- Antimicrobial Stewardship Implications for Primary Health Care, and how it can work

Содержание
- 2. Basic acronyms AMR – antimicrobial resistance Resistance to drugs against microbes: bacteria, virus, protozoan, fungus The
- 3. Outline Why ABS? AMR is an increasing problem Antibiotics are a limited resource We need to
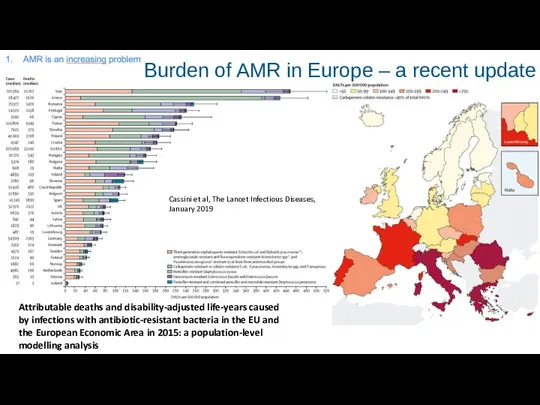
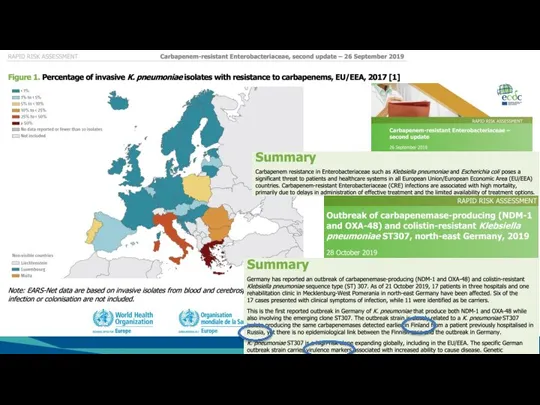
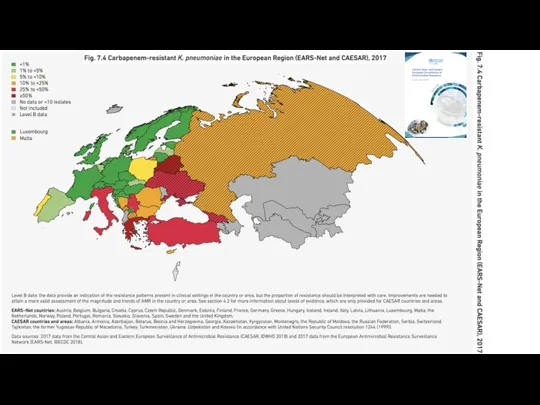
- 4. Burden of AMR in Europe – a recent update Cassini et al, The Lancet Infectious Diseases,
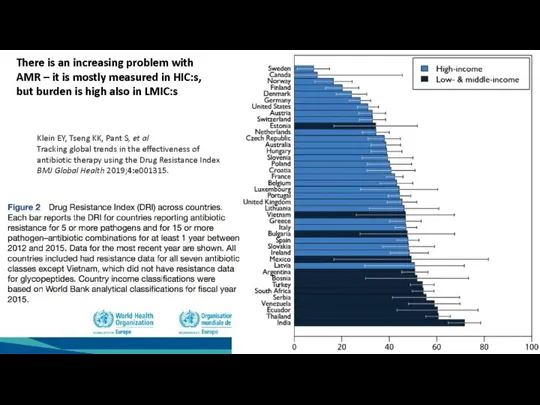
- 5. Klein EY, Tseng KK, Pant S, et al Tracking global trends in the effectiveness of antibiotic
- 6. Hip replacement Organ transplants Cancer chemotherapy Care of preterm babies Some of the Blessings of Modern
- 7. MAKMAX/IACMAC 2009, Feb 18-19, Omsk
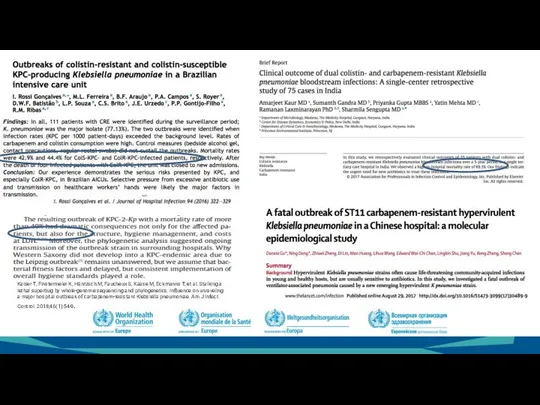
- 8. Kaiser T, Finstermeier K, Häntzsch M, Faucheux S, Kaase M, Eckmanns T, et al. Stalking a
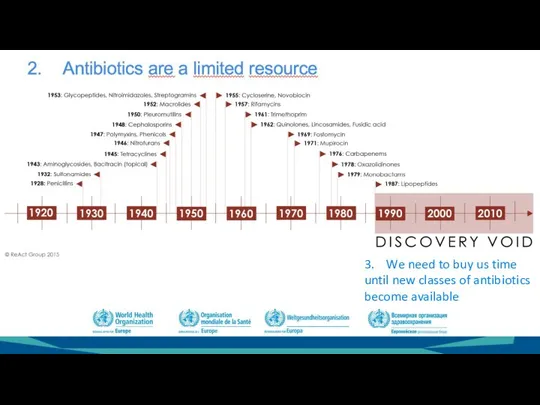
- 11. 3. We need to buy us time until new classes of antibiotics become available
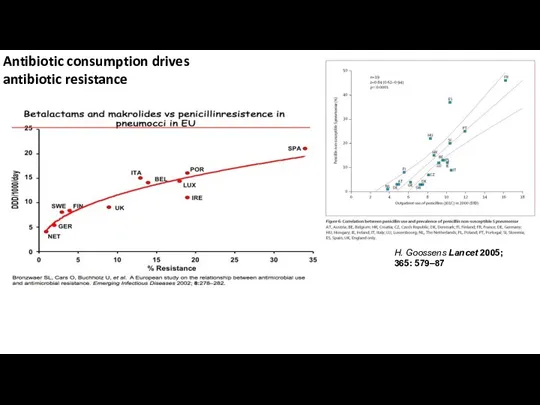
- 12. Antibiotic consumption drives antibiotic resistance H. Goossens Lancet 2005; 365: 579–87
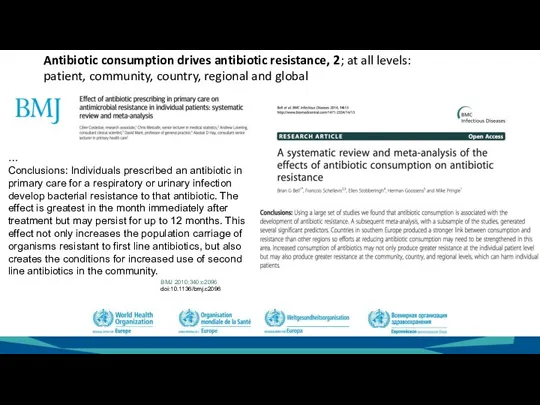
- 13. … Conclusions: Individuals prescribed an antibiotic in primary care for a respiratory or urinary infection develop
- 14. Where to work with ABS? Infectious disease clinics – highly qualified, but small part of all
- 15. Total antibiotic pressure Agri/Vet side Human health sector Country X
- 16. Hospital/in-patient use Community use
- 17. The paradox of seriousness of infection type versus amount of antibiotic use it causes, and thus
- 18. The aim is effective treatment for the present patient with his/her present illness – with no
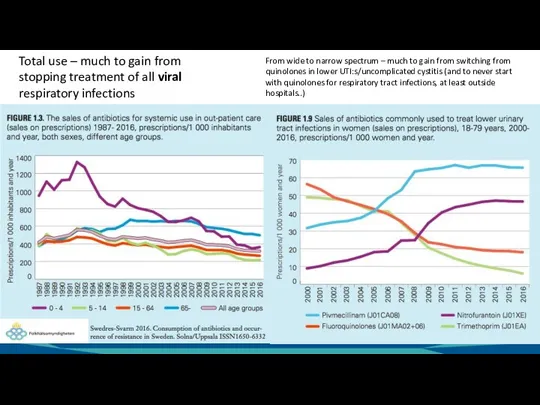
- 19. Total use – much to gain from stopping treatment of all viral respiratory infections From wide
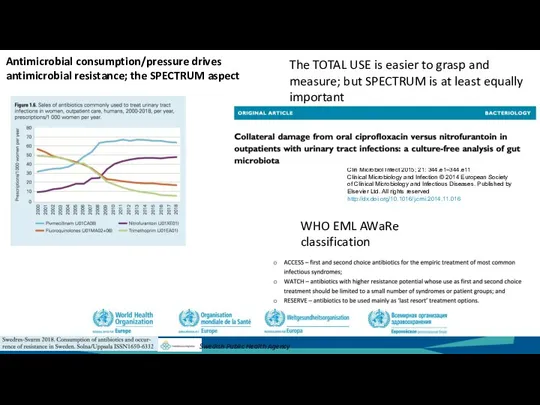
- 20. The TOTAL USE is easier to grasp and measure; but SPECTRUM is at least equally important
- 21. Rational antibiotic use The right antibiotic (for the disease, bacterium, patient condition..) At the right time
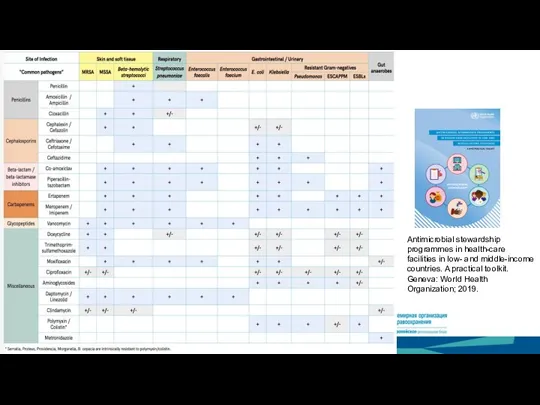
- 22. Antimicrobial stewardship programmes in health-care facilities in low- and middle-income countries. A practical toolkit. Geneva: World
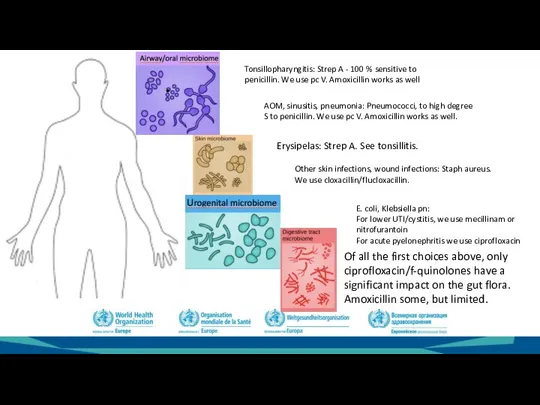
- 23. Tonsillopharyngitis: Strep A - 100 % sensitive to penicillin. We use pc V. Amoxicillin works as
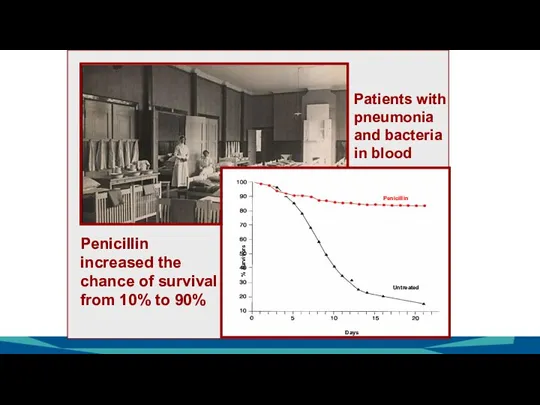
- 24. % survivors Penicillin Untreated Days Penicillin increased the chance of survival from 10% to 90% Patients
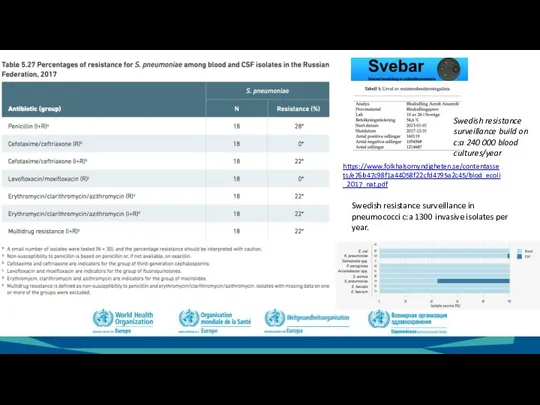
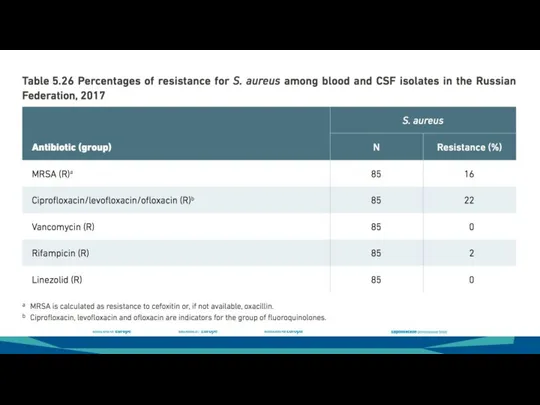
- 25. https://www.folkhalsomyndigheten.se/contentassets/e76b47c98f1a44058f22cfd4795a2c45/blod_ecoli_2017_nat.pdf Swedish resistance surveillance build on c:a 240 000 blood cultures/year Swedish resistance surveillance in pneumococci
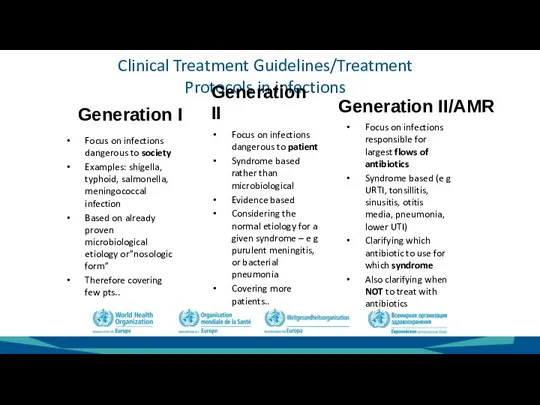
- 29. Clinical Treatment Guidelines/Treatment Protocols in infections Generation I Focus on infections dangerous to society Examples: shigella,
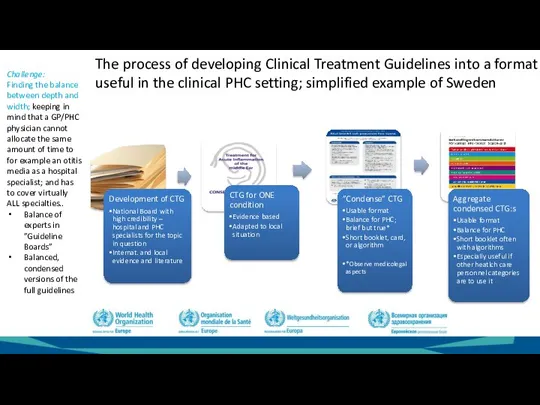
- 30. The process of developing Clinical Treatment Guidelines into a format useful in the clinical PHC setting;
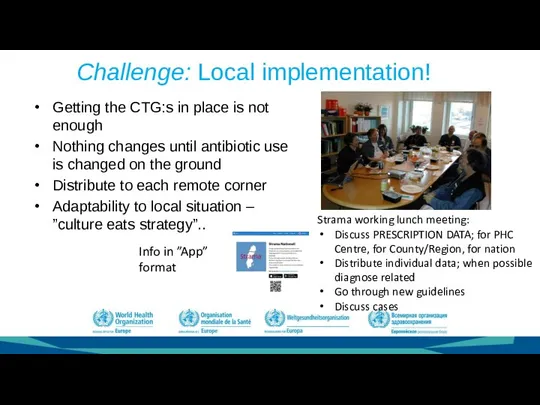
- 31. Challenge: Local implementation! Getting the CTG:s in place is not enough Nothing changes until antibiotic use
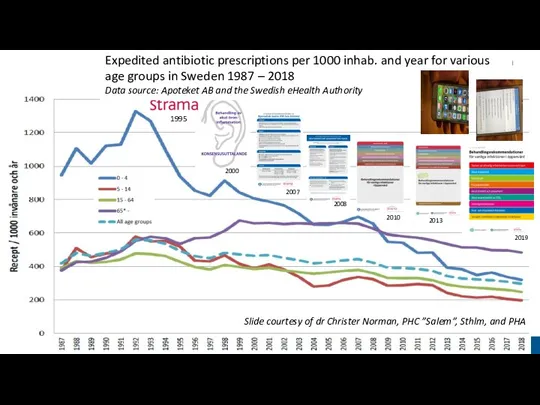
- 32. 2000 2007 2008 2010 2013 2019 1995 Slide courtesy of dr Christer Norman, PHC ”Salem”, Sthlm,
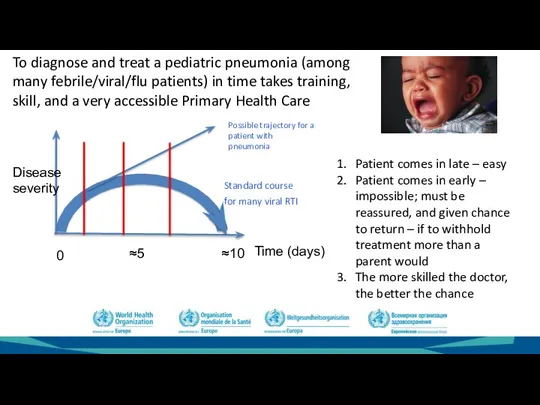
- 33. Time (days) Disease severity 0 ≈5 ≈10 To diagnose and treat a pediatric pneumonia (among many
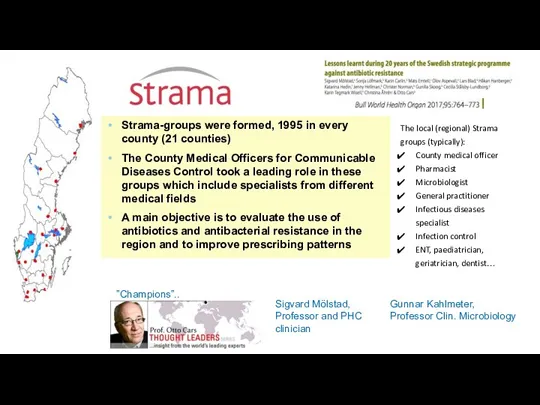
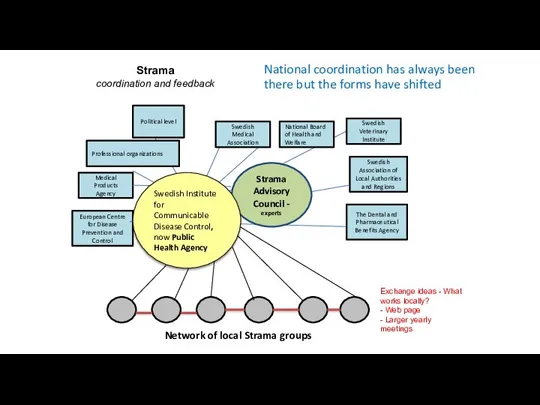
- 34. Strama-groups were formed, 1995 in every county (21 counties) The County Medical Officers for Communicable Diseases
- 35. Strama Advisory Council - experts Swedish Medical Association National Board of Health and Welfare Swedish Veterinary
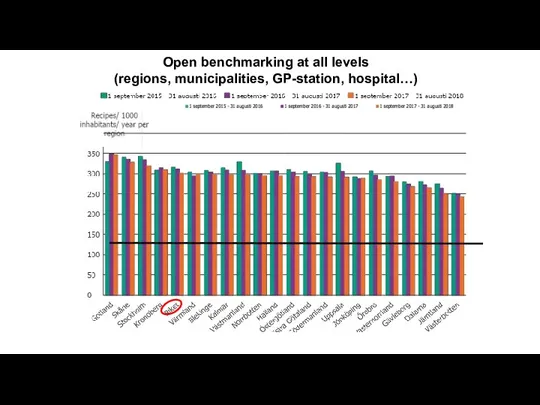
- 36. Open benchmarking at all levels (regions, municipalities, GP-station, hospital…)
- 37. Some LEAD WORDS – possible success factors in the implementation work of Strama Local engagement Network:
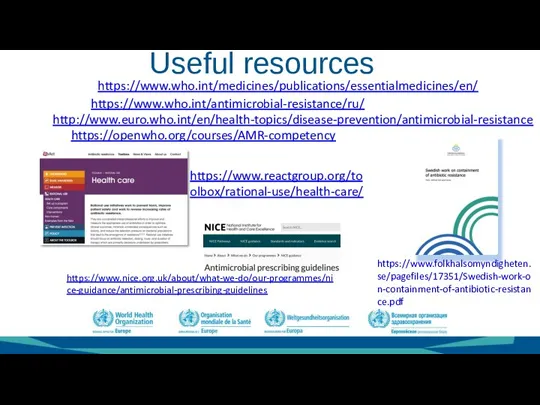
- 38. Useful resources https://www.nice.org.uk/about/what-we-do/our-programmes/nice-guidance/antimicrobial-prescribing-guidelines https://www.who.int/antimicrobial-resistance/ru/ http://www.euro.who.int/en/health-topics/disease-prevention/antimicrobial-resistance https://www.who.int/medicines/publications/essentialmedicines/en/ https://openwho.org/courses/AMR-competency https://www.folkhalsomyndigheten.se/pagefiles/17351/Swedish-work-on-containment-of-antibiotic-resistance.pdf https://www.reactgroup.org/toolbox/rational-use/health-care/
- 40. Скачать презентацию
Слайд 2Basic acronyms
AMR – antimicrobial resistance
Resistance to drugs against microbes: bacteria, virus, protozoan,
Basic acronyms
AMR – antimicrobial resistance
Resistance to drugs against microbes: bacteria, virus, protozoan,
Слайд 3Outline
Why ABS?
AMR is an increasing problem
Antibiotics are a limited resource
We need to
Outline
Why ABS?
AMR is an increasing problem
Antibiotics are a limited resource
We need to
Слайд 4Burden of AMR in Europe – a recent update
Cassini et al, The
Burden of AMR in Europe – a recent update
Cassini et al, The
Слайд 5Klein EY, Tseng KK, Pant S, et al
Tracking global trends in the effectiveness of
antibiotic therapy using
Klein EY, Tseng KK, Pant S, et al
Tracking global trends in the effectiveness of
antibiotic therapy using
Слайд 6Hip replacement
Organ transplants
Cancer chemotherapy
Care of preterm babies
Some of the Blessings of Modern
Hip replacement
Organ transplants
Cancer chemotherapy
Care of preterm babies
Some of the Blessings of Modern
Слайд 7MAKMAX/IACMAC 2009, Feb 18-19, Omsk
MAKMAX/IACMAC 2009, Feb 18-19, Omsk
Слайд 8Kaiser T, Finstermeier K, Häntzsch M, Faucheux S, Kaase M, Eckmanns T, et al. Stalking a lethal superbug by whole-genome sequencing and phylogenetics: Influence
Kaiser T, Finstermeier K, Häntzsch M, Faucheux S, Kaase M, Eckmanns T, et al. Stalking a lethal superbug by whole-genome sequencing and phylogenetics: Influence
Слайд 113. We need to buy us time until new classes of antibiotics
3. We need to buy us time until new classes of antibiotics
Слайд 12Antibiotic consumption drives antibiotic resistance
H. Goossens Lancet 2005; 365: 579–87
Antibiotic consumption drives antibiotic resistance
H. Goossens Lancet 2005; 365: 579–87
Слайд 13…
Conclusions: Individuals prescribed an antibiotic in primary care for a respiratory or
…
Conclusions: Individuals prescribed an antibiotic in primary care for a respiratory or
Слайд 14Where to work with ABS?
Infectious disease clinics – highly qualified, but small
Where to work with ABS?
Infectious disease clinics – highly qualified, but small
Слайд 15Total antibiotic pressure
Agri/Vet side
Human health sector
Country X
Total antibiotic pressure
Agri/Vet side
Human health sector
Country X
Слайд 16Hospital/in-patient use
Community use
Hospital/in-patient use
Community use

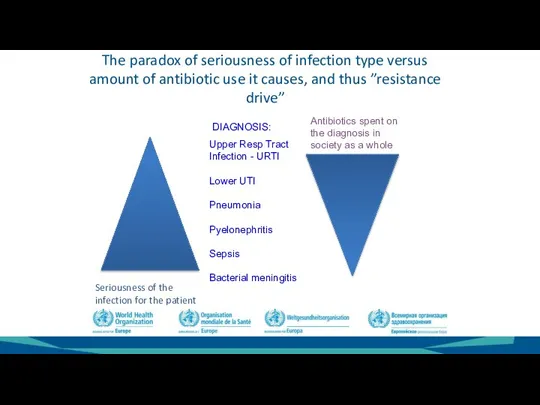
Слайд 17The paradox of seriousness of infection type versus
amount of antibiotic use
The paradox of seriousness of infection type versus amount of antibiotic use
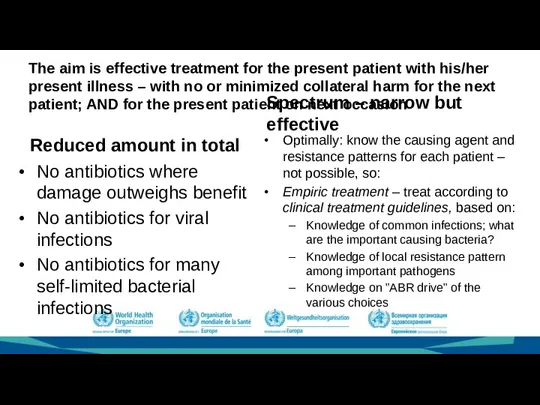
Слайд 18The aim is effective treatment for the present patient with his/her present
The aim is effective treatment for the present patient with his/her present
Слайд 19Total use – much to gain from stopping treatment of all viral
Total use – much to gain from stopping treatment of all viral
Слайд 20The TOTAL USE is easier to grasp and measure; but SPECTRUM is
The TOTAL USE is easier to grasp and measure; but SPECTRUM is
Слайд 21Rational antibiotic use
The right antibiotic (for the disease, bacterium, patient condition..)
At the
Rational antibiotic use
The right antibiotic (for the disease, bacterium, patient condition..)
At the
Слайд 22Antimicrobial stewardship programmes in health-care facilities in low- and middle-income countries. A
Antimicrobial stewardship programmes in health-care facilities in low- and middle-income countries. A
Слайд 23Tonsillopharyngitis: Strep A - 100 % sensitive to penicillin. We use pc
Tonsillopharyngitis: Strep A - 100 % sensitive to penicillin. We use pc
Слайд 24% survivors
Penicillin
Untreated
Days
Penicillin increased the chance of survival from 10% to 90%
Patients
% survivors
Penicillin
Untreated
Days
Penicillin increased the chance of survival from 10% to 90%
Patients
Слайд 25https://www.folkhalsomyndigheten.se/contentassets/e76b47c98f1a44058f22cfd4795a2c45/blod_ecoli_2017_nat.pdf
Swedish resistance surveillance build on
c:a 240 000 blood cultures/year
Swedish resistance surveillance
https://www.folkhalsomyndigheten.se/contentassets/e76b47c98f1a44058f22cfd4795a2c45/blod_ecoli_2017_nat.pdf
Swedish resistance surveillance build on
c:a 240 000 blood cultures/year
Swedish resistance surveillance
Слайд 29Clinical Treatment Guidelines/Treatment Protocols in infections
Generation I
Focus on infections dangerous to society
Examples:
Clinical Treatment Guidelines/Treatment Protocols in infections
Generation I
Focus on infections dangerous to society
Examples:
Слайд 30The process of developing Clinical Treatment Guidelines into a format useful in
The process of developing Clinical Treatment Guidelines into a format useful in
Слайд 31Challenge: Local implementation!
Getting the CTG:s in place is not enough
Nothing changes until
Challenge: Local implementation!
Getting the CTG:s in place is not enough
Nothing changes until
Слайд 322000
2007
2008
2010
2013
2019
1995
Slide courtesy of dr Christer Norman, PHC ”Salem”, Sthlm, and PHA
Expedited antibiotic
2000
2007
2008
2010
2013
2019
1995
Slide courtesy of dr Christer Norman, PHC ”Salem”, Sthlm, and PHA
Expedited antibiotic
Слайд 33Time (days)
Disease
severity
0
≈5
≈10
To diagnose and treat a pediatric pneumonia (among many
Time (days)
Disease
severity
0
≈5
≈10
To diagnose and treat a pediatric pneumonia (among many
Слайд 34Strama-groups were formed, 1995 in every county (21 counties)
The County Medical Officers
Strama-groups were formed, 1995 in every county (21 counties)
The County Medical Officers
Слайд 35Strama Advisory Council -
experts
Swedish
Medical
Association
National Board of Health and Welfare
Swedish
Veterinary
Institute
Swedish
Association of Local Authorities
Strama Advisory Council -
experts
Swedish
Medical
Association
National Board of Health and Welfare
Swedish
Veterinary
Institute
Swedish
Association of Local Authorities
Слайд 36Open benchmarking at all levels
(regions, municipalities, GP-station, hospital…)
Open benchmarking at all levels
(regions, municipalities, GP-station, hospital…)
Слайд 37Some LEAD WORDS – possible success factors in the implementation work of
Some LEAD WORDS – possible success factors in the implementation work of
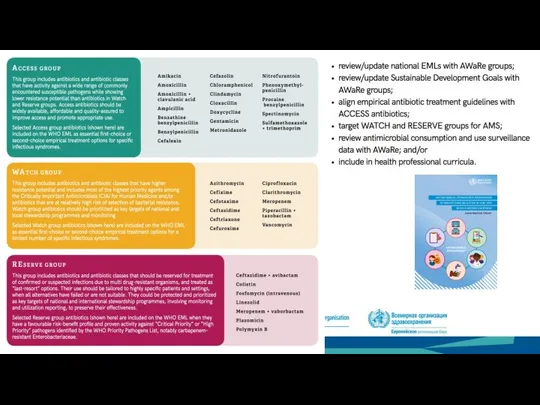
Слайд 38Useful resources
https://www.nice.org.uk/about/what-we-do/our-programmes/nice-guidance/antimicrobial-prescribing-guidelines
https://www.who.int/antimicrobial-resistance/ru/
http://www.euro.who.int/en/health-topics/disease-prevention/antimicrobial-resistance
https://www.who.int/medicines/publications/essentialmedicines/en/
https://openwho.org/courses/AMR-competency
https://www.folkhalsomyndigheten.se/pagefiles/17351/Swedish-work-on-containment-of-antibiotic-resistance.pdf
https://www.reactgroup.org/toolbox/rational-use/health-care/
Useful resources
https://www.nice.org.uk/about/what-we-do/our-programmes/nice-guidance/antimicrobial-prescribing-guidelines
https://www.who.int/antimicrobial-resistance/ru/
http://www.euro.who.int/en/health-topics/disease-prevention/antimicrobial-resistance
https://www.who.int/medicines/publications/essentialmedicines/en/
https://openwho.org/courses/AMR-competency
https://www.folkhalsomyndigheten.se/pagefiles/17351/Swedish-work-on-containment-of-antibiotic-resistance.pdf
https://www.reactgroup.org/toolbox/rational-use/health-care/
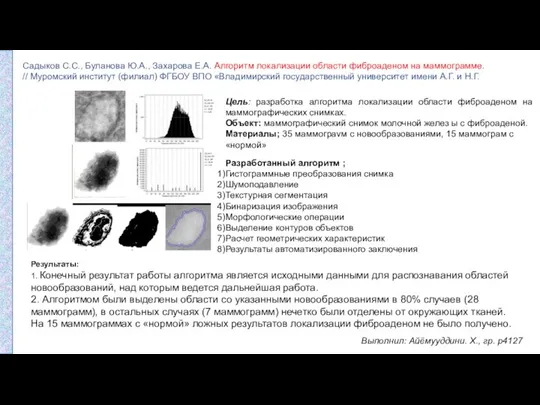 Алгоритм локализации области фиброаденом на маммограмме
Алгоритм локализации области фиброаденом на маммограмме Садықбек Адамбеков. Атындағы жалпы орта мектебі
Садықбек Адамбеков. Атындағы жалпы орта мектебі Максимально очищенные фитопрепараты и индивидуальные соединения. Препарат Фламин
Максимально очищенные фитопрепараты и индивидуальные соединения. Препарат Фламин Medical academy named after
Medical academy named after Трансперинеальная биопсия и Fusion-биопсия
Трансперинеальная биопсия и Fusion-биопсия Methadone pharmacogenetics
Methadone pharmacogenetics Репродуктивное здоровье. Профилактика ИППП
Репродуктивное здоровье. Профилактика ИППП Эффекты и механизмы действия вакуума на ткани раны
Эффекты и механизмы действия вакуума на ткани раны Аутосомно-доминантное наследование
Аутосомно-доминантное наследование Вопросы общей онкологии
Вопросы общей онкологии Легионелла. Экология. Таралуы. Патогендігі. Иммунитет. Лабораториялық диагностика. Профилактика мен емі
Легионелла. Экология. Таралуы. Патогендігі. Иммунитет. Лабораториялық диагностика. Профилактика мен емі Медицинская протозоология
Медицинская протозоология Синдром системной воспалительной реакции - SIRS
Синдром системной воспалительной реакции - SIRS Диета при заболеваниях органов пищеварения
Диета при заболеваниях органов пищеварения Чума
Чума Миома матки
Миома матки Как защитить детей от коронавируса в период снятия ограничений
Как защитить детей от коронавируса в период снятия ограничений Гигиена питания и воды
Гигиена питания и воды Приступ бронхиальной астмы у детей
Приступ бронхиальной астмы у детей Простые реакции антиген-антитело
Простые реакции антиген-антитело Повышение стрессоустойчивости с новым набором от НСП Антистресс
Повышение стрессоустойчивости с новым набором от НСП Антистресс Юридические аспекты оказания психиатрической помощи
Юридические аспекты оказания психиатрической помощи Дифференцированные подходы к терапии ФПН при экстрагенитальных заболеваниях
Дифференцированные подходы к терапии ФПН при экстрагенитальных заболеваниях Порядок проведения профилактических медицинских осмотров обучающихся в общеобразовательных организациях
Порядок проведения профилактических медицинских осмотров обучающихся в общеобразовательных организациях Атипичные пневмонии
Атипичные пневмонии Профилактика тромбозов вен нижних конечностей
Профилактика тромбозов вен нижних конечностей Биохимическое исследование функции желудочно-кишечного тракта
Биохимическое исследование функции желудочно-кишечного тракта prezentatsia_Obsledovanie_rebenka
prezentatsia_Obsledovanie_rebenka