- Абдоминальная травма

Содержание
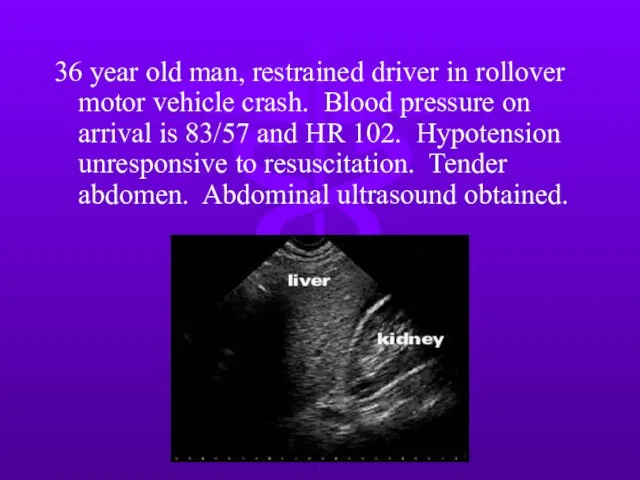
- 2. 36 year old man, restrained driver in rollover motor vehicle crash. Blood pressure on arrival is
- 3. Next step? Exploratory laparotomy Diagnostic peritoneal lavage Abdominal CT scan Serial observation
- 4. 28 y/o woman, unrestrained driver in a motor vehicle crash. Stable vital signs and LUQ tenderness,
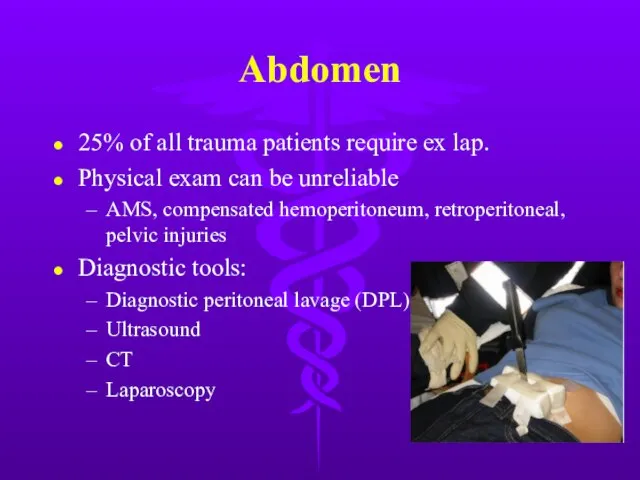
- 5. Abdomen 25% of all trauma patients require ex lap. Physical exam can be unreliable AMS, compensated
- 6. Diagnosis Test of choice dependent on hemodynamic stability and severity of associated injuries. Stable blunt trauma
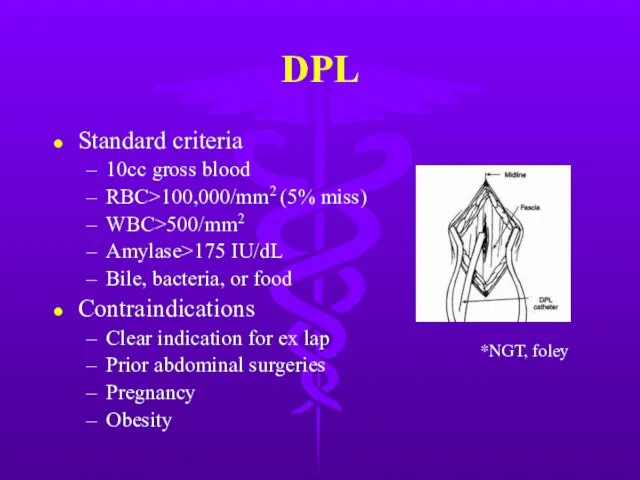
- 7. DPL Standard criteria 10cc gross blood RBC>100,000/mm2 (5% miss) WBC>500/mm2 Amylase>175 IU/dL Bile, bacteria, or food
- 8. DPL Highly sensitive to intraperitoneal blood, but low specificity → nontherapeutic explorations. Supraumbilical if pelvic fracture
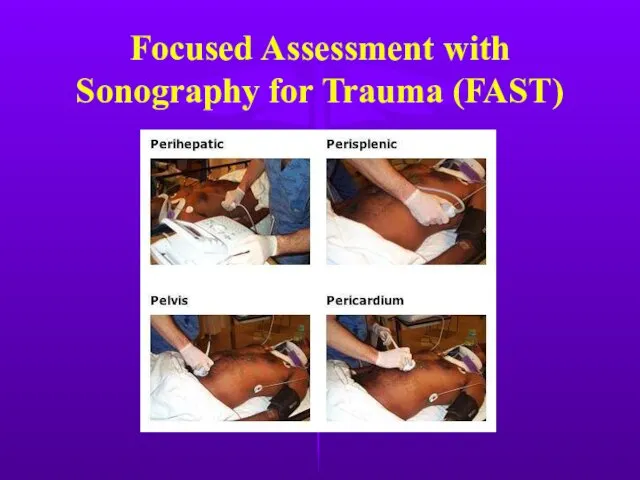
- 9. Focused Assessment with Sonography for Trauma (FAST)
- 10. FAST Pros Noninvasive Fast Low cost Cons User dependent Obesity, gas interposition Misses retroperitoneal/hollow viscus injury
- 11. CT Scan Hemodynamically stable patient Pros Retroperitoneal assessment Nonoperative management of solid organ injury High specificity
- 12. Laparoscopy Role still being defined Good for diaphragm injury evaluation Cons Invasive Expensive Missed small bowel,
- 13. Gastric Injury Mostly penetrating trauma. Including iatrogenic injury from CPR NGT + aspirate for blood Intraop
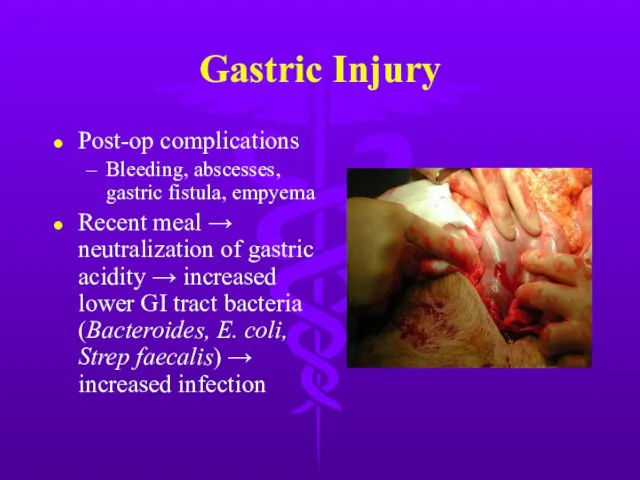
- 14. Gastric Injury Post-op complications Bleeding, abscesses, gastric fistula, empyema Recent meal → neutralization of gastric acidity
- 15. Duodenal Injury Majority due to penetrating trauma. Blunt injury usually secondary to steering wheel blow to
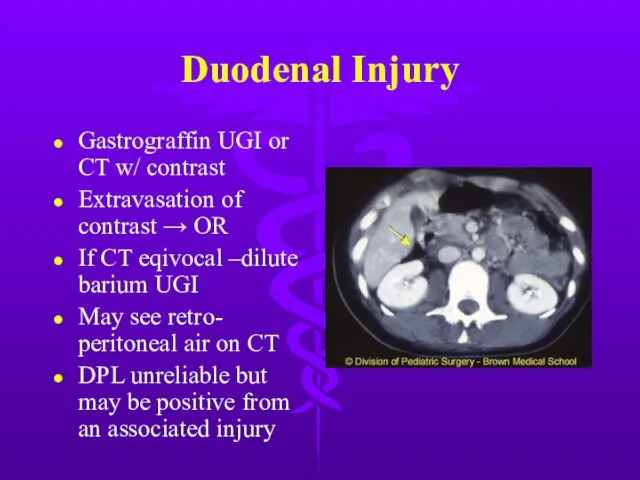
- 16. Duodenal Injury Gastrograffin UGI or CT w/ contrast Extravasation of contrast → OR If CT eqivocal
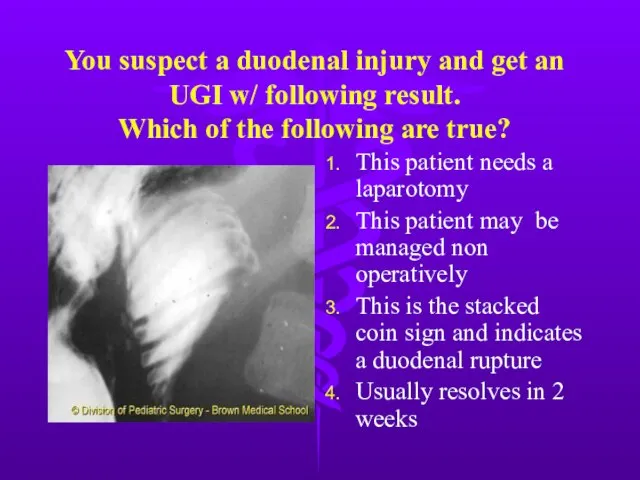
- 17. You suspect a duodenal injury and get an UGI w/ following result. Which of the following
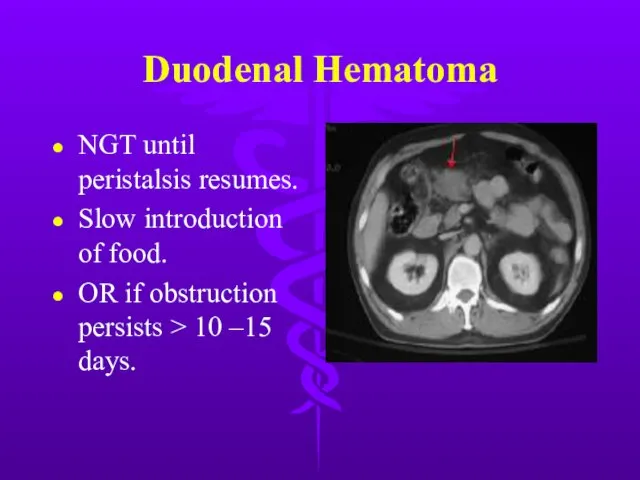
- 18. Duodenal Hematoma NGT until peristalsis resumes. Slow introduction of food. OR if obstruction persists > 10
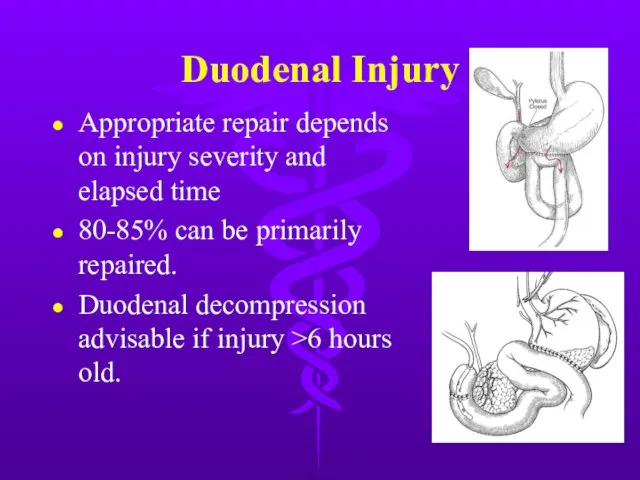
- 19. Duodenal Injury Appropriate repair depends on injury severity and elapsed time 80-85% can be primarily repaired.
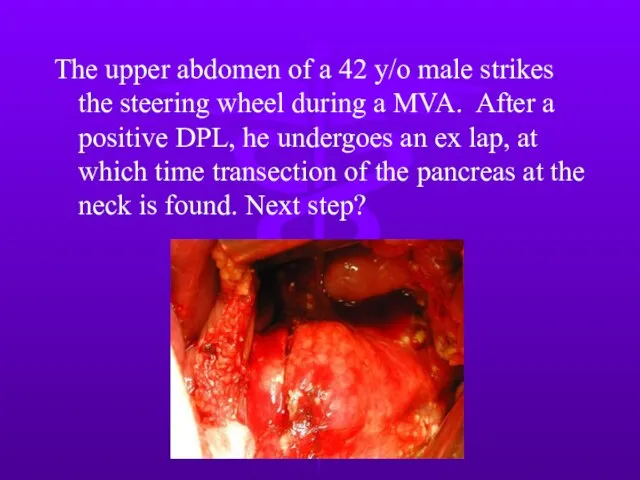
- 20. The upper abdomen of a 42 y/o male strikes the steering wheel during a MVA. After
- 21. Next step? Distal pancreatectomy with oversewing and drainage of proximal stump. Primary repair and drainage of
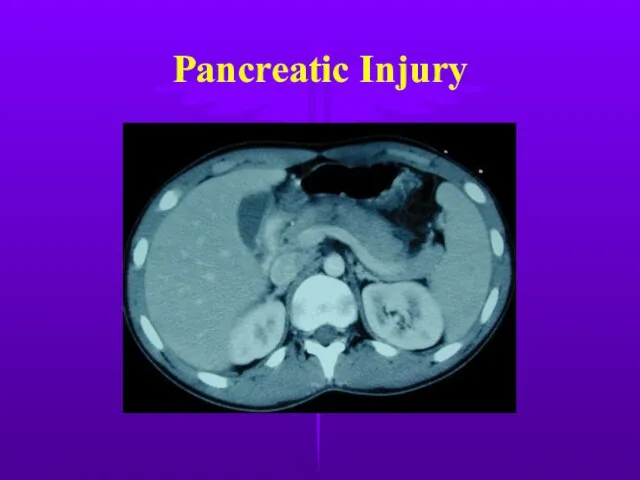
- 23. Pancreatic Injury Rare 10-12% of abdominal injuries, but mortality 10-25%, mostly from associated intra-abd injury Most
- 24. Pancreatic Injury
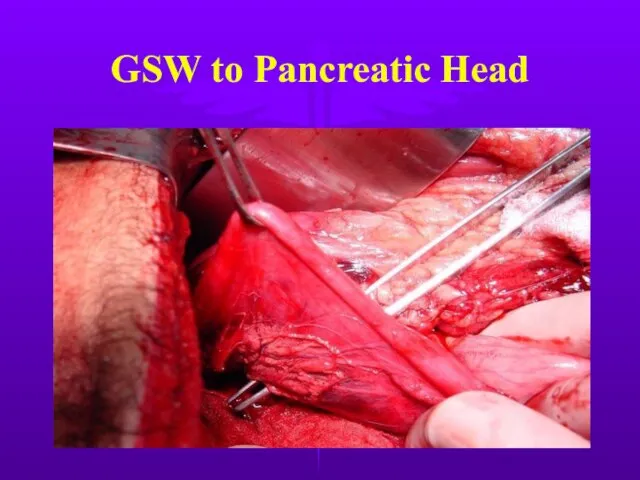
- 25. GSW to Pancreatic Head
- 26. Pancreatic Injury Divided into proximal or distal according to location on the R or L of
- 27. Complications after Pancreatic Trauma High complication rate 35-40% Most common are pancreatic fistulas & abscesses Most
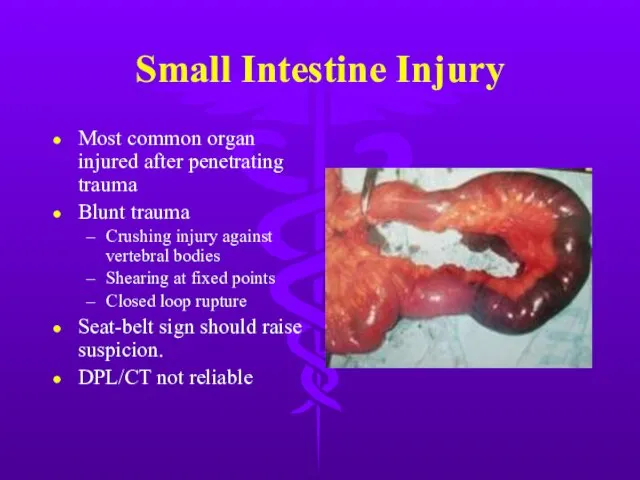
- 28. Small Intestine Injury Most common organ injured after penetrating trauma Blunt trauma Crushing injury against vertebral
- 29. Small Intestine Injury
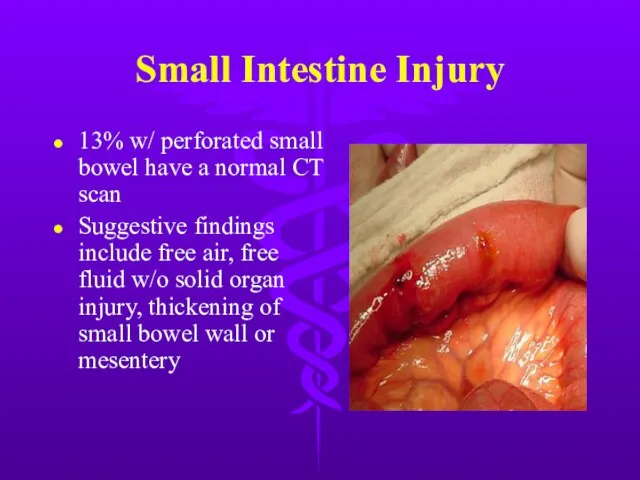
- 30. Small Intestine Injury 13% w/ perforated small bowel have a normal CT scan Suggestive findings include
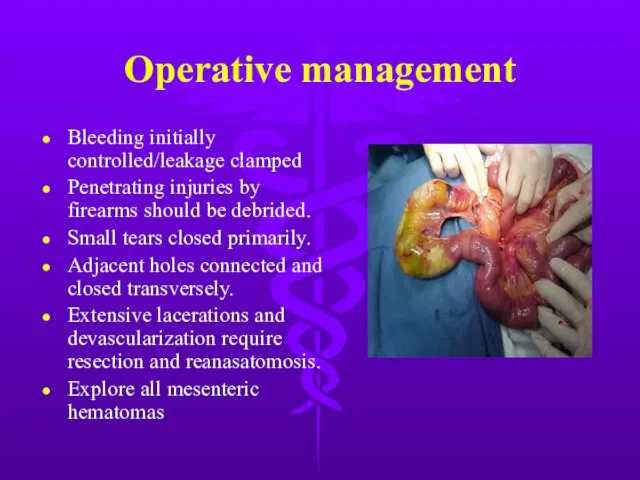
- 31. Operative management Bleeding initially controlled/leakage clamped Penetrating injuries by firearms should be debrided. Small tears closed
- 32. Colon Injury Second most frequent injured organ, usually from penetrating trauma Repair within 2 hours dramatically
- 33. Colon Injury Primary repair criteria Early diagnosis (within 4-6 hours) Absence of prolonged shock/hypotension Absence of
- 34. Rectal Injury Most from GSW Other causes - foreign body, impalement, pelvic fractures, and iatrogenic Lower
- 35. Rectal Injury Extraperitoneal injury Primary closure Diverting colostomy Washout of rectal stump Wide presacral drainage Intraperitoneal
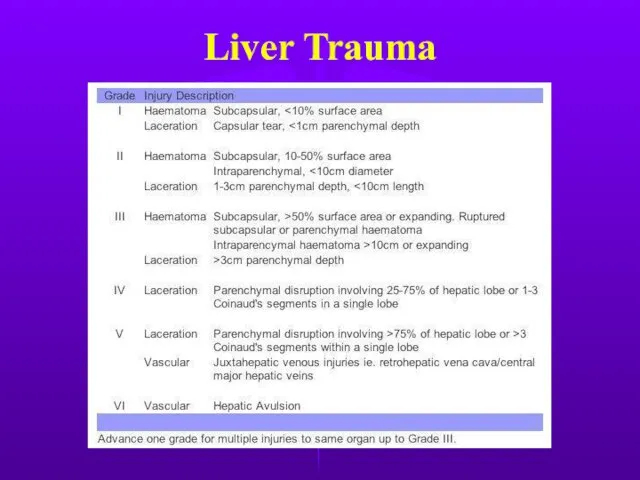
- 36. Liver Trauma Frequently injured in both blunt & penetrating trauma. Control of profuse bleeding from deep
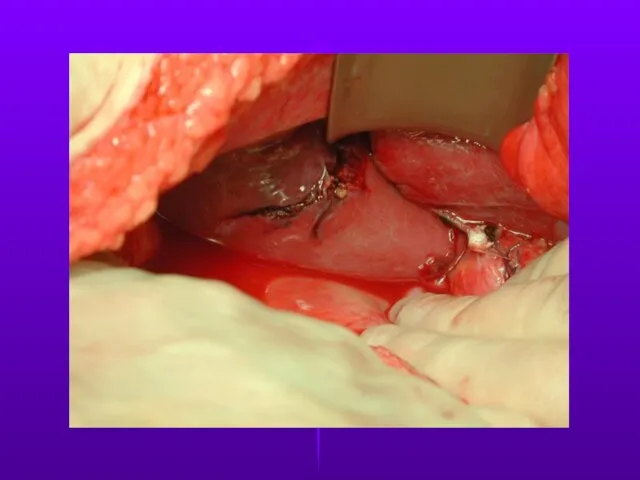
- 37. Liver Trauma
- 38. Liver Trauma
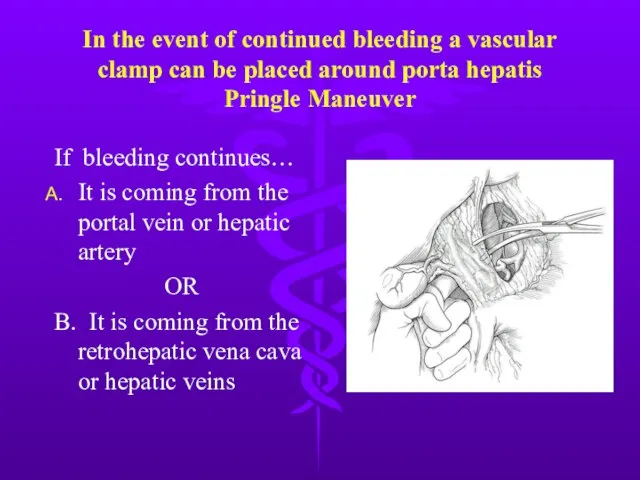
- 39. In the event of continued bleeding a vascular clamp can be placed around porta hepatis Pringle
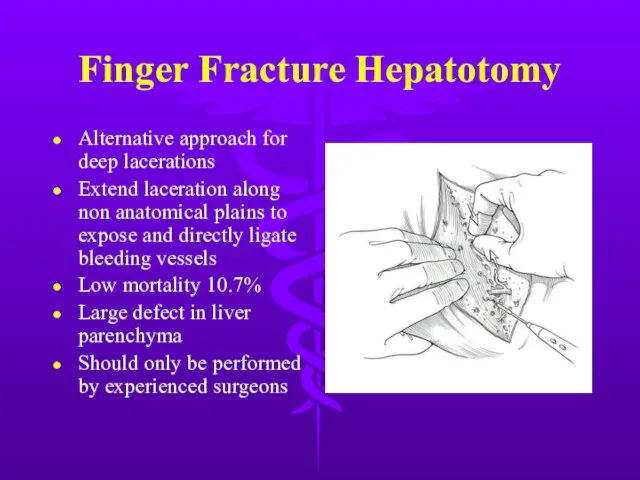
- 40. Finger Fracture Hepatotomy Alternative approach for deep lacerations Extend laceration along non anatomical plains to expose
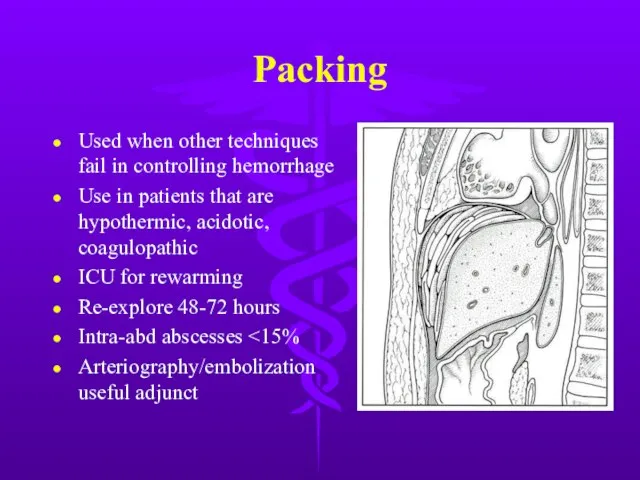
- 41. Packing Used when other techniques fail in controlling hemorrhage Use in patients that are hypothermic, acidotic,
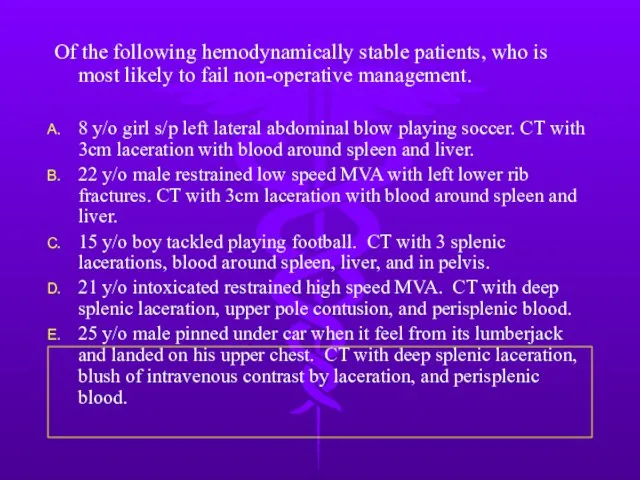
- 42. Of the following hemodynamically stable patients, who is most likely to fail non-operative management. 8 y/o
- 43. Splenic Injury Most frequently injured intra-abdominal organ in blunt trauma. Splenic preservation when possible OPSI (0.6%
- 44. Splenic Injury Nonoperative criteria Hemodynamic stability Negative abdominal examination Absence of contrast extravasation Angiography/embolization an option
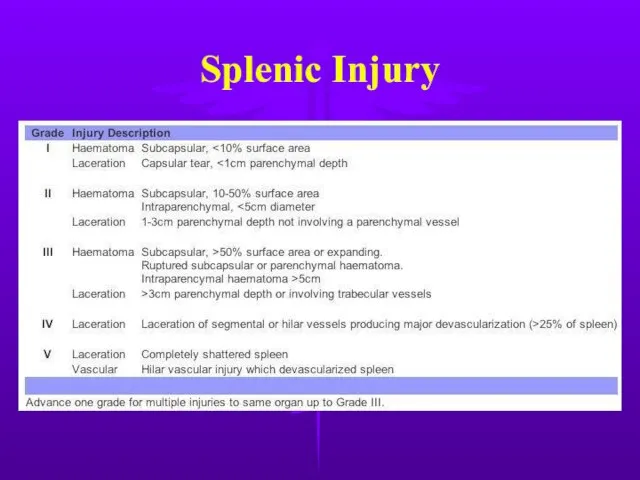
- 45. Splenic Injury
- 46. Splenic Injury
- 47. Splenic Injury
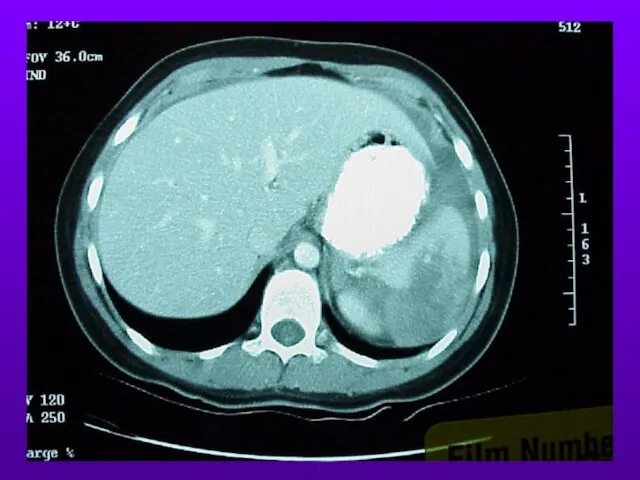
- 48. 30 year-old man ejected from automobile after head-on collision at high speed. Sustained pelvic fracture. Grossly
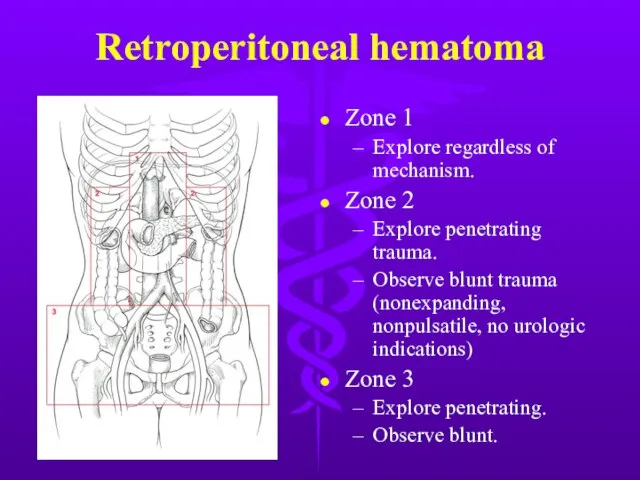
- 49. Retroperitoneal hematoma Zone 1 Explore regardless of mechanism. Zone 2 Explore penetrating trauma. Observe blunt trauma
- 50. Damage Control Abbreviated laparotomy and temporary packing Effort to blunt physiologic response to shock and hemorrhage
- 51. Damage Control
- 52. 30 y/o woman sustained crushing injury to right lower leg. Arrived at hospital 12 hours later.
- 53. Compartment Syndrome Common in forearm and lower leg secondary to defined fascial boundaries. Four Ps: pressure,
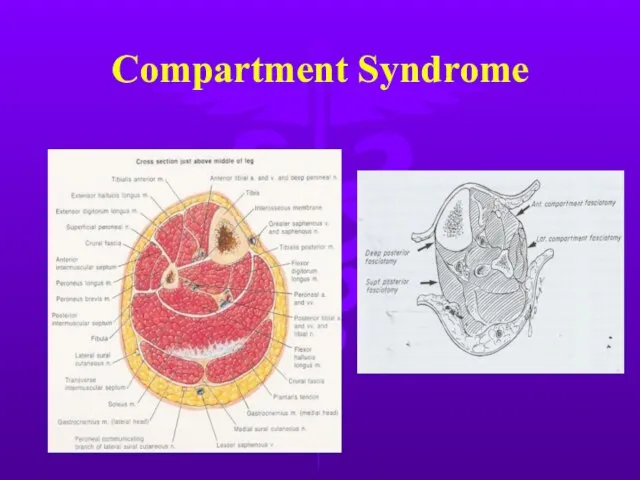
- 54. Compartment Syndrome
- 55. Fasciotomy
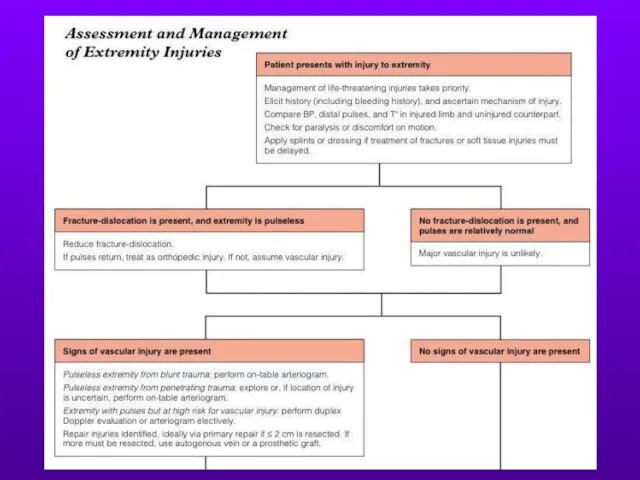
- 56. Extremity Injuries
- 57. With regard to cervical spine injury, which of the following is/are true? Jefferson fractures (C1) are
- 58. Spine Trauma C1 burst fractures (Jefferson’s) Axial loading force Considered stable Treat with rigid cervical collar
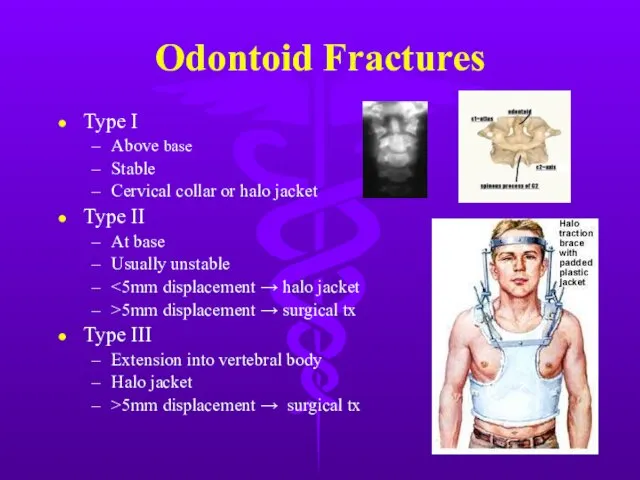
- 59. Odontoid Fractures Type I Above base Stable Cervical collar or halo jacket Type II At base
- 60. Spine Trauma Strict immobilization during ABCDEs Neurogenic shock High spine injuries Loss of sympathetic tone Hypotension,
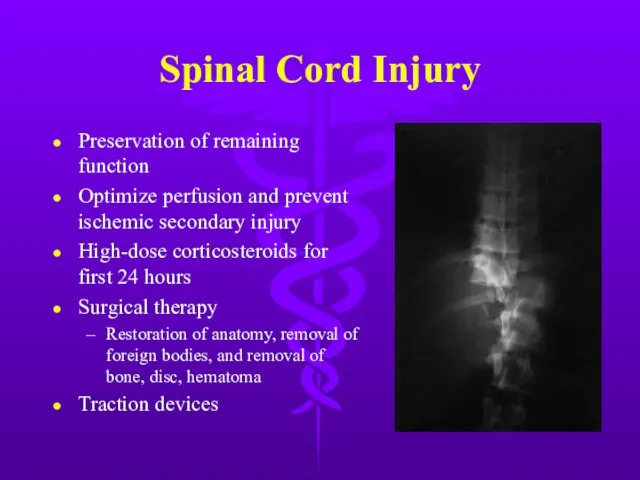
- 61. Spinal Cord Injury Preservation of remaining function Optimize perfusion and prevent ischemic secondary injury High-dose corticosteroids
- 63. Скачать презентацию
Слайд 3Next step?
Exploratory laparotomy
Diagnostic peritoneal lavage
Abdominal CT scan
Serial observation
Next step?
Exploratory laparotomy
Diagnostic peritoneal lavage
Abdominal CT scan
Serial observation
Слайд 428 y/o woman, unrestrained driver in a motor vehicle crash. Stable vital
28 y/o woman, unrestrained driver in a motor vehicle crash. Stable vital
Слайд 5Abdomen
25% of all trauma patients require ex lap.
Physical exam can be unreliable
Abdomen
25% of all trauma patients require ex lap.
Physical exam can be unreliable
Слайд 6Diagnosis
Test of choice dependent on hemodynamic stability and severity of associated injuries.
Stable
Diagnosis
Test of choice dependent on hemodynamic stability and severity of associated injuries.
Stable
Слайд 7DPL
Standard criteria
10cc gross blood
RBC>100,000/mm2 (5% miss)
WBC>500/mm2
Amylase>175 IU/dL
Bile, bacteria, or food
Contraindications
Clear indication for
DPL
Standard criteria
10cc gross blood
RBC>100,000/mm2 (5% miss)
WBC>500/mm2
Amylase>175 IU/dL
Bile, bacteria, or food
Contraindications
Clear indication for
Слайд 8DPL
Highly sensitive to intraperitoneal blood, but low specificity → nontherapeutic explorations.
Supraumbilical if
DPL
Highly sensitive to intraperitoneal blood, but low specificity → nontherapeutic explorations.
Supraumbilical if
Слайд 9Focused Assessment with Sonography for Trauma (FAST)
Focused Assessment with Sonography for Trauma (FAST)
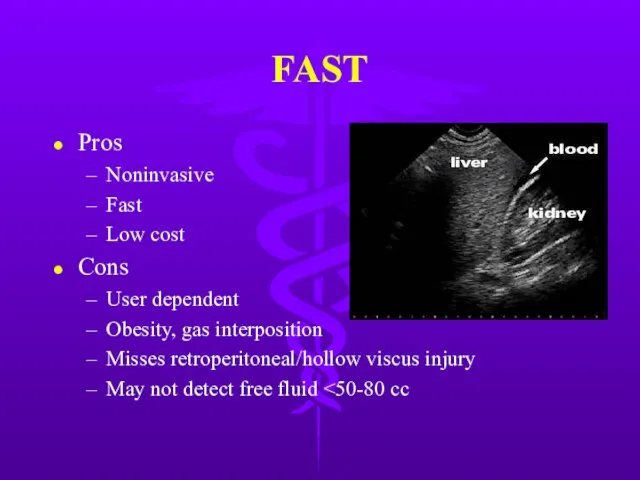
Слайд 10FAST
Pros
Noninvasive
Fast
Low cost
Cons
User dependent
Obesity, gas interposition
Misses retroperitoneal/hollow viscus injury
May not detect free fluid
FAST
Pros
Noninvasive
Fast
Low cost
Cons
User dependent
Obesity, gas interposition
Misses retroperitoneal/hollow viscus injury
May not detect free fluid
Слайд 11CT Scan
Hemodynamically stable patient
Pros
Retroperitoneal assessment
Nonoperative management of solid organ injury
High specificity
Cons
Hardware, cost,
CT Scan
Hemodynamically stable patient
Pros
Retroperitoneal assessment
Nonoperative management of solid organ injury
High specificity
Cons
Hardware, cost,
Слайд 12Laparoscopy
Role still being defined
Good for diaphragm injury evaluation
Cons
Invasive
Expensive
Missed small bowel, splenic, retroperitoneal
Laparoscopy
Role still being defined
Good for diaphragm injury evaluation
Cons
Invasive
Expensive
Missed small bowel, splenic, retroperitoneal
Слайд 13Gastric Injury
Mostly penetrating trauma.
<1% from blunt trauma
Including iatrogenic injury from CPR
NGT
Gastric Injury
Mostly penetrating trauma.
<1% from blunt trauma
Including iatrogenic injury from CPR
NGT
Слайд 14Gastric Injury
Post-op complications
Bleeding, abscesses, gastric fistula, empyema
Recent meal → neutralization of gastric
Gastric Injury
Post-op complications
Bleeding, abscesses, gastric fistula, empyema
Recent meal → neutralization of gastric
Слайд 15Duodenal Injury
Majority due to penetrating trauma.
Blunt injury usually secondary to steering wheel
Duodenal Injury
Majority due to penetrating trauma.
Blunt injury usually secondary to steering wheel
Слайд 16Duodenal Injury
Gastrograffin UGI or CT w/ contrast
Extravasation of contrast → OR
If CT
Duodenal Injury
Gastrograffin UGI or CT w/ contrast
Extravasation of contrast → OR
If CT
Слайд 17You suspect a duodenal injury and get an UGI w/ following result.
You suspect a duodenal injury and get an UGI w/ following result.
Слайд 18Duodenal Hematoma
NGT until peristalsis resumes.
Slow introduction of food.
OR if obstruction persists >
Duodenal Hematoma
NGT until peristalsis resumes.
Slow introduction of food.
OR if obstruction persists >
Слайд 19Duodenal Injury
Appropriate repair depends on injury severity and elapsed time
80-85% can be
Duodenal Injury
Appropriate repair depends on injury severity and elapsed time
80-85% can be
Слайд 20The upper abdomen of a 42 y/o male strikes the steering wheel
The upper abdomen of a 42 y/o male strikes the steering wheel
Слайд 21Next step?
Distal pancreatectomy with oversewing and drainage of proximal stump.
Primary repair and
Next step?
Distal pancreatectomy with oversewing and drainage of proximal stump.
Primary repair and

Слайд 23Pancreatic Injury
Rare 10-12% of abdominal injuries, but mortality 10-25%, mostly from associated
Pancreatic Injury
Rare 10-12% of abdominal injuries, but mortality 10-25%, mostly from associated
Слайд 24Pancreatic Injury
Pancreatic Injury
Слайд 25GSW to Pancreatic Head
GSW to Pancreatic Head
Слайд 26Pancreatic Injury
Divided into proximal or distal according to location on the R
Pancreatic Injury
Divided into proximal or distal according to location on the R
Слайд 27Complications after Pancreatic Trauma
High complication rate 35-40%
Most common are pancreatic fistulas &
Complications after Pancreatic Trauma
High complication rate 35-40%
Most common are pancreatic fistulas &
Слайд 28Small Intestine Injury
Most common organ injured after penetrating trauma
Blunt trauma
Crushing injury against
Small Intestine Injury
Most common organ injured after penetrating trauma
Blunt trauma
Crushing injury against
Слайд 29Small Intestine Injury
Small Intestine Injury

Слайд 30Small Intestine Injury
13% w/ perforated small bowel have a normal CT scan
Suggestive
Small Intestine Injury
13% w/ perforated small bowel have a normal CT scan
Suggestive
Слайд 31Operative management
Bleeding initially controlled/leakage clamped
Penetrating injuries by firearms should be debrided.
Small tears
Operative management
Bleeding initially controlled/leakage clamped
Penetrating injuries by firearms should be debrided.
Small tears
Слайд 32Colon Injury
Second most frequent injured organ, usually from penetrating trauma
Repair within 2
Colon Injury
Second most frequent injured organ, usually from penetrating trauma
Repair within 2
Слайд 33Colon Injury
Primary repair criteria
Early diagnosis (within 4-6 hours)
Absence of prolonged shock/hypotension
Absence of
Colon Injury
Primary repair criteria
Early diagnosis (within 4-6 hours)
Absence of prolonged shock/hypotension
Absence of
Слайд 34Rectal Injury
Most from GSW
Other causes - foreign body, impalement, pelvic fractures, and
Rectal Injury
Most from GSW
Other causes - foreign body, impalement, pelvic fractures, and
Слайд 35Rectal Injury
Extraperitoneal injury
Primary closure
Diverting colostomy
Washout of rectal stump
Wide presacral drainage
Intraperitoneal injury
Primary closure
Diverting
Rectal Injury
Extraperitoneal injury
Primary closure
Diverting colostomy
Washout of rectal stump
Wide presacral drainage
Intraperitoneal injury
Primary closure
Diverting

Слайд 36Liver Trauma
Frequently injured in both blunt & penetrating trauma.
Control of profuse bleeding
Liver Trauma
Frequently injured in both blunt & penetrating trauma.
Control of profuse bleeding
Слайд 37Liver Trauma
Liver Trauma
Слайд 38Liver Trauma
Liver Trauma
Слайд 39In the event of continued bleeding a vascular clamp can be placed
In the event of continued bleeding a vascular clamp can be placed
Слайд 40Finger Fracture Hepatotomy
Alternative approach for deep lacerations
Extend laceration along non anatomical plains
Finger Fracture Hepatotomy
Alternative approach for deep lacerations
Extend laceration along non anatomical plains
Слайд 41Packing
Used when other techniques fail in controlling hemorrhage
Use in patients that are
Packing
Used when other techniques fail in controlling hemorrhage
Use in patients that are
Слайд 42Of the following hemodynamically stable patients, who is most likely to fail
Of the following hemodynamically stable patients, who is most likely to fail
Слайд 43Splenic Injury
Most frequently injured intra-abdominal organ in blunt trauma.
Splenic preservation when possible
OPSI
Splenic Injury
Most frequently injured intra-abdominal organ in blunt trauma.
Splenic preservation when possible
OPSI
Слайд 44Splenic Injury
Nonoperative criteria
Hemodynamic stability
Negative abdominal examination
Absence of contrast extravasation
Angiography/embolization an option
No other
Splenic Injury
Nonoperative criteria
Hemodynamic stability
Negative abdominal examination
Absence of contrast extravasation
Angiography/embolization an option
No other

Слайд 45Splenic Injury
Splenic Injury
Слайд 46Splenic Injury
Splenic Injury
Слайд 47Splenic Injury
Splenic Injury

Слайд 4830 year-old man ejected from automobile after head-on collision at high speed.
30 year-old man ejected from automobile after head-on collision at high speed.
Слайд 49Retroperitoneal hematoma
Zone 1
Explore regardless of mechanism.
Zone 2
Explore penetrating trauma.
Observe blunt trauma (nonexpanding,
Retroperitoneal hematoma
Zone 1
Explore regardless of mechanism.
Zone 2
Explore penetrating trauma.
Observe blunt trauma (nonexpanding,
Слайд 50Damage Control
Abbreviated laparotomy and temporary packing
Effort to blunt physiologic response to shock
Damage Control
Abbreviated laparotomy and temporary packing
Effort to blunt physiologic response to shock
Слайд 51Damage Control
Damage Control

Слайд 5230 y/o woman sustained crushing injury to right lower leg. Arrived at
30 y/o woman sustained crushing injury to right lower leg. Arrived at
Слайд 53Compartment Syndrome
Common in forearm and lower leg secondary to defined fascial boundaries.
Four
Compartment Syndrome
Common in forearm and lower leg secondary to defined fascial boundaries.
Four
Слайд 54Compartment Syndrome
Compartment Syndrome
Слайд 55Fasciotomy
Fasciotomy

Слайд 56Extremity Injuries
Extremity Injuries
Слайд 57With regard to cervical spine injury, which of the following is/are true?
Jefferson
With regard to cervical spine injury, which of the following is/are true?
Jefferson
Слайд 58Spine Trauma
C1 burst fractures (Jefferson’s)
Axial loading force
Considered stable
Treat with rigid cervical collar
Hangman’s
Spine Trauma
C1 burst fractures (Jefferson’s)
Axial loading force
Considered stable
Treat with rigid cervical collar
Hangman’s
Слайд 59Odontoid Fractures
Type I
Above base
Stable
Cervical collar or halo jacket
Type II
At base
Usually unstable
<5mm
Odontoid Fractures
Type I
Above base
Stable
Cervical collar or halo jacket
Type II
At base
Usually unstable
<5mm
Слайд 60Spine Trauma
Strict immobilization during ABCDEs
Neurogenic shock
High spine injuries
Loss of sympathetic tone
Hypotension, bradycardia,
Spine Trauma
Strict immobilization during ABCDEs
Neurogenic shock
High spine injuries
Loss of sympathetic tone
Hypotension, bradycardia,
Слайд 61Spinal Cord Injury
Preservation of remaining function
Optimize perfusion and prevent ischemic secondary injury
High-dose
Spinal Cord Injury
Preservation of remaining function
Optimize perfusion and prevent ischemic secondary injury
High-dose
 Презентация на тему: Политическая система 10 класс
Презентация на тему: Политическая система 10 класс Форма государства и ее элементы
Форма государства и ее элементы Токарь
Токарь Pacnetbi ha npohhoctt mexahhneckhx kohcrpy^hh cogep^ahhe
Pacnetbi ha npohhoctt mexahhneckhx kohcrpy^hh cogep^ahhe Процессуальные риски
Процессуальные риски Палеозойская эра
Палеозойская эра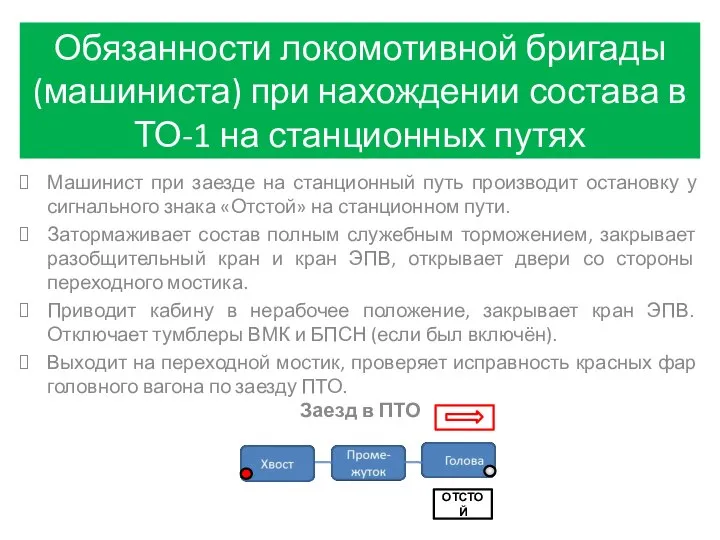 Обязанности машиниста при нахождении состава в ТО-1 на станционных путях
Обязанности машиниста при нахождении состава в ТО-1 на станционных путях В мире иллюзий
В мире иллюзий Dewey e il pensiero riflessivo
Dewey e il pensiero riflessivo Заключение договора управления многоквартирным домом
Заключение договора управления многоквартирным домом ОГОНЬ,
ОГОНЬ, Катастрофы
Катастрофы Семейство розоцветные
Семейство розоцветные Парламент России
Парламент России Выжигание по дереву. Техника безопасности при работе с выжигательным аппаратом. Упражнения по выжиганию
Выжигание по дереву. Техника безопасности при работе с выжигательным аппаратом. Упражнения по выжиганию Использование формы правильных многогранников ПРИРОДАЧЕЛОВЕК ВИРУСЫ АРХИТЕКТУРА УПАКОВКИ БЫТОВЫЕ ПРЕДМЕТЫ КРИСТАЛЛЫ ХИМИЧЕСКИ
Использование формы правильных многогранников ПРИРОДАЧЕЛОВЕК ВИРУСЫ АРХИТЕКТУРА УПАКОВКИ БЫТОВЫЕ ПРЕДМЕТЫ КРИСТАЛЛЫ ХИМИЧЕСКИ О критериях и показателях при аттестации на квалификационные категории заместителей руководителей по административно-хозяйстве
О критериях и показателях при аттестации на квалификационные категории заместителей руководителей по административно-хозяйстве Презентация классного часа ко дню Космонавтики.
Презентация классного часа ко дню Космонавтики. КАЗНЕТ СЕГОДНЯ. - презентация
КАЗНЕТ СЕГОДНЯ. - презентация Греция
Греция o Центр корпоративного обучения « Оксфорд Класс » создан в 2007 г. в партнерстве с языковой школой Оксфорд Класс, г. Киев,Украина, год о
o Центр корпоративного обучения « Оксфорд Класс » создан в 2007 г. в партнерстве с языковой школой Оксфорд Класс, г. Киев,Украина, год о Точка Фест
Точка Фест Highland Games
Highland Games Моя семья. Семейное благополучие глазами детей, 9 класс
Моя семья. Семейное благополучие глазами детей, 9 класс Боевые роботы
Боевые роботы Борис Андреевич Ярков
Борис Андреевич Ярков Приготовление яично-масляных соусов
Приготовление яично-масляных соусов Типаж Джиджи
Типаж Джиджи