- Physics

Содержание
- 2. INTRODUCTION For the safe & efficient use of anaesthetic apparatus, the anaesthetist must have a clear
- 3. INTRODUCTION Physics is the world in measurable terms and the physical laws apply to all states
- 4. UNITS OF MEASUREMENT Base SI units - length (meter) - mass (kilogram) - time (second) -
- 5. UNITS OF MEASUREMENT DERIVED UNITS - temp in degrees celcius - force (newton) - pressure (pascal)
- 6. UNITS OF MEASUREMENT UNITS NOT IN THE SI SYSTEM - pressure (mmHg) - pressure (cmh2o) -
- 7. UNITS OF MEASUREMENT - 1 kilopascal = 7.5mmHg. - 1 Bar = 750mmHg - 1 kilopascal
- 8. PRESSURE Force = mass x acceleration = kgms -2 = Newton Pressure = Force/Area 1 Pascal
- 9. PRESSURE I Bar = 100kPa = Atmospheric pressure at sea level
- 10. PRESSURE Normal thumb pressure on a syringe = 25N 2 ml syringe has an area of
- 11. PRESSURE With a 20 ml syringe, the pressure exerted is 100kPA = 6X SBP of 120
- 12. PRESSURE Bed Sores --- 20kg of patient mass supported on an area of contact of 100cm2
- 13. PRESSURE Pressure relief valves and expiratory valves Pressure in the circuit exerts a force on the
- 14. GAUGE AND ABSOLUTE PRESSURE Full oxygen cylinder has a gauge pressure of 137 bar Empty cylinder
- 15. GAUGE PRESSURE Absolute P = Gauge P + Atmospheric P Most times we ignore atmospheric P
- 16. PRESSURE For ideal gases (air, nitrogen, oxygen)-Full cylinder pressure = 2000 PSI -Full cylinder volume= 660
- 17. FLUID FLOW Flow = quantity of fluid/gas passing a point in unit time Can be turbulent
- 18. LAMINAR FLOW Flow moves in a steady manner with no eddies or turbulence Flow is greatest
- 19. LAMINAR FLOW Flow = ∏Pd4/128ųl P = Pressure d = Diameter Ų = viscosity L =
- 20. THE ANESTHESIA MACHINE The resistance to flow is a function of the viscosity of the gas,
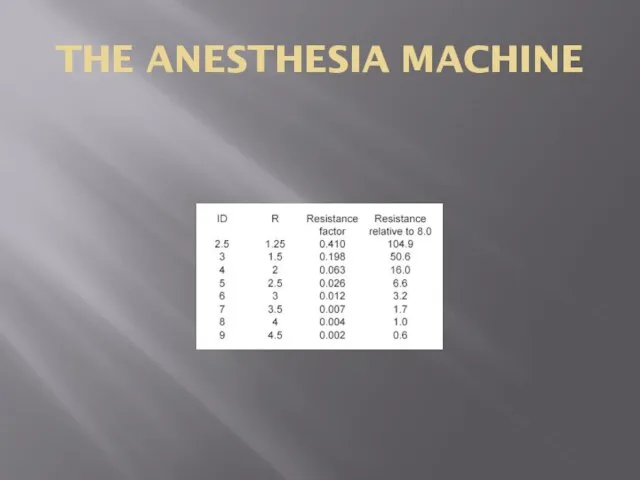
- 21. THE ANESTHESIA MACHINE
- 22. TURBULENT FLOW Swirls or eddies present Resistance is higher than laminar flow Reynold’s Number = vpd/µ
- 23. TURBULENT FLOW Most important property is density which is mass/volume
- 24. CRITICAL FLOW Critical flow for a typical anesthetic gas has approx the same numerical value as
- 25. CRITICAL FLOW Air has a lower density than Nitrous Oxide – laminar flow prevails Air flow
- 26. CRITICAL FLOW Although the bronchi and smaller air passages are narrower than the trachea, the air
- 27. TENSION Tension is a tangential force in Nm acting on a length of wall A balance
- 28. TENSION A fall in pressure in an arteriole tends to distend it less and so would
- 29. SURFACE TENSION Pressure = 2T/R ( wall of a sphere) Surfactant decreases surface tension lining the
- 30. SURFACE TENSION On the surface of a liquid, some of the forces of attraction between molecules
- 31. THE ANESTHESIA MACHINE Tension in the wall of the bag equals Pressure x Radius x ½
- 32. BERNOULLI PRINCIPLE Fall in pressure at a narrowing of a tube Gas/Fluid has potential energy in
- 33. BERNOULLI PRINCIPLE Therefore decrease in potential energy If this pressure falls below atmospheric pressure, can entrain
- 34. THE GAS LAWS Boyles Law Charles Law Third Perfect Gas Law Dalton’s Law of Partial Pressures
- 35. BOYLES LAW At constant temp, V ∞ 1/P How much oxygen is available at atmospheric pressure
- 36. CHARLES LAW At constant pressure, V∞Temp Gases expand when heated
- 37. THIRD PERFECT GAS LAW At constant volume, P ∞ Temp STP – 273.15K and 101.325kPa
- 38. ADIABATIC CHANGE The three gas laws describe the behaviour of a gas when one of the
- 39. ADIABATIC CHANGE The state of a gas can be altered without allowing the gas to exchange
- 40. ADIABATIC CHANGE Thus, the gas is compressed adiabatically and a large temp rise with the associated
- 41. DALTON’S LAW OF PARTIAL PRESSURES In a mixture of gases, the pressure exerted by each gas
- 42. AVOGADRO’S NUMBER States that equal volumes of gases at the same temp and pressure contain equal
- 43. BREATHING SYSTEMS Breathing Circuitsa)Open (non-rebreathing) •Simple face mask or nasal cannula (CO2 diffuses away from the
- 44. AVOGADRO’S NUMBER Typical Nitrous cylinder has 3.4kg of Nitrous Oxide Molec wt = 44 ( 1
- 45. UNIVERSAL GAS CONSTANT PV = nRT In a cylinder, the volume and temp is constant Therefore,
- 46. CRITICAL TEMP Defined as the temp above which a substance cannot be liquefied however much pressure
- 47. CRITICAL TEMP Critical temp for oxygen is -119 degrees Impossible to turn oxygen into its liquid
- 48. SOLUBILITY When a liquid is placed in a closed container, an equilibrium is eventually established at
- 49. SOLUBILITY Saturated Vapour Pressure Henry’s Law – states that at a particular temp, the amt of
- 50. SOLUBILITY The effect of high pressure on the solubility of nitrogen is particularly relevant to deep
- 51. SOLUBILITY Ostwald Solubility Coefficient is the volume of gas which dissolves in one unit volume of
- 52. SOLUBILITY Partition Coefficient is defined as the ratio of the amount of substance present in one
- 53. SOLUBILITY Ether has the highest Ostwald Solubility Coefficient (12). Halothane is 2.3 and Nitrous is 0.47
- 54. SOLUBILITY Second Gas effect Diffusion hypoxia
- 55. SECOND GAS EFFECT During the inspiration of a gas mixture containing nitrous oxide, the N2O is
- 56. DIFFUSION HYPOXIA At the end of an anesthetic using N2O, the N2O diffuses faster into the
- 57. SOLUBILITY Fat is an impt constituent of tissue Oil is therefore used for measurements Agents with
- 58. SOLUBILITY High solubility = lower MAC values Anesthetics tend to interfere with the molecular configuration of
- 59. SOLUBILITY Also attach to the long carbon chain molecules present in rubber and plastics
- 60. DIFFUSION AND OSMOSIS Diffusion is the process by which the molecules of a substance transfer through
- 61. DIFFUSION Pulmonary Diffusing Capacity Rate at which CO leaves the alveoli is dependent on the rate
- 62. EFFECT OF MOLECULAR SIZE Grahams Law states that the rate of diffusion of a gas is
- 63. OSMOLARITY Is the sum total of the molarities of the solutes in a solution RL has
- 64. OSMOLARITY If a patient is transfused hypotonic fluids – get changes in the osmotic pressure gradient
- 65. OSMOLARITY Number of osmoles per kg of water or clear solution Avoids the effect of temp
- 66. HEAT CAPACITY Specific Heat Capacity is defined as the amount of heat required to raise the
- 67. HEAT CAPACITY Body temp = 36 degrees Shivers – increases heat production 4 fold to 320W.
- 68. HEAT CAPACITY This patient will need to shiver for 17 minutes to produce the heat required
- 69. HEAT CAPACITY Specific Heat Capacity of blood = 3.6kJ/kg/C Transfuse 2L of blood at 5 degrees
- 70. HEAT CAPACITY Heat Required = 216kJ (2x3.6x30) Heat Capacity of 70kg person = 245kJ/C Therefore temp
- 71. THE ANESTHESIA MACHINE
- 72. THE ANESTHESIA MACHINE N2O is stored in the tank as a liquid in equilibration with the
- 73. THE ANESTHESIA MACHINE Why does the pressure go down as the gas cools?
- 74. THE ANESTHESIA MACHINE The pressure in the tank reflects the force of the molecules bouncing off
- 75. THE ANESTHESIA MACHINE Thermal energy is taken out of the nitrous tank by heat of vaporization.
- 76. THE ANESTHESIA MACHINE As oxygen is drawn from the tank, both the temp and pressure drop
- 77. CIRCULATION Ohm’s Law Pressure = Flow x Resistance Voltage = Current x Resistance Resistance = Pressure/Flow
- 78. CIRCULATION SVR = (MAP – CVP)/CO Poiseulle’s equation – Resistance to flow is proportional to 1/r4
- 79. CIRCULATION P = 2T/R Failing heart – Increase in R and therefore a decrease in P.
- 80. CIRCULATION MAP dependent on SVR and CO Patient with a decreased SVR, a high BP indicates
- 81. AUSCULTATORY METHOD Based on the Korotkoff sounds The systolic and diastolic pressures are determined and the
- 82. OSCILLOMETRIC METHOD Based on pressure waveform in an air filled cuff coupled to the arterial pulse
- 83. INVASIVE MONITORING Transducer is a strain gauge that linearly converts pressure to electrical resistance The monitor
- 84. INVASIVE MONITORING Strain Gauge – movements of the diaphragm alter the tension in the resistance wire
- 85. INVASIVE MONITORING Wheatstone Bridge 4 resistors, a source and a galvanometer Variable resistor can be zeroed
- 86. INVASIVE MONITORING What does it mean to “zero” the transducer?
- 87. INVASIVE MONITORING The act of zeroing the transducer tells the monitor the electrical resistance that should
- 88. INVASIVE MONITORING Column of water between the point that is opened to air and the transducer
- 89. CARDIAC OUTPUT Gold standard for measuring cardiac output is by applying Fick’s Law to oxygen flow
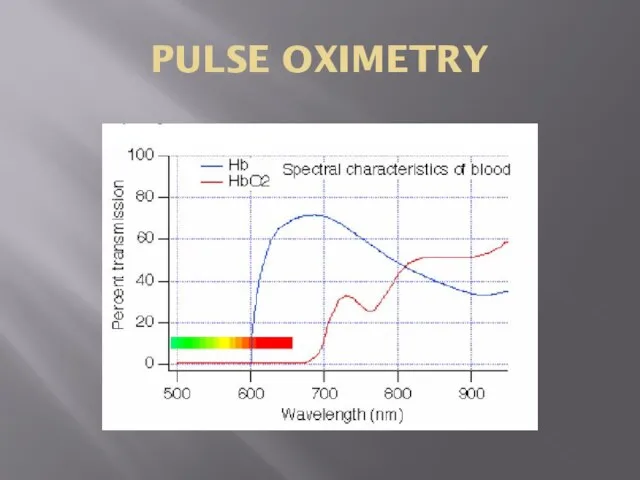
- 90. PULSE OXIMETRY Beer Lambert Law Absorption of light = Concentration x Thickness x extinction coefficient Has
- 91. PULSE OXIMETRY Beer’s Law states that the absorption of radiation by a given thickness of a
- 92. PULSE OXIMETRY Lambert’s Law states that each layer of equal thickness absorbs an equal fraction of
- 93. PULSE OXIMETRY The diodes alternate at about 100 times a second between 660nm, 940nm and off
- 94. PULSE OXIMETRY Two parts to the waveform - static component which represents the absorption of the
- 95. PULSE OXIMETRY On the assumption that the tissue thickness is the same for both oxyHb and
- 96. PULSE OXIMETRY
- 97. PULSE OXIMETRY Unable to distinguish more that two types of Hb Cannot identify carboxyHb --- to
- 98. ELECTRICAL SAFETY Two major hazards - burns - arrhythmias
- 99. ELECTRICAL SAFETY Three types of electrical current - macroshock - microshock - radiofrequency currents
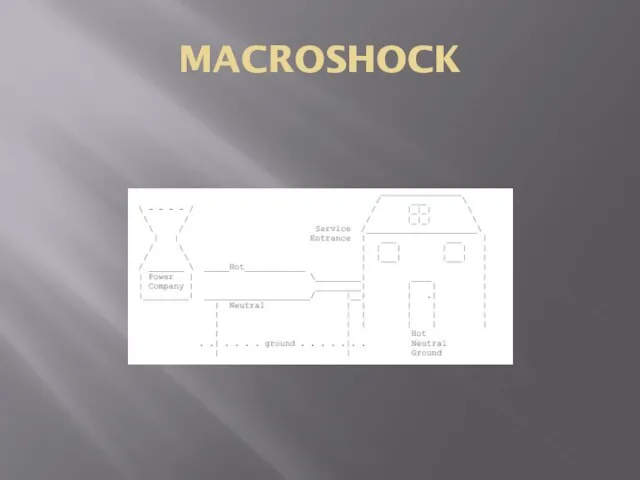
- 100. ELECTRICAL SAFETY A power station supplies electricity at very high voltage to a substation where the
- 101. ELECTRICAL SAFETY Third conductor is connected to earth at the hospital. If a person touches a
- 102. ELECTRICAL SAFETY 1 mA = tingling sensation on touching the live parts of the apparatus Current
- 103. ELECTRICAL SAFETY If you are wearing non standard footwear and standing in a pool of saline
- 104. ELECTRICAL SAFETY Most of the impedence now occurs at the points of contact with the skin
- 105. ELECTRICAL SAFETY Risk of VF Risk is much greater if the current passes through the heart
- 106. CLASS 1 EQUIPMENT Any conducting part that is accessible to the user, such as the metal
- 107. CLASS 2 Double insulated equipment All accessible parts are protected by 2 layers of insulation or
- 108. CLASS 3 Internally powered equipment Has its own power source located within the equipment Although the
- 109. ISOLATED PATIENT CIRCUITS Some equipment requires electrical connections be made to the patient (monitors) A deliberate
- 110. ISOLATED PATIENT CIRCUITS To counteract this, use an isolated patient circuit or a floating circuit The
- 111. ISOLATED PATIENT CIRCUIT Intended to provide protection should a fault develop in the mains part and
- 112. LEAKAGE CURRENT STANDARDS Electromedical equipment is classified according to the maximum leakage current permissible for particular
- 113. LEAKAGE CURRENT STANDARDS B or BF it it has a floating circuit. Leakage current of 500uA
- 114. ELECTRICAL SAFETY Electrical currents flow in circuits A path must exist from the electrical source to
- 115. ELECTRICAL SAFETY Standardized voltage is about 120V The “120” is the root mean square voltage Alternating
- 116. ROOT MEAN SQUARE If all the values of the sine wave are squared, all the amplitudes
- 117. MACROSHOCK Potential for both burns and arrhythmias Current must flow through the thorax In the thorax
- 118. MACROSHOCK- FACTORS FOR ELECTROCUTION Patient unclothed and wet Patient is on a large metal table, frequently
- 119. MACROSHOCK How much current can we deliver to the anesthetized patient?
- 120. MACROSHOCK Patient may receive 150 volts with direct contact The current he receives will depend on
- 121. MACROSHOCK Current required to produce VF is 80mA Therefore 3mA will not cause VF Resistance of
- 122. MACROSHOCK What is the voltage required to produce an 80mA current across wet skin? V =
- 123. MACROSHOCK How could a patient come into contact with 40 volts in the OR?
- 124. MACROSHOCK
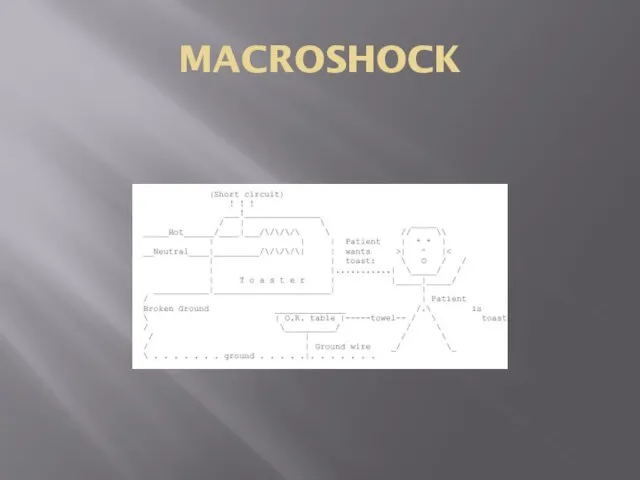
- 125. MACROSHOCK Hot and neutral leads power the device Ground lead connects to the chassis of the
- 126. MACROSHOCK
- 127. MACROSHOCK To avoid helping electrocute the patient, no properly functioning modern monitoring device will complete a
- 128. MACROSHOCK Equipment must be designed so the the hot wire cannot easily short out with the
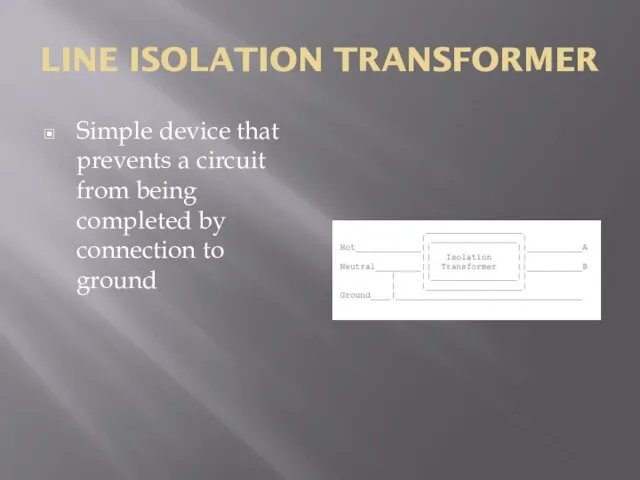
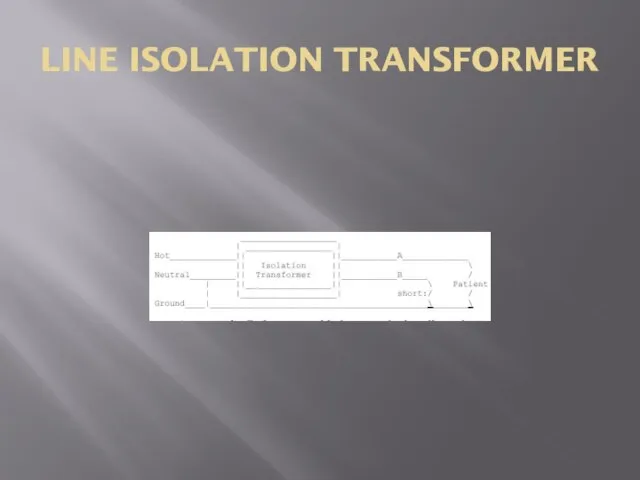
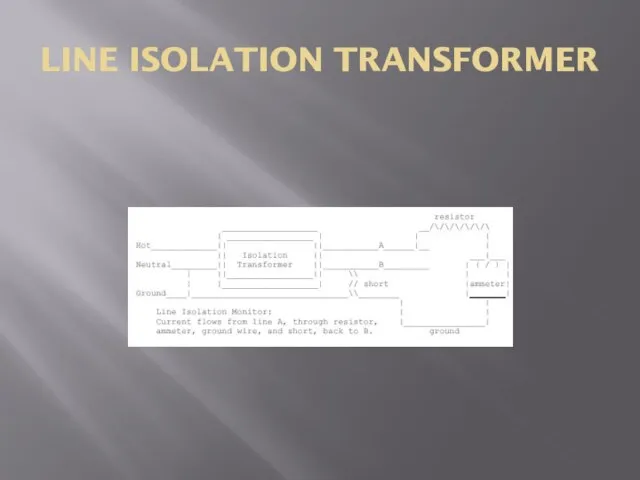
- 129. LINE ISOLATION TRANSFORMER Simple device that prevents a circuit from being completed by connection to ground
- 130. LINE ISOLATION TRANSFORMER
- 131. LINE ISOLATION TRANSFORMER How do you monitor a line isolation transformer to see if there is
- 132. LINE ISOLATION TRANSFORMER
- 133. LINE ISOLATION MONITOR Resistor has a resistance of about 150 000 ohm’s so that the maximum
- 134. MICROSHOCK Refers to currents delivered directly to the myocardium via intracardiac electrodes or catheters. Minimum fibrillation
- 135. MICROSHOCK How much safety does the isolation transformer provide against microshock hazard?
- 136. MICROSHOCK Ground wire should be intact LIM signals a warning if the resistance between the ground
- 137. MICROSHOCK In the presence of a LIM, it takes two shorts to the chassis of two
- 138. ELECTROCAUTERY Current density = current flow per unit area Explains the heating effect of the electrosurgical
- 139. ELECTROCAUTERY These effects become less as the frequency of the current increases being small above 1
- 140. ELECTROCAUTERY Electrosurgical equipment is used to pass a current of a high frequency ( 1Mhz) through
- 141. ELECTROCAUTERY Two connections – neutral or patient plate and the active or cutting electrode The same
- 142. ELECTROCAUTERY If the neutral plate is not properly applied, the area of contact can be reduced
- 143. ELECTROCAUTERY Current density can reach a hazardous value when the electrosurgical current flows through parts of
- 144. ELECTROCAUTERY Frequencies of 500 00- to 2000 000 Hz are used by electrocautery Too high to
- 145. ELECTROCAUTERY The grounding plate does not ground the patient to ground It is the return electrode
- 146. CAPACITANCE Is a measure of the ability of an object to hold electric charge Charge is
- 147. DEFIBRILLATOR Is an example of an instrument in which electric charge is stored and then released
- 148. BREATHING SYSTEMS Open (non-rebreathing) Simple face mask or nasal cannula (CO2 diffuses away from the face)
- 149. BREATHING SYSTEMS Semi-Open (Mapleson / Bain) Most efficient removal of CO2 for a given gas flow
- 150. BREATHING SYSTEMS However, the "A" system is very inefficient (requires high gas flows) to prevent rebreathing
- 151. BREATHING SYSTEMS Semi Closed Circle System Patient gas uptake Some rebreathing of exhaled gas (following removal
- 152. BREATHING SYSTEMS Closed System Gas inflow = Patient Uptake If using sidestream agent / CO2 analyzer,
- 153. CO2 ABSORPTION CO2 Absorption Granules Small enough to have large surface area but large enough to
- 154. CO2 ABSORPTION Composition Sodalime: NaOH, Ca(OH)2 Baralyme: KOH, Ca(OH)2, Ba(OH)2 -More likely to react with anesthetics
- 156. Скачать презентацию
Слайд 3INTRODUCTION
Physics is the world in measurable terms and the physical laws apply
INTRODUCTION
Physics is the world in measurable terms and the physical laws apply
Слайд 4UNITS OF MEASUREMENT
Base SI units
- length (meter)
- mass (kilogram)
-
UNITS OF MEASUREMENT
Base SI units
- length (meter)
- mass (kilogram)
-
Слайд 5UNITS OF MEASUREMENT
DERIVED UNITS
- temp in degrees celcius
- force (newton)
UNITS OF MEASUREMENT
DERIVED UNITS
- temp in degrees celcius
- force (newton)
Слайд 6UNITS OF MEASUREMENT
UNITS NOT IN THE SI SYSTEM
- pressure (mmHg)
-
UNITS OF MEASUREMENT
UNITS NOT IN THE SI SYSTEM
- pressure (mmHg)
-
Слайд 7UNITS OF MEASUREMENT
- 1 kilopascal = 7.5mmHg.
- 1 Bar =
UNITS OF MEASUREMENT
- 1 kilopascal = 7.5mmHg.
- 1 Bar =
Слайд 8PRESSURE
Force = mass x acceleration
= kgms -2 = Newton
Pressure = Force/Area
1
PRESSURE
Force = mass x acceleration
= kgms -2 = Newton
Pressure = Force/Area
1
Слайд 9PRESSURE
I Bar = 100kPa = Atmospheric pressure at sea level
PRESSURE
I Bar = 100kPa = Atmospheric pressure at sea level
Слайд 10PRESSURE
Normal thumb pressure on a syringe = 25N
2 ml syringe has an
PRESSURE
Normal thumb pressure on a syringe = 25N
2 ml syringe has an
Слайд 11PRESSURE
With a 20 ml syringe, the pressure exerted is 100kPA = 6X
PRESSURE
With a 20 ml syringe, the pressure exerted is 100kPA = 6X
Слайд 12PRESSURE
Bed Sores --- 20kg of patient mass supported on an area of
PRESSURE
Bed Sores --- 20kg of patient mass supported on an area of
Слайд 13PRESSURE
Pressure relief valves and expiratory valves
Pressure in the circuit exerts a force
PRESSURE
Pressure relief valves and expiratory valves
Pressure in the circuit exerts a force
Слайд 14GAUGE AND ABSOLUTE PRESSURE
Full oxygen cylinder has a gauge pressure of 137
GAUGE AND ABSOLUTE PRESSURE
Full oxygen cylinder has a gauge pressure of 137
Слайд 15GAUGE PRESSURE
Absolute P = Gauge P + Atmospheric P
Most times we ignore
GAUGE PRESSURE
Absolute P = Gauge P + Atmospheric P
Most times we ignore
Слайд 16PRESSURE
For ideal gases (air, nitrogen, oxygen)-Full cylinder pressure = 2000 PSI -Full
PRESSURE
For ideal gases (air, nitrogen, oxygen)-Full cylinder pressure = 2000 PSI -Full
Слайд 17FLUID FLOW
Flow = quantity of fluid/gas passing a point in unit time
Can
FLUID FLOW
Flow = quantity of fluid/gas passing a point in unit time
Can
Слайд 18LAMINAR FLOW
Flow moves in a steady manner with no eddies or turbulence
Flow
LAMINAR FLOW
Flow moves in a steady manner with no eddies or turbulence
Flow
Слайд 19LAMINAR FLOW
Flow = ∏Pd4/128ųl
P = Pressure
d = Diameter
Ų = viscosity
L = length
LAMINAR FLOW
Flow = ∏Pd4/128ųl
P = Pressure
d = Diameter
Ų = viscosity
L = length
Слайд 20THE ANESTHESIA MACHINE
The resistance to flow is a function of the viscosity
THE ANESTHESIA MACHINE
The resistance to flow is a function of the viscosity
Слайд 21THE ANESTHESIA MACHINE
THE ANESTHESIA MACHINE
Слайд 22TURBULENT FLOW
Swirls or eddies present
Resistance is higher than laminar flow
Reynold’s Number =
TURBULENT FLOW
Swirls or eddies present
Resistance is higher than laminar flow
Reynold’s Number =
Слайд 23TURBULENT FLOW
Most important property is density which is mass/volume
TURBULENT FLOW
Most important property is density which is mass/volume
Слайд 24CRITICAL FLOW
Critical flow for a typical anesthetic gas has approx the same
CRITICAL FLOW
Critical flow for a typical anesthetic gas has approx the same
Слайд 25CRITICAL FLOW
Air has a lower density than Nitrous Oxide – laminar flow
CRITICAL FLOW
Air has a lower density than Nitrous Oxide – laminar flow
Слайд 26CRITICAL FLOW
Although the bronchi and smaller air passages are narrower than the
CRITICAL FLOW
Although the bronchi and smaller air passages are narrower than the
Слайд 27TENSION
Tension is a tangential force in Nm acting on a length of
TENSION
Tension is a tangential force in Nm acting on a length of
Слайд 28TENSION
A fall in pressure in an arteriole tends to distend it less
TENSION
A fall in pressure in an arteriole tends to distend it less
Слайд 29SURFACE TENSION
Pressure = 2T/R ( wall of a sphere)
Surfactant decreases surface tension
SURFACE TENSION
Pressure = 2T/R ( wall of a sphere)
Surfactant decreases surface tension
Слайд 30SURFACE TENSION
On the surface of a liquid, some of the forces of
SURFACE TENSION
On the surface of a liquid, some of the forces of
Слайд 31THE ANESTHESIA MACHINE
Tension in the wall of the bag equals Pressure x
THE ANESTHESIA MACHINE
Tension in the wall of the bag equals Pressure x
Слайд 32BERNOULLI PRINCIPLE
Fall in pressure at a narrowing of a tube
Gas/Fluid has potential
BERNOULLI PRINCIPLE
Fall in pressure at a narrowing of a tube
Gas/Fluid has potential
Слайд 33BERNOULLI PRINCIPLE
Therefore decrease in potential energy
If this pressure falls below atmospheric pressure,
BERNOULLI PRINCIPLE
Therefore decrease in potential energy
If this pressure falls below atmospheric pressure,
Слайд 34THE GAS LAWS
Boyles Law
Charles Law
Third Perfect Gas Law
Dalton’s Law of Partial Pressures
Universal
THE GAS LAWS
Boyles Law
Charles Law
Third Perfect Gas Law
Dalton’s Law of Partial Pressures
Universal
Слайд 35BOYLES LAW
At constant temp, V ∞ 1/P
How much oxygen is available at
BOYLES LAW
At constant temp, V ∞ 1/P
How much oxygen is available at
Слайд 36CHARLES LAW
At constant pressure, V∞Temp
Gases expand when heated
CHARLES LAW
At constant pressure, V∞Temp
Gases expand when heated
Слайд 37THIRD PERFECT GAS LAW
At constant volume, P ∞ Temp
STP – 273.15K and
THIRD PERFECT GAS LAW
At constant volume, P ∞ Temp
STP – 273.15K and
Слайд 38ADIABATIC CHANGE
The three gas laws describe the behaviour of a gas when
ADIABATIC CHANGE
The three gas laws describe the behaviour of a gas when
Слайд 39ADIABATIC CHANGE
The state of a gas can be altered without allowing the
ADIABATIC CHANGE
The state of a gas can be altered without allowing the
Слайд 40ADIABATIC CHANGE
Thus, the gas is compressed adiabatically and a large temp rise
ADIABATIC CHANGE
Thus, the gas is compressed adiabatically and a large temp rise
Слайд 41DALTON’S LAW OF PARTIAL PRESSURES
In a mixture of gases, the pressure exerted
DALTON’S LAW OF PARTIAL PRESSURES
In a mixture of gases, the pressure exerted
Слайд 42AVOGADRO’S NUMBER
States that equal volumes of gases at the same temp and
AVOGADRO’S NUMBER
States that equal volumes of gases at the same temp and
Слайд 43BREATHING SYSTEMS
Breathing Circuitsa)Open (non-rebreathing) •Simple face mask or nasal cannula (CO2 diffuses
BREATHING SYSTEMS
Breathing Circuitsa)Open (non-rebreathing) •Simple face mask or nasal cannula (CO2 diffuses
Слайд 44AVOGADRO’S NUMBER
Typical Nitrous cylinder has 3.4kg of Nitrous Oxide
Molec wt = 44
AVOGADRO’S NUMBER
Typical Nitrous cylinder has 3.4kg of Nitrous Oxide
Molec wt = 44
Слайд 45UNIVERSAL GAS CONSTANT
PV = nRT
In a cylinder, the volume and temp is
UNIVERSAL GAS CONSTANT
PV = nRT
In a cylinder, the volume and temp is
Слайд 46CRITICAL TEMP
Defined as the temp above which a substance cannot be liquefied
CRITICAL TEMP
Defined as the temp above which a substance cannot be liquefied
Слайд 47CRITICAL TEMP
Critical temp for oxygen is -119 degrees
Impossible to turn oxygen into
CRITICAL TEMP
Critical temp for oxygen is -119 degrees
Impossible to turn oxygen into
Слайд 48SOLUBILITY
When a liquid is placed in a closed container, an equilibrium is
SOLUBILITY
When a liquid is placed in a closed container, an equilibrium is
Слайд 49SOLUBILITY
Saturated Vapour Pressure
Henry’s Law – states that at a particular temp, the
SOLUBILITY
Saturated Vapour Pressure
Henry’s Law – states that at a particular temp, the
Слайд 50SOLUBILITY
The effect of high pressure on the solubility of nitrogen is particularly
SOLUBILITY
The effect of high pressure on the solubility of nitrogen is particularly
Слайд 51SOLUBILITY
Ostwald Solubility Coefficient is the volume of gas which dissolves in one
SOLUBILITY
Ostwald Solubility Coefficient is the volume of gas which dissolves in one
Слайд 52SOLUBILITY
Partition Coefficient is defined as the ratio of the amount of substance
SOLUBILITY
Partition Coefficient is defined as the ratio of the amount of substance
Слайд 53SOLUBILITY
Ether has the highest Ostwald Solubility Coefficient (12). Halothane is 2.3 and
SOLUBILITY
Ether has the highest Ostwald Solubility Coefficient (12). Halothane is 2.3 and
Слайд 54SOLUBILITY
Second Gas effect
Diffusion hypoxia
SOLUBILITY
Second Gas effect
Diffusion hypoxia
Слайд 55SECOND GAS EFFECT
During the inspiration of a gas mixture containing nitrous oxide,
SECOND GAS EFFECT
During the inspiration of a gas mixture containing nitrous oxide,
Слайд 56DIFFUSION HYPOXIA
At the end of an anesthetic using N2O, the N2O diffuses
DIFFUSION HYPOXIA
At the end of an anesthetic using N2O, the N2O diffuses
Слайд 57SOLUBILITY
Fat is an impt constituent of tissue
Oil is therefore used for measurements
Agents
SOLUBILITY
Fat is an impt constituent of tissue
Oil is therefore used for measurements
Agents
Слайд 58SOLUBILITY
High solubility = lower MAC values
Anesthetics tend to interfere with the molecular
SOLUBILITY
High solubility = lower MAC values
Anesthetics tend to interfere with the molecular
Слайд 59SOLUBILITY
Also attach to the long carbon chain molecules present in rubber and
SOLUBILITY
Also attach to the long carbon chain molecules present in rubber and
Слайд 60DIFFUSION AND OSMOSIS
Diffusion is the process by which the molecules of a
DIFFUSION AND OSMOSIS
Diffusion is the process by which the molecules of a
Слайд 61DIFFUSION
Pulmonary Diffusing Capacity
Rate at which CO leaves the alveoli is dependent on
DIFFUSION
Pulmonary Diffusing Capacity
Rate at which CO leaves the alveoli is dependent on
Слайд 62EFFECT OF MOLECULAR SIZE
Grahams Law states that the rate of diffusion of
EFFECT OF MOLECULAR SIZE
Grahams Law states that the rate of diffusion of
Слайд 63OSMOLARITY
Is the sum total of the molarities of the solutes in a
OSMOLARITY
Is the sum total of the molarities of the solutes in a
Слайд 64OSMOLARITY
If a patient is transfused hypotonic fluids – get changes in the
OSMOLARITY
If a patient is transfused hypotonic fluids – get changes in the
Слайд 65OSMOLARITY
Number of osmoles per kg of water or clear solution
Avoids the effect
OSMOLARITY
Number of osmoles per kg of water or clear solution
Avoids the effect
Слайд 66HEAT CAPACITY
Specific Heat Capacity is defined as the amount of heat required
HEAT CAPACITY
Specific Heat Capacity is defined as the amount of heat required
Слайд 67HEAT CAPACITY
Body temp = 36 degrees
Shivers – increases heat production 4 fold
HEAT CAPACITY
Body temp = 36 degrees
Shivers – increases heat production 4 fold
Слайд 68HEAT CAPACITY
This patient will need to shiver for 17 minutes to produce
HEAT CAPACITY
This patient will need to shiver for 17 minutes to produce
Слайд 69HEAT CAPACITY
Specific Heat Capacity of blood = 3.6kJ/kg/C
Transfuse 2L of blood at
HEAT CAPACITY
Specific Heat Capacity of blood = 3.6kJ/kg/C
Transfuse 2L of blood at
Слайд 70HEAT CAPACITY
Heat Required = 216kJ (2x3.6x30)
Heat Capacity of 70kg person = 245kJ/C
Therefore
HEAT CAPACITY
Heat Required = 216kJ (2x3.6x30)
Heat Capacity of 70kg person = 245kJ/C
Therefore
Слайд 71THE ANESTHESIA MACHINE
THE ANESTHESIA MACHINE
Слайд 72THE ANESTHESIA MACHINE
N2O is stored in the tank as a liquid in
THE ANESTHESIA MACHINE
N2O is stored in the tank as a liquid in
Слайд 73THE ANESTHESIA MACHINE
Why does the pressure go down as the gas cools?
THE ANESTHESIA MACHINE
Why does the pressure go down as the gas cools?
Слайд 74THE ANESTHESIA MACHINE
The pressure in the tank reflects the force of the
THE ANESTHESIA MACHINE
The pressure in the tank reflects the force of the
Слайд 75THE ANESTHESIA MACHINE
Thermal energy is taken out of the nitrous tank by
THE ANESTHESIA MACHINE
Thermal energy is taken out of the nitrous tank by
Слайд 76THE ANESTHESIA MACHINE
As oxygen is drawn from the tank, both the temp
THE ANESTHESIA MACHINE
As oxygen is drawn from the tank, both the temp
Слайд 77CIRCULATION
Ohm’s Law
Pressure = Flow x Resistance
Voltage = Current x Resistance
Resistance = Pressure/Flow
CIRCULATION
Ohm’s Law
Pressure = Flow x Resistance
Voltage = Current x Resistance
Resistance = Pressure/Flow
Слайд 78CIRCULATION
SVR = (MAP – CVP)/CO
Poiseulle’s equation – Resistance to flow is proportional
CIRCULATION
SVR = (MAP – CVP)/CO
Poiseulle’s equation – Resistance to flow is proportional
Слайд 79CIRCULATION
P = 2T/R
Failing heart – Increase in R and therefore a decrease
CIRCULATION
P = 2T/R
Failing heart – Increase in R and therefore a decrease
Слайд 80CIRCULATION
MAP dependent on SVR and CO
Patient with a decreased SVR, a high
CIRCULATION
MAP dependent on SVR and CO
Patient with a decreased SVR, a high
Слайд 81AUSCULTATORY METHOD
Based on the Korotkoff sounds
The systolic and diastolic pressures are determined
AUSCULTATORY METHOD
Based on the Korotkoff sounds
The systolic and diastolic pressures are determined
Слайд 82OSCILLOMETRIC METHOD
Based on pressure waveform in an air filled cuff coupled to
OSCILLOMETRIC METHOD
Based on pressure waveform in an air filled cuff coupled to
Слайд 83INVASIVE MONITORING
Transducer is a strain gauge that linearly converts pressure to electrical
INVASIVE MONITORING
Transducer is a strain gauge that linearly converts pressure to electrical
Слайд 84INVASIVE MONITORING
Strain Gauge – movements of the diaphragm alter the tension in
INVASIVE MONITORING
Strain Gauge – movements of the diaphragm alter the tension in
Слайд 85INVASIVE MONITORING
Wheatstone Bridge
4 resistors, a source and a galvanometer
Variable resistor can be
INVASIVE MONITORING
Wheatstone Bridge
4 resistors, a source and a galvanometer
Variable resistor can be
Слайд 86INVASIVE MONITORING
What does it mean to “zero” the transducer?
INVASIVE MONITORING
What does it mean to “zero” the transducer?
Слайд 87INVASIVE MONITORING
The act of zeroing the transducer tells the monitor the electrical
INVASIVE MONITORING
The act of zeroing the transducer tells the monitor the electrical
Слайд 88INVASIVE MONITORING
Column of water between the point that is opened to air
INVASIVE MONITORING
Column of water between the point that is opened to air
Слайд 89CARDIAC OUTPUT
Gold standard for measuring cardiac output is by applying Fick’s Law
CARDIAC OUTPUT
Gold standard for measuring cardiac output is by applying Fick’s Law
Слайд 90PULSE OXIMETRY
Beer Lambert Law
Absorption of light = Concentration x Thickness x extinction
PULSE OXIMETRY
Beer Lambert Law
Absorption of light = Concentration x Thickness x extinction
Слайд 91PULSE OXIMETRY
Beer’s Law states that the absorption of radiation by a given
PULSE OXIMETRY
Beer’s Law states that the absorption of radiation by a given
Слайд 92PULSE OXIMETRY
Lambert’s Law states that each layer of equal thickness absorbs an
PULSE OXIMETRY
Lambert’s Law states that each layer of equal thickness absorbs an
Слайд 93PULSE OXIMETRY
The diodes alternate at about 100 times a second between 660nm,
PULSE OXIMETRY
The diodes alternate at about 100 times a second between 660nm,
Слайд 94PULSE OXIMETRY
Two parts to the waveform
- static component which represents the
PULSE OXIMETRY
Two parts to the waveform
- static component which represents the
Слайд 95PULSE OXIMETRY
On the assumption that the tissue thickness is the same for
PULSE OXIMETRY
On the assumption that the tissue thickness is the same for
Слайд 96PULSE OXIMETRY
PULSE OXIMETRY
Слайд 97PULSE OXIMETRY
Unable to distinguish more that two types of Hb
Cannot identify carboxyHb
PULSE OXIMETRY
Unable to distinguish more that two types of Hb
Cannot identify carboxyHb
Слайд 98ELECTRICAL SAFETY
Two major hazards
- burns
- arrhythmias
ELECTRICAL SAFETY
Two major hazards
- burns
- arrhythmias
Слайд 99ELECTRICAL SAFETY
Three types of electrical current
- macroshock
- microshock
-
ELECTRICAL SAFETY
Three types of electrical current
- macroshock
- microshock
-
Слайд 100ELECTRICAL SAFETY
A power station supplies electricity at very high voltage to a
ELECTRICAL SAFETY
A power station supplies electricity at very high voltage to a
Слайд 101ELECTRICAL SAFETY
Third conductor is connected to earth at the hospital.
If a person
ELECTRICAL SAFETY
Third conductor is connected to earth at the hospital.
If a person
Слайд 102ELECTRICAL SAFETY
1 mA = tingling sensation on touching the live parts of
ELECTRICAL SAFETY
1 mA = tingling sensation on touching the live parts of
Слайд 103ELECTRICAL SAFETY
If you are wearing non standard footwear and standing in a
ELECTRICAL SAFETY
If you are wearing non standard footwear and standing in a
Слайд 104ELECTRICAL SAFETY
Most of the impedence now occurs at the points of contact
ELECTRICAL SAFETY
Most of the impedence now occurs at the points of contact
Слайд 105ELECTRICAL SAFETY
Risk of VF
Risk is much greater if the current passes through
ELECTRICAL SAFETY
Risk of VF
Risk is much greater if the current passes through
Слайд 106CLASS 1 EQUIPMENT
Any conducting part that is accessible to the user, such
CLASS 1 EQUIPMENT
Any conducting part that is accessible to the user, such
Слайд 107CLASS 2
Double insulated equipment
All accessible parts are protected by 2 layers of
CLASS 2
Double insulated equipment
All accessible parts are protected by 2 layers of
Слайд 108CLASS 3
Internally powered equipment
Has its own power source located within the equipment
Although
CLASS 3
Internally powered equipment
Has its own power source located within the equipment
Although
Слайд 109ISOLATED PATIENT CIRCUITS
Some equipment requires electrical connections be made to the patient
ISOLATED PATIENT CIRCUITS
Some equipment requires electrical connections be made to the patient
Слайд 110ISOLATED PATIENT CIRCUITS
To counteract this, use an isolated patient circuit or a
ISOLATED PATIENT CIRCUITS
To counteract this, use an isolated patient circuit or a

Слайд 111ISOLATED PATIENT CIRCUIT
Intended to provide protection should a fault develop in the
ISOLATED PATIENT CIRCUIT
Intended to provide protection should a fault develop in the
Слайд 112LEAKAGE CURRENT STANDARDS
Electromedical equipment is classified according to the maximum leakage current
LEAKAGE CURRENT STANDARDS
Electromedical equipment is classified according to the maximum leakage current
Слайд 113LEAKAGE CURRENT STANDARDS
B or BF it it has a floating circuit. Leakage
LEAKAGE CURRENT STANDARDS
B or BF it it has a floating circuit. Leakage
Слайд 114ELECTRICAL SAFETY
Electrical currents flow in circuits
A path must exist from the electrical
ELECTRICAL SAFETY
Electrical currents flow in circuits
A path must exist from the electrical
Слайд 115ELECTRICAL SAFETY
Standardized voltage is about 120V
The “120” is the root mean square
ELECTRICAL SAFETY
Standardized voltage is about 120V
The “120” is the root mean square
Слайд 116ROOT MEAN SQUARE
If all the values of the sine wave are squared,
ROOT MEAN SQUARE
If all the values of the sine wave are squared,
Слайд 117MACROSHOCK
Potential for both burns and arrhythmias
Current must flow through the thorax
In the
MACROSHOCK
Potential for both burns and arrhythmias
Current must flow through the thorax
In the
Слайд 118MACROSHOCK- FACTORS FOR ELECTROCUTION
Patient unclothed and wet
Patient is on a large metal
MACROSHOCK- FACTORS FOR ELECTROCUTION
Patient unclothed and wet
Patient is on a large metal
Слайд 119MACROSHOCK
How much current can we deliver to the anesthetized patient?
MACROSHOCK
How much current can we deliver to the anesthetized patient?
Слайд 120MACROSHOCK
Patient may receive 150 volts with direct contact
The current he receives will
MACROSHOCK
Patient may receive 150 volts with direct contact
The current he receives will
Слайд 121MACROSHOCK
Current required to produce VF is 80mA
Therefore 3mA will not cause VF
Resistance
MACROSHOCK
Current required to produce VF is 80mA
Therefore 3mA will not cause VF
Resistance
Слайд 122MACROSHOCK
What is the voltage required to produce an 80mA current across wet
MACROSHOCK
What is the voltage required to produce an 80mA current across wet
Слайд 123MACROSHOCK
How could a patient come into contact with 40 volts in the
MACROSHOCK
How could a patient come into contact with 40 volts in the
Слайд 124MACROSHOCK
MACROSHOCK
Слайд 125MACROSHOCK
Hot and neutral leads power the device
Ground lead connects to the chassis
MACROSHOCK
Hot and neutral leads power the device
Ground lead connects to the chassis
Слайд 126MACROSHOCK
MACROSHOCK
Слайд 127MACROSHOCK
To avoid helping electrocute the patient, no properly functioning modern monitoring device
MACROSHOCK
To avoid helping electrocute the patient, no properly functioning modern monitoring device
Слайд 128MACROSHOCK
Equipment must be designed so the the hot wire cannot easily short
MACROSHOCK
Equipment must be designed so the the hot wire cannot easily short
Слайд 129LINE ISOLATION TRANSFORMER
Simple device that prevents a circuit from being completed by
LINE ISOLATION TRANSFORMER
Simple device that prevents a circuit from being completed by
Слайд 130LINE ISOLATION TRANSFORMER
LINE ISOLATION TRANSFORMER
Слайд 131LINE ISOLATION TRANSFORMER
How do you monitor a line isolation transformer to see
LINE ISOLATION TRANSFORMER
How do you monitor a line isolation transformer to see
Слайд 132LINE ISOLATION TRANSFORMER
LINE ISOLATION TRANSFORMER
Слайд 133LINE ISOLATION MONITOR
Resistor has a resistance of about 150 000 ohm’s so
LINE ISOLATION MONITOR
Resistor has a resistance of about 150 000 ohm’s so
Слайд 134MICROSHOCK
Refers to currents delivered directly to the myocardium via intracardiac electrodes or
MICROSHOCK
Refers to currents delivered directly to the myocardium via intracardiac electrodes or
Слайд 135MICROSHOCK
How much safety does the isolation transformer provide against microshock hazard?
MICROSHOCK
How much safety does the isolation transformer provide against microshock hazard?
Слайд 136MICROSHOCK
Ground wire should be intact
LIM signals a warning if the resistance between
MICROSHOCK
Ground wire should be intact
LIM signals a warning if the resistance between
Слайд 137MICROSHOCK
In the presence of a LIM, it takes two shorts to the
MICROSHOCK
In the presence of a LIM, it takes two shorts to the
Слайд 138ELECTROCAUTERY
Current density = current flow per unit area
Explains the heating effect of
ELECTROCAUTERY
Current density = current flow per unit area
Explains the heating effect of
Слайд 139ELECTROCAUTERY
These effects become less as the frequency of the current increases being
ELECTROCAUTERY
These effects become less as the frequency of the current increases being
Слайд 140ELECTROCAUTERY
Electrosurgical equipment is used to pass a current of a high frequency
ELECTROCAUTERY
Electrosurgical equipment is used to pass a current of a high frequency
Слайд 141ELECTROCAUTERY
Two connections – neutral or patient plate and the active or cutting
ELECTROCAUTERY
Two connections – neutral or patient plate and the active or cutting
Слайд 142ELECTROCAUTERY
If the neutral plate is not properly applied, the area of contact
ELECTROCAUTERY
If the neutral plate is not properly applied, the area of contact
Слайд 143ELECTROCAUTERY
Current density can reach a hazardous value when the electrosurgical current flows
ELECTROCAUTERY
Current density can reach a hazardous value when the electrosurgical current flows
Слайд 144ELECTROCAUTERY
Frequencies of 500 00- to 2000 000 Hz are used by electrocautery
Too
ELECTROCAUTERY
Frequencies of 500 00- to 2000 000 Hz are used by electrocautery
Too
Слайд 145ELECTROCAUTERY
The grounding plate does not ground the patient to ground
It is the
ELECTROCAUTERY
The grounding plate does not ground the patient to ground
It is the
Слайд 146CAPACITANCE
Is a measure of the ability of an object to hold electric
CAPACITANCE
Is a measure of the ability of an object to hold electric
Слайд 147DEFIBRILLATOR
Is an example of an instrument in which electric charge is stored
DEFIBRILLATOR
Is an example of an instrument in which electric charge is stored
Слайд 148BREATHING SYSTEMS
Open (non-rebreathing)
Simple face mask or nasal cannula (CO2 diffuses away
BREATHING SYSTEMS
Open (non-rebreathing)
Simple face mask or nasal cannula (CO2 diffuses away
Слайд 149BREATHING SYSTEMS
Semi-Open (Mapleson / Bain)
Most efficient removal of CO2 for a given
BREATHING SYSTEMS
Semi-Open (Mapleson / Bain)
Most efficient removal of CO2 for a given
Слайд 150BREATHING SYSTEMS
However, the "A" system is very inefficient (requires high gas flows)
BREATHING SYSTEMS
However, the "A" system is very inefficient (requires high gas flows)
Слайд 151BREATHING SYSTEMS
Semi Closed Circle System
Patient gas uptake < fresh gas flow <
BREATHING SYSTEMS
Semi Closed Circle System
Patient gas uptake < fresh gas flow <
Слайд 152BREATHING SYSTEMS
Closed System
Gas inflow = Patient Uptake
If using sidestream agent
BREATHING SYSTEMS
Closed System
Gas inflow = Patient Uptake
If using sidestream agent
Слайд 153CO2 ABSORPTION
CO2 Absorption Granules
Small enough to have large surface area but
CO2 ABSORPTION
CO2 Absorption Granules
Small enough to have large surface area but
Слайд 154CO2 ABSORPTION
Composition
Sodalime: NaOH, Ca(OH)2
Baralyme: KOH, Ca(OH)2, Ba(OH)2 -More likely to react
CO2 ABSORPTION
Composition
Sodalime: NaOH, Ca(OH)2
Baralyme: KOH, Ca(OH)2, Ba(OH)2 -More likely to react
 Работа - как жизненный путь
Работа - как жизненный путь Психологическая структура осознанной саморегуляции студентов разных типов специальностей
Психологическая структура осознанной саморегуляции студентов разных типов специальностей К уроку ИЗО 7 класс Учитель ИЗО Тумахович З.Г.
К уроку ИЗО 7 класс Учитель ИЗО Тумахович З.Г. Технология установки дверного замка
Технология установки дверного замка «Художественная культура 60-90-х гг. XIX в.».
«Художественная культура 60-90-х гг. XIX в.». Ядерное оружие
Ядерное оружие Презентация по математике на тему _Обыкновенные дроби_ (5 класс)
Презентация по математике на тему _Обыкновенные дроби_ (5 класс) Физические и механические свойства древесины
Физические и механические свойства древесины Процесс изготовления монет
Процесс изготовления монет Лечение рака толстой кишки
Лечение рака толстой кишки Презентация на тему Музыкальные шедевры П.И. Чайковского на уроках литературы
Презентация на тему Музыкальные шедевры П.И. Чайковского на уроках литературы  Julia Smirnova. Сделайте жизнь ярче
Julia Smirnova. Сделайте жизнь ярче Особенности природы региона
Особенности природы региона Универсальный ледовый спортивно-концертный комплекс в городе Туймазы
Универсальный ледовый спортивно-концертный комплекс в городе Туймазы Svadebnye_i_pokhoronye_plachi_i_prichitania
Svadebnye_i_pokhoronye_plachi_i_prichitania Тайна острова Пасхи
Тайна острова Пасхи Изображение головы
Изображение головы Длина окружности и площадь круга
Длина окружности и площадь круга Основы инфокоммуникационных технологийБлок 2: Сетевые модели
Основы инфокоммуникационных технологийБлок 2: Сетевые модели Презентация на тему Зимние забавы
Презентация на тему Зимние забавы Взаимодействие учителя и ученика как средство развития коммуникативной и языковой компетенций
Взаимодействие учителя и ученика как средство развития коммуникативной и языковой компетенций архитектор
архитектор Многообразие пресмыкающихся
Многообразие пресмыкающихся Коннекторы (2020)
Коннекторы (2020) развития речи
развития речи Презентация на тему Млекопитающие
Презентация на тему Млекопитающие Основы соционики
Основы соционики ASBIS Россия 2009
ASBIS Россия 2009