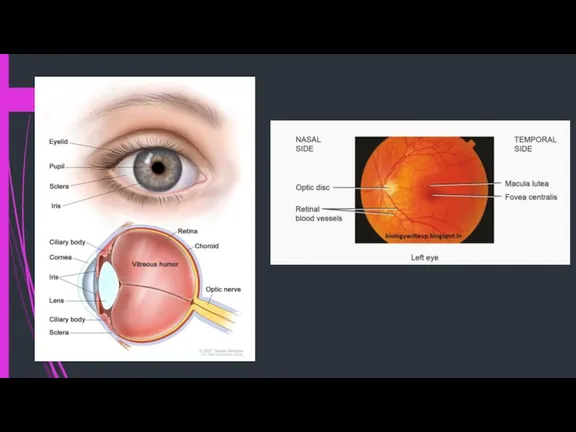
- Ophthalmology

Содержание
- 3. Orbital cellulitis a systemically unwell patient proptosis peri-ocular swelling and erythema tenderness over the sinuses ocular
- 4. Conjunctivitis “Pink eye” Risk factors: exposure to someone infected, rubbing eyes, contact lenses. Symptoms: Marked, diffuse
- 5. Scleritis and episcleritis Episcleritis: itching a red and sore eye no discharge no watering vision normal
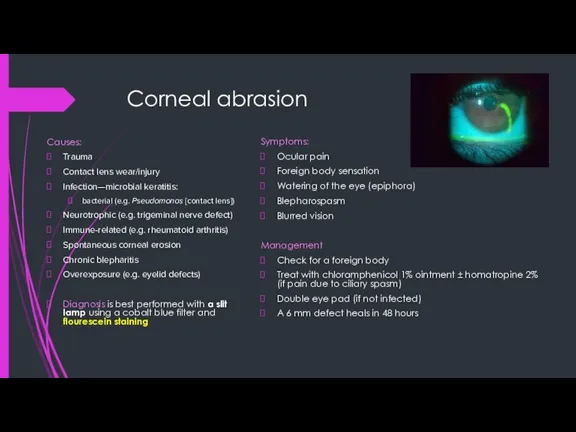
- 6. Corneal abrasion Causes: Trauma Contact lens wear/injury Infection—microbial keratitis: bacterial (e.g. Pseudomonas [contact lens]) Neurotrophic (e.g.
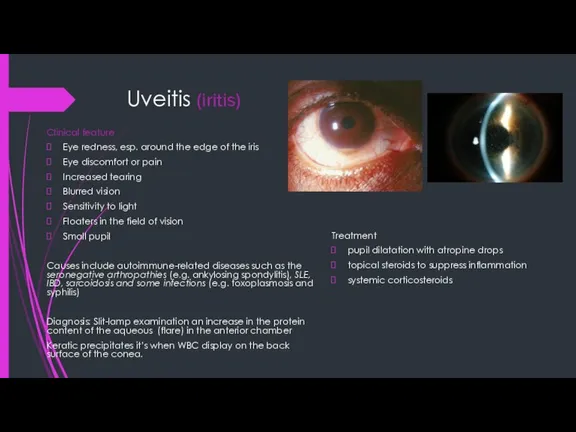
- 7. Uveitis (iritis) Clinical feature Eye redness, esp. around the edge of the iris Eye discomfort or
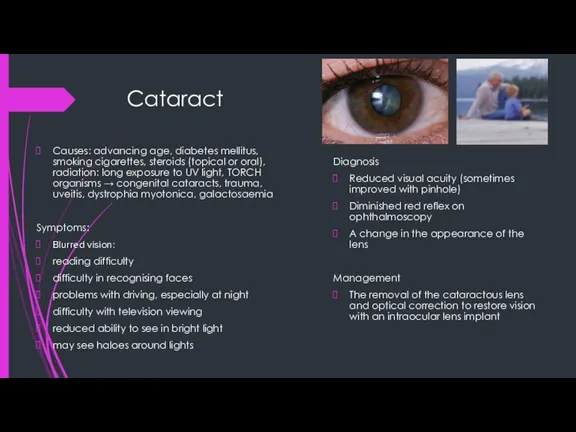
- 8. Cataract Causes: advancing age, diabetes mellitus, smoking cigarettes, steroids (topical or oral), radiation: long exposure to
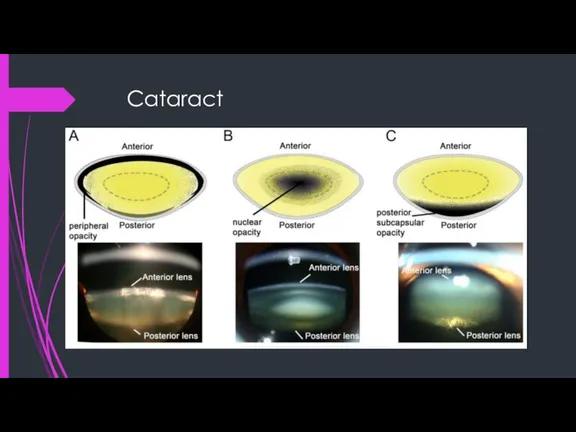
- 9. Cataract
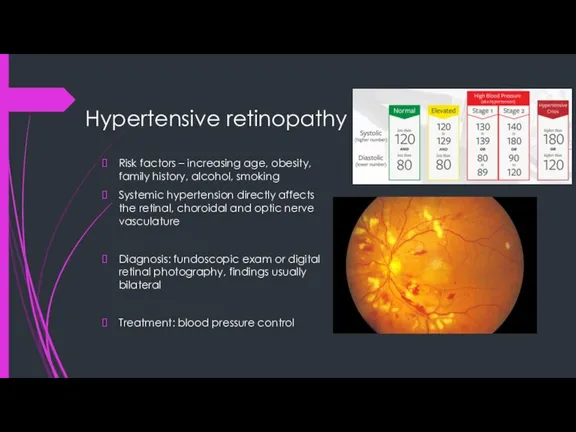
- 10. Hypertensive retinopathy Risk factors – increasing age, obesity, family history, alcohol, smoking Systemic hypertension directly affects
- 11. Retinal vessel occlusion Central retinal artery occlusion Sudden loss of vision like a ‘curtain descending’ in
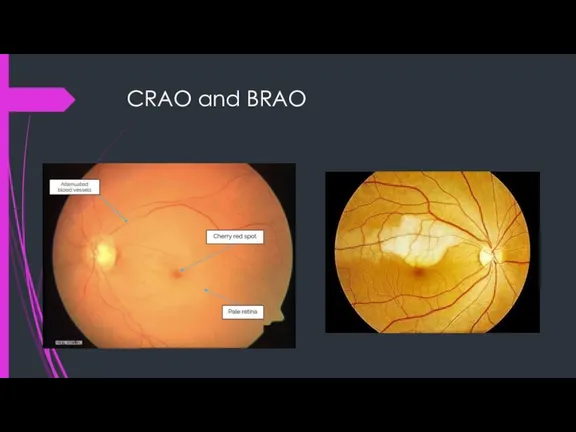
- 12. CRAO and BRAO
- 13. Retinal vessel occlusion Central retinal vein thrombosis Sudden loss of central vision in one eye (if
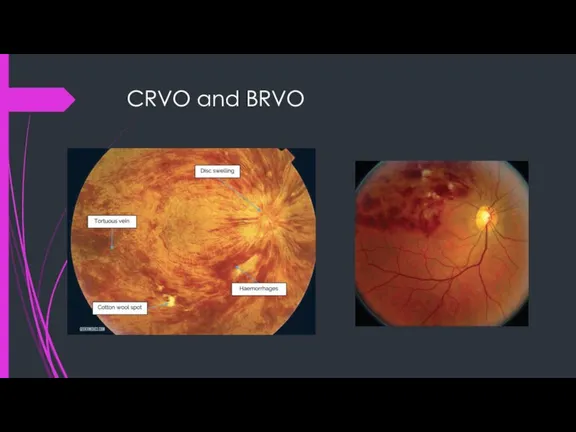
- 14. CRVO and BRVO
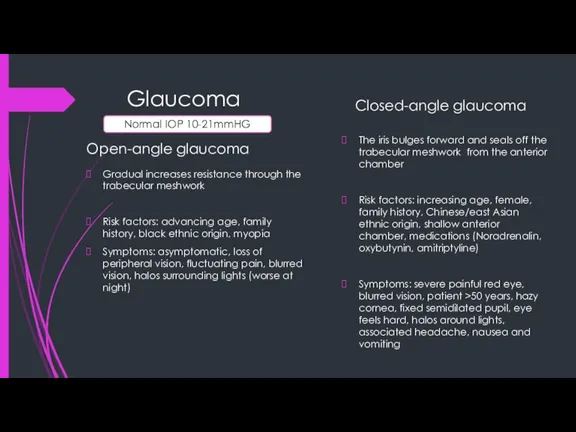
- 15. Glaucoma Open-angle glaucoma Gradual increases resistance through the trabecular meshwork Risk factors: advancing age, family history,
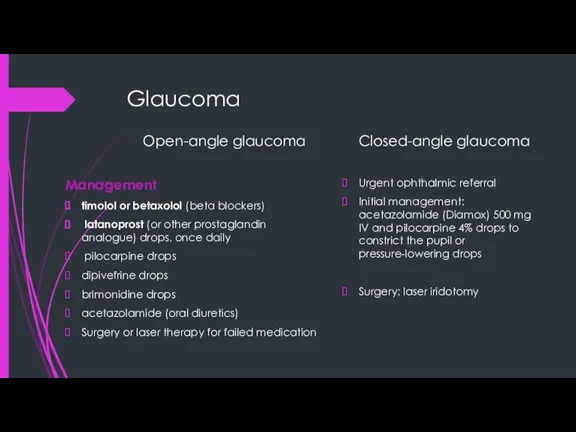
- 16. Glaucoma Open-angle glaucoma Management timolol or betaxolol (beta blockers) latanoprost (or other prostaglandin analogue) drops, once
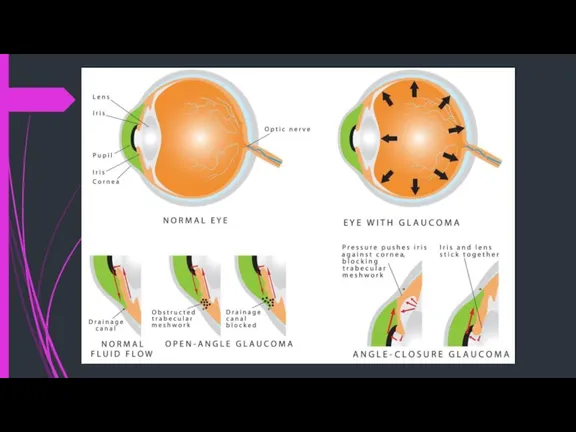
- 17. Glaucoma
- 18. Glaucoma Investigations Tonometry (Goldmann applanation tonometry) Upper limit of normal is 22 mmHg Ophthalmoscopy Optic disc
- 19. Keratitis Keratitis is inflammation of the cornea pain, impaired eyesight, photophobia (light sensitivity), red eye and
- 20. Blepharitis Clinical features Persistent sore eyes or eyelids Irritation, grittiness, burning, dryness and ‘something in the
- 21. Blepharitis Management Anterior blepharitis A systematic and long-term commitment to a program of eyelid margin hygiene
- 22. Subconjunctival hemorrhage A beefy red localised haemorrhage with a definite posterior margin, it is pain free.
- 23. Hypopyon and hyphema inflammatory cells in the anterior chamber of the eye. The most common cause
- 25. Скачать презентацию
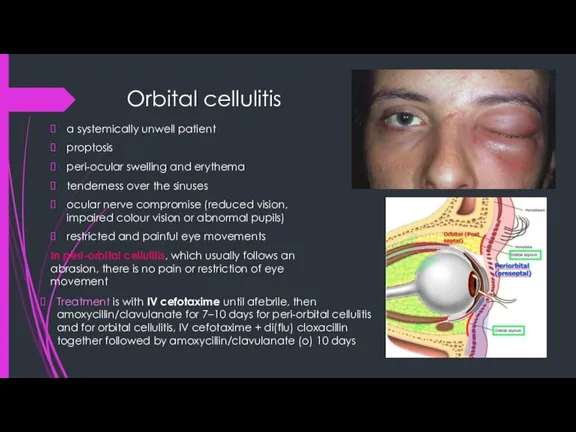
Слайд 3Orbital cellulitis
a systemically unwell patient
proptosis
peri-ocular swelling and erythema
tenderness over the sinuses
ocular nerve
Orbital cellulitis
a systemically unwell patient
proptosis
peri-ocular swelling and erythema
tenderness over the sinuses
ocular nerve
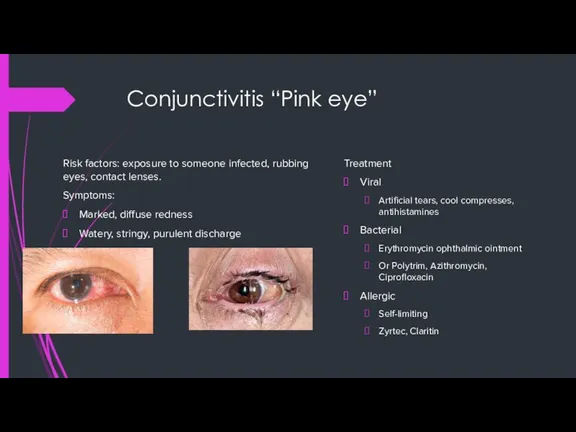
Слайд 4Conjunctivitis “Pink eye”
Risk factors: exposure to someone infected, rubbing eyes, contact lenses.
Symptoms:
Marked,
Conjunctivitis “Pink eye”
Risk factors: exposure to someone infected, rubbing eyes, contact lenses.
Symptoms:
Marked,
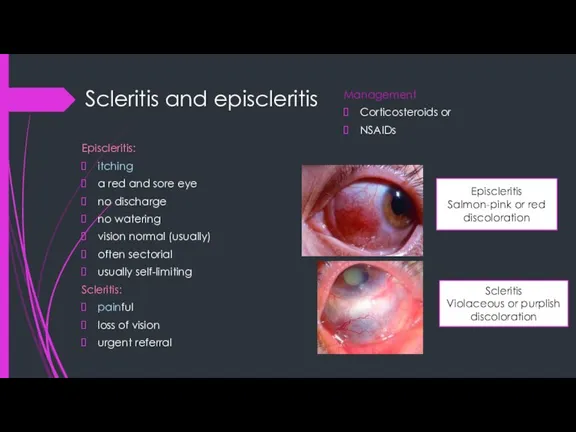
Слайд 5Scleritis and episcleritis
Episcleritis:
itching
a red and sore eye
no discharge
no watering
vision normal (usually)
often sectorial
usually
Scleritis and episcleritis
Episcleritis:
itching
a red and sore eye
no discharge
no watering
vision normal (usually)
often sectorial
usually
Слайд 6Corneal abrasion
Causes:
Trauma
Contact lens wear/injury
Infection—microbial keratitis:
bacterial (e.g. Pseudomonas [contact lens])
Neurotrophic (e.g. trigeminal nerve
Corneal abrasion
Causes:
Trauma
Contact lens wear/injury
Infection—microbial keratitis:
bacterial (e.g. Pseudomonas [contact lens])
Neurotrophic (e.g. trigeminal nerve
Слайд 7Uveitis (iritis)
Clinical feature
Eye redness, esp. around the edge of the iris
Eye discomfort
Uveitis (iritis)
Clinical feature
Eye redness, esp. around the edge of the iris
Eye discomfort
Слайд 8Cataract
Causes: advancing age, diabetes mellitus, smoking cigarettes, steroids (topical or oral), radiation:
Cataract
Causes: advancing age, diabetes mellitus, smoking cigarettes, steroids (topical or oral), radiation:
Слайд 9Cataract
Cataract
Слайд 10Hypertensive retinopathy
Risk factors – increasing age, obesity, family history, alcohol, smoking
Systemic hypertension
Hypertensive retinopathy
Risk factors – increasing age, obesity, family history, alcohol, smoking
Systemic hypertension
Слайд 11Retinal vessel occlusion
Central retinal artery occlusion
Sudden loss of vision like a ‘curtain
Retinal vessel occlusion
Central retinal artery occlusion
Sudden loss of vision like a ‘curtain
Слайд 12CRAO and BRAO
CRAO and BRAO
Слайд 13Retinal vessel occlusion
Central retinal vein thrombosis
Sudden loss of central vision in one
Retinal vessel occlusion
Central retinal vein thrombosis
Sudden loss of central vision in one
Слайд 14CRVO and BRVO
CRVO and BRVO
Слайд 15Glaucoma
Open-angle glaucoma
Gradual increases resistance through the trabecular meshwork
Risk factors: advancing age, family
Glaucoma
Open-angle glaucoma
Gradual increases resistance through the trabecular meshwork
Risk factors: advancing age, family
Слайд 16Glaucoma
Open-angle glaucoma
Management
timolol or betaxolol (beta blockers)
latanoprost (or other prostaglandin analogue) drops,
Glaucoma
Open-angle glaucoma
Management
timolol or betaxolol (beta blockers)
latanoprost (or other prostaglandin analogue) drops,
Слайд 17Glaucoma
Glaucoma
Слайд 18Glaucoma
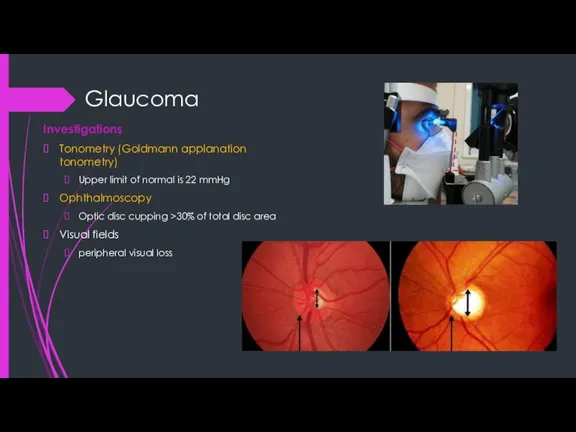
Investigations
Tonometry (Goldmann applanation tonometry)
Upper limit of normal is 22 mmHg
Ophthalmoscopy
Optic disc cupping
Glaucoma
Investigations
Tonometry (Goldmann applanation tonometry)
Upper limit of normal is 22 mmHg
Ophthalmoscopy
Optic disc cupping
Слайд 19Keratitis
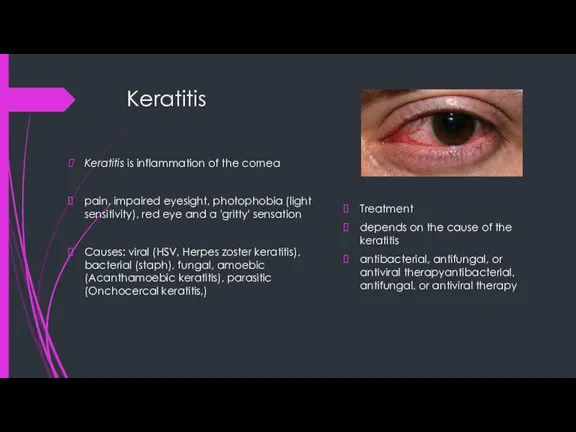
Keratitis is inflammation of the cornea
pain, impaired eyesight, photophobia (light sensitivity), red
Keratitis
Keratitis is inflammation of the cornea
pain, impaired eyesight, photophobia (light sensitivity), red
Слайд 20Blepharitis
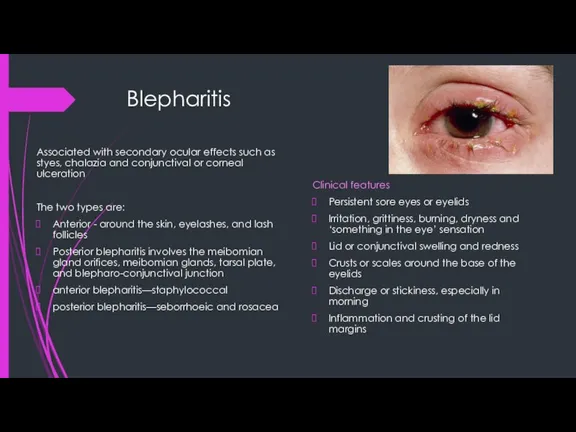
Clinical features
Persistent sore eyes or eyelids
Irritation, grittiness, burning, dryness and ‘something in
Blepharitis
Clinical features
Persistent sore eyes or eyelids
Irritation, grittiness, burning, dryness and ‘something in
Слайд 21Blepharitis
Management
Anterior blepharitis
A systematic and long-term commitment to a program of eyelid margin
Blepharitis
Management
Anterior blepharitis
A systematic and long-term commitment to a program of eyelid margin
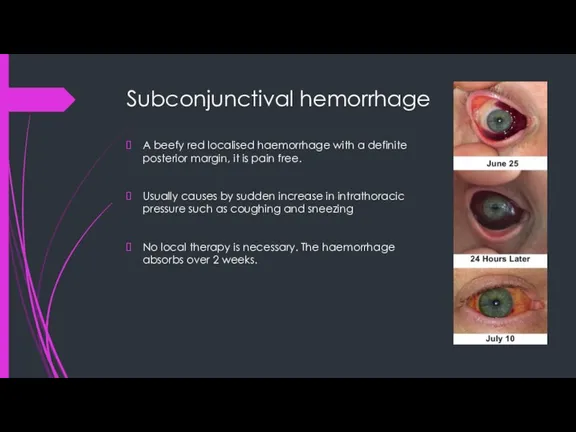
Слайд 22Subconjunctival hemorrhage
A beefy red localised haemorrhage with a definite posterior margin, it
Subconjunctival hemorrhage
A beefy red localised haemorrhage with a definite posterior margin, it
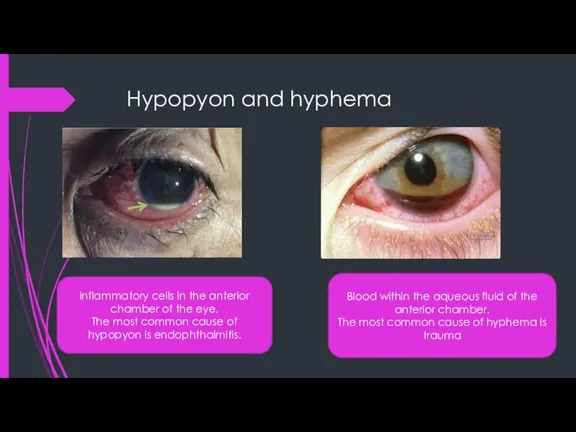
Слайд 23Hypopyon and hyphema
inflammatory cells in the anterior chamber of the eye.
The most
Hypopyon and hyphema
inflammatory cells in the anterior chamber of the eye.
The most
 Клещи. Заболевания, переносчиками которых они являются
Клещи. Заболевания, переносчиками которых они являются Патология дыхания. Нарушения тканевого обмена. Гипоксия
Патология дыхания. Нарушения тканевого обмена. Гипоксия Пам’ятка щодо запобіганню z захворювання covid 19. Порядок дій у разі захворювання!
Пам’ятка щодо запобіганню z захворювання covid 19. Порядок дій у разі захворювання! Нозокомиальные инфекции
Нозокомиальные инфекции Беременность и миома матки. Беременность и рак шейки матки
Беременность и миома матки. Беременность и рак шейки матки Синдром обструктивного апноэ сна (СОАС)
Синдром обструктивного апноэ сна (СОАС) Корсаковский синдром
Корсаковский синдром Клиническая биохимия при нарушениях обмена липидов
Клиническая биохимия при нарушениях обмена липидов Микробиом и расстройства пищевого поведения
Микробиом и расстройства пищевого поведения Опыт применения Time-lapse микроскопии в программах экстракорпорального оплодотворения
Опыт применения Time-lapse микроскопии в программах экстракорпорального оплодотворения Железы внутренней секреции
Железы внутренней секреции ОРВИ (острые респираторные вирусные инфекции)
ОРВИ (острые респираторные вирусные инфекции) СПИД и ВИЧ
СПИД и ВИЧ Гигиена сердечно-сосудистой системы
Гигиена сердечно-сосудистой системы Миома (маточный фиброид). Этиология, патогенез, клиника, диагностика, лечение
Миома (маточный фиброид). Этиология, патогенез, клиника, диагностика, лечение Желтуха. Типы желтухи
Желтуха. Типы желтухи Вкр (роль и значение helicobacter pylori в лабораторной диагностике)
Вкр (роль и значение helicobacter pylori в лабораторной диагностике) Муколитическая терапия в педиатрической практике
Муколитическая терапия в педиатрической практике Иммунологиялық реакциялар:маңызы,түрлері,механизмері. Инфекциялық аурулардың иммунопрофилактикасы және иммунотерапия негіздері
Иммунологиялық реакциялар:маңызы,түрлері,механизмері. Инфекциялық аурулардың иммунопрофилактикасы және иммунотерапия негіздері Миома матки
Миома матки Эра антибиотиков
Эра антибиотиков Показання до госпіталізації в нейрохірургічне відділення КЗ Сумська обласна клінічна лікарня
Показання до госпіталізації в нейрохірургічне відділення КЗ Сумська обласна клінічна лікарня Аускультация легких
Аускультация легких Инфаркт миокарда. Медицинские аспекты. Модуль 2
Инфаркт миокарда. Медицинские аспекты. Модуль 2 Геморрой
Геморрой 7-Нарушения водно-солевого обмена
7-Нарушения водно-солевого обмена Антиинтерлейкиновые препараты в лечении бронхиальной астмы
Антиинтерлейкиновые препараты в лечении бронхиальной астмы Новокаиновые блокады
Новокаиновые блокады