- Cardiac murmurs

Содержание
- 2. 11/12/02 Lubna Piracha, D.O. What is a Murmur? It maybe a normal or abnormal sound that
- 3. 11/12/02 Lubna Piracha, D.O. Timing and Location Timing: Systolic Diastolic Continuous Location: RUSB LUSB LLSB apex
- 4. 11/12/02 Lubna Piracha, D.O. Intensity and Frequency High Frequency MR TR AR Low Frequency MS TS
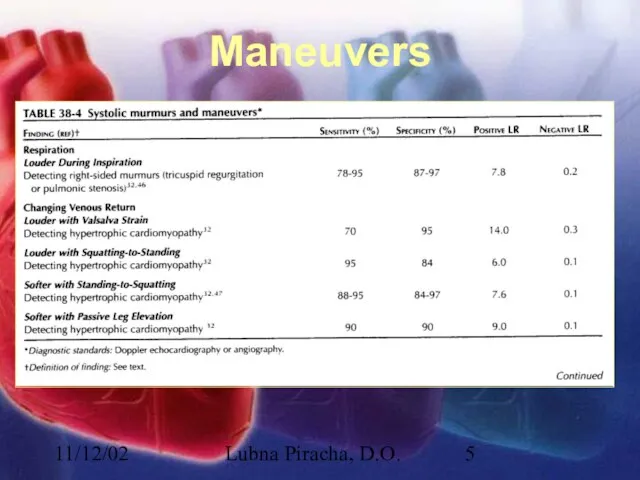
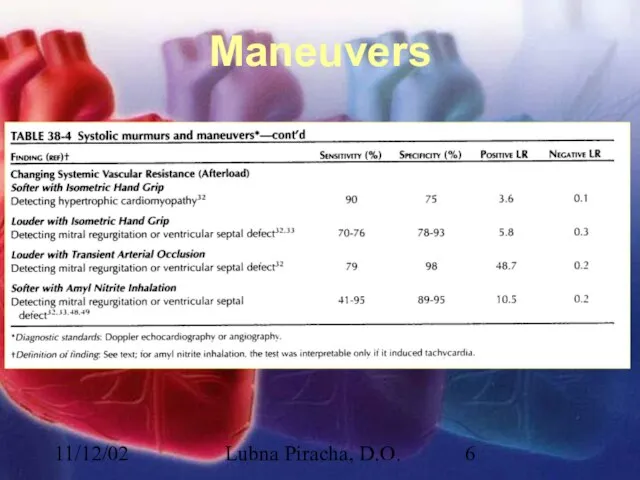
- 5. 11/12/02 Lubna Piracha, D.O. Maneuvers
- 6. 11/12/02 Lubna Piracha, D.O. Maneuvers
- 7. 11/12/02 Lubna Piracha, D.O. Case Studies A 50 year old male with a known heart murmur
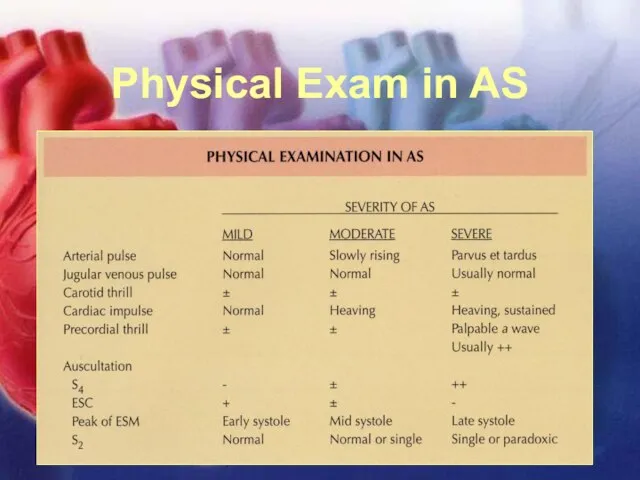
- 8. 11/12/02 Lubna Piracha, D.O. Physical Exam in AS
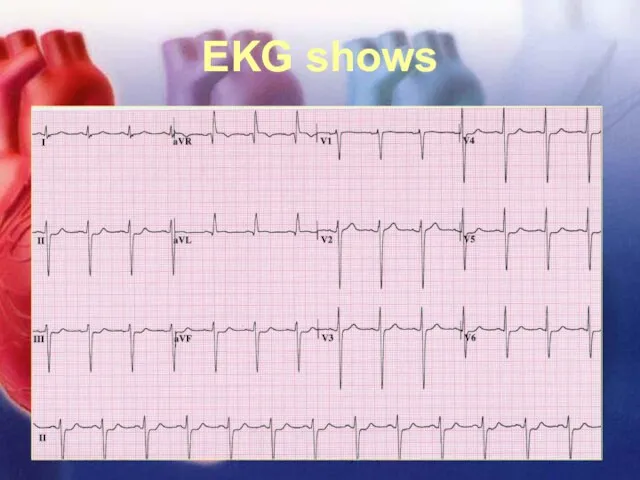
- 9. 11/12/02 Lubna Piracha, D.O. EKG shows
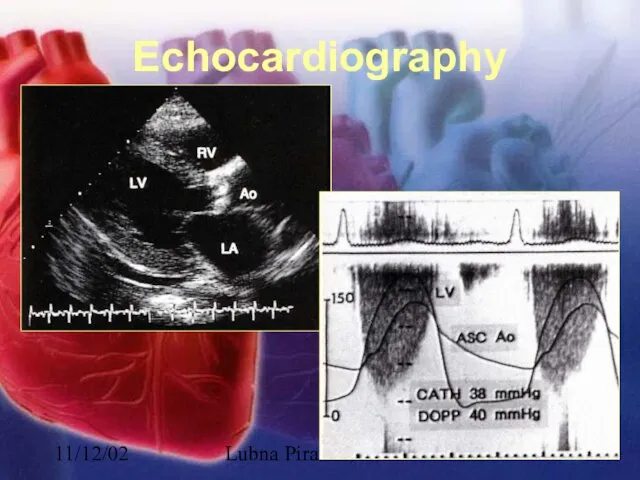
- 10. 11/12/02 Lubna Piracha, D.O. Echocardiography
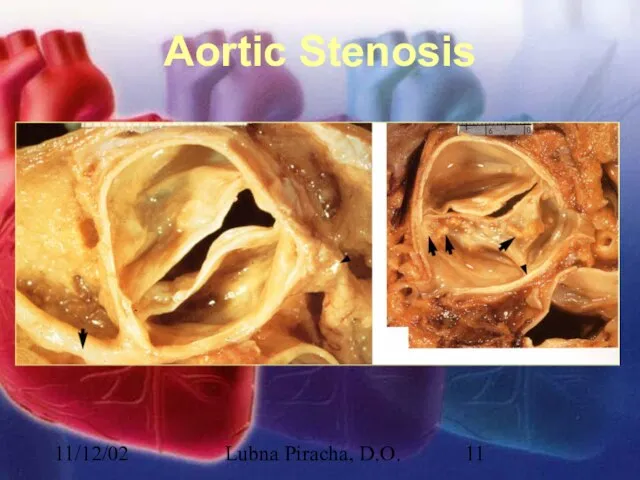
- 11. 11/12/02 Lubna Piracha, D.O. Aortic Stenosis
- 12. 11/12/02 Lubna Piracha, D.O. Aortic Stenosis There is little hemodynamic disturbance that occurs as the valve
- 13. 11/12/02 Lubna Piracha, D.O. Aortic Stenosis continued: Concentric hypertrophy develops in response to this overload. The
- 14. 11/12/02 Lubna Piracha, D.O. Case Study: A 45 year old male with a history of rheumatic
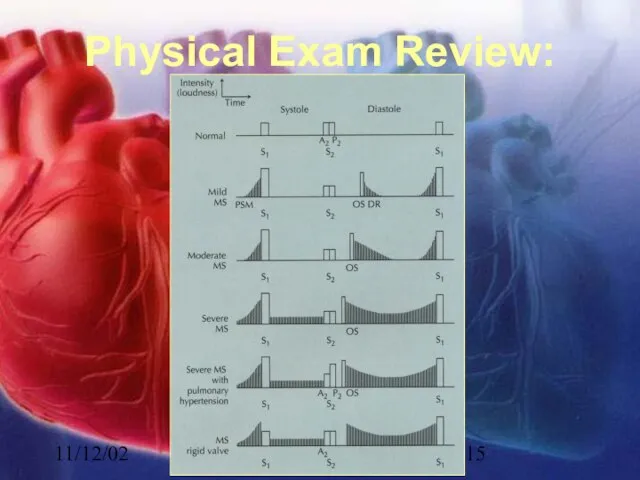
- 15. 11/12/02 Lubna Piracha, D.O. Physical Exam Review:
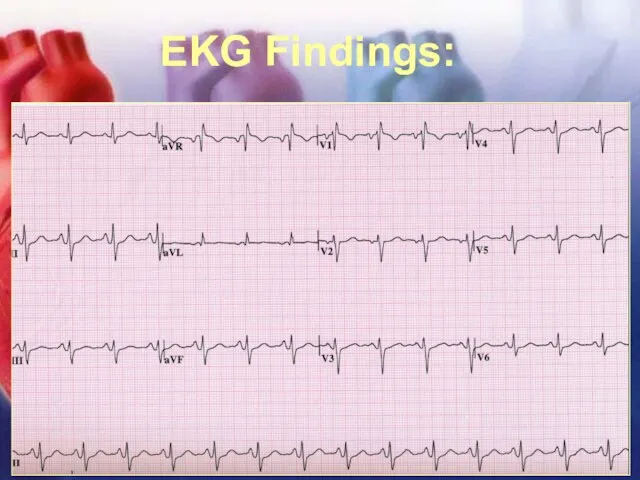
- 16. 11/12/02 Lubna Piracha, D.O. EKG Findings:
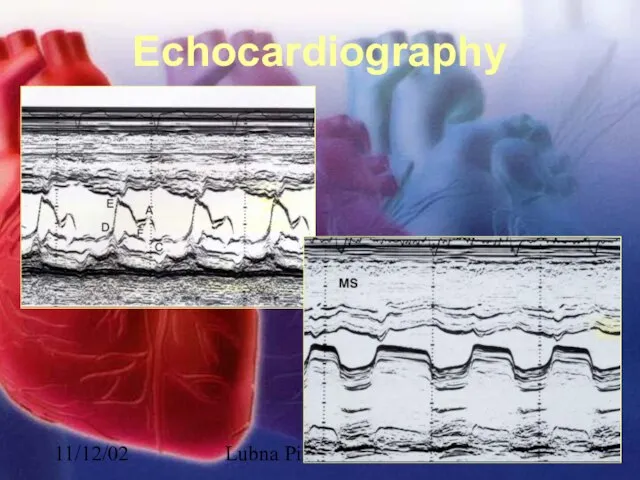
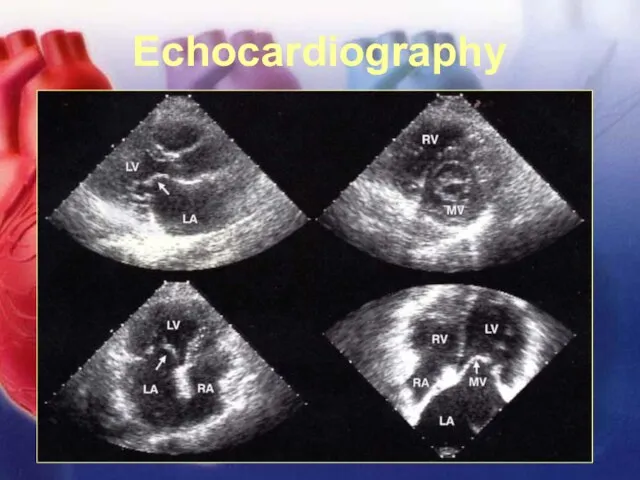
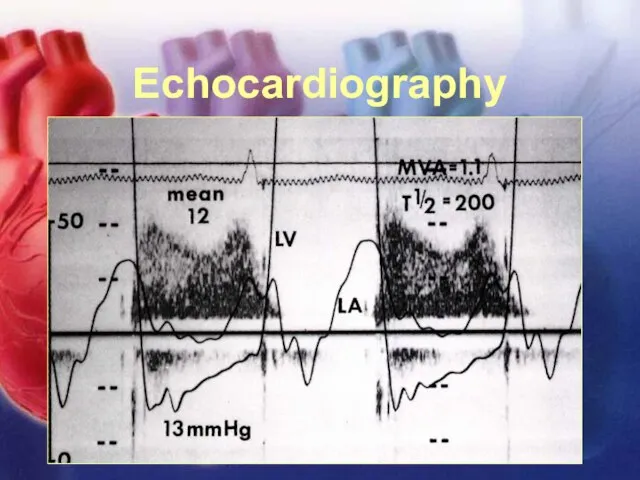
- 17. 11/12/02 Lubna Piracha, D.O. Echocardiography
- 18. 11/12/02 Lubna Piracha, D.O. Echocardiography
- 19. 11/12/02 Lubna Piracha, D.O. Echocardiography
- 20. 11/12/02 Lubna Piracha, D.O. Mitral Stenosis In severe mitral stenosis the left ventricle is spared and
- 21. 11/12/02 Lubna Piracha, D.O. Case Studies: A 52 year old female presents with complaints of slowly
- 22. 11/12/02 Lubna Piracha, D.O. Physical Exam Review Early diastolic murmur of regurgitation blowing, and high frequency,
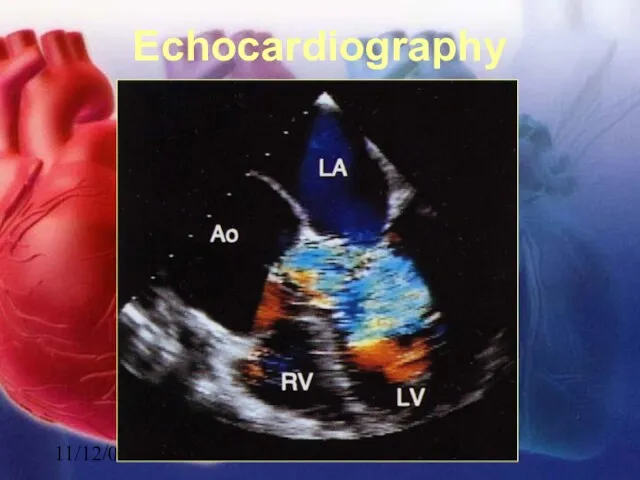
- 23. 11/12/02 Lubna Piracha, D.O. Echocardiography
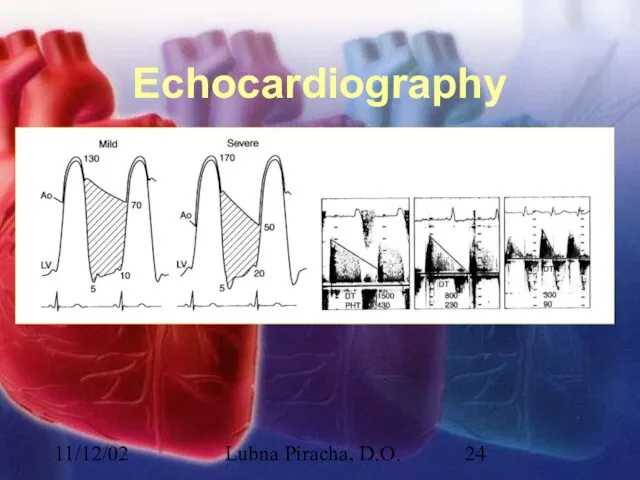
- 24. 11/12/02 Lubna Piracha, D.O. Echocardiography
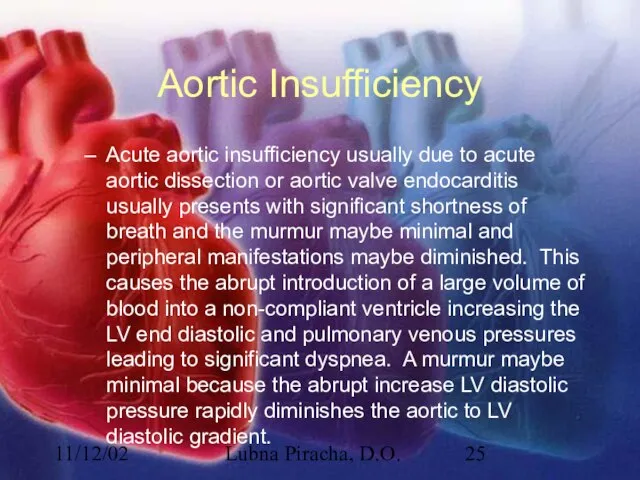
- 25. 11/12/02 Lubna Piracha, D.O. Aortic Insufficiency Acute aortic insufficiency usually due to acute aortic dissection or
- 26. 11/12/02 Lubna Piracha, D.O. Aortic Insufficiency In chronic aortic insufficiency, compensatory left ventricular changes occur over
- 27. 11/12/02 Lubna Piracha, D.O. Case Study A 75 year old male present to the emergency room
- 28. 11/12/02 Lubna Piracha, D.O. Physical Exam Review In acute MR, there is tachycardia, the murmur maybe
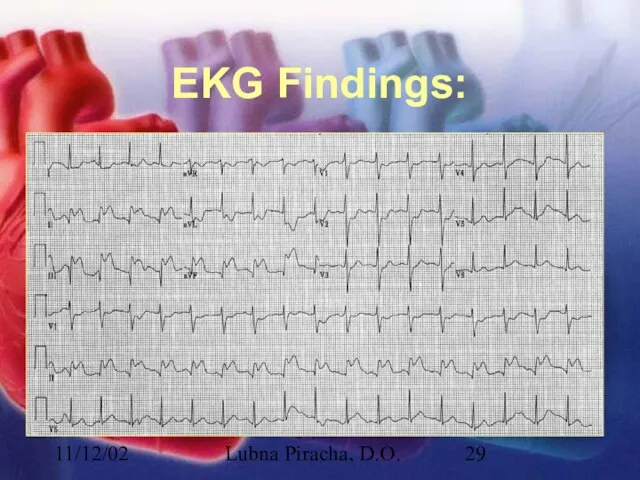
- 29. 11/12/02 Lubna Piracha, D.O. EKG Findings:
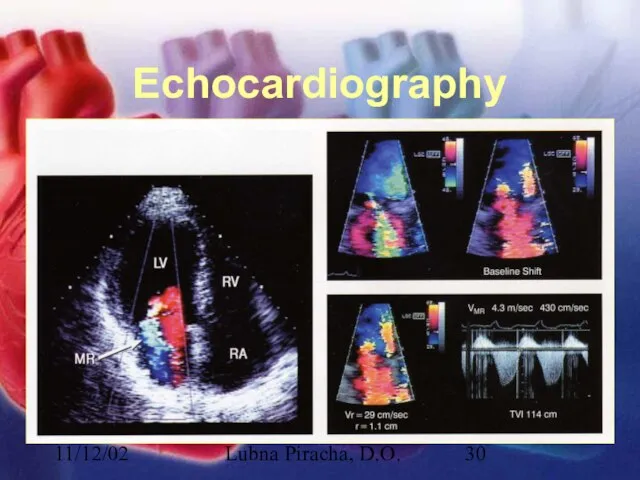
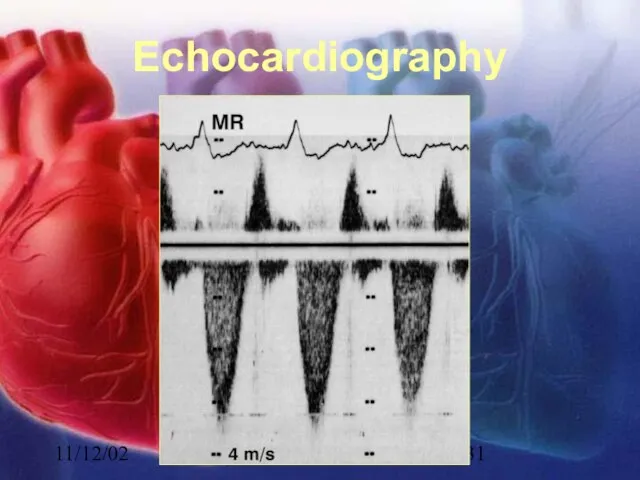
- 30. 11/12/02 Lubna Piracha, D.O. Echocardiography
- 31. 11/12/02 Lubna Piracha, D.O. Echocardiography
- 32. 11/12/02 Lubna Piracha, D.O. Mitral Regurgitation There is acute volume overload on left ventricle with an
- 33. 11/12/02 Lubna Piracha, D.O. Mitral Regurgitation In chronic MR, the LA will slowly dilate, the LV
- 34. 11/12/02 Lubna Piracha, D.O. Case Study A 22 year old male presents for a routine physical
- 35. 11/12/02 Lubna Piracha, D.O. Physical Exam Review A spike and dome arterial pulse PMI will be
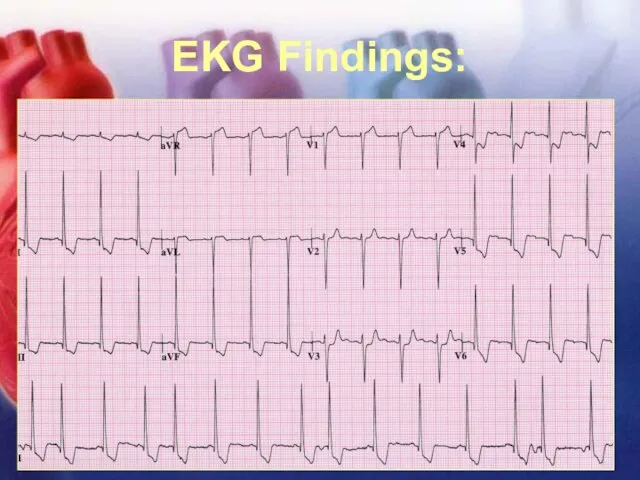
- 36. 11/12/02 Lubna Piracha, D.O. EKG Findings:
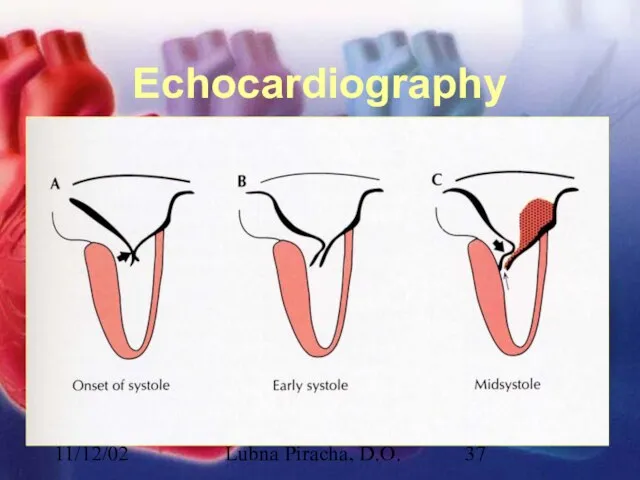
- 37. 11/12/02 Lubna Piracha, D.O. Echocardiography
- 38. 11/12/02 Lubna Piracha, D.O. Echocardiography
- 39. 11/12/02 Lubna Piracha, D.O. Echocardiography
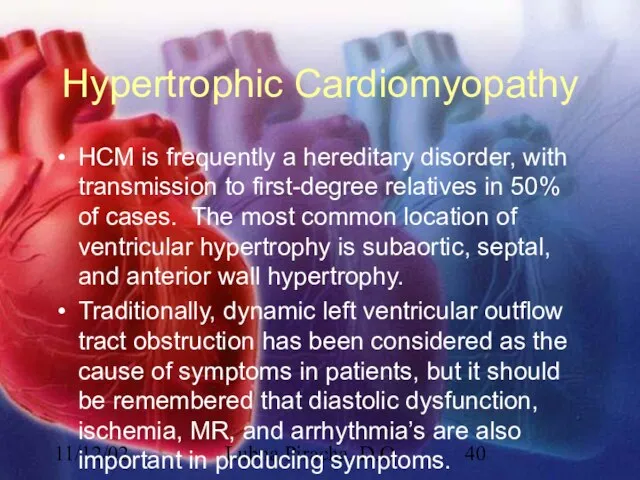
- 40. 11/12/02 Lubna Piracha, D.O. Hypertrophic Cardiomyopathy HCM is frequently a hereditary disorder, with transmission to first-degree
- 42. Скачать презентацию
Слайд 311/12/02
Lubna Piracha, D.O.
Timing and Location
Timing:
Systolic
Diastolic
Continuous
Location:
RUSB
LUSB
LLSB
apex
11/12/02
Lubna Piracha, D.O.
Timing and Location
Timing:
Systolic
Diastolic
Continuous
Location:
RUSB
LUSB
LLSB
apex
Слайд 411/12/02
Lubna Piracha, D.O.
Intensity and Frequency
High Frequency
MR
TR
AR
Low Frequency
MS
TS
Intensity
Grade 1
Grade 2
Grade 3
Grade 4
Grade
11/12/02
Lubna Piracha, D.O.
Intensity and Frequency
High Frequency
MR
TR
AR
Low Frequency
MS
TS
Intensity
Grade 1
Grade 2
Grade 3
Grade 4
Grade
Слайд 511/12/02
Lubna Piracha, D.O.
Maneuvers
11/12/02
Lubna Piracha, D.O.
Maneuvers
Слайд 611/12/02
Lubna Piracha, D.O.
Maneuvers
11/12/02
Lubna Piracha, D.O.
Maneuvers
Слайд 711/12/02
Lubna Piracha, D.O.
Case Studies
A 50 year old male with a known heart
11/12/02
Lubna Piracha, D.O.
Case Studies
A 50 year old male with a known heart
Слайд 811/12/02
Lubna Piracha, D.O.
Physical Exam in AS
11/12/02
Lubna Piracha, D.O.
Physical Exam in AS
Слайд 911/12/02
Lubna Piracha, D.O.
EKG shows
11/12/02
Lubna Piracha, D.O.
EKG shows
Слайд 1011/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Echocardiography
Слайд 1111/12/02
Lubna Piracha, D.O.
Aortic Stenosis
11/12/02
Lubna Piracha, D.O.
Aortic Stenosis
Слайд 1211/12/02
Lubna Piracha, D.O.
Aortic Stenosis
There is little hemodynamic disturbance that occurs as the
11/12/02
Lubna Piracha, D.O.
Aortic Stenosis
There is little hemodynamic disturbance that occurs as the
Слайд 1311/12/02
Lubna Piracha, D.O.
Aortic Stenosis continued:
Concentric hypertrophy develops in response to this overload.
11/12/02
Lubna Piracha, D.O.
Aortic Stenosis continued:
Concentric hypertrophy develops in response to this overload.
Слайд 1411/12/02
Lubna Piracha, D.O.
Case Study:
A 45 year old male with a history of
11/12/02
Lubna Piracha, D.O.
Case Study:
A 45 year old male with a history of
Слайд 1511/12/02
Lubna Piracha, D.O.
Physical Exam Review:
11/12/02
Lubna Piracha, D.O.
Physical Exam Review:
Слайд 1611/12/02
Lubna Piracha, D.O.
EKG Findings:
11/12/02
Lubna Piracha, D.O.
EKG Findings:
Слайд 1711/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Echocardiography
Слайд 1811/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Echocardiography
Слайд 1911/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Echocardiography
Слайд 2011/12/02
Lubna Piracha, D.O.
Mitral Stenosis
In severe mitral stenosis the left ventricle is
11/12/02
Lubna Piracha, D.O.
Mitral Stenosis
In severe mitral stenosis the left ventricle is
Слайд 2111/12/02
Lubna Piracha, D.O.
Case Studies:
A 52 year old female presents with complaints of
11/12/02
Lubna Piracha, D.O.
Case Studies:
A 52 year old female presents with complaints of
Слайд 2211/12/02
Lubna Piracha, D.O.
Physical Exam Review
Early diastolic murmur of regurgitation
blowing, and high frequency,
11/12/02
Lubna Piracha, D.O.
Physical Exam Review
Early diastolic murmur of regurgitation
blowing, and high frequency,
Слайд 2311/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Echocardiography
Слайд 2411/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Echocardiography
Слайд 2511/12/02
Lubna Piracha, D.O.
Aortic Insufficiency
Acute aortic insufficiency usually due to acute aortic dissection
11/12/02
Lubna Piracha, D.O.
Aortic Insufficiency
Acute aortic insufficiency usually due to acute aortic dissection
Слайд 2611/12/02
Lubna Piracha, D.O.
Aortic Insufficiency
In chronic aortic insufficiency, compensatory left ventricular changes occur
11/12/02
Lubna Piracha, D.O.
Aortic Insufficiency
In chronic aortic insufficiency, compensatory left ventricular changes occur
Слайд 2711/12/02
Lubna Piracha, D.O.
Case Study
A 75 year old male present to the emergency
11/12/02
Lubna Piracha, D.O.
Case Study
A 75 year old male present to the emergency
Слайд 2811/12/02
Lubna Piracha, D.O.
Physical Exam Review
In acute MR, there is tachycardia, the murmur
11/12/02
Lubna Piracha, D.O.
Physical Exam Review
In acute MR, there is tachycardia, the murmur
Слайд 2911/12/02
Lubna Piracha, D.O.
EKG Findings:
11/12/02
Lubna Piracha, D.O.
EKG Findings:
Слайд 3011/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Echocardiography
Слайд 3111/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Echocardiography
Слайд 3211/12/02
Lubna Piracha, D.O.
Mitral Regurgitation
There is acute volume overload on left ventricle with
11/12/02
Lubna Piracha, D.O.
Mitral Regurgitation
There is acute volume overload on left ventricle with
Слайд 3311/12/02
Lubna Piracha, D.O.
Mitral Regurgitation
In chronic MR, the LA will slowly dilate, the
11/12/02
Lubna Piracha, D.O.
Mitral Regurgitation
In chronic MR, the LA will slowly dilate, the
Слайд 3411/12/02
Lubna Piracha, D.O.
Case Study
A 22 year old male presents for a routine
11/12/02
Lubna Piracha, D.O.
Case Study
A 22 year old male presents for a routine
Слайд 3511/12/02
Lubna Piracha, D.O.
Physical Exam Review
A spike and dome arterial pulse
PMI will be
11/12/02
Lubna Piracha, D.O.
Physical Exam Review
A spike and dome arterial pulse
PMI will be
Слайд 3611/12/02
Lubna Piracha, D.O.
EKG Findings:
11/12/02
Lubna Piracha, D.O.
EKG Findings:
Слайд 3711/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Echocardiography
Слайд 3811/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Echocardiography
Слайд 3911/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Echocardiography
Слайд 4011/12/02
Lubna Piracha, D.O.
Hypertrophic Cardiomyopathy
HCM is frequently a hereditary disorder, with transmission to
11/12/02
Lubna Piracha, D.O.
Hypertrophic Cardiomyopathy
HCM is frequently a hereditary disorder, with transmission to
 Презентация на тему Что такое информация. Виды информации
Презентация на тему Что такое информация. Виды информации Программасоциально-экономического развития Пермского краяна 2009-2012 годыи на период до 2017 годаВ.А.Сухих, председатель Правите
Программасоциально-экономического развития Пермского краяна 2009-2012 годыи на период до 2017 годаВ.А.Сухих, председатель Правите Устное народное творчество Урала.
Устное народное творчество Урала. Количественные имена числительные
Количественные имена числительные Балансовый метод исследования в Зарубежном туристском страноведении
Балансовый метод исследования в Зарубежном туристском страноведении Отчет за 1 квартал2011-2012
Отчет за 1 квартал2011-2012 Решение задач механики жидкости и газа с использованием прикладного пакета инженерного анализа STAR-CD
Решение задач механики жидкости и газа с использованием прикладного пакета инженерного анализа STAR-CD «Прозрачный диалог с властью как форма общественного контроля» г.Новосибирск 15 сентября 2011г.
«Прозрачный диалог с властью как форма общественного контроля» г.Новосибирск 15 сентября 2011г. Экскурсия в лес
Экскурсия в лес Понятие и признаки права
Понятие и признаки права План как вектор перемен
План как вектор перемен «СВОЯ ИГРА»
«СВОЯ ИГРА» Резултатите в Google.bg по ключова дума "аквичоп" 22.07.2011
Резултатите в Google.bg по ключова дума "аквичоп" 22.07.2011 Доклад Тема: «Редкие животные Алтайского края» Выполнила: Ускова К.
Доклад Тема: «Редкие животные Алтайского края» Выполнила: Ускова К.  Основные механизмы повышения качества дошкольного образования
Основные механизмы повышения качества дошкольного образования Маркетинговая стратегия бизнес-планирования (часть 1)
Маркетинговая стратегия бизнес-планирования (часть 1) ДЕВЯТЬ ДЕСЯТЫХ МИРА…
ДЕВЯТЬ ДЕСЯТЫХ МИРА… Секреты продаж через системы онлайн-консультаций
Секреты продаж через системы онлайн-консультаций 7840fc6f2793659aec37bad987934ba7073b57be-1664610122974
7840fc6f2793659aec37bad987934ba7073b57be-1664610122974 Past simple
Past simple ЧИЧКОВСКАЯ СРЕДНЯЯ ОБЩЕОБРАЗОВАТЕЛЬНАЯ ШКОЛА
ЧИЧКОВСКАЯ СРЕДНЯЯ ОБЩЕОБРАЗОВАТЕЛЬНАЯ ШКОЛА Системы стандартизации и добровольной оценки соответствия НОСТРОЙ
Системы стандартизации и добровольной оценки соответствия НОСТРОЙ Улучшение городской среды
Улучшение городской среды Конфликты и пути их разрешения
Конфликты и пути их разрешения Результаты эволюции
Результаты эволюции Формирование образа центральной библиотеки региона в виртуальной среде:анализ веб-сайтов
Формирование образа центральной библиотеки региона в виртуальной среде:анализ веб-сайтов КООРДИНАТНАЯ ПЛОСКОСТЬ
КООРДИНАТНАЯ ПЛОСКОСТЬ Становление и развитие дополнительного образования с 1907 года до 1917 года
Становление и развитие дополнительного образования с 1907 года до 1917 года