscle Function: power with vertical elevation of the mandible; deep portion stabilizes the condyle
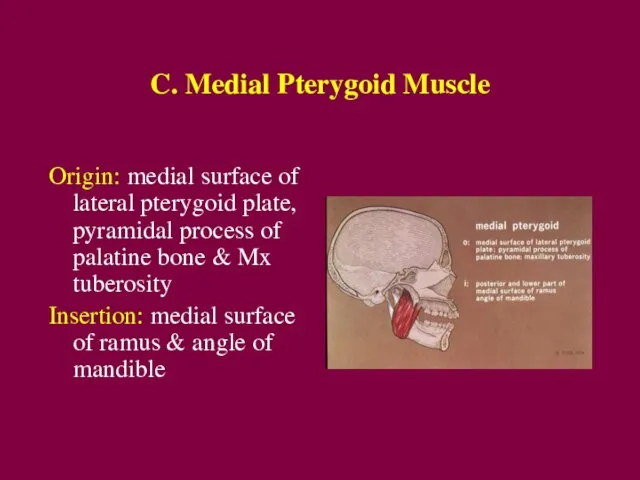
- 7. C. Medial Pterygoid Muscle Origin: medial surface of lateral pterygoid plate, pyramidal process of palatine bone
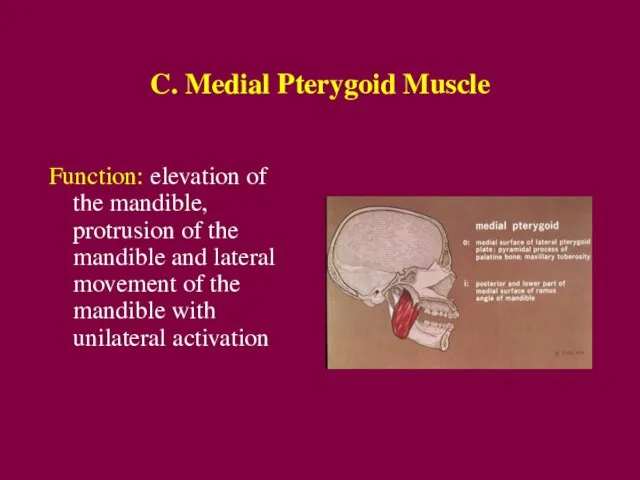
- 8. C. Medial Pterygoid Muscle Function: elevation of the mandible, protrusion of the mandible and lateral movement
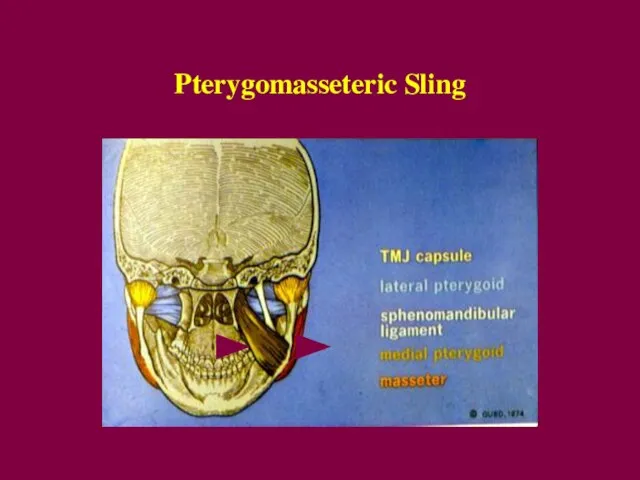
- 9. Pterygomasseteric Sling
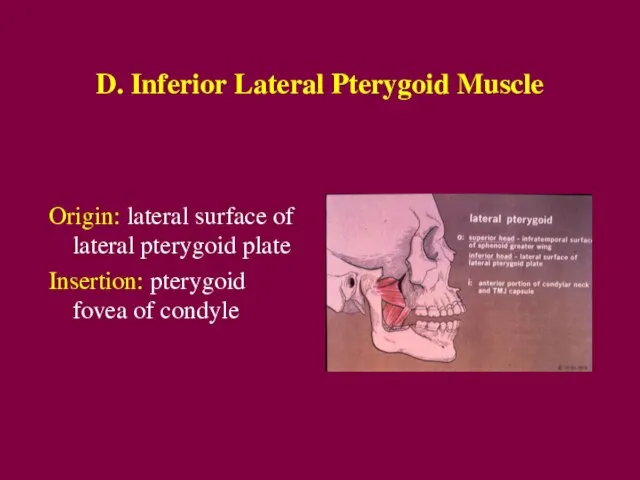
- 10. D. Inferior Lateral Pterygoid Muscle Origin: lateral surface of lateral pterygoid plate Insertion: pterygoid fovea of
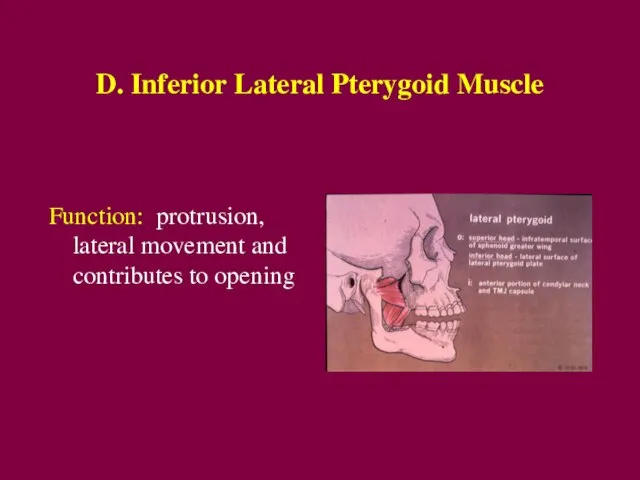
- 11. D. Inferior Lateral Pterygoid Muscle Function: protrusion, lateral movement and contributes to opening
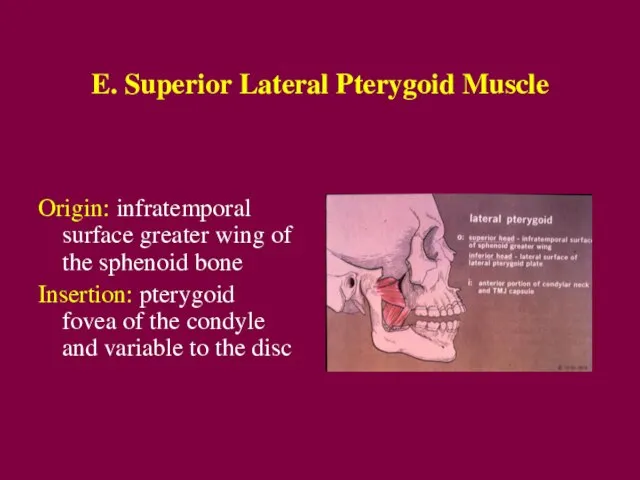
- 12. E. Superior Lateral Pterygoid Muscle Origin: infratemporal surface greater wing of the sphenoid bone Insertion: pterygoid
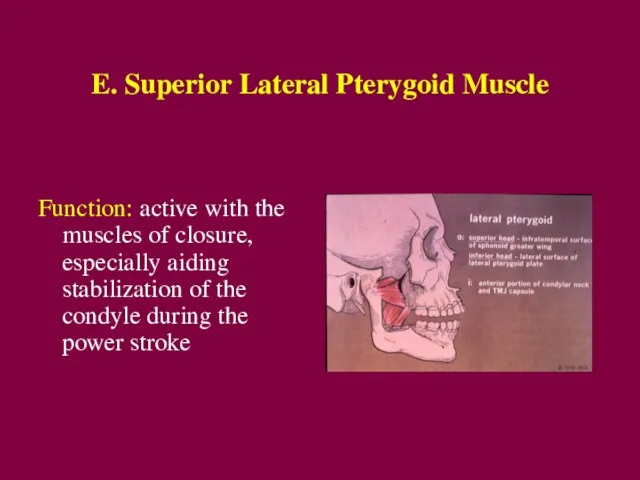
- 13. E. Superior Lateral Pterygoid Muscle Function: active with the muscles of closure, especially aiding stabilization of
- 14. Temporomandibular Joint Anatomy
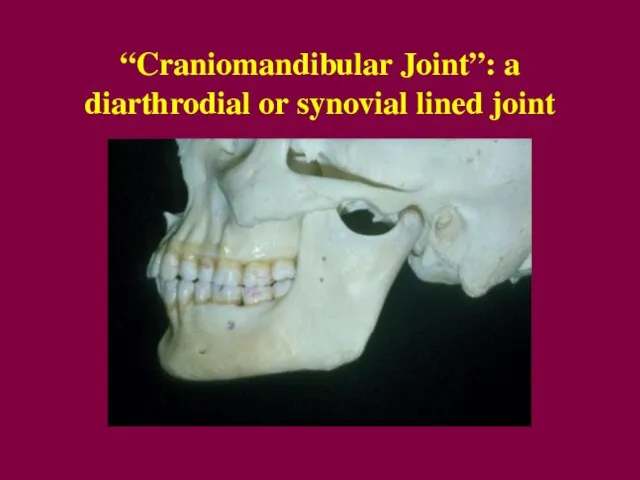
- 15. “Craniomandibular Joint”: a diarthrodial or synovial lined joint
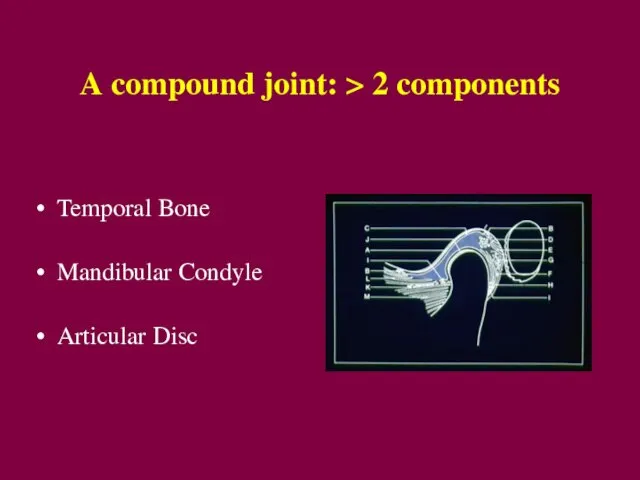
- 16. A compound joint: > 2 components Temporal Bone Mandibular Condyle Articular Disc
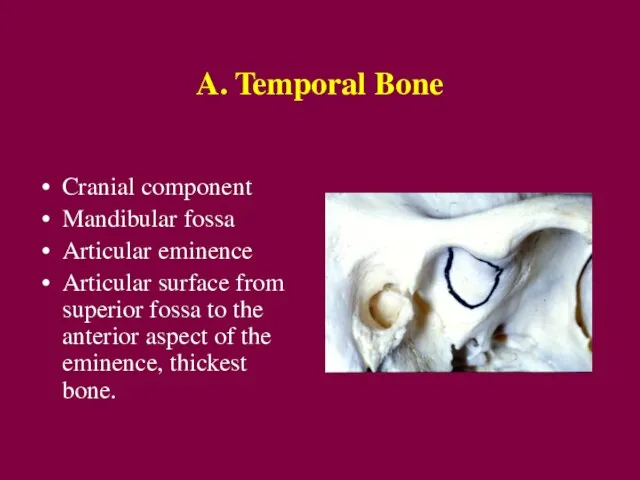
- 17. A. Temporal Bone Cranial component Mandibular fossa Articular eminence Articular surface from superior fossa to the
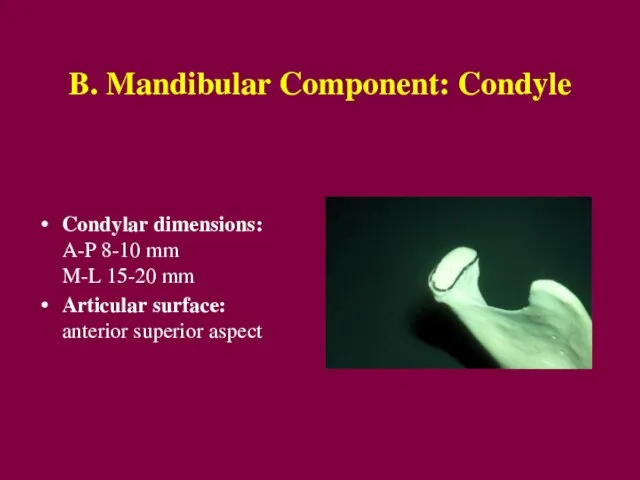
- 18. B. Mandibular Component: Condyle Condylar dimensions: A-P 8-10 mm M-L 15-20 mm Articular surface: anterior superior
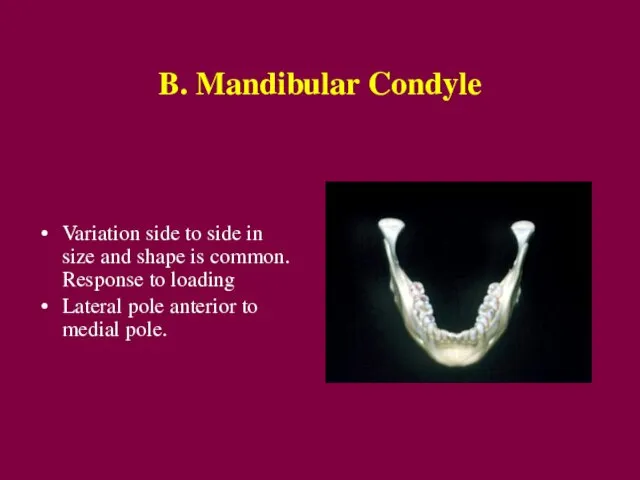
- 19. B. Mandibular Condyle Variation side to side in size and shape is common. Response to loading
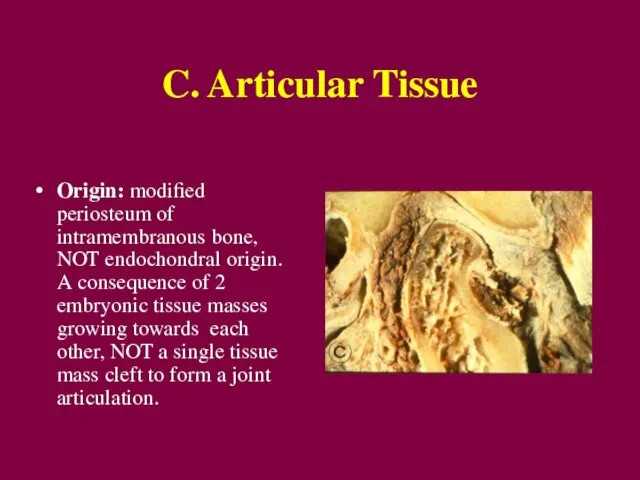
- 20. C. Articular Tissue Origin: modified periosteum of intramembranous bone, NOT endochondral origin. A consequence of 2
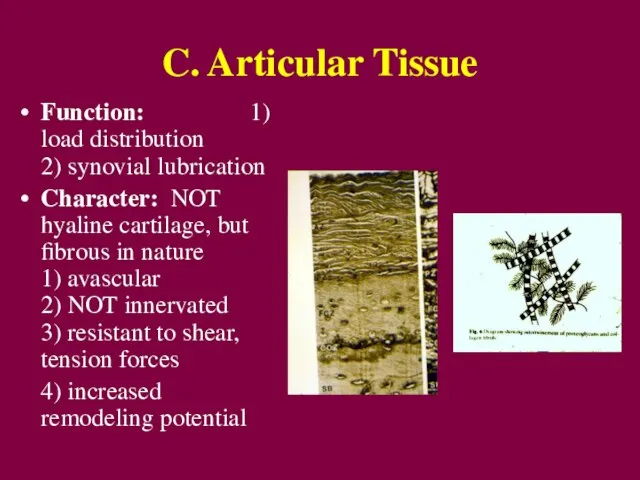
- 21. C. Articular Tissue Function: 1) load distribution 2) synovial lubrication Character: NOT hyaline cartilage, but fibrous
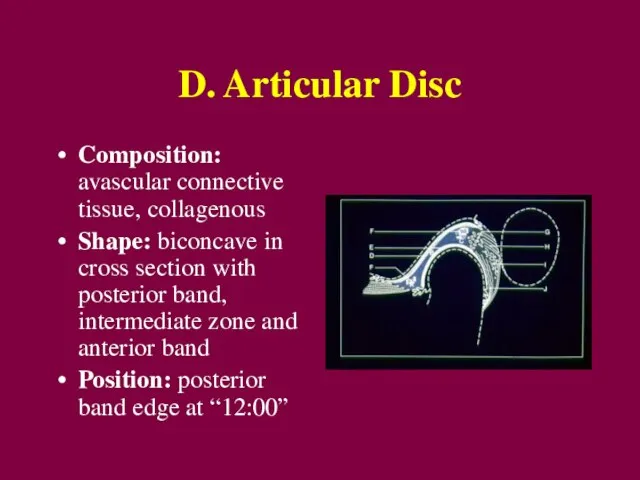
- 22. D. Articular Disc Composition: avascular connective tissue, collagenous Shape: biconcave in cross section with posterior band,
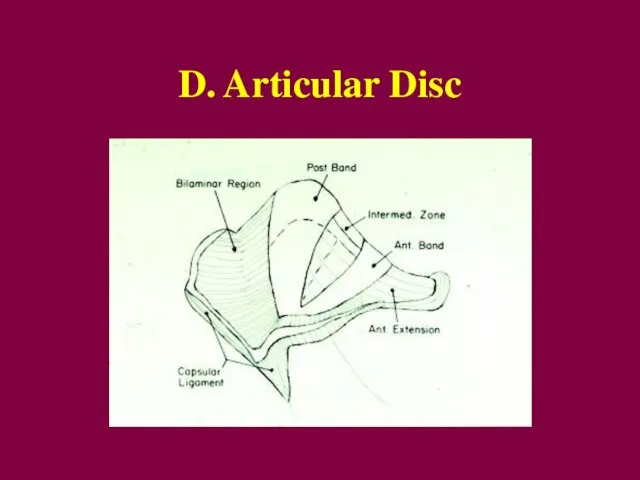
- 23. D. Articular Disc
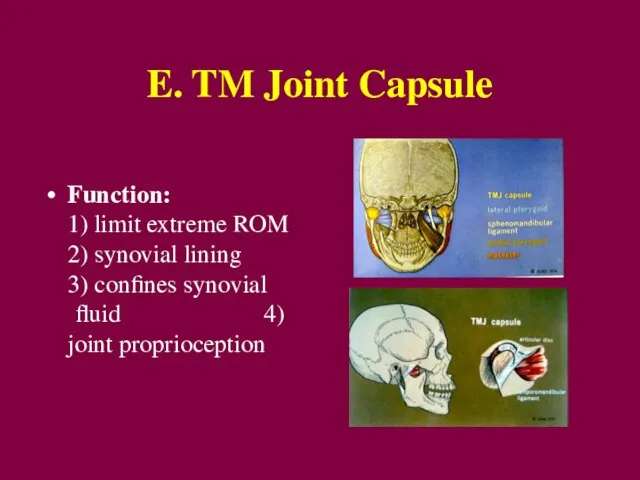
- 24. E. TM Joint Capsule Function: 1) limit extreme ROM 2) synovial lining 3) confines synovial fluid
- 25. F. Mandibular Ligaments Restrict and limit joint range of motion
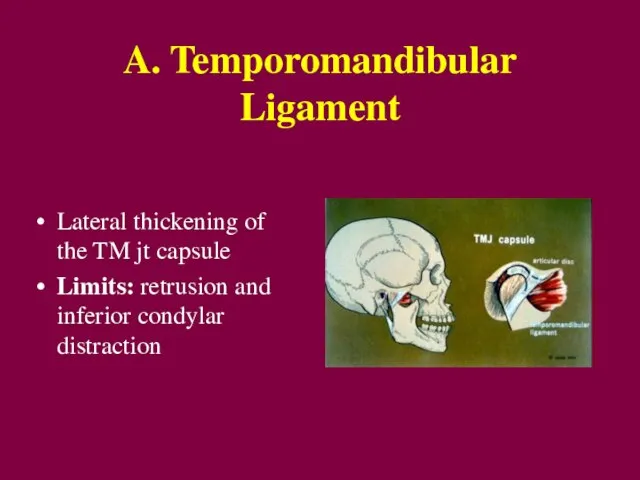
- 26. A. Temporomandibular Ligament Lateral thickening of the TM jt capsule Limits: retrusion and inferior condylar distraction
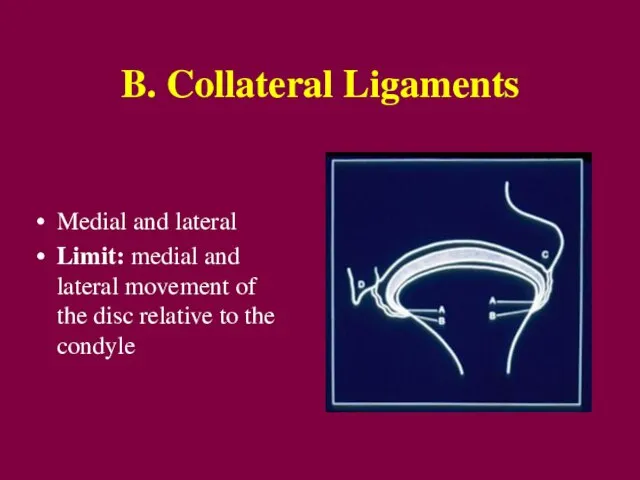
- 27. B. Collateral Ligaments Medial and lateral Limit: medial and lateral movement of the disc relative to
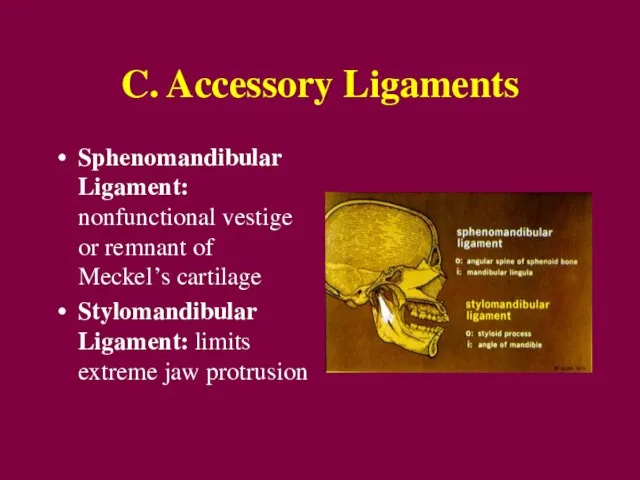
- 28. C. Accessory Ligaments Sphenomandibular Ligament: nonfunctional vestige or remnant of Meckel’s cartilage Stylomandibular Ligament: limits extreme
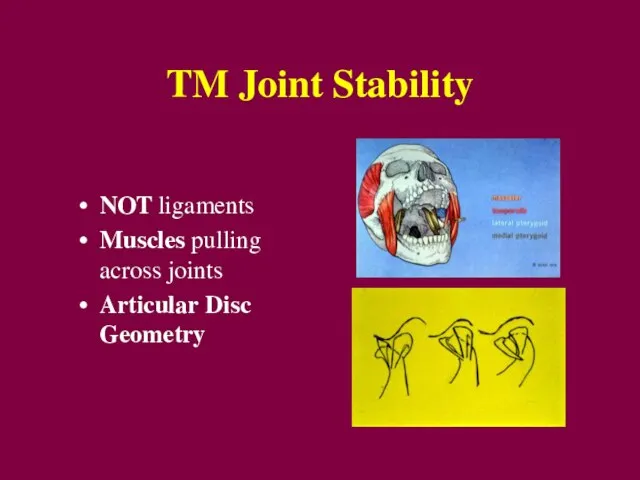
- 29. TM Joint Stability NOT ligaments Muscles pulling across joints Articular Disc Geometry
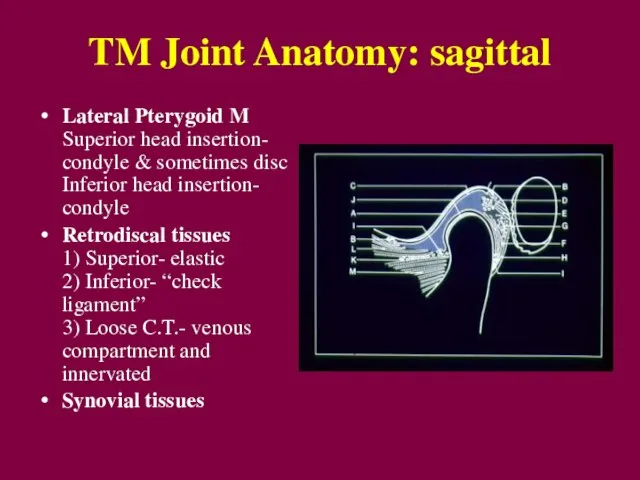
- 30. TM Joint Anatomy: sagittal Lateral Pterygoid M Superior head insertion- condyle & sometimes disc Inferior head
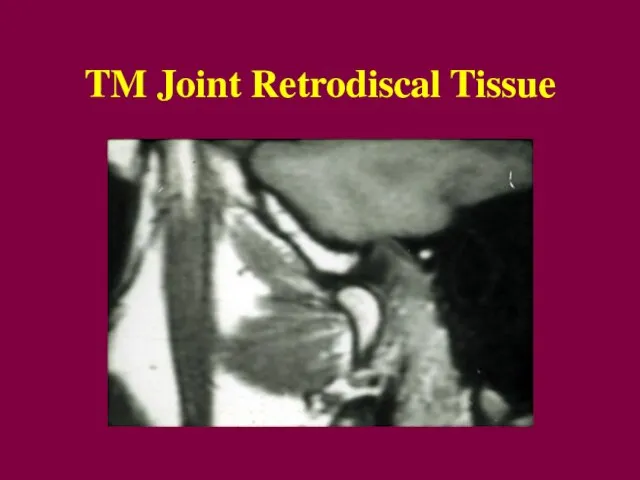
- 31. TM Joint Retrodiscal Tissue
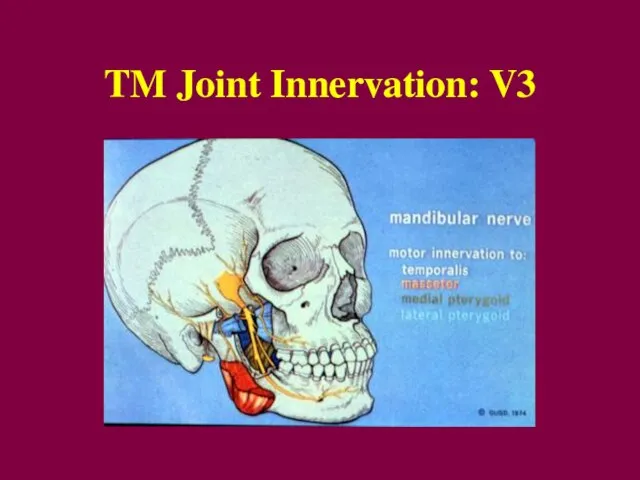
- 32. TM Joint Innervation: V3
- 33. TM Joint Functional Anatomy Read pages in Okeson, pp. 22-26!
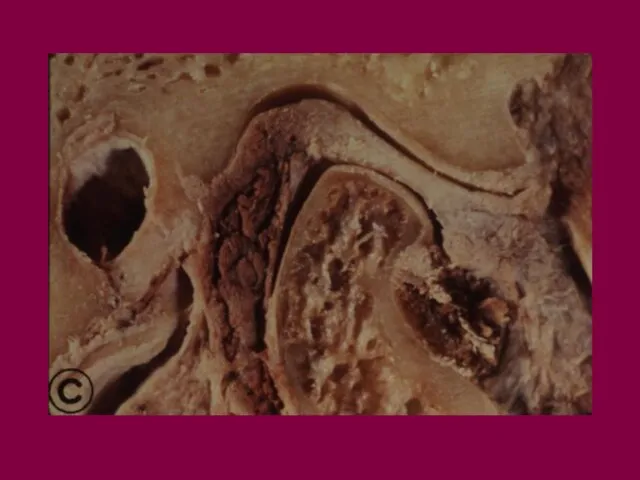
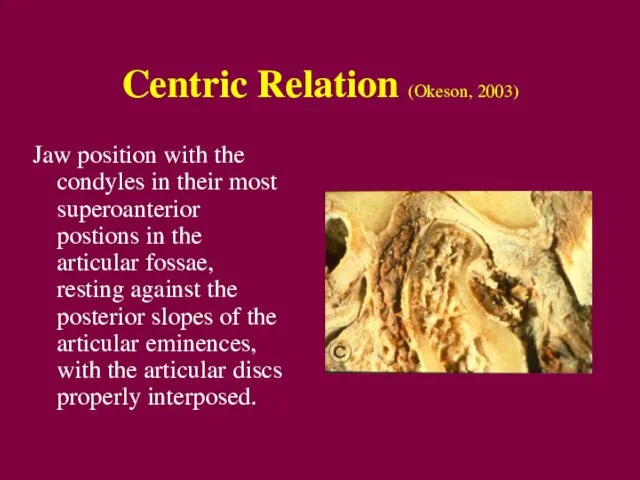
- 37. Centric Relation (Okeson, 2003) Jaw position with the condyles in their most superoanterior postions in the
- 38. Biology of Centric Relation Muscloskeletal Stability: a stable position in which to load the joint, mm
- 39. Biology of Centric Relation Clinically repeatable: a reference position for restorative dental procedures … but NOT
- 41. Скачать презентацию
Слайд 3A. Temporalis Muscle
Origin: temporal fossa & temporal fascia
Insertion: coronoid process & anterior
A. Temporalis Muscle
Origin: temporal fossa & temporal fascia
Insertion: coronoid process & anterior
Слайд 4A. Temporalis Muscle
Function: Elevation and positioning of the mandible
A. Temporalis Muscle
Function: Elevation and positioning of the mandible
Слайд 5B. Masseter Muscle
Origin: zygomatic arch
Insertion: lateral surface of ramus, coronoid process &
B. Masseter Muscle
Origin: zygomatic arch
Insertion: lateral surface of ramus, coronoid process &
Слайд 6B. Masseter Muscle
Function: power with vertical elevation of the mandible; deep portion
B. Masseter Muscle
Function: power with vertical elevation of the mandible; deep portion
Слайд 7C. Medial Pterygoid Muscle
Origin: medial surface of lateral pterygoid plate, pyramidal process
C. Medial Pterygoid Muscle
Origin: medial surface of lateral pterygoid plate, pyramidal process
Слайд 8C. Medial Pterygoid Muscle
Function: elevation of the mandible, protrusion of the mandible
C. Medial Pterygoid Muscle
Function: elevation of the mandible, protrusion of the mandible
Слайд 9Pterygomasseteric Sling
Pterygomasseteric Sling
Слайд 10D. Inferior Lateral Pterygoid Muscle
Origin: lateral surface of lateral pterygoid plate
Insertion: pterygoid
D. Inferior Lateral Pterygoid Muscle
Origin: lateral surface of lateral pterygoid plate
Insertion: pterygoid
Слайд 11D. Inferior Lateral Pterygoid Muscle
Function: protrusion, lateral movement and contributes to opening
D. Inferior Lateral Pterygoid Muscle
Function: protrusion, lateral movement and contributes to opening
Слайд 12E. Superior Lateral Pterygoid Muscle
Origin: infratemporal surface greater wing of the sphenoid
E. Superior Lateral Pterygoid Muscle
Origin: infratemporal surface greater wing of the sphenoid
Слайд 13E. Superior Lateral Pterygoid Muscle
Function: active with the muscles of closure, especially
E. Superior Lateral Pterygoid Muscle
Function: active with the muscles of closure, especially
Слайд 14Temporomandibular Joint Anatomy
Temporomandibular Joint Anatomy
Слайд 15“Craniomandibular Joint”: a diarthrodial or synovial lined joint
“Craniomandibular Joint”: a diarthrodial or synovial lined joint
Слайд 16A compound joint: > 2 components
Temporal Bone
Mandibular Condyle
Articular Disc
A compound joint: > 2 components
Temporal Bone
Mandibular Condyle
Articular Disc
Слайд 17A. Temporal Bone
Cranial component
Mandibular fossa
Articular eminence
Articular surface from superior
A. Temporal Bone
Cranial component
Mandibular fossa
Articular eminence
Articular surface from superior
Слайд 18B. Mandibular Component: Condyle
Condylar dimensions: A-P 8-10 mm M-L 15-20 mm
B. Mandibular Component: Condyle
Condylar dimensions: A-P 8-10 mm M-L 15-20 mm
Слайд 19B. Mandibular Condyle
Variation side to side in size and shape is
B. Mandibular Condyle
Variation side to side in size and shape is
Слайд 20C. Articular Tissue
Origin: modified periosteum of intramembranous bone, NOT endochondral origin.
C. Articular Tissue
Origin: modified periosteum of intramembranous bone, NOT endochondral origin.
Слайд 21C. Articular Tissue
Function: 1) load distribution 2) synovial lubrication
Character: NOT
C. Articular Tissue
Function: 1) load distribution 2) synovial lubrication
Character: NOT
Слайд 22D. Articular Disc
Composition: avascular connective tissue, collagenous
Shape: biconcave in cross
D. Articular Disc
Composition: avascular connective tissue, collagenous
Shape: biconcave in cross
Слайд 23D. Articular Disc
D. Articular Disc
Слайд 24E. TM Joint Capsule
Function: 1) limit extreme ROM 2) synovial lining 3)
E. TM Joint Capsule
Function: 1) limit extreme ROM 2) synovial lining 3)
Слайд 25F. Mandibular Ligaments
Restrict and limit
joint range of motion
F. Mandibular Ligaments
Restrict and limit
joint range of motion
Слайд 26A. Temporomandibular Ligament
Lateral thickening of the TM jt capsule
Limits: retrusion and
A. Temporomandibular Ligament
Lateral thickening of the TM jt capsule
Limits: retrusion and
Слайд 27B. Collateral Ligaments
Medial and lateral
Limit: medial and lateral movement of the
B. Collateral Ligaments
Medial and lateral
Limit: medial and lateral movement of the
Слайд 28C. Accessory Ligaments
Sphenomandibular Ligament: nonfunctional vestige or remnant of Meckel’s cartilage
Stylomandibular Ligament:
C. Accessory Ligaments
Sphenomandibular Ligament: nonfunctional vestige or remnant of Meckel’s cartilage
Stylomandibular Ligament:
Слайд 29TM Joint Stability
NOT ligaments
Muscles pulling across joints
Articular Disc Geometry
TM Joint Stability
NOT ligaments
Muscles pulling across joints
Articular Disc Geometry
Слайд 30TM Joint Anatomy: sagittal
Lateral Pterygoid M Superior head insertion- condyle & sometimes
TM Joint Anatomy: sagittal
Lateral Pterygoid M Superior head insertion- condyle & sometimes
Слайд 31TM Joint Retrodiscal Tissue
TM Joint Retrodiscal Tissue
Слайд 32TM Joint Innervation: V3
TM Joint Innervation: V3
Слайд 33TM Joint Functional Anatomy
Read pages in Okeson, pp. 22-26!
TM Joint Functional Anatomy
Read pages in Okeson, pp. 22-26!

Слайд 37Centric Relation (Okeson, 2003)
Jaw position with the condyles in their most superoanterior
Centric Relation (Okeson, 2003)
Jaw position with the condyles in their most superoanterior
Слайд 38Biology of Centric Relation
Muscloskeletal Stability: a stable position in which to load
Biology of Centric Relation
Muscloskeletal Stability: a stable position in which to load
Слайд 39Biology of Centric Relation
Clinically repeatable: a reference position for restorative dental procedures
…
Biology of Centric Relation
Clinically repeatable: a reference position for restorative dental procedures
…
 Основные сведения внешней баллистики
Основные сведения внешней баллистики Презентация на тему Освоение Сибири
Презентация на тему Освоение Сибири  Содружество Независимых Государств (СНГ)
Содружество Независимых Государств (СНГ) Графики вокруг нас
Графики вокруг нас Зарождение демократии в Афинах
Зарождение демократии в Афинах Ислам: противостояние Востока и Запада
Ислам: противостояние Востока и Запада Построение плана местности
Построение плана местности Менеджмент как вид деятельности и системы управления
Менеджмент как вид деятельности и системы управления Creation of Transport & Logistic Centre (TLC) on the Territory of Free Economic Zone Gomel-Raton
Creation of Transport & Logistic Centre (TLC) on the Territory of Free Economic Zone Gomel-Raton Геоцентрическая система мира. Система мира Птолемея
Геоцентрическая система мира. Система мира Птолемея Презентация на тему Что такое молоко
Презентация на тему Что такое молоко Презентация на тему Основные участники процесса формирования цен
Презентация на тему Основные участники процесса формирования цен  Производственная практика на сублиматном заводе
Производственная практика на сублиматном заводе Культура и быт народов Северного Кавказа
Культура и быт народов Северного Кавказа Презентация на тему Мастера русского авангарда
Презентация на тему Мастера русского авангарда FR-A700 Мастер на все руки
FR-A700 Мастер на все руки Habble резентация
Habble резентация Презентация для тройничка
Презентация для тройничка Лаборатория юного исследователя за 2020-2021 уч. год
Лаборатория юного исследователя за 2020-2021 уч. год Практика по заданиям 20, 24 ЕГЭ
Практика по заданиям 20, 24 ЕГЭ CELLEND Совершенный фитокосмецевтический комплекс
CELLEND Совершенный фитокосмецевтический комплекс  Железы внешней, внутренней и смешанной секреции
Железы внешней, внутренней и смешанной секреции  Презентация на тему Религия древних египтян (5 класс)
Презентация на тему Религия древних египтян (5 класс) Пример разработки высоконагруженной реляционной базы данных
Пример разработки высоконагруженной реляционной базы данных Содержание и методика подготовки исследовательских работ обучающихся по краеведению
Содержание и методика подготовки исследовательских работ обучающихся по краеведению Куда едет школа,
Куда едет школа, оппзл
оппзл Номинация Золотые руки. Валентина Александровна Лобанова
Номинация Золотые руки. Валентина Александровна Лобанова