- Congenital torticollis

Содержание
- 2. Fibrosis or shortening of the sternomastoid muscle found in infants the head is contralateral rotated and
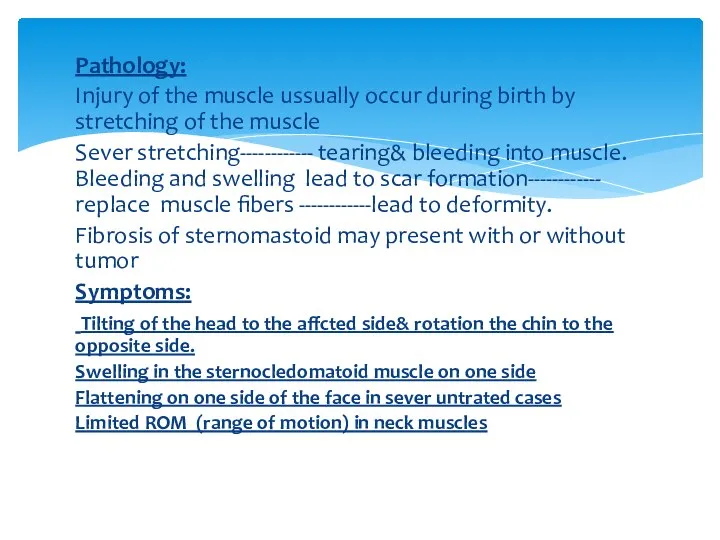
- 3. Symptoms: Head positioned in the characteristic fashion - The head is tilted toward the affected side
- 4. Etiology: The cause of torticollis is unknown, there are several theories , the most advanced one
- 5. Intrauterine pressure on the neck due to positioning in the womb Trauma to sternomastoid lead to
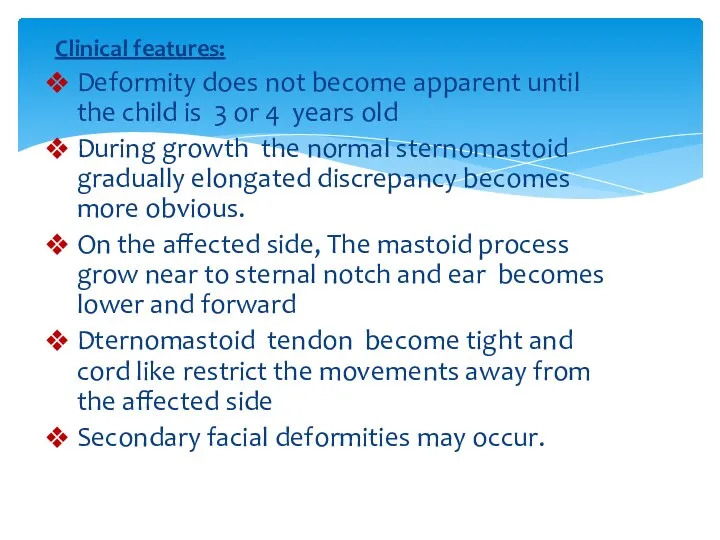
- 6. Clinical features: Deformity does not become apparent until the child is 3 or 4 years old
- 7. Pathology: Injury of the muscle ussually occur during birth by stretching of the muscle Sever stretching------------
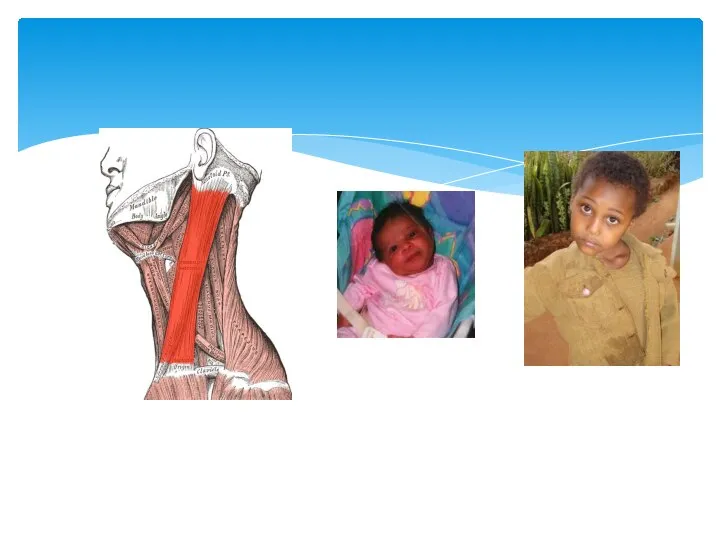
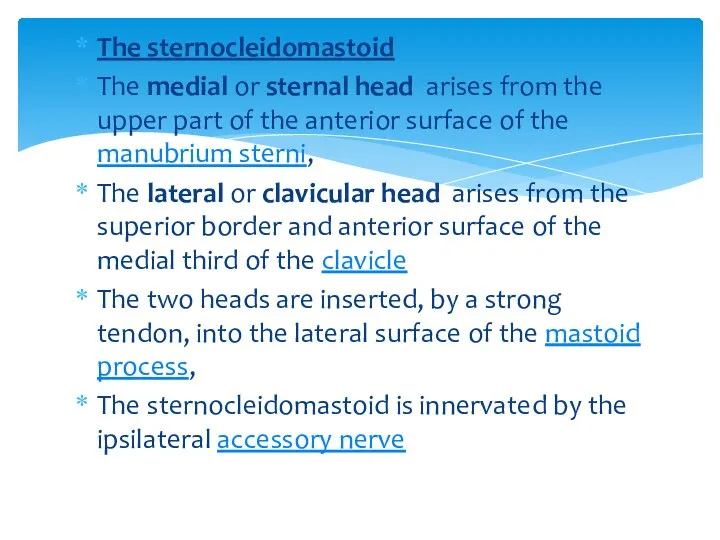
- 9. The sternocleidomastoid The medial or sternal head arises from the upper part of the anterior surface
- 10. Physical Therapy management: A)Evaluation History: trauma, pain, birth history Position of the head in relation to
- 12. P.T treatment Goals: prevent development of contracture Stretch tight muscles Strength the antagonist muscles including contralateral
- 13. P.T modalities: Ice, ultrasound, massage and stretching are all effective in reducing spasm. Instructions in posture
- 14. 1) Passive Stretching: Baby position: The baby is placed on a padded table in supine with
- 15. Another method of Stretching: The baby is resting on therapist arms in side lying position with
- 16. Home routine: Explain to parent not only the purpose of the treatment but also the practical
- 18. Скачать презентацию
Слайд 3Symptoms:
Head positioned in the characteristic fashion
- The head is tilted
Symptoms:
Head positioned in the characteristic fashion
- The head is tilted
Слайд 4Etiology:
The cause of torticollis is unknown, there are several theories ,
Etiology:
The cause of torticollis is unknown, there are several theories ,
Слайд 5Intrauterine pressure on the neck due to positioning in the womb
Trauma to
Intrauterine pressure on the neck due to positioning in the womb
Trauma to
Слайд 6Clinical features:
Deformity does not become apparent until the child is 3 or
Clinical features:
Deformity does not become apparent until the child is 3 or
Слайд 7Pathology:
Injury of the muscle ussually occur during birth by stretching of the
Pathology:
Injury of the muscle ussually occur during birth by stretching of the
Слайд 9The sternocleidomastoid
The medial or sternal head arises from the upper part
The sternocleidomastoid
The medial or sternal head arises from the upper part
Слайд 10Physical Therapy management:
A)Evaluation
History: trauma, pain, birth history
Position of the head in relation
Physical Therapy management:
A)Evaluation
History: trauma, pain, birth history
Position of the head in relation

Слайд 12P.T treatment
Goals:
prevent development of contracture
Stretch tight muscles
Strength the antagonist muscles including
P.T treatment
Goals:
prevent development of contracture
Stretch tight muscles
Strength the antagonist muscles including
Слайд 13P.T modalities:
Ice, ultrasound, massage and stretching are all effective in reducing spasm.
Instructions
P.T modalities:
Ice, ultrasound, massage and stretching are all effective in reducing spasm.
Instructions
Слайд 141) Passive Stretching:
Baby position: The baby is placed on a padded table
1) Passive Stretching:
Baby position: The baby is placed on a padded table
Слайд 15Another method of Stretching:
The baby is resting on therapist arms in side
Another method of Stretching:
The baby is resting on therapist arms in side
Слайд 16Home routine:
Explain to parent not only the purpose of the treatment but
Home routine:
Explain to parent not only the purpose of the treatment but
 Кроссворд медицинский
Кроссворд медицинский Биомикроскопия глаза
Биомикроскопия глаза Симптомы и синдромы при заболеваниях желудка. Хронический гастрит, язва желудка и 12-перстной кишки
Симптомы и синдромы при заболеваниях желудка. Хронический гастрит, язва желудка и 12-перстной кишки Синдром Туретта
Синдром Туретта Медиация в нашей жизни
Медиация в нашей жизни Сердечно-легочная реанимация собак и кошек
Сердечно-легочная реанимация собак и кошек Осмотические диуретики
Осмотические диуретики Легочные стронгилятозы жвачных
Легочные стронгилятозы жвачных Организация санитарно-противоэпидемического обеспечения в чрезвычайных ситуациях. Тема № 8
Организация санитарно-противоэпидемического обеспечения в чрезвычайных ситуациях. Тема № 8 Артроскопия – что это такое?
Артроскопия – что это такое? Синдром нервной анорексии
Синдром нервной анорексии Неотложные состояния в диабетологии
Неотложные состояния в диабетологии Инфекция
Инфекция Оценка состояния сознание при воспалении челюстно-лицевой области
Оценка состояния сознание при воспалении челюстно-лицевой области SMAS-лифтинг
SMAS-лифтинг Омфалоцеле емі
Омфалоцеле емі Лейкоцитарная формула - стихи для запоминания
Лейкоцитарная формула - стихи для запоминания Лимфоидная ткань
Лимфоидная ткань Профилактика, диагностика и лечение осложнений после введения филлеров на основе гиалуроновой кислоты (ГК)
Профилактика, диагностика и лечение осложнений после введения филлеров на основе гиалуроновой кислоты (ГК) Краткий обзор московской конференции Аутизм: вызовы и решения. Методы альтернативной речи
Краткий обзор московской конференции Аутизм: вызовы и решения. Методы альтернативной речи Клинико-эпидемиологическая характеристика дебюта рассеянного склероза в Рязанской области
Клинико-эпидемиологическая характеристика дебюта рассеянного склероза в Рязанской области Системные васкулиты
Системные васкулиты Результаты исследования кремов с антивозрастным эффектом
Результаты исследования кремов с антивозрастным эффектом Лечение среднего кариеса. Техника наложения постоянной пломбы из композита химического и светового отверждения
Лечение среднего кариеса. Техника наложения постоянной пломбы из композита химического и светового отверждения Артериальная гипертензия
Артериальная гипертензия Antidepressants
Antidepressants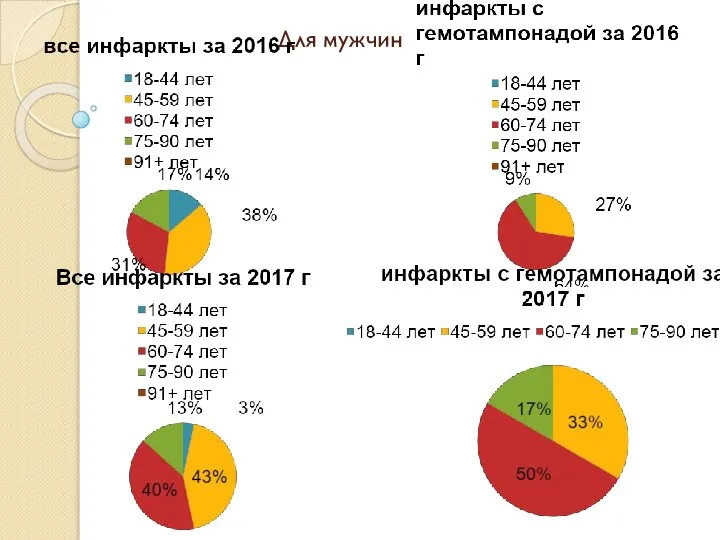 Инфаркты с гемотампонадой
Инфаркты с гемотампонадой Гепатит. Найпоширеніші види
Гепатит. Найпоширеніші види