- גישה למטופלת צעירה עם שלפוחית שתן רגיזה

Содержание
- 2. Case . מטופלת בשם גיל, בת 23, פרופיל 97. עובדת בעבודה משרדית אשקנזיה, שוללת תרופות קבוע.
- 3. בדיקה פיזיקלית תקינה בדיקת שתן כללית תקין, תרבית שתן תקין. STD תקין נבדקה אצל רופא נשים
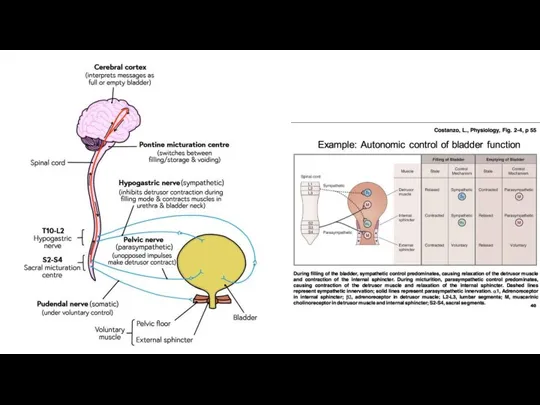
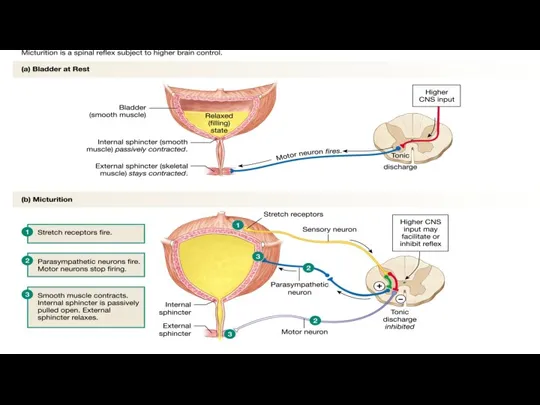
- 4. What is it? URINARY INCONTINENCE Neurogenic Bladder ANXIETY Nicturia Enuresis
- 5. Definitions Dysuria is a symptom of pain, discomfort, or burning when urinating Nocturia is “the complaint
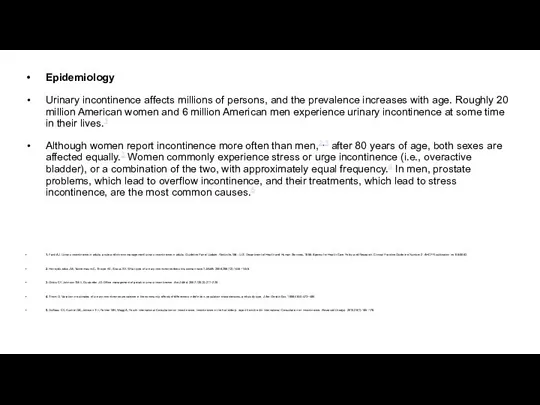
- 9. Epidemiology Urinary incontinence affects millions of persons, and the prevalence increases with age. Roughly 20 million
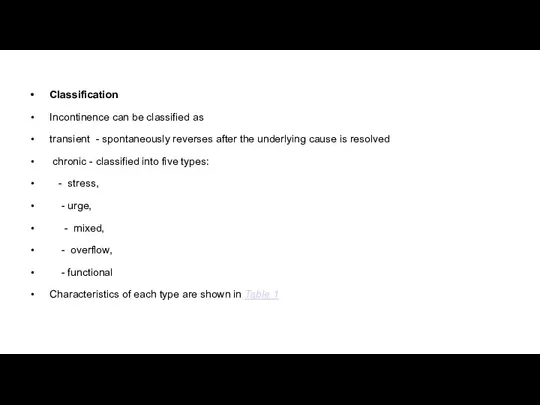
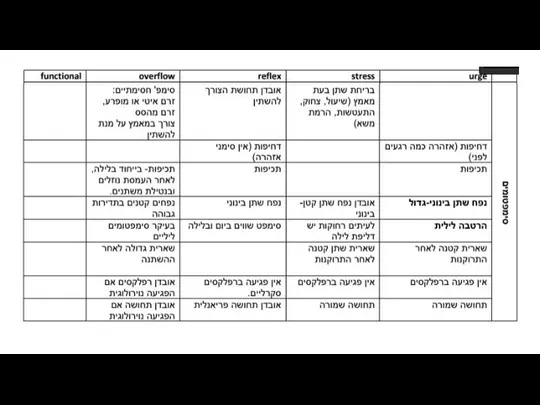
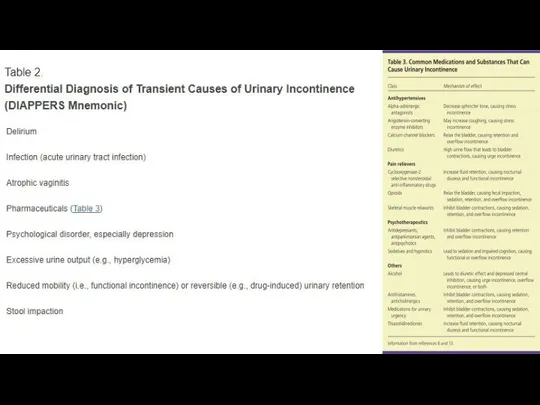
- 10. Classification Incontinence can be classified as transient - spontaneously reverses after the underlying cause is resolved
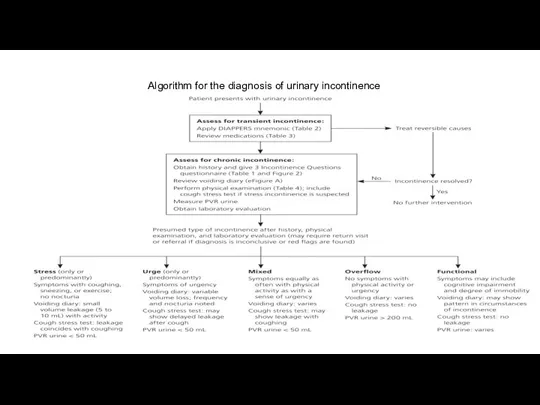
- 14. Algorithm for the diagnosis of urinary incontinence
- 16. Chronic Urinary Incontinence The 3 Incontinence Questions is a reliable questionnaire available free of charge- It
- 17. ASSESSMENT OF MEDICAL PROBLEMS The patient history should include an assessment of other medical conditions and
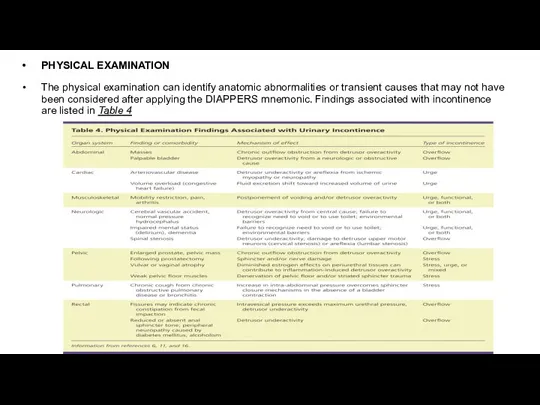
- 18. PHYSICAL EXAMINATION The physical examination can identify anatomic abnormalities or transient causes that may not have
- 19. COUGH STRESS TEST If stress incontinence is suspected, the cough stress test is the most reliable
- 20. LABORATORY TESTS a serum creatinine level - may be elevated if there is urinary retention (overflow
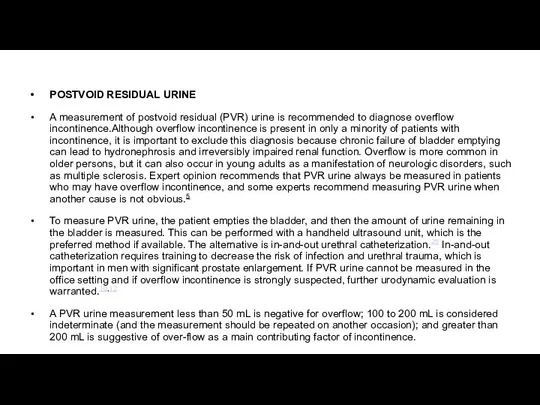
- 21. POSTVOID RESIDUAL URINE A measurement of postvoid residual (PVR) urine is recommended to diagnose overflow incontinence.Although
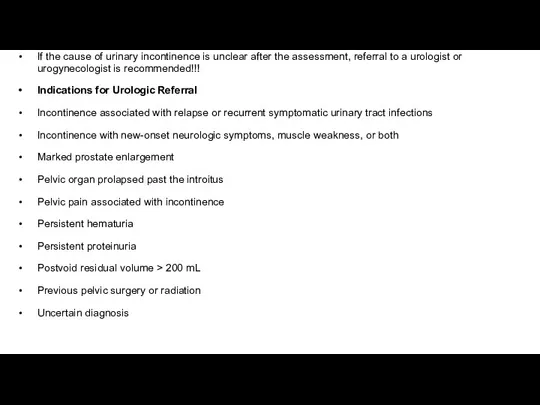
- 22. If the cause of urinary incontinence is unclear after the assessment, referral to a urologist or
- 23. Routine referral for urodynamic testing is not recommended, even if a patient is a candidate for
- 26. Pelvic floor muscle (Kegel) exercises — Consistent with guidelines from the American College of Physicians, we
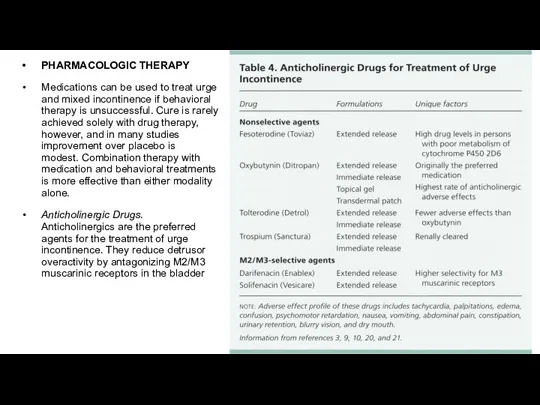
- 27. PHARMACOLOGIC THERAPY Medications can be used to treat urge and mixed incontinence if behavioral therapy is
- 30. Beta-Adrenergic Agonists. Approved by the FDA in 2012, mirabegron (Myrbetriq) is from a new class of
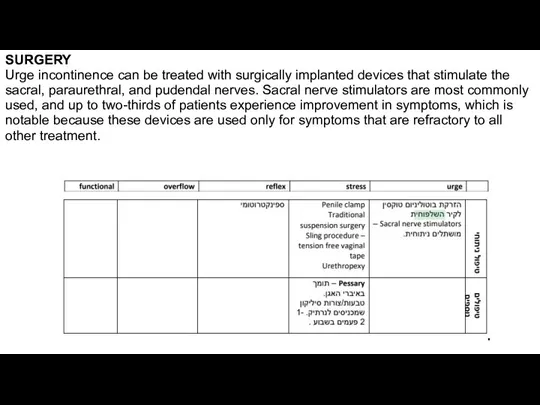
- 31. SURGERY Urge incontinence can be treated with surgically implanted devices that stimulate the sacral, paraurethral, and
- 33. Скачать презентацию
Слайд 3בדיקה פיזיקלית תקינה
בדיקת שתן כללית תקין, תרבית שתן תקין.
STD תקין
נבדקה
בדיקה פיזיקלית תקינה
בדיקת שתן כללית תקין, תרבית שתן תקין.
STD תקין
נבדקה
Слайд 4What is it?
URINARY INCONTINENCE
Neurogenic Bladder
ANXIETY
Nicturia
Enuresis
What is it?
URINARY INCONTINENCE
Neurogenic Bladder
ANXIETY
Nicturia
Enuresis
Слайд 5Definitions
Dysuria is a symptom of pain, discomfort, or burning when urinating
Nocturia is “the
Definitions
Dysuria is a symptom of pain, discomfort, or burning when urinating
Nocturia is “the
Слайд 9Epidemiology
Urinary incontinence affects millions of persons, and the prevalence increases with age.
Epidemiology
Urinary incontinence affects millions of persons, and the prevalence increases with age.
Слайд 10Classification
Incontinence can be classified as
transient - spontaneously reverses after the underlying
Classification
Incontinence can be classified as
transient - spontaneously reverses after the underlying


Слайд 14Algorithm for the diagnosis of urinary incontinence
Algorithm for the diagnosis of urinary incontinence
Слайд 16Chronic Urinary Incontinence
The 3 Incontinence Questions is a reliable questionnaire available free
Chronic Urinary Incontinence
The 3 Incontinence Questions is a reliable questionnaire available free

Слайд 17ASSESSMENT OF MEDICAL PROBLEMS
The patient history should include an assessment of other
ASSESSMENT OF MEDICAL PROBLEMS
The patient history should include an assessment of other
Слайд 18PHYSICAL EXAMINATION
The physical examination can identify anatomic abnormalities or transient causes that
PHYSICAL EXAMINATION
The physical examination can identify anatomic abnormalities or transient causes that
Слайд 19COUGH STRESS TEST
If stress incontinence is suspected, the cough stress test is
COUGH STRESS TEST
If stress incontinence is suspected, the cough stress test is
Слайд 20LABORATORY TESTS
a serum creatinine level - may be elevated if there is
LABORATORY TESTS
a serum creatinine level - may be elevated if there is
Слайд 21POSTVOID RESIDUAL URINE
A measurement of postvoid residual (PVR) urine is recommended to
POSTVOID RESIDUAL URINE
A measurement of postvoid residual (PVR) urine is recommended to
Слайд 22If the cause of urinary incontinence is unclear after the assessment, referral
If the cause of urinary incontinence is unclear after the assessment, referral
Слайд 23Routine referral for urodynamic testing is not recommended, even if a patient
Routine referral for urodynamic testing is not recommended, even if a patient

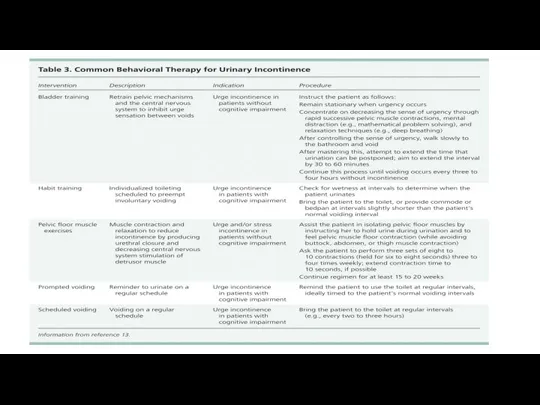
Слайд 26Pelvic floor muscle (Kegel) exercises — Consistent with guidelines from the American College of
Pelvic floor muscle (Kegel) exercises — Consistent with guidelines from the American College of
Слайд 27PHARMACOLOGIC THERAPY
Medications can be used to treat urge and mixed incontinence if
PHARMACOLOGIC THERAPY
Medications can be used to treat urge and mixed incontinence if


Слайд 30Beta-Adrenergic Agonists. Approved by the FDA in 2012, mirabegron (Myrbetriq) is from
Beta-Adrenergic Agonists. Approved by the FDA in 2012, mirabegron (Myrbetriq) is from
Слайд 31SURGERY
Urge incontinence can be treated with surgically implanted devices that stimulate the
SURGERY
Urge incontinence can be treated with surgically implanted devices that stimulate the
 Исследование пользы дневного сна у пожилых людей и после ночного утомления
Исследование пользы дневного сна у пожилых людей и после ночного утомления Коррекция у старших дошкольников со стертой дизартрией произносительной стороны речи
Коррекция у старших дошкольников со стертой дизартрией произносительной стороны речи Туберкулинодиагностика
Туберкулинодиагностика Операции на органах брюшной полости
Операции на органах брюшной полости Персональный биобанкинг BBS. Комплект услуг
Персональный биобанкинг BBS. Комплект услуг Интерфейсы при потере подвижности (лекция 1)
Интерфейсы при потере подвижности (лекция 1) Астенический синдром
Астенический синдром Infective endocarditis
Infective endocarditis Морфофункциональная характеристика скелета и аппарата движения нижних конечностей. Мышцы нижних конечностей
Морфофункциональная характеристика скелета и аппарата движения нижних конечностей. Мышцы нижних конечностей МКБ NEW коротко
МКБ NEW коротко День борьбы с инсультом
День борьбы с инсультом Pcos diet and lifestyle
Pcos diet and lifestyle Мочевая система
Мочевая система Тест Какой у меня обмен веществ?
Тест Какой у меня обмен веществ? Детское питание. Родительское собрание в школе
Детское питание. Родительское собрание в школе Жулдикораева
Жулдикораева Profilaktika_ISMP
Profilaktika_ISMP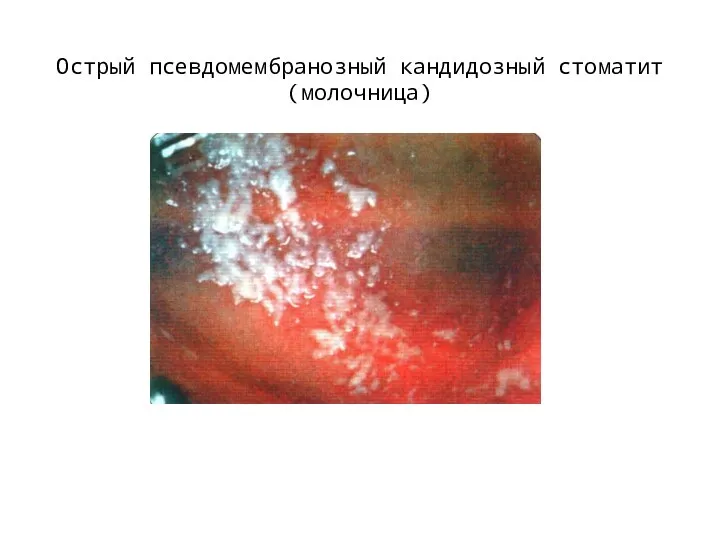 Острый псевдомембранозный кандидозный стоматит (молочница)
Острый псевдомембранозный кандидозный стоматит (молочница) Аритмии сердца
Аритмии сердца Особенности диагностики и лечения пациентов инфекционного профиля
Особенности диагностики и лечения пациентов инфекционного профиля Неэпителиальные опухоли ЖКТ
Неэпителиальные опухоли ЖКТ Влияние танцевального фитнеса с элементами зумбы на физическое состояние женщин 55-75 лет с гипертонией 1-й степени
Влияние танцевального фитнеса с элементами зумбы на физическое состояние женщин 55-75 лет с гипертонией 1-й степени Организация медицинского обслуживания в дошкольных образовательных учреждениях
Организация медицинского обслуживания в дошкольных образовательных учреждениях Новокузнецкий перинатальный центр. Преференции для молодых специалистов
Новокузнецкий перинатальный центр. Преференции для молодых специалистов Национальная патронажная служба
Национальная патронажная служба Инфекционные заболевания
Инфекционные заболевания Гигиенические требования к физкультурным занятиям. Зал, температура, уборка, инвентарь, форма одежды
Гигиенические требования к физкультурным занятиям. Зал, температура, уборка, инвентарь, форма одежды Субретинальная имплантация
Субретинальная имплантация