- Thyroid gland diseases

Содержание
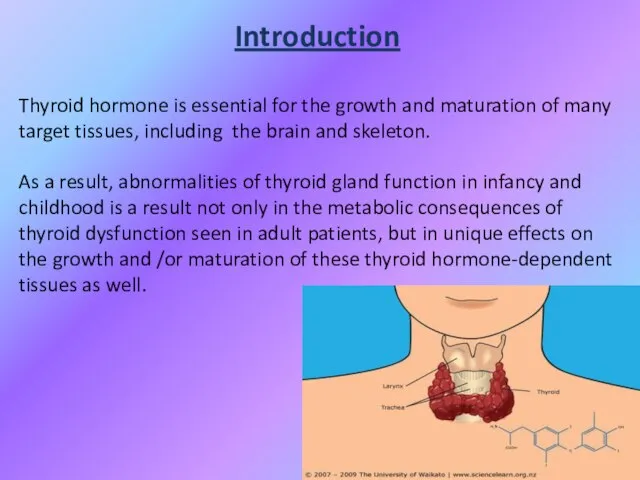
- 3. Introduction Thyroid hormone is essential for the growth and maturation of many target tissues, including the
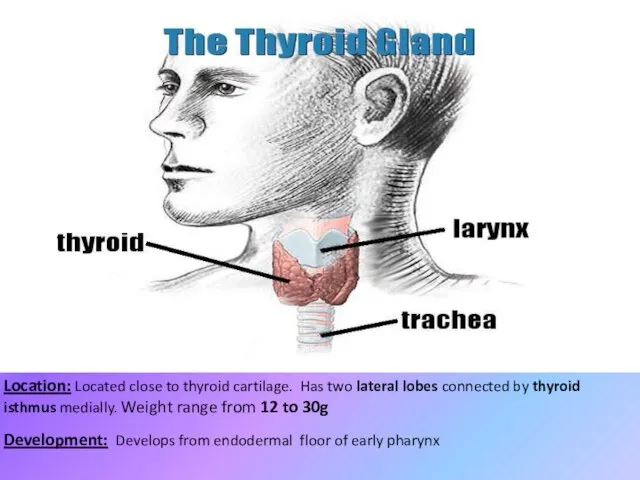
- 4. Location: Located close to thyroid cartilage. Has two lateral lobes connected by thyroid isthmus medially. Weight
- 7. Thyroid Physiology
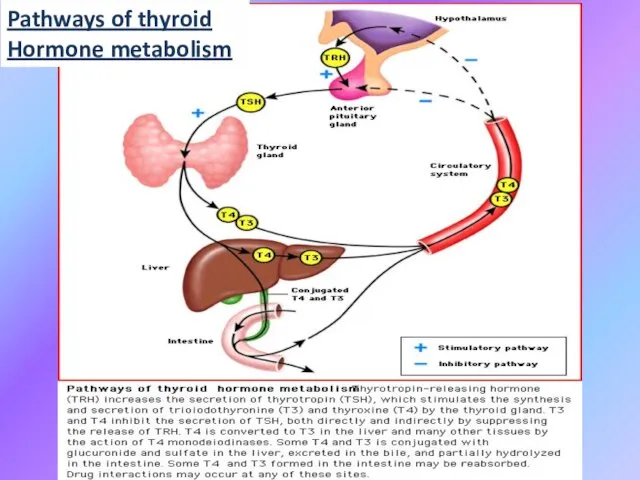
- 8. Pathways of thyroid Hormone metabolism
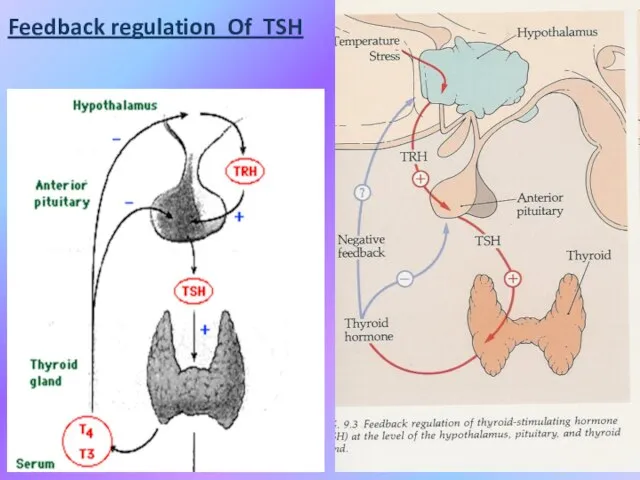
- 9. Feedback regulation Of TSH
- 10. Thyroid physiology, continuation
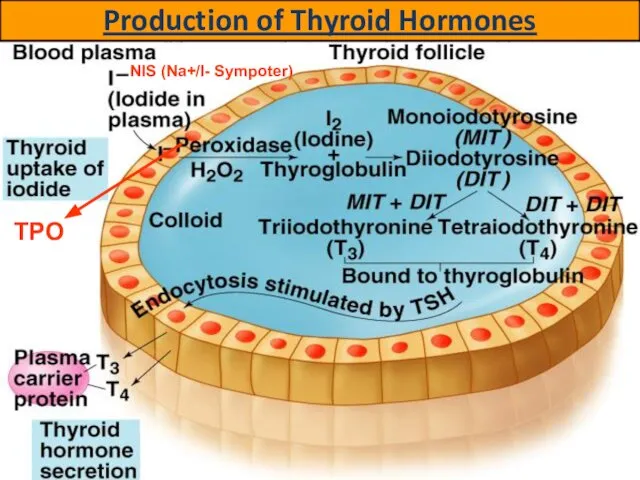
- 11. Production of Thyroid Hormones NIS (Na+/I- Sympoter) TPO
- 12. Thyroid Hormone Majority of circulating hormone is T4 (98,5% T4, 1,5% T3 ) Total Hormone load
- 13. Effects of thyroid hormones Fetal brain and skeletal maturation; Increase in basal metabolic rate; Inotropic and
- 14. Thyroid hormones
- 15. Comparative analysis of thyroid hormones
- 16. THYROTOXICOSIS (Hyperthyroidism) Overproduction of thyroid hormones; HYPOTHYROIDISM (Gland destruction) Underproduction of thyroid hormones; NEOPLASTIC PROCESSES Benign;
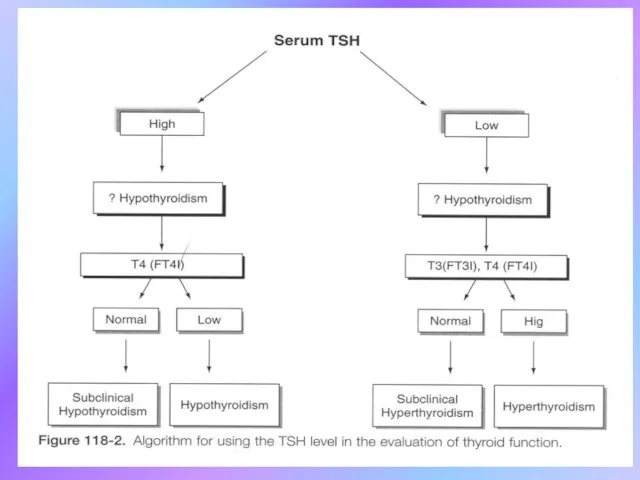
- 17. Diagnostic of Thyroid gland disease
- 18. LABORATORY EVALUATION TSH (thyroid-stimulating hormone) normal, practically excludes abnormality
- 19. High TSH usually means Hypothyroidism Rare causes: TSH-secreting pituitary tumor; Thyroid hormone resistance; Assay artifact. Low
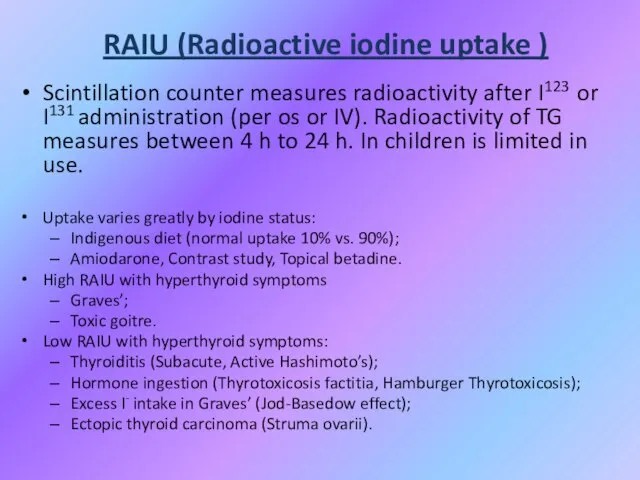
- 21. RAIU (Radioactive iodine uptake ) Scintillation counter measures radioactivity after I123 or I131 administration (per os
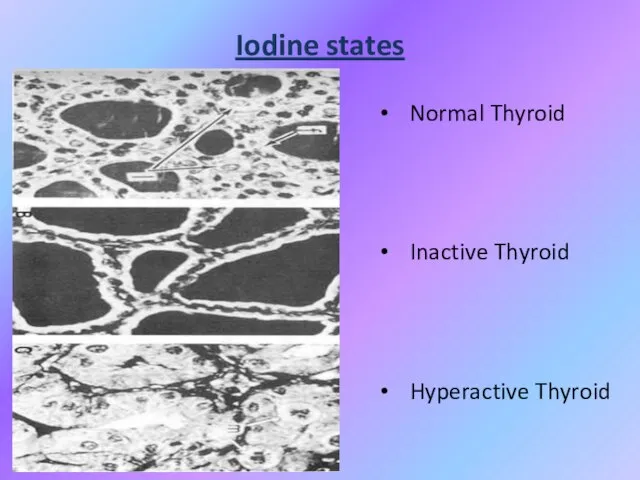
- 22. Iodine states Normal Thyroid Inactive Thyroid Hyperactive Thyroid
- 23. Thyrotoxicosis Primary; Secondary; Without Hyperthyroidism; Exogenous or factitious. Hypothyroidism Primary; Secondary; Peripheral.
- 24. HYPERTHYROIDISM or THYROTOXICOSIS: - is the result of excessive thyroid gland function because is defined as
- 25. Primary Hyperthyroidism: Graves’; Toxic Multinodular Goitre; Toxic adenoma; Functioning thyroid carcinoma metastases; Activating mutation of TSH
- 26. Causes of Thyrotoxicosis: Thyrotoxicosis without hyperthyroidism: Subacute thyroiditis; Silent thyroiditis; Other causes of thyroid destruction: Amiodarone,
- 27. Symptoms of Hyperthyroidism Heat intolerance, dislike of hot weather; Hyperactivity, irritability, nervousness, fatigue; Weight loss (normal
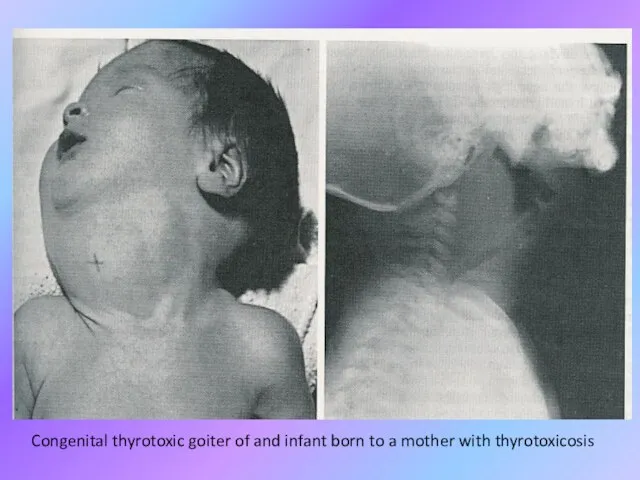
- 28. Causes of Transient Neonatal Hyperthyroidism Neonatal hyperthyroidism is almost always transient and results from the transplacental
- 29. Situations That Should Prompt Consideration of Neonatal Hyperthyroidism: ● Unexplained tachycardia, goitre or stare; ● Unexplained
- 30. Congenital thyrotoxic goiter of and infant born to a mother with thyrotoxicosis
- 31. Therapy of Transient neonatal hyperthyroidism Treatment is accomplished by maternal administration of antithyroid medication in fetus.
- 32. Therapy of Transient neonatal hyperthyroidism In the neonate, treatment is the follows: either PTU (5 to10
- 33. Therapy of Transient neonatal hyperthyroidism Propranolol (2 mg/kg/day in 2 or 3 divided doses) is added
- 34. Permanent neonatal hyperthyroidism Rarely, neonatal hyperthyroidism is inconvertible and is due to a germline mutation in
- 35. Permanent neonatal hyperthyroidism Early recognition is important because the thyroid function of affected infants is frequently
- 37. Goitre Endemic goitre: Areas where > 5% of children 6-12 years old have goiter Common in
- 38. Goitre Etiology Hashimoto’s thyroiditis: Early stages only, late stages show atrophic changes; May present with hypo,
- 39. Goitre
- 40. Classification of Goitre WHO (1994) 0 – goitre is absent; I – goitre isn’t visualized, but
- 41. Functional condition of Thyroid influence may be as Euthyroidism; Hypothyroidism; Hyperthyroidism.
- 42. Non-Toxic Goitre Cancer screening in non-toxic MNG (Multinodular goitre ) Longstanding MNG has a risk of
- 43. Non-Toxic Goitre Treatment options (no compressive symptoms): Use follow-up to monitor for progression; Thyroid suppression therapy:
- 44. Non-Toxic Goitre Treatment options (compressive symptoms): Radioactive iodine (RAI) ablation: Volume reduction 33% - 66% in
- 45. Toxic Goitre Treatment for Toxic MNG: Thionamide medications: Not indicated for long-term use due to complications;
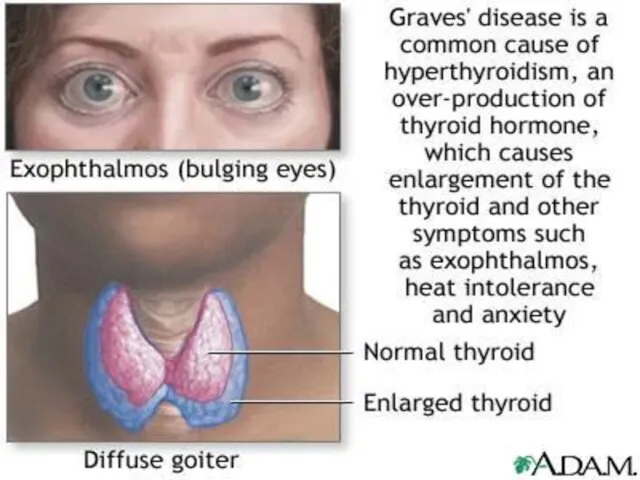
- 46. Graves’ Disease Diffuse toxic goitre is an autoimmune pathology with prolonged elevation T3 and T4 and
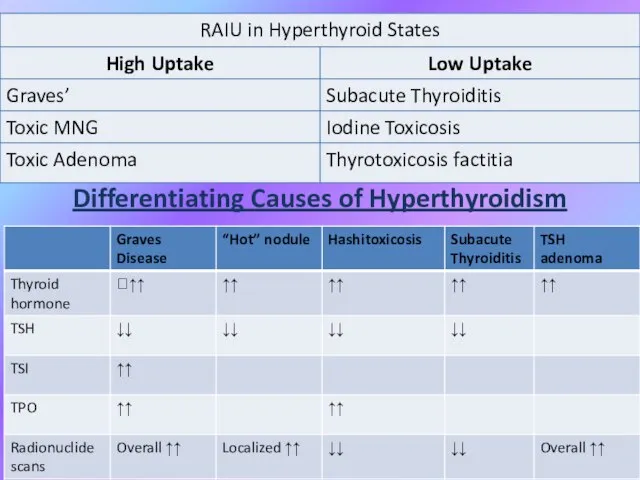
- 48. Differentiating Causes of Hyperthyroidism
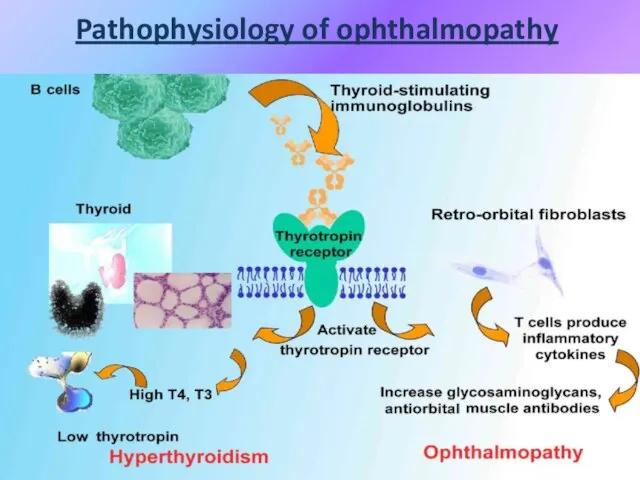
- 49. Pathophysiology of ophthalmopathy
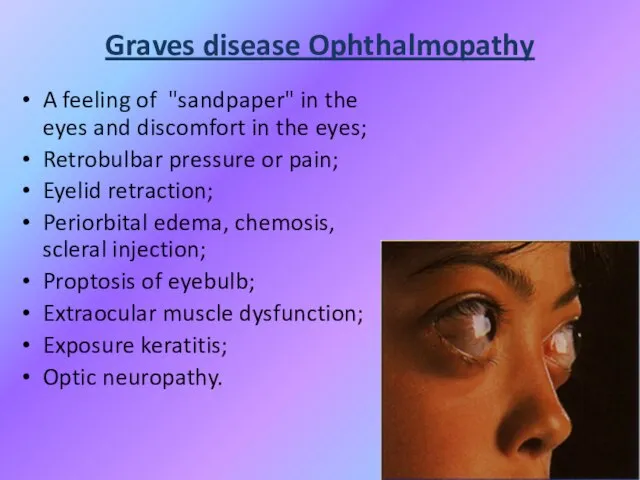
- 50. Graves disease Ophthalmopathy A feeling of "sandpaper" in the eyes and discomfort in the eyes; Retrobulbar
- 51. Graves Disease: Treatment • Medications: – Beta-blockers for symptoms – can be discontinued as thyroid function
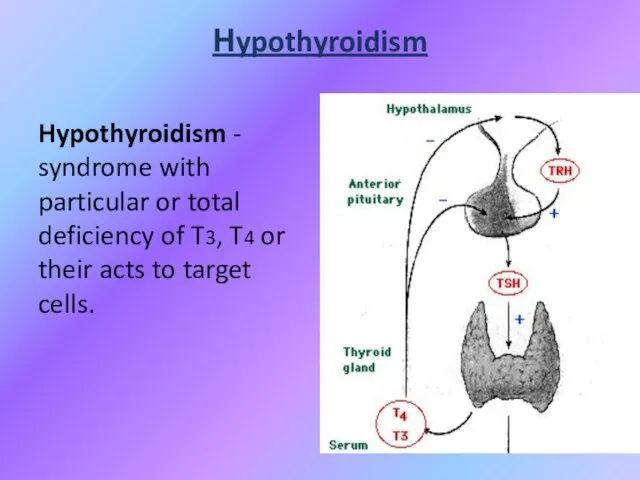
- 52. Нypothyroidism Hypothyroidism - syndrome with particular or total deficiency of T3, T4 or their acts to
- 53. Classification of hypothyroidism PRIMARY - defects of biosynthesis of T3, T4 due to pathology of thyroid
- 54. Primary: Autoimmune (Hashimoto´s); Iatrogenic Surgery or 131I administration; Drugs: amiodarone, lithium; Congenital (1 in 3000 to
- 55. Secondary: Pituitary gland destruction; Isolated TSH deficiency; Bexarotene treatment; Hypothalamic disorders. Peripheral: Rare, familial tendency.
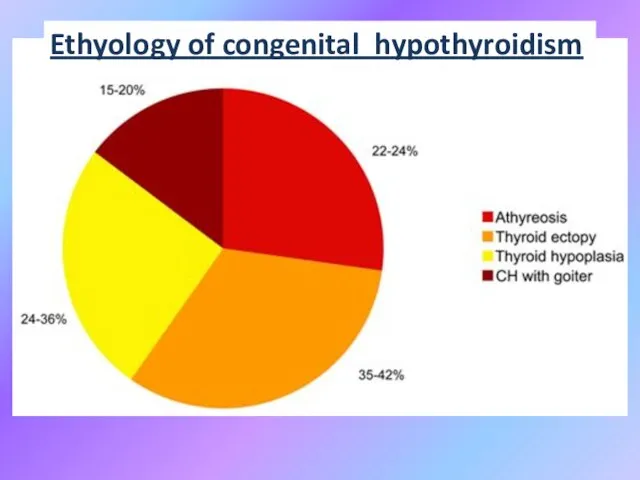
- 56. Ethyology of congenital hypothyroidism
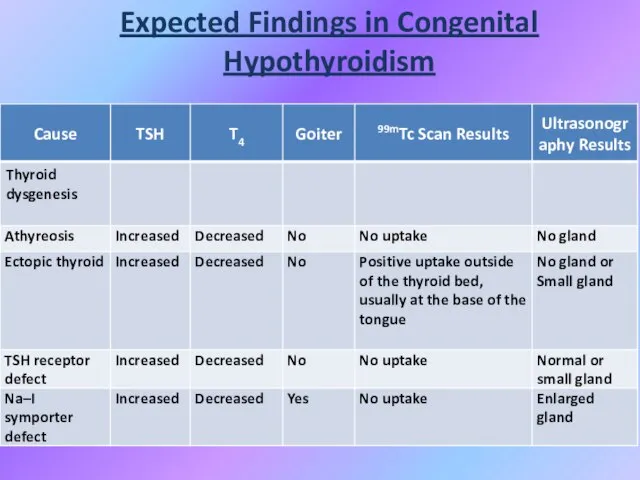
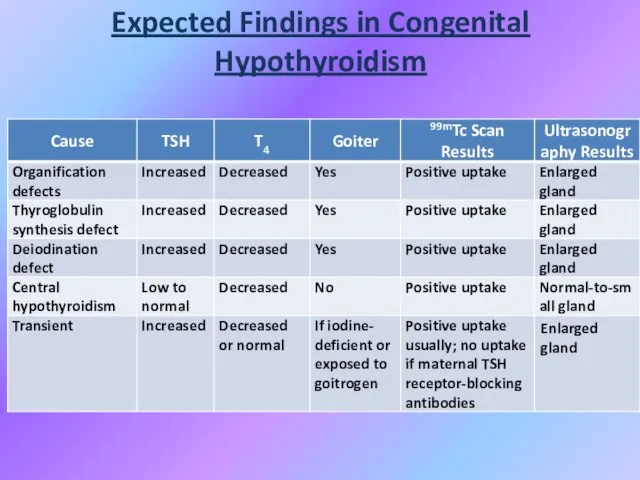
- 57. Expected Findings in Congenital Hypothyroidism
- 58. Expected Findings in Congenital Hypothyroidism
- 59. Congenital hypothyroidism Agenesis (no goiter) or dysgenesis ( aplasia, hypoplasia, ectopic gland) are the most common
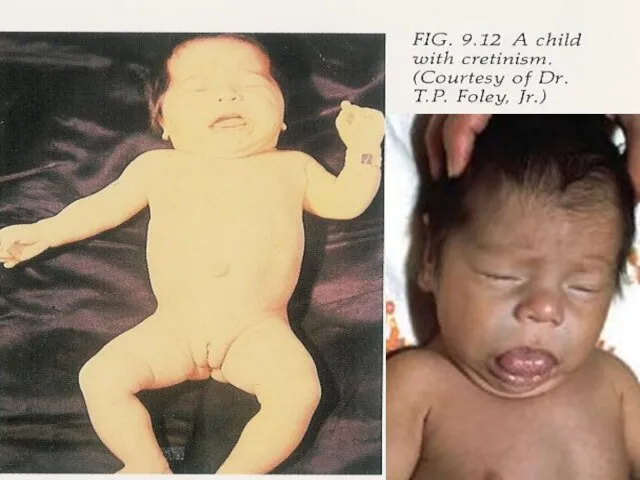
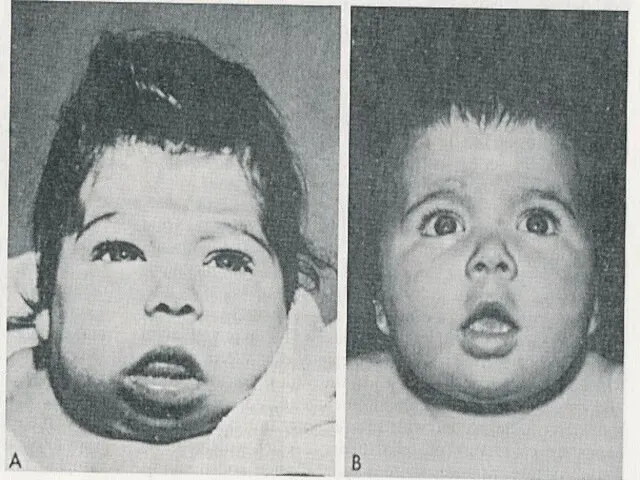
- 60. Congenital hypothyroidism Clinical features Coarse facial features, dry skin, prolonged jaundice, large fontanelles, posterior fontanell >
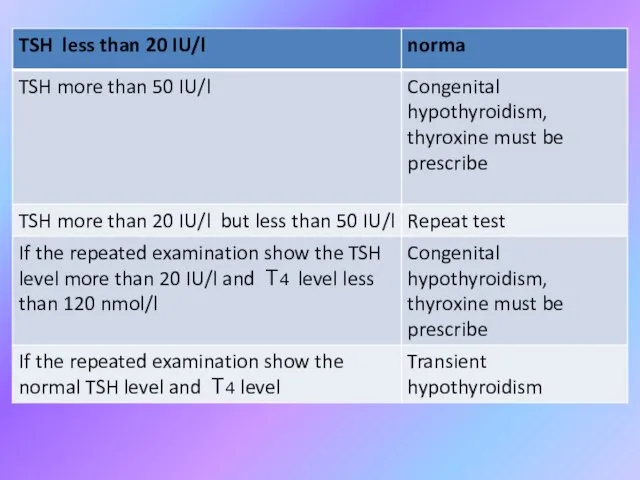
- 63. Hypothyroidism Screening in the Newborn More often the heel stick dried blood spot on 4th day
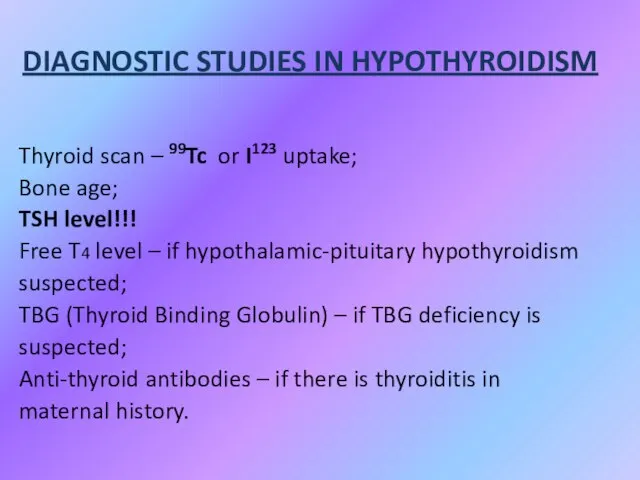
- 66. DIAGNOSTIC STUDIES IN HYPOTHYROIDISM Thyroid scan – 99Tc or I123 uptake; Bone age; TSH level!!! Free
- 67. Biochemical markers of CH Low serum T4 level and T3 level with evaluated TSH (primary) level;
- 68. Biochemical markers of CH Other: Elevated serum cholesterol; Elevated creatinphosphokinase; Hyponatriemia.
- 69. Instrumental data Slightly decrease heart rate and amplitude of R wave (ECG); Increased left ventricular wall
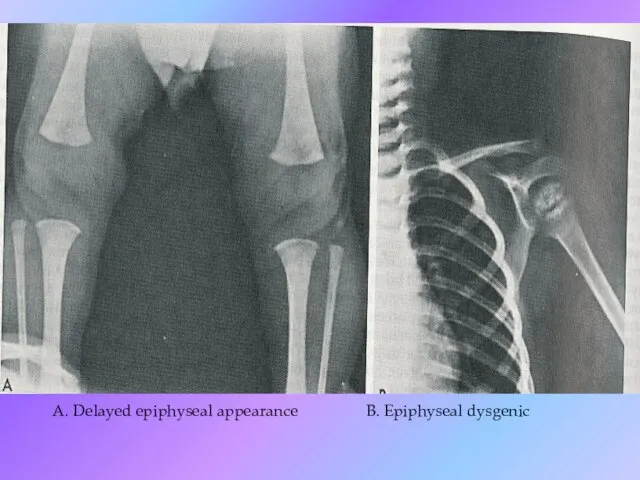
- 70. A. Delayed epiphyseal appearance B. Epiphyseal dysgenic
- 71. High TSH and Low T4 Management Primary Congenital Hypothyroidism Thyroxine Tablets 25-50-75 ug Crush it, add
- 72. Myxedema coma Reduced level of consciousness, seizures; Hypotension/shock; Hypothermia; Hyponatremia.
- 73. Treatment L-thyroxin (Levothyroxine)
- 74. PROGNOSIS If treatment is delayed, physical development can be hurt slightly. Early treatment is crucial to
- 75. Juvenile hypothyroidism A child with growth retardation, constipation, becomes less sociable, gain weight; his school performance
- 76. Causes of juvenile hypothyroidism Hashimoto thyroiditis. More common in girls who may have initial thyrotoxicosis or
- 77. JH investigations Antithyroglobulin and antimicrosomal antibodies are found. Serum T4 is low (earlier than T3). Bone
- 78. ETIOLOGY OF ACQUIRED HYPOTHYROIDISM Chronic lymphocytic (Hashimoto`s) thyroiditis (CLT); Subacute thyroiditis (De Quervain`s); Goitrogens (iodide, thiouracil,
- 79. SYMPTOMS OF ACQUIRED HYPOTHYROIDISM Slow growth; Edema; Decreased appetite; Constipation; Swollen thyroid gland; Lethargy; Drop in
- 80. SIGNS OF ACQUIRED HYPOTHYROIDISM Delayed reflex return; Mental depression; Pale, thick, or cool skin; Muscle pseudohypertrophy;
- 81. Chronic thyroiditis Hashimoto disease Clinical presentation: Painless diffuse goiter; Goiter with euthyroidism; Toxic thyroiditis; Hypothyroidism with
- 82. Autoimmune hypothyroidism
- 83. Diagnosis Hashimoto disease T4 total and free, serum TSH; Biopsy; Antibodies test: antithyroglobulin antibodies to thyroperoxidase,
- 84. Treatment Levothyroxine if hypothyroid; Triiodothyronine (for myxedema coma); Thyroid suppression (levothyroxine) to decrease goiter size; Surgery
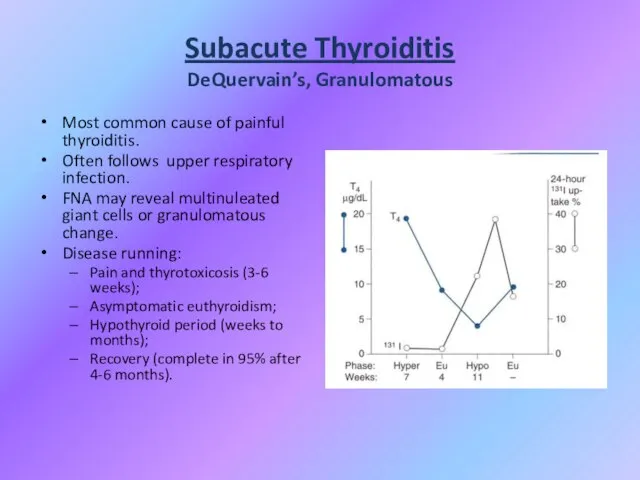
- 85. Subacute Thyroiditis DeQuervain’s, Granulomatous Most common cause of painful thyroiditis. Often follows upper respiratory infection. FNA
- 86. Subacute Thyroiditis DeQuervain’s, Granulomatous
- 87. Acute Thyroiditis Causes: 68% Bacterial (S. aureus, S. pyogenes); 15% Fungal; 9% Mycobacterial. May occur secondary
- 88. Acute Thyroiditis Diagnosis: Warm, painful, enlarged thyroid; FNA to drain abscess; RAIU normal (versus decreased in
- 90. Скачать презентацию
Слайд 3Introduction
Thyroid hormone is essential for the growth and maturation of many target
Introduction
Thyroid hormone is essential for the growth and maturation of many target
Слайд 4Location: Located close to thyroid cartilage. Has two lateral lobes connected by
Location: Located close to thyroid cartilage. Has two lateral lobes connected by
Слайд 7Thyroid Physiology
Thyroid Physiology
Слайд 8Pathways of thyroid
Hormone metabolism
Pathways of thyroid
Hormone metabolism
Слайд 9Feedback regulation Of TSH
Feedback regulation Of TSH
Слайд 10Thyroid physiology, continuation
Thyroid physiology, continuation
Слайд 11Production of Thyroid Hormones
NIS (Na+/I- Sympoter)
TPO
Production of Thyroid Hormones
NIS (Na+/I- Sympoter)
TPO
Слайд 12Thyroid Hormone
Majority of circulating hormone is T4 (98,5% T4, 1,5% T3 )
Thyroid Hormone
Majority of circulating hormone is T4 (98,5% T4, 1,5% T3 )
Слайд 13Effects of thyroid hormones
Fetal brain and skeletal maturation;
Increase in basal metabolic rate;
Inotropic
Effects of thyroid hormones
Fetal brain and skeletal maturation;
Increase in basal metabolic rate;
Inotropic
Слайд 14Thyroid hormones
Thyroid hormones
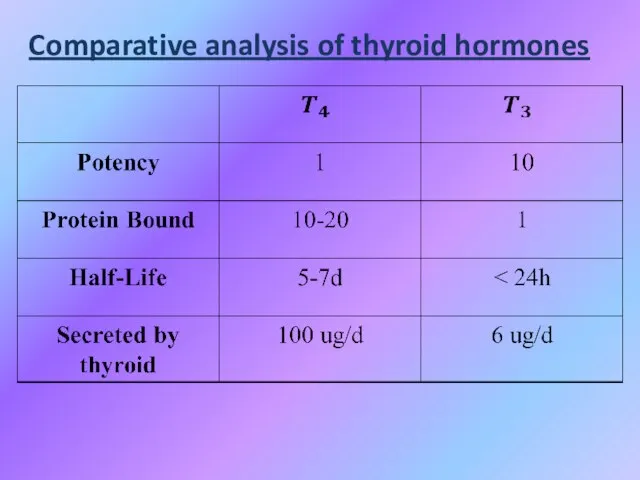
Слайд 15Comparative analysis of thyroid hormones
Comparative analysis of thyroid hormones
Слайд 16THYROTOXICOSIS (Hyperthyroidism)
Overproduction of thyroid hormones;
HYPOTHYROIDISM (Gland destruction)
Underproduction of thyroid hormones;
NEOPLASTIC PROCESSES
Benign;
Malignant.
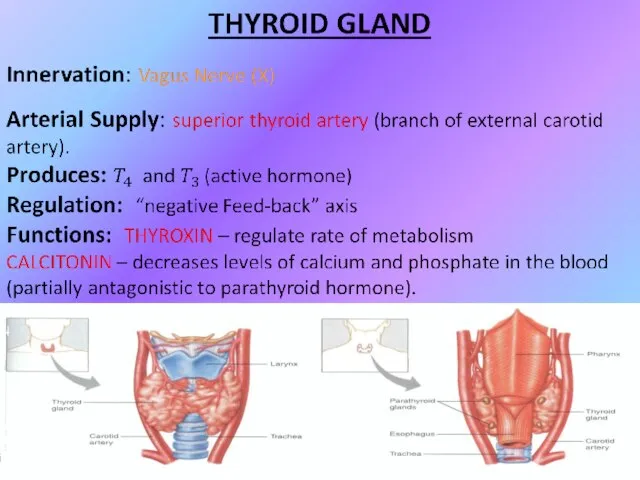
THYROID GLAND
Overproduction of thyroid hormones;
HYPOTHYROIDISM (Gland destruction)
Underproduction of thyroid hormones;
NEOPLASTIC PROCESSES
Benign;
Malignant.
THYROID GLAND
Слайд 17Diagnostic of Thyroid gland disease
Diagnostic of Thyroid gland disease
Слайд 18LABORATORY EVALUATION
TSH (thyroid-stimulating hormone) normal, practically excludes abnormality
LABORATORY EVALUATION
TSH (thyroid-stimulating hormone) normal, practically excludes abnormality
Слайд 19High TSH usually means Hypothyroidism
Rare causes:
TSH-secreting pituitary tumor;
Thyroid hormone resistance;
Assay artifact.
Low TSH
High TSH usually means Hypothyroidism
Rare causes:
TSH-secreting pituitary tumor;
Thyroid hormone resistance;
Assay artifact.
Low TSH
Слайд 21RAIU (Radioactive iodine uptake )
Scintillation counter measures radioactivity after I123 or I131
RAIU (Radioactive iodine uptake )
Scintillation counter measures radioactivity after I123 or I131
Слайд 22Iodine states
Normal Thyroid
Inactive Thyroid
Hyperactive Thyroid
Iodine states
Normal Thyroid
Inactive Thyroid
Hyperactive Thyroid
Слайд 23Thyrotoxicosis
Primary;
Secondary;
Without Hyperthyroidism;
Exogenous or factitious.
Hypothyroidism
Primary;
Secondary;
Peripheral.
Primary;
Secondary;
Without Hyperthyroidism;
Exogenous or factitious.
Hypothyroidism
Primary;
Secondary;
Peripheral.
Слайд 24HYPERTHYROIDISM or THYROTOXICOSIS:
- is the result of excessive thyroid gland function
HYPERTHYROIDISM or THYROTOXICOSIS:
- is the result of excessive thyroid gland function
Слайд 25Primary Hyperthyroidism:
Graves’;
Toxic Multinodular Goitre;
Toxic adenoma;
Functioning thyroid carcinoma metastases;
Activating mutation of TSH receptor;
Struma
Primary Hyperthyroidism:
Graves’;
Toxic Multinodular Goitre;
Toxic adenoma;
Functioning thyroid carcinoma metastases;
Activating mutation of TSH receptor;
Struma
Слайд 26Causes of Thyrotoxicosis:
Thyrotoxicosis without hyperthyroidism:
Subacute thyroiditis;
Silent thyroiditis;
Other causes of thyroid destruction:
Amiodarone, radiation,
Causes of Thyrotoxicosis:
Thyrotoxicosis without hyperthyroidism:
Subacute thyroiditis;
Silent thyroiditis;
Other causes of thyroid destruction:
Amiodarone, radiation,
Слайд 27Symptoms of Hyperthyroidism
Heat intolerance, dislike of hot weather;
Hyperactivity, irritability, nervousness, fatigue;
Weight loss
Symptoms of Hyperthyroidism
Heat intolerance, dislike of hot weather;
Hyperactivity, irritability, nervousness, fatigue;
Weight loss
Слайд 28Causes of Transient Neonatal Hyperthyroidism
Neonatal hyperthyroidism is almost always transient and results
Causes of Transient Neonatal Hyperthyroidism
Neonatal hyperthyroidism is almost always transient and results
Слайд 29Situations That Should Prompt Consideration of Neonatal
Hyperthyroidism:
● Unexplained tachycardia, goitre or stare;
●
Situations That Should Prompt Consideration of Neonatal
Hyperthyroidism:
● Unexplained tachycardia, goitre or stare;
●
Слайд 30Congenital thyrotoxic goiter of and infant born to a mother with thyrotoxicosis
Congenital thyrotoxic goiter of and infant born to a mother with thyrotoxicosis
Слайд 31Therapy of Transient neonatal hyperthyroidism
Treatment is accomplished by maternal administration of antithyroid
Therapy of Transient neonatal hyperthyroidism
Treatment is accomplished by maternal administration of antithyroid
Слайд 32Therapy of Transient neonatal hyperthyroidism
In the neonate, treatment is the follows: either
Therapy of Transient neonatal hyperthyroidism
In the neonate, treatment is the follows: either
Слайд 33Therapy of Transient neonatal
hyperthyroidism
Propranolol (2 mg/kg/day in 2 or 3 divided
Therapy of Transient neonatal
hyperthyroidism
Propranolol (2 mg/kg/day in 2 or 3 divided
Слайд 34Permanent neonatal hyperthyroidism
Rarely, neonatal hyperthyroidism is inconvertible and is due to a
Permanent neonatal hyperthyroidism
Rarely, neonatal hyperthyroidism is inconvertible and is due to a
Слайд 35Permanent neonatal hyperthyroidism
Early recognition is important because the thyroid function of affected
Permanent neonatal hyperthyroidism
Early recognition is important because the thyroid function of affected
Слайд 37Goitre
Endemic goitre:
Areas where > 5% of children 6-12 years old have goiter
Common
Goitre
Endemic goitre:
Areas where > 5% of children 6-12 years old have goiter
Common
Слайд 38Goitre
Etiology
Hashimoto’s thyroiditis:
Early stages only, late stages show atrophic changes;
May present with hypo,
Goitre
Etiology
Hashimoto’s thyroiditis:
Early stages only, late stages show atrophic changes;
May present with hypo,
Слайд 39Goitre
Goitre
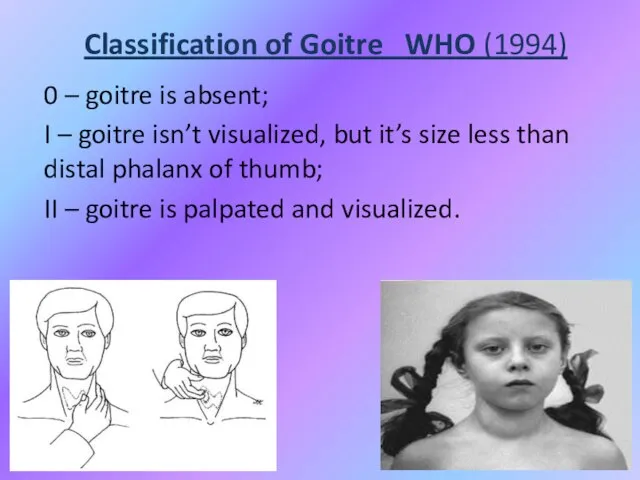
Слайд 40Classification of Goitre WHO (1994)
0 – goitre is absent;
I – goitre isn’t
Classification of Goitre WHO (1994)
0 – goitre is absent;
I – goitre isn’t
Слайд 41Functional condition of Thyroid influence may be as
Euthyroidism;
Hypothyroidism;
Hyperthyroidism.
Functional condition of Thyroid influence may be as
Euthyroidism;
Hypothyroidism;
Hyperthyroidism.
Слайд 42Non-Toxic Goitre
Cancer screening in non-toxic MNG (Multinodular goitre )
Longstanding MNG has a
Non-Toxic Goitre
Cancer screening in non-toxic MNG (Multinodular goitre )
Longstanding MNG has a
Слайд 43Non-Toxic Goitre
Treatment options (no compressive symptoms):
Use follow-up to monitor for progression;
Thyroid suppression
Non-Toxic Goitre
Treatment options (no compressive symptoms):
Use follow-up to monitor for progression;
Thyroid suppression
Слайд 44Non-Toxic Goitre
Treatment options (compressive symptoms):
Radioactive iodine (RAI) ablation:
Volume reduction 33% - 66%
Non-Toxic Goitre
Treatment options (compressive symptoms):
Radioactive iodine (RAI) ablation:
Volume reduction 33% - 66%
Слайд 45Toxic Goitre
Treatment for Toxic MNG:
Thionamide medications:
Not indicated for long-term use due to
Toxic Goitre
Treatment for Toxic MNG:
Thionamide medications:
Not indicated for long-term use due to
Слайд 46Graves’ Disease
Diffuse toxic goitre is an autoimmune pathology with prolonged elevation T3
Graves’ Disease
Diffuse toxic goitre is an autoimmune pathology with prolonged elevation T3
Слайд 48Differentiating Causes of Hyperthyroidism
Differentiating Causes of Hyperthyroidism
Слайд 49Pathophysiology of ophthalmopathy
Pathophysiology of ophthalmopathy
Слайд 50Graves disease Ophthalmopathy
A feeling of "sandpaper" in the eyes and discomfort in
Graves disease Ophthalmopathy
A feeling of "sandpaper" in the eyes and discomfort in
Слайд 51Graves Disease: Treatment
• Medications:
– Beta-blockers for symptoms – can be discontinued as
Graves Disease: Treatment
• Medications:
– Beta-blockers for symptoms – can be discontinued as
Слайд 52Нypothyroidism
Hypothyroidism - syndrome with particular or total deficiency of T3, T4 or
Нypothyroidism
Hypothyroidism - syndrome with particular or total deficiency of T3, T4 or
Слайд 53Classification of hypothyroidism
PRIMARY - defects of biosynthesis of T3, T4 due
to pathology
Classification of hypothyroidism
PRIMARY - defects of biosynthesis of T3, T4 due
to pathology
Слайд 54Primary:
Autoimmune (Hashimoto´s);
Iatrogenic Surgery or 131I administration;
Drugs: amiodarone, lithium;
Congenital (1 in 3000 to
Primary:
Autoimmune (Hashimoto´s);
Iatrogenic Surgery or 131I administration;
Drugs: amiodarone, lithium;
Congenital (1 in 3000 to
Слайд 55Secondary:
Pituitary gland destruction;
Isolated TSH deficiency;
Bexarotene treatment;
Hypothalamic disorders.
Peripheral:
Rare, familial tendency.
Pituitary gland destruction;
Isolated TSH deficiency;
Bexarotene treatment;
Hypothalamic disorders.
Peripheral:
Rare, familial tendency.
Слайд 56Ethyology of congenital hypothyroidism
Ethyology of congenital hypothyroidism
Слайд 57Expected Findings in Congenital Hypothyroidism
Expected Findings in Congenital Hypothyroidism
Слайд 58Expected Findings in Congenital Hypothyroidism
Expected Findings in Congenital Hypothyroidism
Слайд 59Congenital hypothyroidism
Agenesis (no goiter) or dysgenesis ( aplasia, hypoplasia, ectopic gland) are
Congenital hypothyroidism
Agenesis (no goiter) or dysgenesis ( aplasia, hypoplasia, ectopic gland) are
Слайд 60Congenital hypothyroidism
Clinical features
Coarse facial features, dry skin, prolonged jaundice, large fontanelles, posterior
Congenital hypothyroidism
Clinical features
Coarse facial features, dry skin, prolonged jaundice, large fontanelles, posterior
Слайд 63Hypothyroidism Screening in the Newborn
More often the heel stick dried blood spot
Hypothyroidism Screening in the Newborn
More often the heel stick dried blood spot

Слайд 66DIAGNOSTIC STUDIES IN HYPOTHYROIDISM
Thyroid scan – 99Tc or I123 uptake;
Bone age;
TSH
DIAGNOSTIC STUDIES IN HYPOTHYROIDISM
Thyroid scan – 99Tc or I123 uptake;
Bone age;
TSH
Слайд 67Biochemical markers of CH
Low serum T4 level and T3 level with evaluated
Biochemical markers of CH
Low serum T4 level and T3 level with evaluated
Слайд 68Biochemical markers of CH
Other:
Elevated serum cholesterol;
Elevated creatinphosphokinase;
Hyponatriemia.
Biochemical markers of CH
Other:
Elevated serum cholesterol;
Elevated creatinphosphokinase;
Hyponatriemia.
Слайд 69Instrumental data
Slightly decrease heart rate and amplitude of R wave (ECG);
Increased left
Instrumental data
Slightly decrease heart rate and amplitude of R wave (ECG);
Increased left
Слайд 70A. Delayed epiphyseal appearance B. Epiphyseal dysgenic
A. Delayed epiphyseal appearance B. Epiphyseal dysgenic
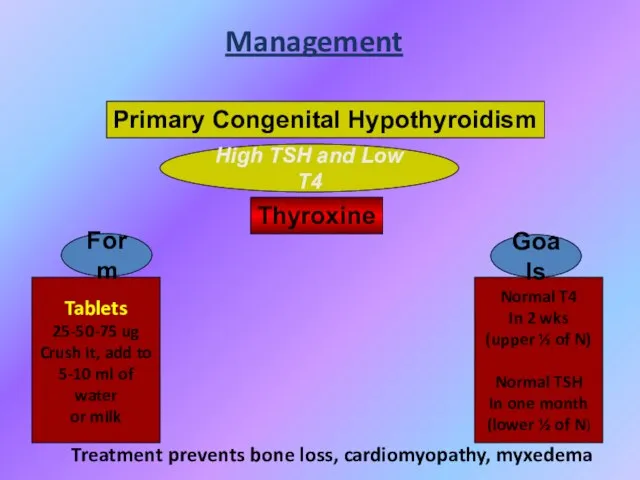
Слайд 71High TSH and Low T4
Management
Primary Congenital Hypothyroidism
Thyroxine
Tablets
25-50-75 ug
Crush it, add to
5-10
High TSH and Low T4
Management
Primary Congenital Hypothyroidism
Thyroxine
Tablets
25-50-75 ug
Crush it, add to
5-10
Слайд 72Myxedema coma
Reduced level of consciousness, seizures;
Hypotension/shock;
Hypothermia;
Hyponatremia.
Myxedema coma
Reduced level of consciousness, seizures;
Hypotension/shock;
Hypothermia;
Hyponatremia.
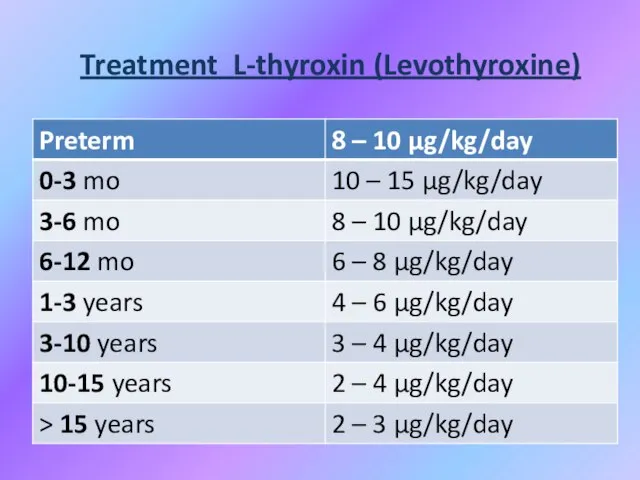
Слайд 73Treatment L-thyroxin (Levothyroxine)
Treatment L-thyroxin (Levothyroxine)
Слайд 74PROGNOSIS
If treatment is delayed, physical development can be hurt slightly. Early treatment
PROGNOSIS
If treatment is delayed, physical development can be hurt slightly. Early treatment
Слайд 75Juvenile hypothyroidism
A child with growth retardation, constipation, becomes less sociable, gain weight;
Juvenile hypothyroidism
A child with growth retardation, constipation, becomes less sociable, gain weight;
Слайд 76Causes of juvenile hypothyroidism
Hashimoto thyroiditis. More common in girls who may have
Causes of juvenile hypothyroidism
Hashimoto thyroiditis. More common in girls who may have
Слайд 77JH investigations
Antithyroglobulin and antimicrosomal antibodies are found.
Serum T4 is low (earlier
JH investigations
Antithyroglobulin and antimicrosomal antibodies are found.
Serum T4 is low (earlier
Слайд 78ETIOLOGY OF ACQUIRED HYPOTHYROIDISM
Chronic lymphocytic (Hashimoto`s) thyroiditis (CLT);
Subacute thyroiditis (De Quervain`s);
Goitrogens (iodide,
ETIOLOGY OF ACQUIRED HYPOTHYROIDISM
Chronic lymphocytic (Hashimoto`s) thyroiditis (CLT);
Subacute thyroiditis (De Quervain`s);
Goitrogens (iodide,
Слайд 79SYMPTOMS OF ACQUIRED HYPOTHYROIDISM
Slow growth;
Edema;
Decreased appetite;
Constipation;
Swollen thyroid gland;
Lethargy;
Drop in school performance;
Cold
SYMPTOMS OF ACQUIRED HYPOTHYROIDISM
Slow growth;
Edema;
Decreased appetite;
Constipation;
Swollen thyroid gland;
Lethargy;
Drop in school performance;
Cold
Слайд 80SIGNS OF ACQUIRED HYPOTHYROIDISM
Delayed reflex return;
Mental depression;
Pale, thick, or cool
SIGNS OF ACQUIRED HYPOTHYROIDISM
Delayed reflex return;
Mental depression;
Pale, thick, or cool
Слайд 81Chronic thyroiditis Hashimoto disease
Clinical presentation:
Painless diffuse goiter;
Goiter with euthyroidism;
Toxic thyroiditis;
Hypothyroidism
Chronic thyroiditis Hashimoto disease
Clinical presentation:
Painless diffuse goiter;
Goiter with euthyroidism;
Toxic thyroiditis;
Hypothyroidism
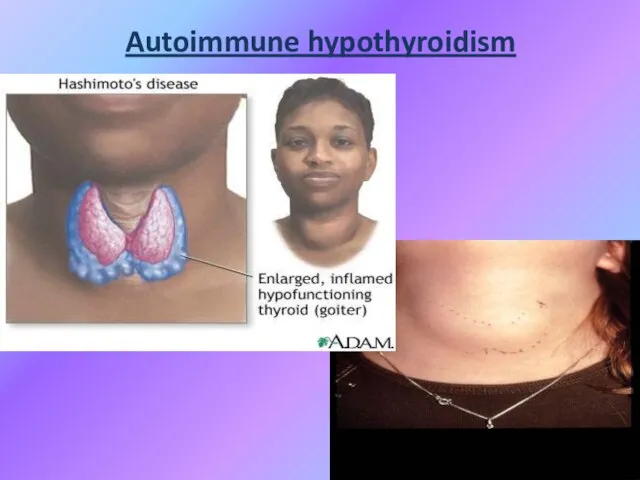
Слайд 82Autoimmune hypothyroidism
Autoimmune hypothyroidism
Слайд 83Diagnosis Hashimoto disease
T4 total and free, serum TSH;
Biopsy;
Antibodies test: antithyroglobulin antibodies to
Diagnosis Hashimoto disease
T4 total and free, serum TSH;
Biopsy;
Antibodies test: antithyroglobulin antibodies to
Слайд 84Treatment
Levothyroxine if hypothyroid;
Triiodothyronine (for myxedema coma);
Thyroid suppression (levothyroxine) to decrease goiter size;
Surgery
Treatment
Levothyroxine if hypothyroid;
Triiodothyronine (for myxedema coma);
Thyroid suppression (levothyroxine) to decrease goiter size;
Surgery
Слайд 85Subacute Thyroiditis
DeQuervain’s, Granulomatous
Most common cause of painful thyroiditis.
Often follows upper respiratory infection.
FNA
Subacute Thyroiditis
DeQuervain’s, Granulomatous
Most common cause of painful thyroiditis.
Often follows upper respiratory infection.
FNA
Слайд 86Subacute Thyroiditis
DeQuervain’s, Granulomatous
Subacute Thyroiditis
DeQuervain’s, Granulomatous
Слайд 87Acute Thyroiditis
Causes:
68% Bacterial (S. aureus, S. pyogenes);
15% Fungal;
9% Mycobacterial.
May occur secondary to:
Pyriform
Acute Thyroiditis
Causes:
68% Bacterial (S. aureus, S. pyogenes);
15% Fungal;
9% Mycobacterial.
May occur secondary to:
Pyriform
Слайд 88Acute Thyroiditis
Diagnosis:
Warm, painful, enlarged thyroid;
FNA to drain abscess;
RAIU normal (versus decreased in
Acute Thyroiditis
Diagnosis:
Warm, painful, enlarged thyroid;
FNA to drain abscess;
RAIU normal (versus decreased in
 РАЗВИТИЕ КАРТОГРАФИИ В РОССИИ(XVI – ПЕРВАЯ ПОЛОВИНА XIX ВЕКА)
РАЗВИТИЕ КАРТОГРАФИИ В РОССИИ(XVI – ПЕРВАЯ ПОЛОВИНА XIX ВЕКА) Методика обучения спуска на лыжах.
Методика обучения спуска на лыжах. Hallo!Wie hei?t du?Meine Familie.Meine Freunde.
Hallo!Wie hei?t du?Meine Familie.Meine Freunde. Ты, человек, любя природу,Хоть иногда её жалей:В увеселительных походахНе растопчи её полей.В вокзальной сутолоке векаТы оценит
Ты, человек, любя природу,Хоть иногда её жалей:В увеселительных походахНе растопчи её полей.В вокзальной сутолоке векаТы оценит Проект Район и деревня, где я живу Октябрьский район с.Черницыно
Проект Район и деревня, где я живу Октябрьский район с.Черницыно Брак в Древней Иудее
Брак в Древней Иудее Тема: Отмена крепостного права в России
Тема: Отмена крепостного права в России Водно-электролитные нарушения у хирургических больных, инвазивная терапия
Водно-электролитные нарушения у хирургических больных, инвазивная терапия Петербург Ф.М.Достоевского «Преступление и наказание»
Петербург Ф.М.Достоевского «Преступление и наказание» Презентация на тему Все профессии важны
Презентация на тему Все профессии важны  Проверка домашнего задания
Проверка домашнего задания Атмосфера и ее свойства
Атмосфера и ее свойства Теорема Фалеса
Теорема Фалеса «Я иду на урок биологии»
«Я иду на урок биологии» Восстание декабристов
Восстание декабристов Распространение колебаний в упругих средах. Волны
Распространение колебаний в упругих средах. Волны Иван Алексеевич Бунин1870-1953
Иван Алексеевич Бунин1870-1953 Фонд новых форм развития образования о вызовах современности
Фонд новых форм развития образования о вызовах современности Модуль управления тепловизионным комплексом
Модуль управления тепловизионным комплексом Состязание юных Математиков
Состязание юных Математиков Константин Сергеевич Станиславский
Константин Сергеевич Станиславский _AFTsNS_Lektsiya_1 (2)
_AFTsNS_Lektsiya_1 (2) Судебная система РФ
Судебная система РФ Иван Грозный
Иван Грозный система оценки качества образования в школе
система оценки качества образования в школе Заполнение Психоматрицы. Занятие 2
Заполнение Психоматрицы. Занятие 2 Предложение по размещению на фасаде
Предложение по размещению на фасаде Декабристы в Ялуторовске
Декабристы в Ялуторовске