- Normal labour

Содержание
- 2. Labour is the expulsion of the fetus and placenta from the uterus and is traditionally divided
- 3. Mechanism of labour In humans, the cause of labour is unknown. The following facts are accepted:
- 4. Mechanism of labour • The decidua releases prostaglandins (PGs), mainly PGE2 and PGF2a. Such PGs cause
- 5. Mechanism of labour • Oxytocin, released from the posterior pituitary, cannot be detected in the blood
- 6. Uterine action The fetus is propelled down the birth canal by the action of the myometrium.
- 7. Uterine action During labour, contractions increase in frequency and strength. Contractions are painful and this may
- 8. Uterine action Labour starts with contractions about one in every 10 minutes increasing to one in
- 9. Stages 1 The first stage, dilatation —from the onset of labour until the cervix is fully
- 10. The uterus in the first stage 1 Uterine muscle fibres contract and retract, so they do
- 11. The uterus in the second stage 1 A diminution in the transverse diameters because of: •
- 12. The uterus in the third stage 1 The uterine muscles contract so constricting the blood vessels
- 13. The uterus in the third stage The placenta is therefore sheared off and is finally expelled
- 14. Diagnosis of labour The onset of labour is defined as regular painful uterine contractions that cause
- 15. First stage of labour Progress in labour is monitored by descent of the fetal head together
- 16. 1 High-risk factors—obstetric, paediatric or anaesthetic. 2 A record of the fetal heart rate. Higher risk
- 17. 3 The cervicogram: graphical record of the rate of cervical dilatation. 4 Descent of fetal head.
- 18. After the first examination the following should be plotted: 1 The amount of the fetal head
- 19. 3 A line of expected cervical dilatation should then also be plotted. The WHO have produced
- 20. The level of descent of the presenting part should be checked and plotted every hour, whilst
- 22. A partogram used to assess the progress of labour. The lines in the cervical dilated section
- 23. Care of the patient • The woman should not be left alone during labour. Ideally there
- 24. Бажано забезпечити співвідношення одна роділля – одна акушерка
- 25. На пологах присутній партнер
- 26. Second stage of labour 1 During the expulsive stage, the woman is encouraged to push with
- 27. Second stage of labour 2 Monitoring progress in the second stage of labour is by vaginal
- 28. Second stage of labour 6 The baby’s mouth and nasal passages are usually sucked free of
- 30. Third stage of labour 1 Syntometrine has been given with the delivery. Signs of placental separation
- 31. Third stage of labour 4 The membranes usually follow the placenta andcan be removed by gentle
- 32. Pain relief in labour • Labour is usually painful. Relief of pain is better given before
- 33. Nitrous oxide This is self-administered, pre-mixed with O2 (50%of each), in Entonox machines. Inhalation should start
- 34. Pethidine Pethidine has been used for many years as an analgesic in labour. Many units have
- 35. Non-drug analgesia Increasing numbers of women are turning to nonpharmacological methods of pain relief. Pain is
- 36. Relaxation The woman should take training in pregnancy. The method works best if there is a
- 37. Acupuncture Some women opt for acupuncture in labour. The effects are very variable from one person
- 38. Transcutaneous nerve stimulation (TENS) Small pulses of electrical vibration to the muscles of the back, from
- 39. Anaesthesia Depression of the central or peripheral nervous system to prevent transmission and reception of painful
- 40. Regional Nerve roots are blocked at their outflow. Spinal block • Heavy nupivercaine into subarachnoid space.
- 41. Epidural block • Bupivacaine 1% or Marcain 0.25–0.5% through a cannula inserted into peridural fat. Affects
- 42. Complications • A serious complication of the epidural block is puncture of the dura and so
- 43. Caudal block • Localized epidural through sacral hiatus. • Gives good anaesthesia for operative deliveries but
- 44. Local Pudendal • Block pudendal nerve with Xylocaine 0.5 or 1% as its two or three
- 45. Field block A local infiltration of the nerve endings in the vulva and labia: • Prior
- 47. Скачать презентацию
Слайд 3Mechanism of labour
In humans, the cause of labour is unknown. The following
Mechanism of labour
In humans, the cause of labour is unknown. The following
Слайд 4Mechanism of labour
• The decidua releases prostaglandins (PGs), mainly PGE2 and PGF2a.
Mechanism of labour
• The decidua releases prostaglandins (PGs), mainly PGE2 and PGF2a.
Слайд 5Mechanism of labour
• Oxytocin, released from the posterior pituitary, cannot be detected
Mechanism of labour
• Oxytocin, released from the posterior pituitary, cannot be detected
Слайд 6Uterine action
The fetus is propelled down the birth canal by the action
Uterine action
The fetus is propelled down the birth canal by the action
Слайд 7Uterine action
During labour, contractions increase in frequency
and strength. Contractions are painful
Uterine action
During labour, contractions increase in frequency
and strength. Contractions are painful
Слайд 8Uterine action
Labour starts with contractions about one in
every 10 minutes increasing
Uterine action
Labour starts with contractions about one in
every 10 minutes increasing
Слайд 9Stages
1 The first stage, dilatation —from the onset of labour until the
Stages
1 The first stage, dilatation —from the onset of labour until the
Слайд 10The uterus in the first stage
1 Uterine muscle fibres contract and retract,
The uterus in the first stage
1 Uterine muscle fibres contract and retract,
Слайд 11The uterus in the second stage
1 A diminution in the transverse diameters
The uterus in the second stage
1 A diminution in the transverse diameters
Слайд 12The uterus in the third stage
1 The uterine muscles contract so constricting
The uterus in the third stage
1 The uterine muscles contract so constricting
Слайд 13The uterus in the third stage
The placenta is therefore sheared off and
The uterus in the third stage
The placenta is therefore sheared off and
Слайд 14Diagnosis of labour
The onset of labour is defined as regular painful uterine
Diagnosis of labour
The onset of labour is defined as regular painful uterine
Слайд 15First stage of labour
Progress in labour is monitored by descent of the
First stage of labour
Progress in labour is monitored by descent of the
Слайд 161 High-risk factors—obstetric, paediatric or anaesthetic.
2 A record of the fetal heart
1 High-risk factors—obstetric, paediatric or anaesthetic.
2 A record of the fetal heart
Слайд 173 The cervicogram: graphical record of the rate of cervical dilatation.
4 Descent
3 The cervicogram: graphical record of the rate of cervical dilatation.
4 Descent
Слайд 18After the first examination the following should be plotted:
1 The amount of
After the first examination the following should be plotted:
1 The amount of
Слайд 193 A line of expected cervical dilatation should then also be plotted.
3 A line of expected cervical dilatation should then also be plotted.
Слайд 20The level of descent of the presenting part should be checked and
The level of descent of the presenting part should be checked and
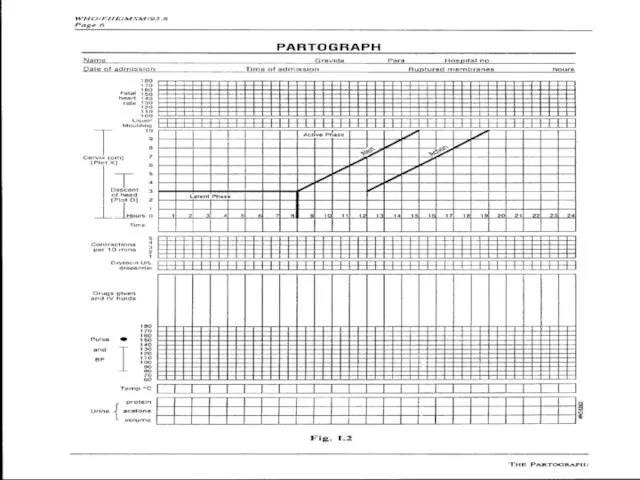
Слайд 22A partogram used to assess the progress of labour. The lines in
A partogram used to assess the progress of labour. The lines in
Слайд 23Care of the patient
• The woman should not be left alone during
Care of the patient
• The woman should not be left alone during
Слайд 24Бажано забезпечити
співвідношення
одна роділля –
одна акушерка
Бажано забезпечити
співвідношення
одна роділля –
одна акушерка

Слайд 25На пологах
присутній партнер
На пологах
присутній партнер
Слайд 26Second stage of labour
1 During the expulsive stage, the woman is encouraged
Second stage of labour
1 During the expulsive stage, the woman is encouraged
Слайд 27Second stage of labour
2 Monitoring progress in the second stage of labour
Second stage of labour
2 Monitoring progress in the second stage of labour
Слайд 28Second stage of labour
6 The baby’s mouth and nasal passages are usually
Second stage of labour
6 The baby’s mouth and nasal passages are usually

Слайд 30Third stage of labour
1 Syntometrine has been given with the delivery. Signs
Third stage of labour
1 Syntometrine has been given with the delivery. Signs
Слайд 31Third stage of labour
4 The membranes usually follow the placenta andcan be
Third stage of labour
4 The membranes usually follow the placenta andcan be
Слайд 32Pain relief in labour
• Labour is usually painful. Relief of pain is
Pain relief in labour
• Labour is usually painful. Relief of pain is
Слайд 33Nitrous oxide
This is self-administered, pre-mixed with O2 (50%of each), in Entonox machines.
Nitrous oxide
This is self-administered, pre-mixed with O2 (50%of each), in Entonox machines.
Слайд 34Pethidine
Pethidine has been used for many years as an analgesic in labour.
Pethidine
Pethidine has been used for many years as an analgesic in labour.
Слайд 35Non-drug analgesia
Increasing numbers of women are turning to nonpharmacological methods of pain
Non-drug analgesia
Increasing numbers of women are turning to nonpharmacological methods of pain
Слайд 36Relaxation
The woman should take training in pregnancy. The method works best
Relaxation
The woman should take training in pregnancy. The method works best
Слайд 37Acupuncture
Some women opt for acupuncture in labour. The effects are very variable
Acupuncture
Some women opt for acupuncture in labour. The effects are very variable
Слайд 38Transcutaneous nerve stimulation (TENS)
Small pulses of electrical vibration to the muscles of
Transcutaneous nerve stimulation (TENS)
Small pulses of electrical vibration to the muscles of
Слайд 39Anaesthesia
Depression of the central or peripheral nervous system to prevent transmission and
Anaesthesia
Depression of the central or peripheral nervous system to prevent transmission and
Слайд 40Regional
Nerve roots are blocked at their outflow.
Spinal block
• Heavy nupivercaine
Regional
Nerve roots are blocked at their outflow.
Spinal block
• Heavy nupivercaine
Слайд 41Epidural block
• Bupivacaine 1% or Marcain 0.25–0.5% through a cannula inserted into
Epidural block
• Bupivacaine 1% or Marcain 0.25–0.5% through a cannula inserted into
Слайд 42Complications
• A serious complication of the epidural block is puncture of the
Complications
• A serious complication of the epidural block is puncture of the
Слайд 43Caudal block
• Localized epidural through sacral hiatus.
• Gives good anaesthesia for operative
Caudal block
• Localized epidural through sacral hiatus.
• Gives good anaesthesia for operative
Слайд 44Local
Pudendal
• Block pudendal nerve with Xylocaine 0.5 or 1%
as its two or
Local
Pudendal
• Block pudendal nerve with Xylocaine 0.5 or 1%
as its two or
Слайд 45Field block
A local infiltration of the nerve endings in the vulva and
Field block
A local infiltration of the nerve endings in the vulva and
 Одежда на английском
Одежда на английском Дисперсные системы
Дисперсные системы TV Families
TV Families Пушкин на Юге
Пушкин на Юге Кім екенін тап ойыны
Кім екенін тап ойыны Транзисторный коммутатор зажигания
Транзисторный коммутатор зажигания БАНКЕТНАЯ ПЛОЩАДКА
БАНКЕТНАЯ ПЛОЩАДКА Презентация на тему Транспорт и правила дорожного движения
Презентация на тему Транспорт и правила дорожного движения Визитная карточка
Визитная карточка Кинезиологические упражнения как вид здоровьесберегающих технологий
Кинезиологические упражнения как вид здоровьесберегающих технологий Презентация на тему Защита окружающей среды
Презентация на тему Защита окружающей среды  ПРИКЛАДНОЕ регионоведение рекреационная регионализация
ПРИКЛАДНОЕ регионоведение рекреационная регионализация  Изразцы. Виды изразцов
Изразцы. Виды изразцов Лизинг
Лизинг История компании Наша история началась в 1990 году с создания первой в России компьютерной программы для финансового анализа деятел
История компании Наша история началась в 1990 году с создания первой в России компьютерной программы для финансового анализа деятел Новое слово в раскрое листовых материалов от
Новое слово в раскрое листовых материалов от Kleidung
Kleidung Отношения
Отношения Бизнес-планирование: основные понятия, структура, ключевые показатели
Бизнес-планирование: основные понятия, структура, ключевые показатели Стандартизация, основные понятия и определения
Стандартизация, основные понятия и определения Неделя истории в МБОУ СОШ № 2
Неделя истории в МБОУ СОШ № 2 Позвоночные.Тип Хордовые
Позвоночные.Тип Хордовые Использование викторины как средства повышения мотивации
Использование викторины как средства повышения мотивации КРИМИНАЛИСТИЧЕСКОЕ ИССЛЕДОВАНИЕ МАТЕРИАЛОВ ДОКУМЕНТОВ
КРИМИНАЛИСТИЧЕСКОЕ ИССЛЕДОВАНИЕ МАТЕРИАЛОВ ДОКУМЕНТОВ «Технология формирования готовности педагога к исследовательской деятельности»
«Технология формирования готовности педагога к исследовательской деятельности» lektsia_1
lektsia_1 Лекция 2. Позиционирование и навигация Геоинформационные системы
Лекция 2. Позиционирование и навигация Геоинформационные системы Сказка – рассказ, который повествует о таких событиях, которые в жизни произойти не могут, они невероятны фантастичны, Учат добру.
Сказка – рассказ, который повествует о таких событиях, которые в жизни произойти не могут, они невероятны фантастичны, Учат добру.