- Disorders of the Cornea, Sclera and Orbit

Содержание
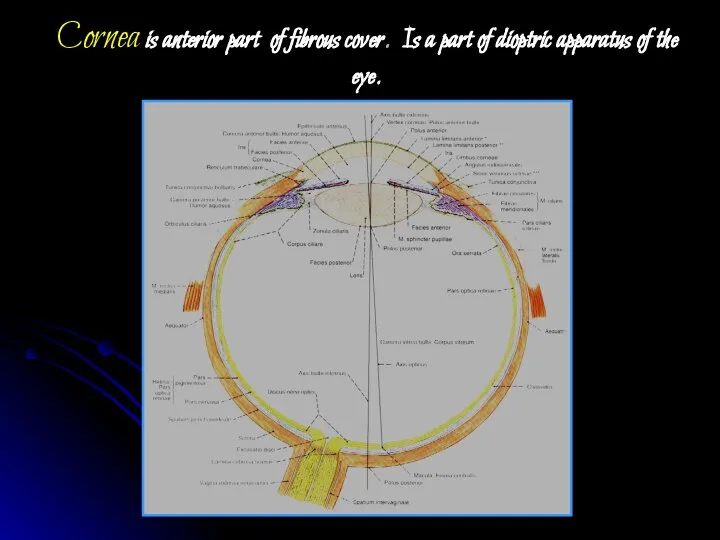
- 2. Cornea is anterior part of fibrous cover. Is a part of dioptric apparatus of the eye.
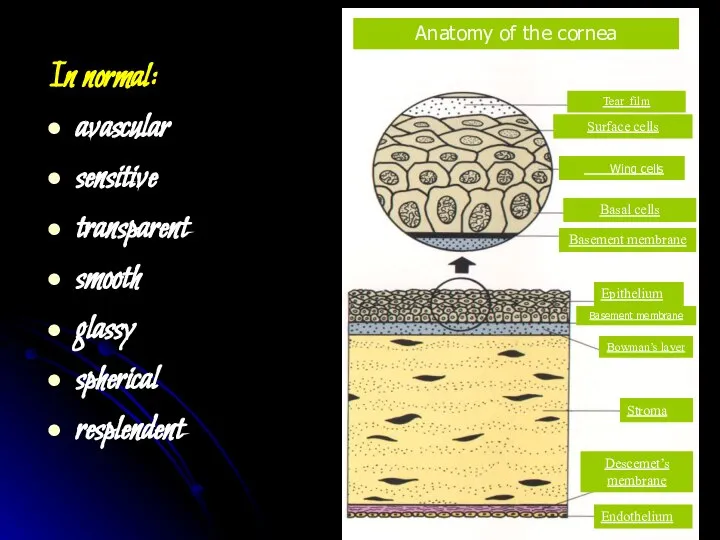
- 3. In normal: avascular sensitive transparent smooth glassy spherical resplendent
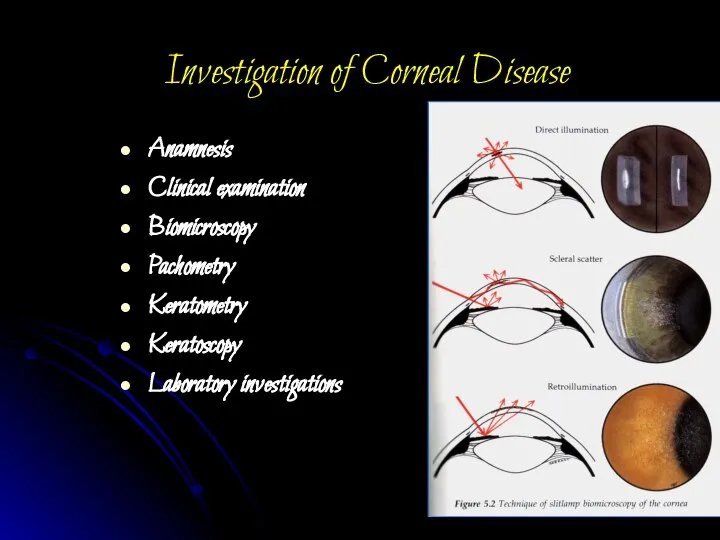
- 5. Investigation of Corneal Disease Anamnesis Clinical examination Biomicroscopy Pachometry Keratometry Keratoscopy Laboratory investigations
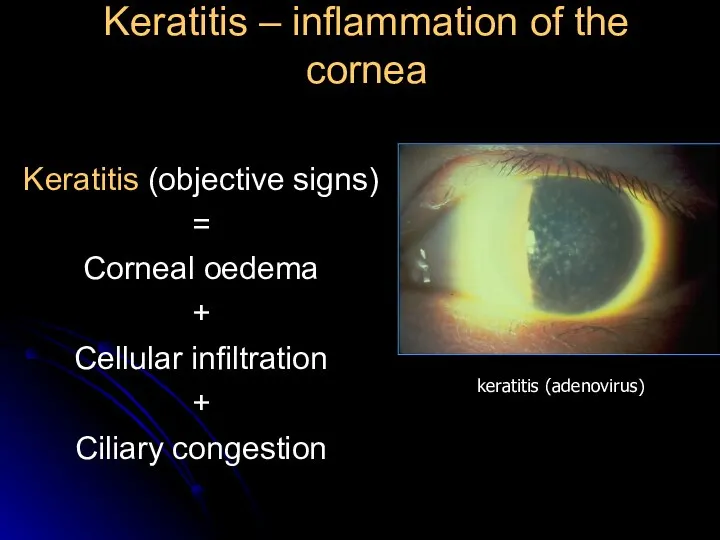
- 6. Keratitis – inflammation of the cornea Keratitis (objective signs) = Corneal oedema + Cellular infiltration +
- 7. Corneal syndrome photophobia lacrimation blepharospasm a sensation of a foreign body present behind the eyelids pain
- 8. Classification 1. Exogenous keratitis Corneal erosions Traumatic keratitis Bacterial keratitis Keratitis, caused by disease of conjunctiva,
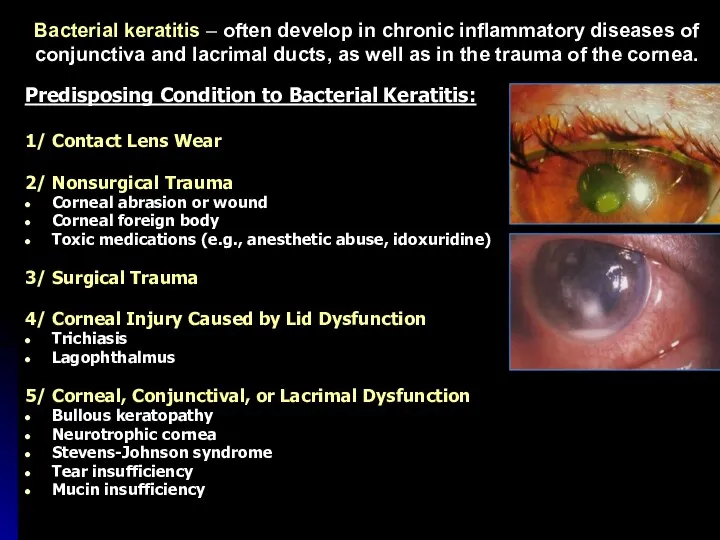
- 9. Bacterial keratitis – often develop in chronic inflammatory diseases of conjunctiva and lacrimal ducts, as well
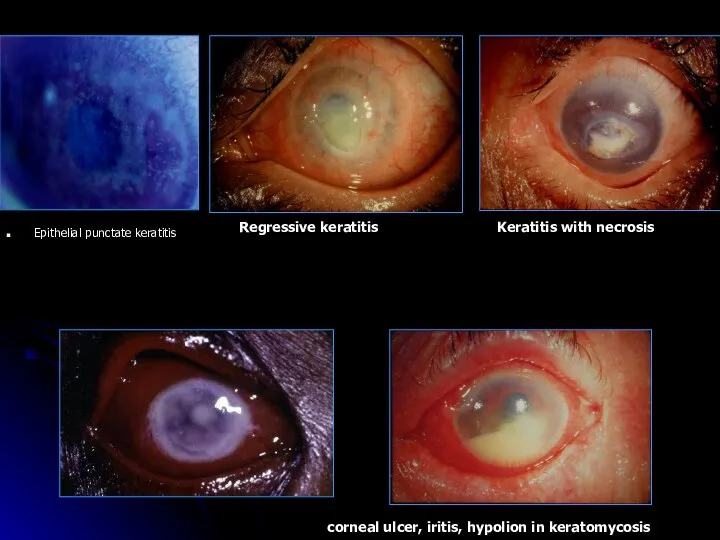
- 10. Epithelial punctate keratitis Keratitis with necrosis Regressive keratitis corneal ulcer, iritis, hypolion in keratomycosis
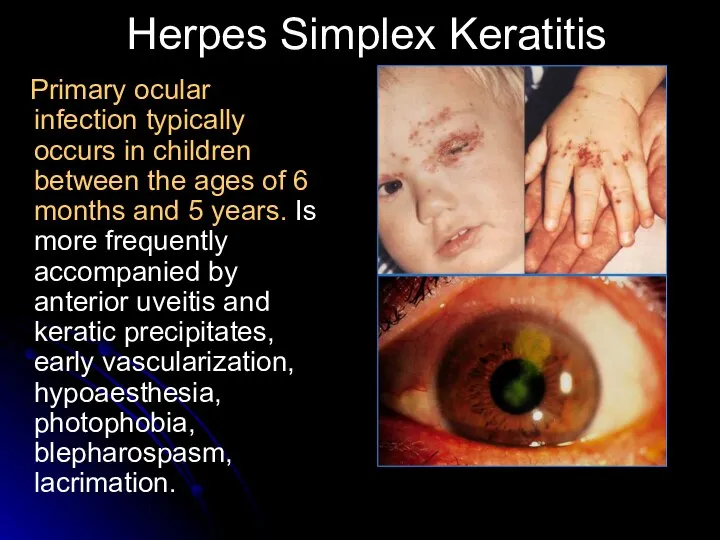
- 11. Herpes Simplex Keratitis Primary ocular infection typically occurs in children between the ages of 6 months
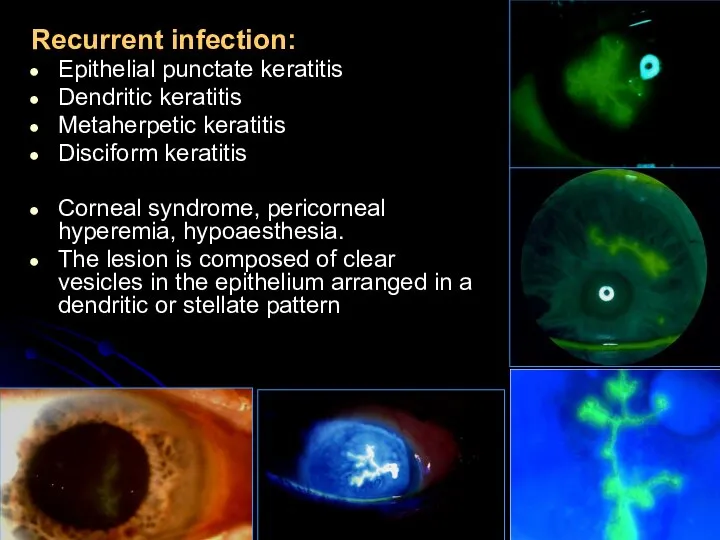
- 12. Recurrent infection: Epithelial punctate keratitis Dendritic keratitis Metaherpetic keratitis Disciform keratitis Corneal syndrome, pericorneal hyperemia, hypoaesthesia.
- 13. additional investigations of patients with keratitis review roentgenography of the additional nasal sinus and organs of
- 14. Laboratory diagnosis Herpeviral Express-diagnosis-method of fluorescining antibodies – revealing of virus in the scrub of conjunctiva
- 15. The differential diagnosis of primary ocular infection includes: 1. Keratitis with lid lesions: zoster, chickenpox, molluscum
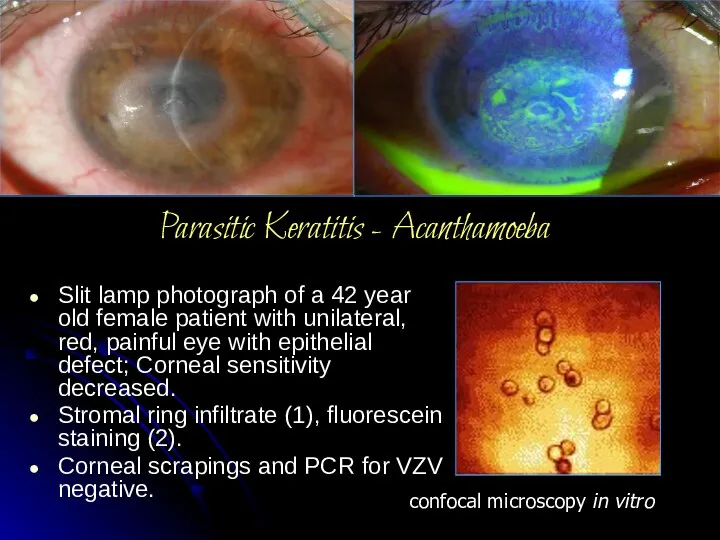
- 16. Parasitic Keratitis - Acanthamoeba Slit lamp photograph of a 42 year old female patient with unilateral,
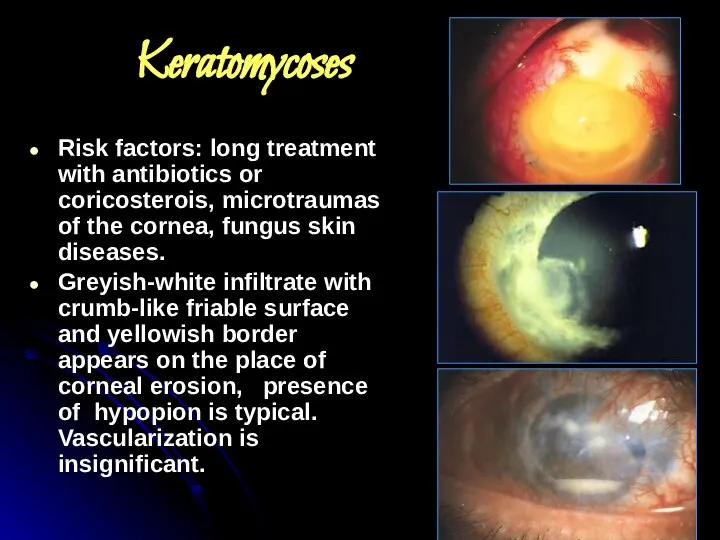
- 17. Keratomycoses Risk factors: long treatment with antibiotics or coricosterois, microtraumas of the cornea, fungus skin diseases.
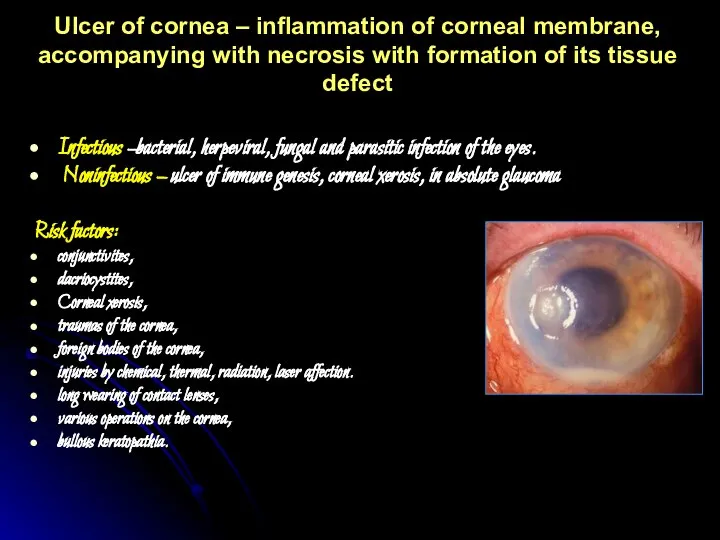
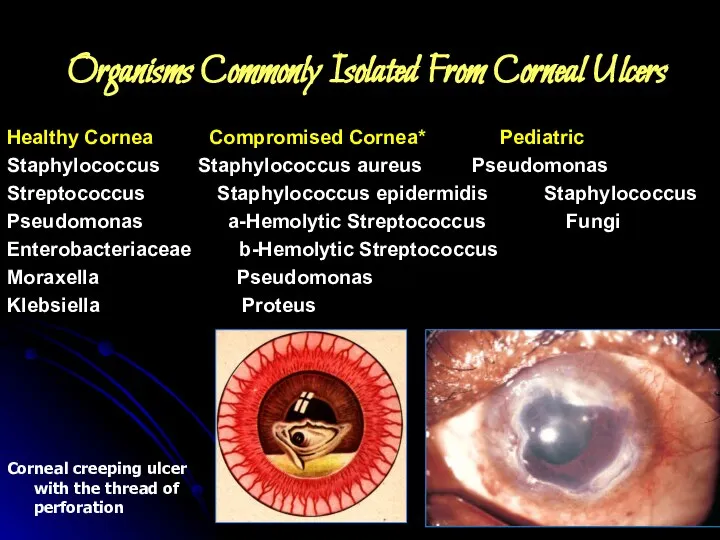
- 18. Ulcer of cornea – inflammation of corneal membrane, accompanying with necrosis with formation of its tissue
- 19. Organisms Commonly Isolated From Corneal Ulcers Healthy Cornea Compromised Cornea* Pediatric Staphylococcus Staphylococcus aureus Pseudomonas Streptococcus
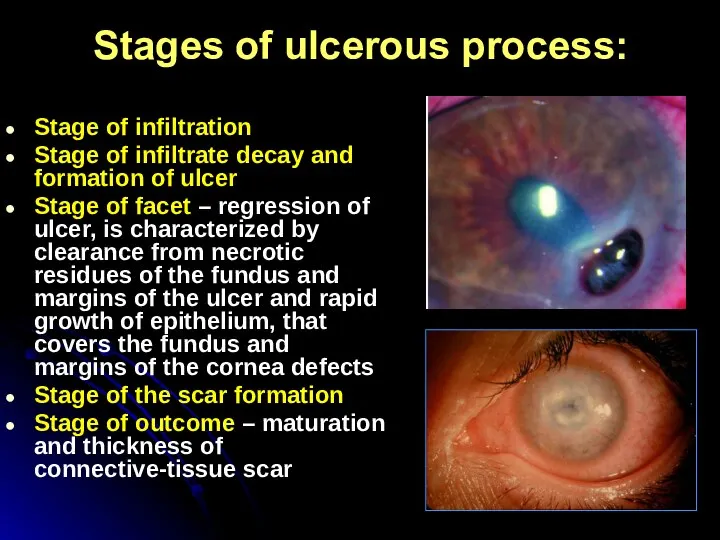
- 20. Stages of ulcerous process: Stage of infiltration Stage of infiltrate decay and formation of ulcer Stage
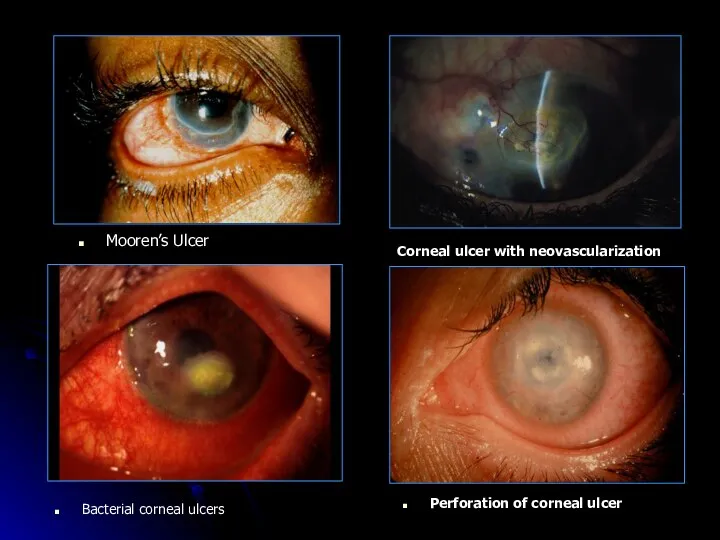
- 21. Mooren’s Ulcer Corneal ulcer with neovascularization Bacterial corneal ulcers Perforation of corneal ulcer
- 22. Principles of Keratitis and Corneal Ulcers treatment 1. Specific therapy: a) Antiviral (Zovirax, Aceclovir ointment 3%
- 23. 2. Pathogenetic therapy Antiinflammatory (Eye drops – only non-steroidal antiinflammatory: Naclof. Parabular or intravenous injection of
- 24. Following arresting of inflammatory process a course of resolving therapy (fibrinolysin, lidase) Penetrating keratoplasty indicated for
- 25. Complications of keratitis: limbal and scleral extension corneal perforation iridocyclitis endophthalmitis Panophthalmitis Secondary glaucoma Corneal scarring:
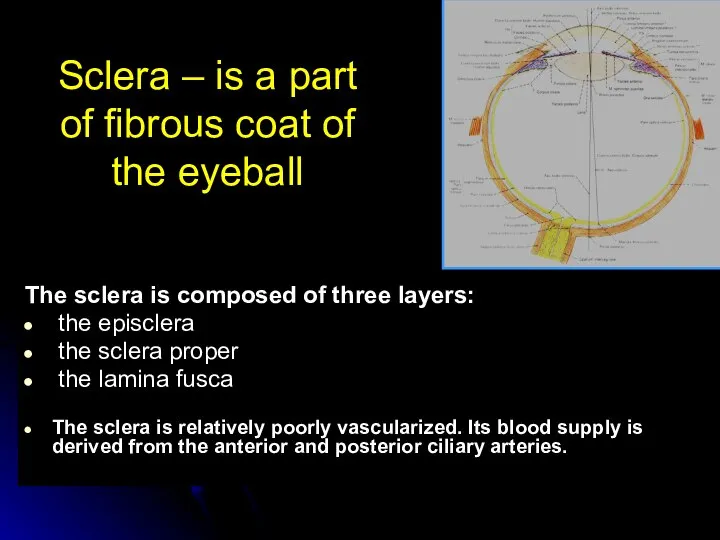
- 26. Sclera – is a part of fibrous coat of the eyeball The sclera is composed of
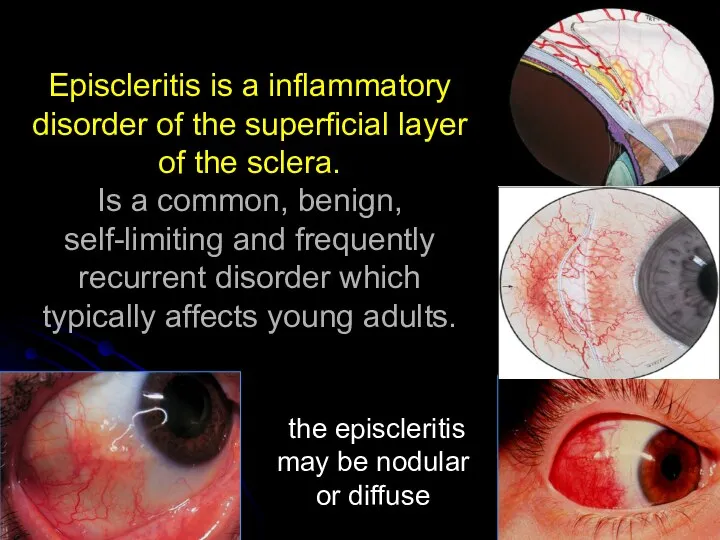
- 28. Episcleritis is a inflammatory disorder of the superficial layer of the sclera. Is a common, benign,
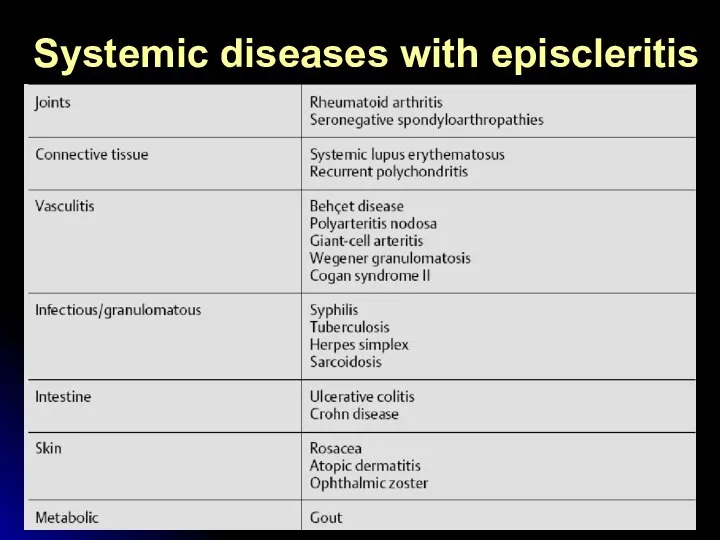
- 29. Systemic diseases with episcleritis
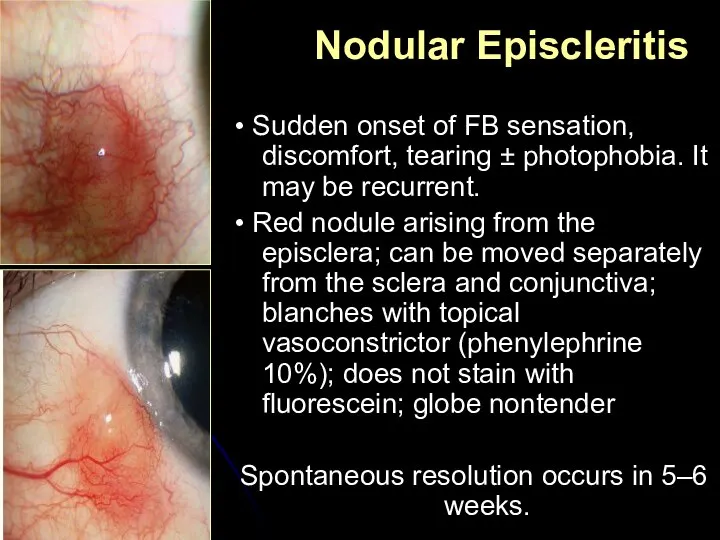
- 30. • Sudden onset of FB sensation, discomfort, tearing ± photophobia. It may be recurrent. • Red
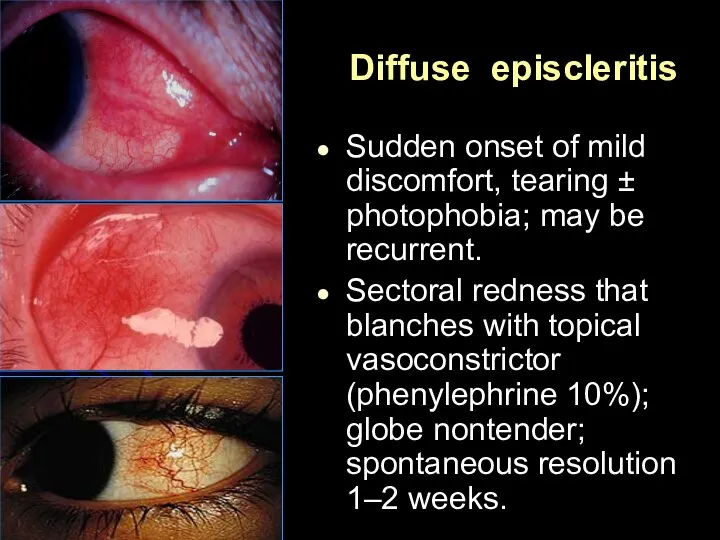
- 31. Diffuse episcleritis Sudden onset of mild discomfort, tearing ± photophobia; may be recurrent. Sectoral redness that
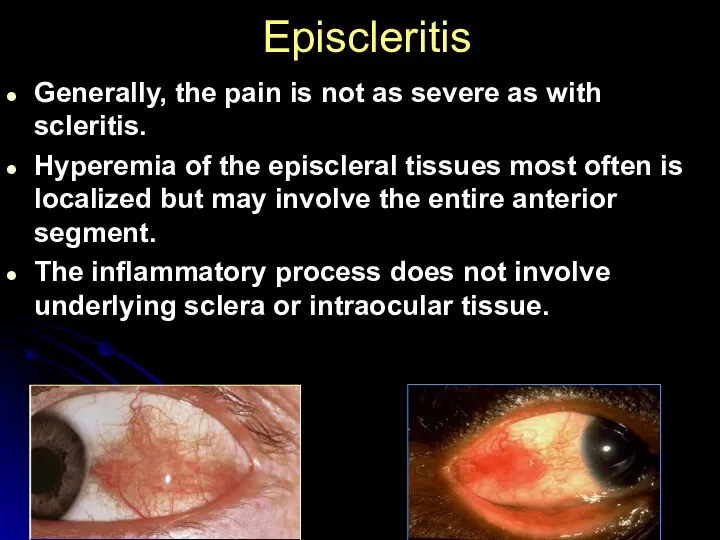
- 32. Episcleritis Generally, the pain is not as severe as with scleritis. Hyperemia of the episcleral tissues
- 33. Treatment If mild, no treatment is required. Supportive: reassurance ± cold compresses. Topical: consider lubricants ±
- 34. COMPLICATIONS Involvement of other ocular structures is rare in patients with episcleritis. The peripheral cornea can
- 35. COURSE AND PROGNOSIS Episcleritis is a mild, non-vision-threatening inflammation of the episclera that may recur over
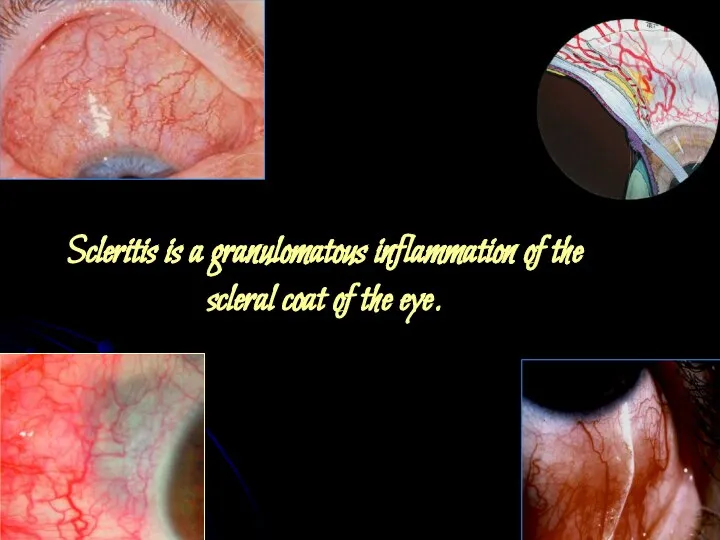
- 36. Scleritis is a granulomatous inflammation of the scleral coat of the eye.
- 37. Underlying systemic diseases Other causes: infection (e.g., syphilis, tuberculosis, bacterial, fungal, and herpes zoster). trauma, surgery
- 38. Scleritis Anterior scleritis Non-necrotizing Diffuse Nodular Necrotizing With inflammation Without inflammation Posterior scleritis Non-necrotizing Diffuse Nodular
- 39. Scleritis presents in the fourth to sixth decade with the gradual onset of classic symptoms of
- 40. Differentiation between episcleritis and scleritis
- 41. Posterior scleritis Posterior scleritis is a serious, potentially blinding condition, which is often misdiagnosed and treated
- 42. Drugs commonly used in the treatment of scleritis • Oral: NSAID (e.g., flurbiprofen 100 mg 3x/day;
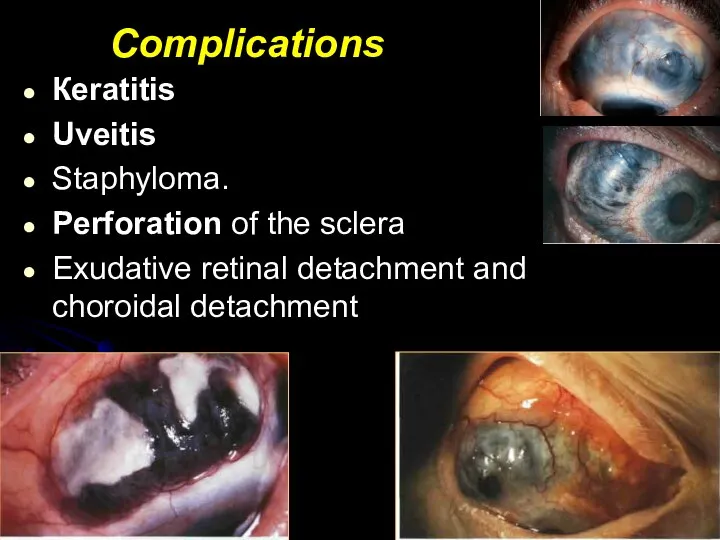
- 43. Complications Кeratitis Uveitis Staphyloma. Perforation of the sclera Exudative retinal detachment and choroidal detachment
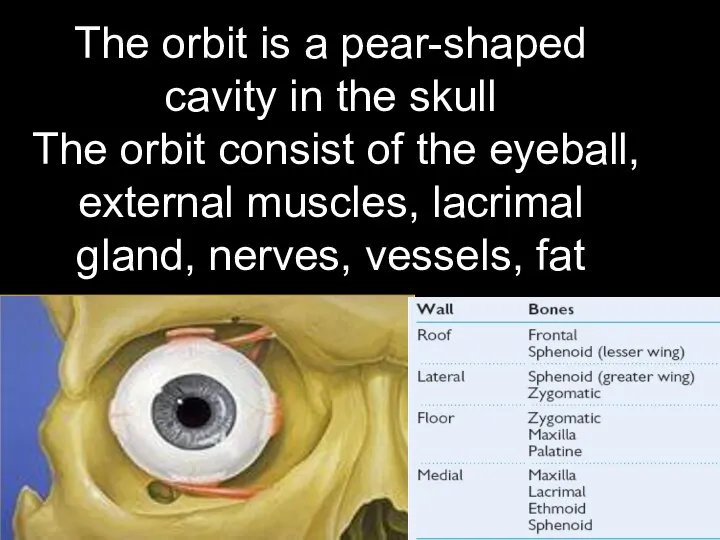
- 44. The orbit is a pear-shaped cavity in the skull The orbit consist of the eyeball, external
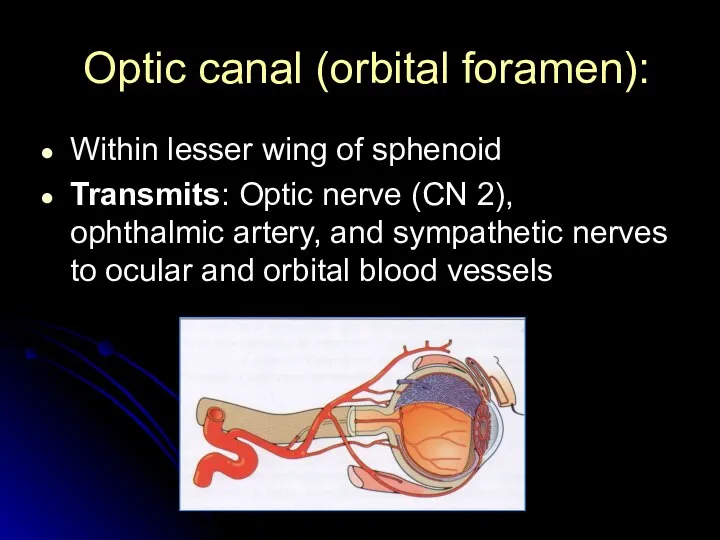
- 45. Optic canal (orbital foramen): Within lesser wing of sphenoid Transmits: Optic nerve (CN 2), ophthalmic artery,
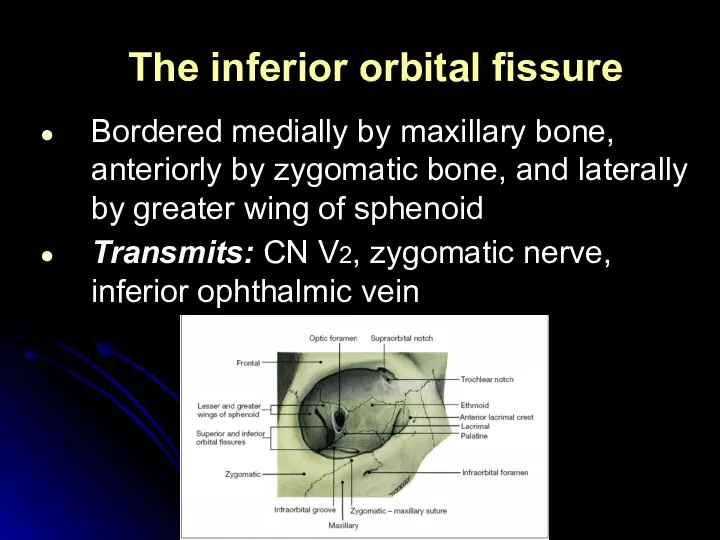
- 46. The inferior orbital fissure Bordered medially by maxillary bone, anteriorly by zygomatic bone, and laterally by
- 47. The superior orbital fissure is a slit linking the cranium and the orbit, between the greater
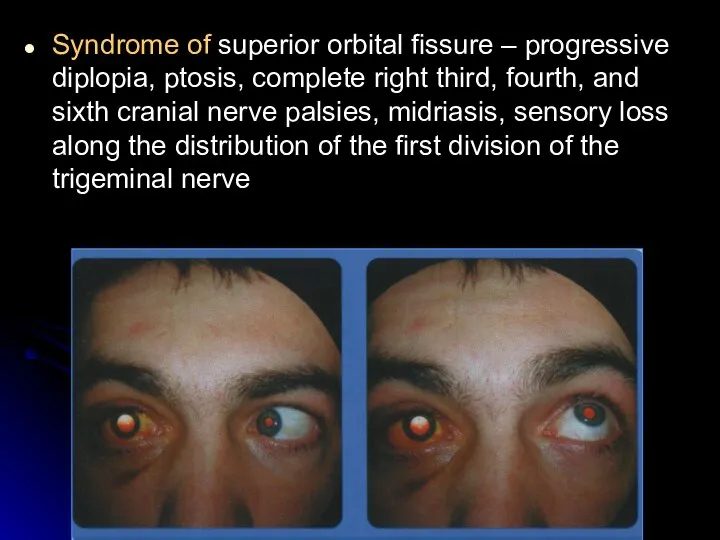
- 48. Syndrome of superior orbital fissure – progressive diplopia, ptosis, complete right third, fourth, and sixth cranial
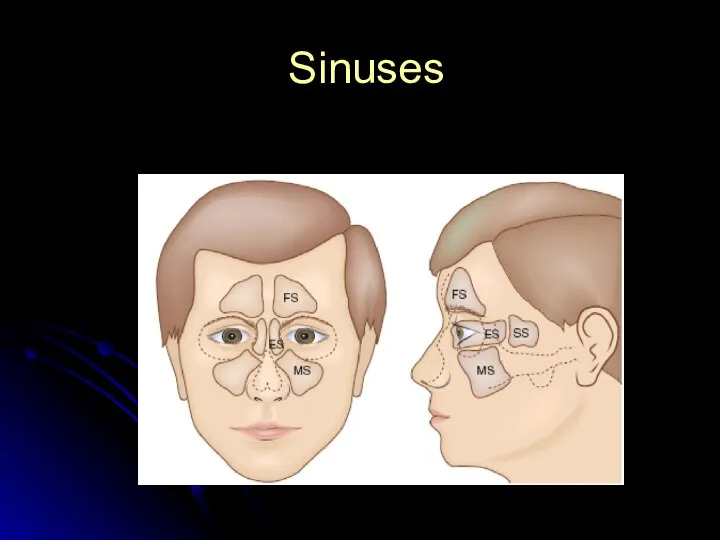
- 49. Sinuses
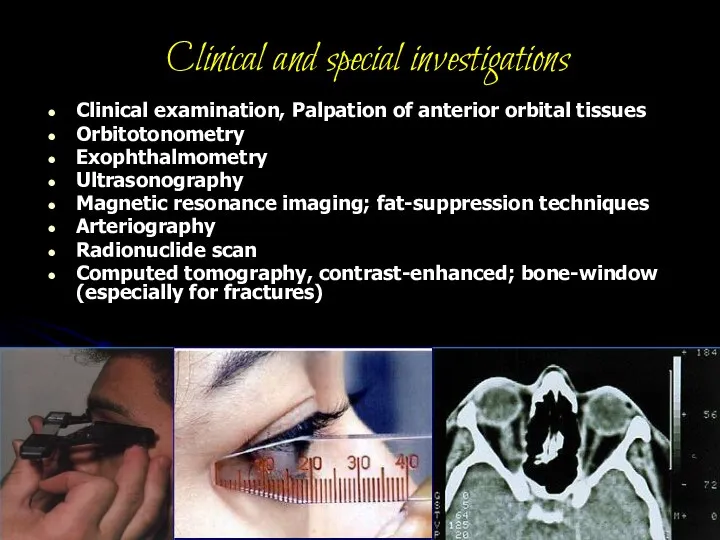
- 50. Clinical and special investigations Clinical examination, Palpation of anterior orbital tissues Orbitotonometry Exophthalmometry Ultrasonography Magnetic resonance
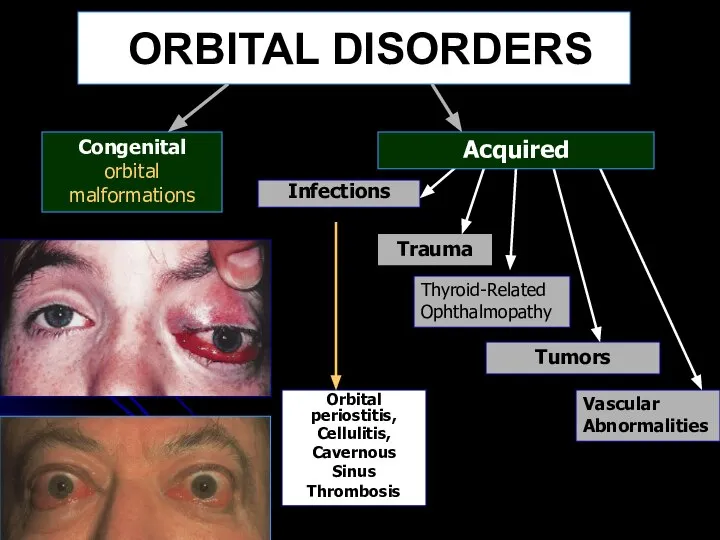
- 51. ORBITAL DISORDERS Congenital orbital malformations Infections Orbital periostitis, Cellulitis, Cavernous Sinus Thrombosis Trauma Thyroid-Related Ophthalmopathy Vascular
- 52. Osteoperiostitis It may result from injuries or as an extension of infection from the surrounding structures
- 53. Cellulitis - inflammation of the orbit
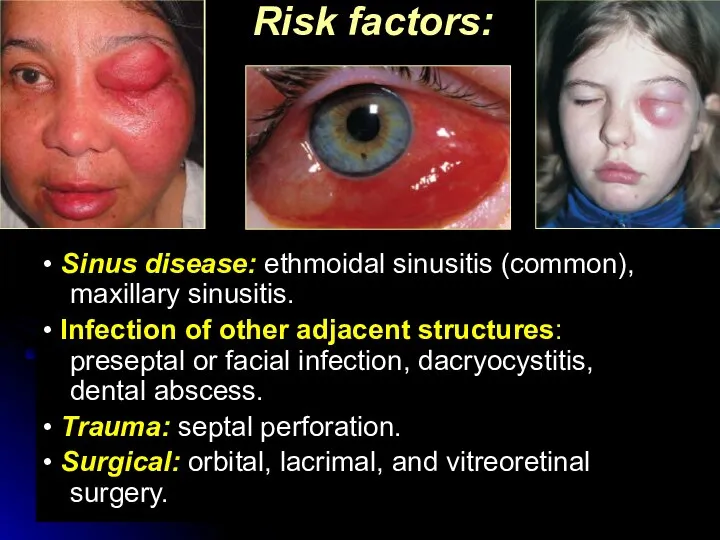
- 54. Risk factors: • Sinus disease: ethmoidal sinusitis (common), maxillary sinusitis. • Infection of other adjacent structures:
- 55. Symptoms include rapid onset of headache, fever, pain, nausea, in some cases – prostration. Eyelids are
- 56. Potential complications: Intracranial complications include meningitis, brain abscess and cavernosus sinus thrombosis Subperiorbital abscess (it is
- 57. Principles of treatment of inflammatory diseases of the orbit It is an emergency requiring hospital admission.
- 59. Скачать презентацию
Слайд 3In normal:
avascular
sensitive
transparent
smooth
glassy
spherical
resplendent
In normal:
avascular
sensitive
transparent
smooth
glassy
spherical
resplendent

Слайд 5Investigation of Corneal Disease
Anamnesis
Clinical examination
Biomicroscopy
Pachometry
Keratometry
Keratoscopy
Laboratory investigations
Investigation of Corneal Disease
Anamnesis
Clinical examination
Biomicroscopy
Pachometry
Keratometry
Keratoscopy
Laboratory investigations
Слайд 6Keratitis – inflammation of the cornea
Keratitis (objective signs)
=
Corneal oedema
+
Cellular infiltration
+
Ciliary congestion
keratitis
Keratitis – inflammation of the cornea
Keratitis (objective signs)
=
Corneal oedema
+
Cellular infiltration
+
Ciliary congestion
keratitis
Слайд 7Corneal syndrome
photophobia
lacrimation
blepharospasm
a sensation of a foreign body present behind the eyelids
pain
Corneal syndrome
photophobia
lacrimation
blepharospasm
a sensation of a foreign body present behind the eyelids
pain
Слайд 8Classification
1. Exogenous keratitis
Corneal erosions
Traumatic keratitis
Bacterial keratitis
Keratitis, caused by disease of
Classification
1. Exogenous keratitis
Corneal erosions
Traumatic keratitis
Bacterial keratitis
Keratitis, caused by disease of
Слайд 9Bacterial keratitis – often develop in chronic inflammatory diseases of conjunctiva and
Bacterial keratitis – often develop in chronic inflammatory diseases of conjunctiva and
Слайд 10Epithelial punctate keratitis
Keratitis with necrosis
Regressive keratitis
corneal ulcer, iritis, hypolion in
Epithelial punctate keratitis
Keratitis with necrosis
Regressive keratitis
corneal ulcer, iritis, hypolion in
Слайд 11Herpes Simplex Keratitis
Primary ocular infection typically occurs in children between the
Herpes Simplex Keratitis
Primary ocular infection typically occurs in children between the
Слайд 12Recurrent infection:
Epithelial punctate keratitis
Dendritic keratitis
Metaherpetic keratitis
Disciform keratitis
Corneal syndrome, pericorneal hyperemia, hypoaesthesia.
The
Recurrent infection:
Epithelial punctate keratitis
Dendritic keratitis
Metaherpetic keratitis
Disciform keratitis
Corneal syndrome, pericorneal hyperemia, hypoaesthesia.
The
Слайд 13additional investigations of patients with keratitis
review roentgenography of the additional nasal sinus
additional investigations of patients with keratitis
review roentgenography of the additional nasal sinus
Слайд 14Laboratory diagnosis
Herpeviral
Express-diagnosis-method of fluorescining antibodies – revealing of virus in the scrub
Laboratory diagnosis
Herpeviral
Express-diagnosis-method of fluorescining antibodies – revealing of virus in the scrub
Слайд 15The differential diagnosis of primary ocular infection includes:
1. Keratitis with lid lesions:
The differential diagnosis of primary ocular infection includes:
1. Keratitis with lid lesions:
Слайд 16Parasitic Keratitis - Acanthamoeba
Slit lamp photograph of a 42 year old female
Parasitic Keratitis - Acanthamoeba
Slit lamp photograph of a 42 year old female
Слайд 17Keratomycoses
Risk factors: long treatment with antibiotics or coricosterois, microtraumas of
Keratomycoses
Risk factors: long treatment with antibiotics or coricosterois, microtraumas of
Слайд 18Ulcer of cornea – inflammation of corneal membrane, accompanying with necrosis with
Ulcer of cornea – inflammation of corneal membrane, accompanying with necrosis with
Слайд 19Organisms Commonly Isolated From Corneal Ulcers
Healthy Cornea Compromised Cornea* Pediatric
Staphylococcus Staphylococcus aureus
Organisms Commonly Isolated From Corneal Ulcers
Healthy Cornea Compromised Cornea* Pediatric
Staphylococcus Staphylococcus aureus
Слайд 20Stages of ulcerous process:
Stage of infiltration
Stage of infiltrate decay and formation of
Stages of ulcerous process:
Stage of infiltration
Stage of infiltrate decay and formation of
Слайд 21Mooren’s Ulcer
Corneal ulcer with neovascularization
Bacterial corneal ulcers
Perforation of corneal ulcer
Mooren’s Ulcer
Corneal ulcer with neovascularization
Bacterial corneal ulcers
Perforation of corneal ulcer
Слайд 22Principles of Keratitis and Corneal Ulcers treatment
1. Specific therapy:
a) Antiviral (Zovirax, Aceclovir
Principles of Keratitis and Corneal Ulcers treatment
1. Specific therapy:
a) Antiviral (Zovirax, Aceclovir
Слайд 232. Pathogenetic therapy
Antiinflammatory (Eye drops – only non-steroidal antiinflammatory: Naclof. Parabular or
2. Pathogenetic therapy
Antiinflammatory (Eye drops – only non-steroidal antiinflammatory: Naclof. Parabular or
Слайд 24Following arresting of inflammatory process a course of resolving therapy (fibrinolysin, lidase)
Penetrating
Following arresting of inflammatory process a course of resolving therapy (fibrinolysin, lidase)
Penetrating

Слайд 25Complications of keratitis:
limbal and scleral extension
corneal perforation
iridocyclitis
endophthalmitis
Panophthalmitis
Secondary glaucoma
Corneal scarring:
Complications of keratitis:
limbal and scleral extension
corneal perforation
iridocyclitis
endophthalmitis
Panophthalmitis
Secondary glaucoma
Corneal scarring:
Слайд 26Sclera – is a part of fibrous coat of the eyeball
The sclera
Sclera – is a part of fibrous coat of the eyeball
The sclera

Слайд 28
Episcleritis is a inflammatory disorder of the superficial layer of the
Episcleritis is a inflammatory disorder of the superficial layer of the
Слайд 29Systemic diseases with episcleritis
Systemic diseases with episcleritis
Слайд 30• Sudden onset of FB sensation, discomfort, tearing ± photophobia. It may
• Sudden onset of FB sensation, discomfort, tearing ± photophobia. It may
Слайд 31Diffuse episcleritis
Sudden onset of mild discomfort, tearing ± photophobia; may be recurrent.
Diffuse episcleritis
Sudden onset of mild discomfort, tearing ± photophobia; may be recurrent.
Слайд 32Episcleritis
Generally, the pain is not as severe as with scleritis.
Hyperemia of
Episcleritis
Generally, the pain is not as severe as with scleritis.
Hyperemia of
Слайд 33Treatment
If mild, no treatment is required.
Supportive: reassurance ± cold compresses.
Topical: consider lubricants
Treatment
If mild, no treatment is required.
Supportive: reassurance ± cold compresses.
Topical: consider lubricants
Слайд 34COMPLICATIONS
Involvement of other ocular structures is rare in patients with episcleritis.
The
COMPLICATIONS
Involvement of other ocular structures is rare in patients with episcleritis.
The
Слайд 35COURSE AND PROGNOSIS
Episcleritis is a mild, non-vision-threatening inflammation of the episclera that
COURSE AND PROGNOSIS
Episcleritis is a mild, non-vision-threatening inflammation of the episclera that
Слайд 36Scleritis is a granulomatous inflammation of the scleral coat of the eye.
Scleritis is a granulomatous inflammation of the scleral coat of the eye.
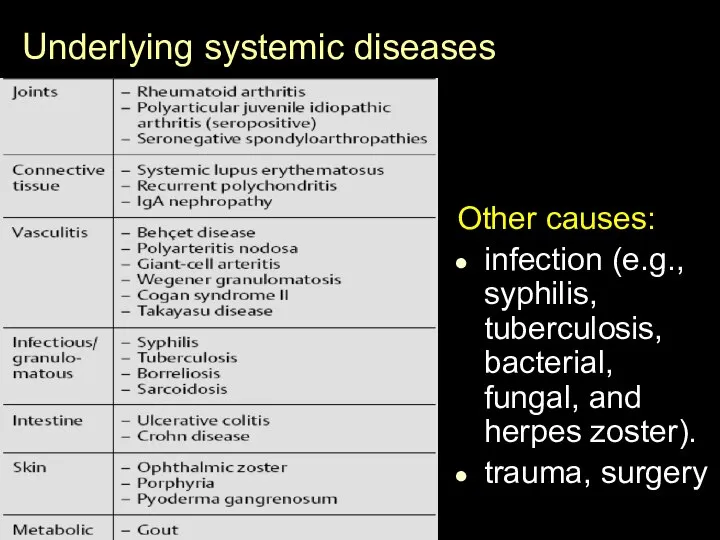
Слайд 37Underlying systemic diseases
Other causes:
infection (e.g., syphilis, tuberculosis, bacterial, fungal, and herpes zoster).
trauma,
Underlying systemic diseases
Other causes:
infection (e.g., syphilis, tuberculosis, bacterial, fungal, and herpes zoster).
trauma,
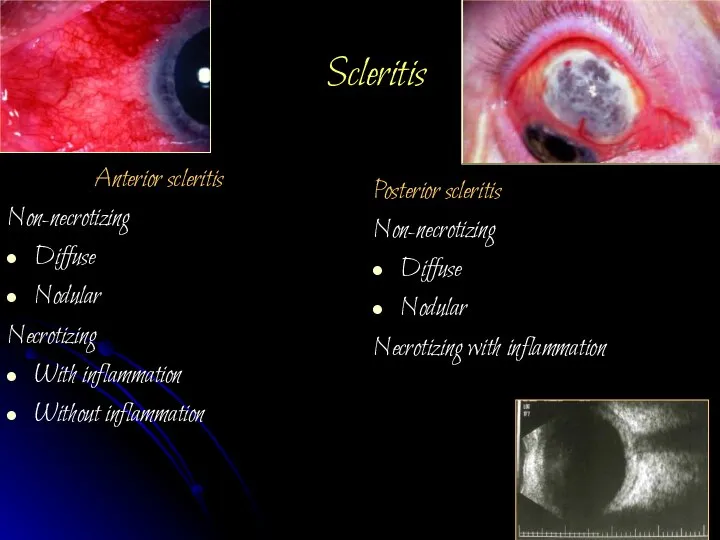
Слайд 38Scleritis
Anterior scleritis
Non-necrotizing
Diffuse
Nodular
Necrotizing
With inflammation
Without inflammation
Posterior scleritis
Non-necrotizing
Diffuse
Nodular
Necrotizing with inflammation
Scleritis
Anterior scleritis
Non-necrotizing
Diffuse
Nodular
Necrotizing
With inflammation
Without inflammation
Posterior scleritis
Non-necrotizing
Diffuse
Nodular
Necrotizing with inflammation
Слайд 39Scleritis presents in the fourth to sixth decade with the gradual onset
Scleritis presents in the fourth to sixth decade with the gradual onset

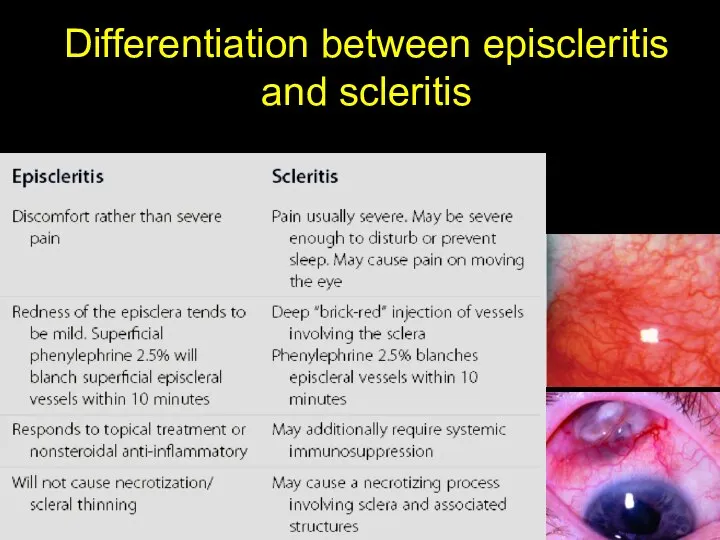
Слайд 40Differentiation between episcleritis and scleritis
Differentiation between episcleritis and scleritis
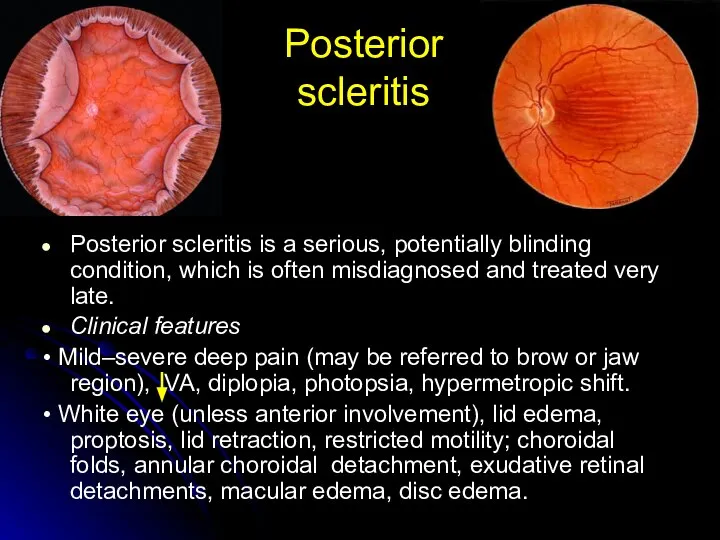
Слайд 41Posterior scleritis
Posterior scleritis is a serious, potentially blinding condition, which is often
Posterior scleritis
Posterior scleritis is a serious, potentially blinding condition, which is often
Слайд 42Drugs commonly used in the treatment of scleritis
• Oral: NSAID (e.g., flurbiprofen
Drugs commonly used in the treatment of scleritis
• Oral: NSAID (e.g., flurbiprofen
Слайд 43Complications
Кeratitis
Uveitis
Staphyloma.
Perforation of the sclera
Exudative retinal detachment and choroidal detachment
Complications
Кeratitis
Uveitis
Staphyloma.
Perforation of the sclera
Exudative retinal detachment and choroidal detachment
Слайд 44The orbit is a pear-shaped cavity in the skull
The orbit consist
The orbit is a pear-shaped cavity in the skull The orbit consist
Слайд 45Optic canal (orbital foramen):
Within lesser wing of sphenoid
Transmits: Optic nerve (CN 2),
Optic canal (orbital foramen):
Within lesser wing of sphenoid
Transmits: Optic nerve (CN 2),
Слайд 46The inferior orbital fissure
Bordered medially by maxillary bone, anteriorly by zygomatic bone,
The inferior orbital fissure
Bordered medially by maxillary bone, anteriorly by zygomatic bone,
Слайд 47The superior orbital fissure is a slit linking the
cranium and the orbit,
The superior orbital fissure is a slit linking the cranium and the orbit,
Слайд 48Syndrome of superior orbital fissure – progressive diplopia, ptosis, complete right third,
Syndrome of superior orbital fissure – progressive diplopia, ptosis, complete right third,
Слайд 49Sinuses
Sinuses
Слайд 50Clinical and special investigations
Clinical examination, Palpation of anterior orbital tissues
Orbitotonometry
Exophthalmometry
Ultrasonography
Magnetic resonance
Clinical and special investigations
Clinical examination, Palpation of anterior orbital tissues
Orbitotonometry
Exophthalmometry
Ultrasonography
Magnetic resonance
Слайд 51ORBITAL DISORDERS
Congenital orbital malformations
Infections
Orbital periostitis,
Cellulitis, Cavernous Sinus Thrombosis
Trauma
Thyroid-Related Ophthalmopathy
Vascular Abnormalities
Tumors
Acquired
ORBITAL DISORDERS
Congenital orbital malformations
Infections
Orbital periostitis,
Cellulitis, Cavernous Sinus Thrombosis
Trauma
Thyroid-Related Ophthalmopathy
Vascular Abnormalities
Tumors
Acquired
Слайд 52Osteoperiostitis
It may result from injuries or as an extension of infection from
Osteoperiostitis
It may result from injuries or as an extension of infection from
Слайд 53Cellulitis
- inflammation of the orbit
Cellulitis
- inflammation of the orbit

Слайд 54Risk factors:
• Sinus disease: ethmoidal sinusitis (common), maxillary sinusitis.
• Infection of other
Risk factors:
• Sinus disease: ethmoidal sinusitis (common), maxillary sinusitis.
• Infection of other
Слайд 55Symptoms include rapid onset of headache, fever, pain, nausea, in some cases
Symptoms include rapid onset of headache, fever, pain, nausea, in some cases
Слайд 56Potential complications:
Intracranial complications include meningitis, brain abscess and cavernosus sinus thrombosis
Subperiorbital abscess
Potential complications:
Intracranial complications include meningitis, brain abscess and cavernosus sinus thrombosis
Subperiorbital abscess
Слайд 57Principles of treatment of inflammatory diseases of the orbit
It is an emergency
Principles of treatment of inflammatory diseases of the orbit
It is an emergency
 Диагностика заболеваний периодонта. Электроодонтометрия
Диагностика заболеваний периодонта. Электроодонтометрия Осложнения имплантации электронных устройств
Осложнения имплантации электронных устройств Анализ крови при В12-дефицитной анемии. Макроцитоз, пойкилоцитоз, тельца Жолли и кольца Кэбота
Анализ крови при В12-дефицитной анемии. Макроцитоз, пойкилоцитоз, тельца Жолли и кольца Кэбота Цвет нас лечит и бодрит
Цвет нас лечит и бодрит Волчаночный нефрит
Волчаночный нефрит Эффективность лечения гломерулонефритов ингибиторами синтеза нуклеотидов
Эффективность лечения гломерулонефритов ингибиторами синтеза нуклеотидов Ғылыми зерттеу жүргізуде маманның құқықтары мен міндеттері
Ғылыми зерттеу жүргізуде маманның құқықтары мен міндеттері Терминоэлементы, обозначающие методы исследования, размер, количество
Терминоэлементы, обозначающие методы исследования, размер, количество Мерцательная аритмия
Мерцательная аритмия Правила личной гигиены и здоровье
Правила личной гигиены и здоровье Натуральное жаропонижающее Флю стоп+
Натуральное жаропонижающее Флю стоп+ Кома. Анатомо-физиологические основы и принципы интенсивной терапии
Кома. Анатомо-физиологические основы и принципы интенсивной терапии Этапы лечения хирургического больного. Предоперационный период. Хирургическая операция и её влияние на организм больного
Этапы лечения хирургического больного. Предоперационный период. Хирургическая операция и её влияние на организм больного Жедел жағдай патогенезі, пайда болу механизмі
Жедел жағдай патогенезі, пайда болу механизмі The cause of tooth abscess
The cause of tooth abscess Методы обследования ребёнка в практике врача детского стоматолога
Методы обследования ребёнка в практике врача детского стоматолога Обследование звукопроизношения
Обследование звукопроизношения Гормоны в дерматологии
Гормоны в дерматологии В-12 дефицитная анемия
В-12 дефицитная анемия Онихомикоздар. Жіктелуі
Онихомикоздар. Жіктелуі Здоровый сон – основа счастливого дня!
Здоровый сон – основа счастливого дня! Рациональное питание и Nutrilite TM: на пути к оптимальному здоровью
Рациональное питание и Nutrilite TM: на пути к оптимальному здоровью Анализ проведения противоэпидемических и профилактических мер в учреждениях здравоохранения по итогам 2016-2017 годов
Анализ проведения противоэпидемических и профилактических мер в учреждениях здравоохранения по итогам 2016-2017 годов Клиническая физиология
Клиническая физиология Лёгочный кровоток
Лёгочный кровоток Современный биомедицинский клинико-антропологический подход
Современный биомедицинский клинико-антропологический подход Вопросы онконастороженности. Онкопатруль
Вопросы онконастороженности. Онкопатруль Геронтология
Геронтология